Abstract
Background and Objectives: This study aims to evaluate the adequacy of the liberal transfusion strategy applied in patients undergoing endoscopy-assisted Metopic, Coronal, or Sagittal craniosynostosis surgery according to the Pre-Transfusion and Post-Transfusion Estimated Red Blood Cell Mass (ERCM) ratios. Materials and Methods: This retrospective cohort study, conducted at the Pamukkale University Faculty of Medicine (2017–2023), utilized anesthesia, surgical records, and hospital electronic data of patients undergoing endoscopic craniosynostosis surgery. The primary endpoints were the rates of Post-Transfusion 1st-hour ERCM/Pre-Transfusion ERCM (%) and Post-Transfusion 24th-hour ERCM/Pre-Transfusion ERCM (%). The secondary endpoints were determined as Hemoglobin (Hb) and Hematocrit (Hct) values at the 1st and 24th hours after surgery, Calculated Blood Loss (CBL) during surgery (%), total 24 h CBL (%), ERCM (%), and Estimated Blood Loss (EBV) during surgery and total 24 h transfusions, Packed Red Blood Cells (PRBCs) (mL/kg) amounts during surgery, and total 24 h transfusions. Results: A total of 86 pediatric craniosynostosis cases were evaluated and categorized into Metopic (n = 38), Sagittal (n = 33), and Coronal (n = 15) groups, with Post-Transfusion evaluation conducted across these groups. Post-Transfusion 1st-hour ERCM/Pre-Transfusion ERCM ratios were found to have median values of 90.70% in the Metopic group, 91.61% in the Sagittal group, and 93.09% in the Coronal group. Post-Transfusion 24th-hour ERCM/Pre-Transfusion ERCM ratios were found to be median values of 94.05% in the Metopic group, 88.3% in the Sagittal group, and 87.08% in the Coronal group. Conclusions: The liberal transfusion strategy provided adequate transfusion, maintaining ERCM ratios within the 85–115% range across all groups. Significant decreases in Hb and Hct levels were observed from preoperative to postoperative measurements at 1 and 24 h. Changes in CBL, ERCM, EBV, and PRBC volumes were noted between the postoperative 1 h and 24 h measurements across all groups.
1. Introduction
Craniosynostosis, a congenital anomaly characterized by the premature closure of one or more cranial sutures, restricts brain development and causes abnormal head shapes [1]. While often isolated, it may be associated with genetic syndromes. Diagnosis involves clinical evaluation, physical examination, and imaging, with surgical intervention being the only treatment to prevent intracranial pressure and cosmetic issues [2]. Open cranial vault surgery, commonly performed between 6 and 12 months, is effective but associated with prolonged recovery and significant blood loss [3]. Alternatively, endoscopy-assisted craniosynostosis surgery (EACS) combined with helmet therapy, typically performed before 6 months of age, offers reduced bleeding and shorter recovery times [4].
A critical challenge in craniosynostosis surgery is managing fluid and blood transfusion due to the significant blood loss associated with the large cranial structure in pediatric patients [5]. The accurate assessment of blood loss remains difficult, often leading to risks from under- or over-transfusion [6]. Current transfusion practices rely on Estimated Blood Loss (EBL) and Hemoglobin (Hb) levels, with guidelines recommending minimum intraoperative Hb levels of 8–10 g/dL, to prevent hypoxia and complications [7,8,9]. The European Society of Anaesthesiology and Intensive Care suggests target Hb levels of 7–9 g/dL for intraoperative bleeding, excluding premature infants and cyanotic neonates [10]. However, standard Hb threshold values have not yet been specified regarding transfusion protocol and management in pediatric neurosurgery [11].
Although more studies are needed to determine the ideal Hb level in pediatric patients, recent research suggests that avoiding unnecessary transfusions for non-ongoing bleeding in pediatric surgery is appropriate and highlights the need for individualized transfusion decisions based on physiological conditions rather than fixed Hb thresholds [12,13]. Proposed target Hb levels in pediatric neurosurgical patients vary, with recommendations such as 9.5 g/dL for transfusion and acceptable changes in Estimated Red Blood Cell Mass (ERCM) ranging from 12% to 15% to guide transfusion appropriateness [13,14,15].
This study evaluates the adequacy of liberal transfusion strategies in patients undergoing EACS for Metopic, Coronal, or Sagittal craniosynostosis using Pre- and Post-Transfusion ERCM ratios. We hypothesize that while transfusion adequacy will be maintained across surgical subtypes, there may be an increased rate of excessive transfusions.
2. Materials and Methods
This retrospective cohort study was conducted at Pamukkale University’s Faculty of Medicine between 2017 and 2023 using anesthesia and surgical records of patients undergoing EACS and information obtained from hospital electronic data systems. This study was approved by the Ethics Committee of Non-Interventional Clinical Trials of Pamukkale University (Date and Number of Approval: 10 January 2024, E.474199) and was carried out in accordance with the Declaration of Helsinki.
2.1. Data Collection
Patients who underwent EACS were divided into three groups: Metopic, Coronal, and Sagittal, according to the type of closed suture. Gender, age (day), weight (kg), and American Society of Anesthesiologists (ASA) score were recorded for the patients in each group. The amount of fluid they received during the intraoperative (Intra-op) period was recorded in milliliters (mL), and the duration of anesthesia and surgery was recorded in minutes (min). The duration of anesthesia was defined as the time between anesthesia induction and the patient’s awakening, while the surgical time was defined as the time between the start of the surgical incision and the final closing suture. The duration of each patient’s stay in the intensive care unit was recorded in hours, and their stay in the ward and the hospital was recorded as days. It was also recorded whether the patients experienced death during their hospitalization. The Hb and Hematocrit (Hct) values of all patients at preoperative (Pre-op) and postoperative (Post-op) 1 and 24 h were recorded. Blood samples taken within the first hour of each patient’s admission to Post-op intensive care, and the first blood samples taken on the next day of surgery were, respectively, “Post-op 1. the hour” and “Post-op 24. the watch was described as having” values of. The amount of allogeneic Packed Red Blood Cells (PRBCs) transfused into the patients in the intraoperative period, postoperative period, and the first 24 h were recorded in mL.
2.2. Inclusion Criteria
Patients under one year of age who underwent EACS, underwent allogeneic PRBC transfusion during the Intra-op period, and underwent standard anesthesia and surgical protocols were included in this study.
2.3. Exclusion Criteria
Patients who had a known blood transfusion before surgery; those with a syndrome; those who had more than one closed suture line; those whom another surgeon operated on; those who were re-operated; those who had an abnormal International Normalized Ratio, Prothrombin Time, or Activated Partial Thromboplastin Time value during the Pre-op period; those with a platelet count below 100,000/mm3, known bleeding history, or abnormal electrolyte imbalance in Sodium (mEq/L), Potassium (mEq/L), Calcium (mg/dL or mmol/L), and Chloride (mEq/L) levels; and those known to be taking nonsteroidal anti-inflammatory drugs that may affect the bleeding profile prior to surgery were excluded from this study.
2.4. Surgical Technique
EACS was preferred for all synostosis types in our study. A single surgeon performed all the surgeries. Patients with Metopic suture synostosis were generally taken to the operating table in a supine and neutral position. A transverse skin incision of approximately 3 cm was made at the anterior border of the hairline. After a burr hole was placed on the 1 cm lateral to the Metopic suture, craniectomy was performed by crossing the middle line with the help of a rongeur. The subcutaneous and epidural areas were dissected with the help of an endoscope. Craniectomy was performed first posteriorly to bregma, then to the anterior interorbital, extending to an approximately 1–2 cm triangular suturectomy. During craniectomy, the nasofrontal suture was preserved in the anterior, and the procedure was performed up to the nasofrontal suture.
Patients with Sagittal suture synostosis were usually taken to the operating table in the prone position with a slight head extension (Sphinx position). However, a supine full lateral position was also preferred in some patients. Depending on the surgeon’s preference, a single or two incisions were performed along the Sagittal suture. After placing the burr hole 1 cm lateral to the Sagittal suture, craniectomy was performed by crossing the suture with the help of a rongeur. The emissary’s veins were cauterized using an endoscope, and a craniectomy was performed along the suture line. The craniectomy width was determined as 2–4 cm. Bregma in the anterior and lambda in the posterior were accepted as the limits of suturectomy.
Patients with Coronal suture synostosis were taken to the operating table with their heads turned to the side and contralateral in the supine position. A linear skin incision of approximately 3 cm in length was made parallel to the Coronal suture to center the Stephanion point. The craniectomy width was between 1 and 2 cm. Bleeding from the bone at the pterion level was carefully stopped with the help of an endoscope. The suturectomy boundaries were accepted as being between the bregma and the pterion point.
2.5. Anesthesia Management
All surgical procedures were performed under general anesthesia. Standard monitoring included electrocardiography, invasive arterial blood pressure, capnography, pulse oximetry, body temperature measurement with a skin probe, and central venous pressure monitoring with the help of a central venous catheter. A heating blanket was applied to all patients to prevent heat loss during the Intra-op period. Anesthesia induction was achieved using propofol (2.0 mg/kg) and rocuronium (0.6 mg/kg). Anesthesia was maintained with a sevoflurane and remifentanil infusion of 0.1–0.2 µg/kg/min. In order to reduce the amount of bleeding, tranexamic acid (10 mg/kg loading, followed by 5 mg/kg maintenance) was started after intubation and given to all patients during the anesthesia period. Tranexamic acid was not given to the patients in the Post-op period. Autologous transfusion, Pre-op hemodilution, and blood preservative techniques or devices were not used in any of the patients.
A balanced crystalloid solution (2.5% dextrose and 0.45% isotonic saline) was administered as a continuous infusion for maintenance fluid therapy. According to the Pre-op fasting period, Intra-op fluid losses, and basal fluid requirements, the amount of fluid was determined by the anesthesiologist who followed the patient during the operation. Allogeneic PRBC transfusion was performed in all patients during the Intra-op period.
Although there is no standard protocol for transfusion in EACS, allogenic PRBC transfusion is routinely performed with the joint approval of the anesthesia and surgical teams if the Hb level drops below 9 g/dL or is expected in cases of ongoing bleeding in our clinic, and a Hb level of 10 g/dL and above is targeted after transfusion.
At the end of the surgery, paracetamol 15 mg/kg intravenous infusion was given to all patients to provide Post-op analgesia. All patients were extubated in the operating room.
Post-Transfusion in our study 1st-hour ERCM/Pre-Transfusion ERCM and Post-Transfusion 24th-hour ERCM/Pre-Transfusion ERCM rates are below 85% “insufficient transfusion”, 85–115% among them, it was defined as “sufficient transfusion” and over 115% as “excessive transfusion”. This calculation method has been used to evaluate transfusion adequacy in previous studies [14,15]. In addition, the Calculated Blood Loss (CBL) percentage, Transfusion ERCM (%), and transfusion Estimated Blood Volume (EBV) (%) were calculated for each patient according to the methods used by Lopez et al. [16]. The Hct value of the PRBCs used in our hospital was taken as 70(%). Perioperative Transfusion Volumes, Percentages, and Blood Loss Calculations are shown in Table 1.

Table 1.
Perioperative Transfusion Volumes, Percentages, and Blood Loss Calculations.
The primary endpoints were the rates of Post-Transfusion 1st-hour ERCM/Pre-Transfusion ERCM/and Post-Transfusion 24th-hour ERCM/Pre-Transfusion ERCM (%)/Pre-Transfusion ERCM. The secondary endpoints were determined as Hb and Hct values at the 1st and 24th hours after surgery; CBL during surgery (%); total 24 h CBL (%); ERCM (%); EBV during surgery and total 24 h transfusions; and PRBC (mL/kg) amounts during surgery and total 24 h transfusions.
2.6. Statistical Analysis
For the power analysis of this study, G*Power version 3.1.9.7. was used. Craniosynostosis cases with a prevalence of 0.02% were used to calculate 95% validity and 95% reliability for the patients to be included in this study. It was determined that a total of 36 patients would be sufficient. The collected data were analyzed using the IBM Statistical Package for the Social Sciences 25.0 software. The Chi-square test was used to compare the initial characteristics of nominal variables. The Mann–Whitney U test was used to analyze continuous variables between the groups. The Wilcoxon test was used to compare the transfusion percentages between the groups. The numerical variables obtained were written as Mean ± SD (Median). A value of p < 0.05 was considered statistically significant in all analyses.
3. Results
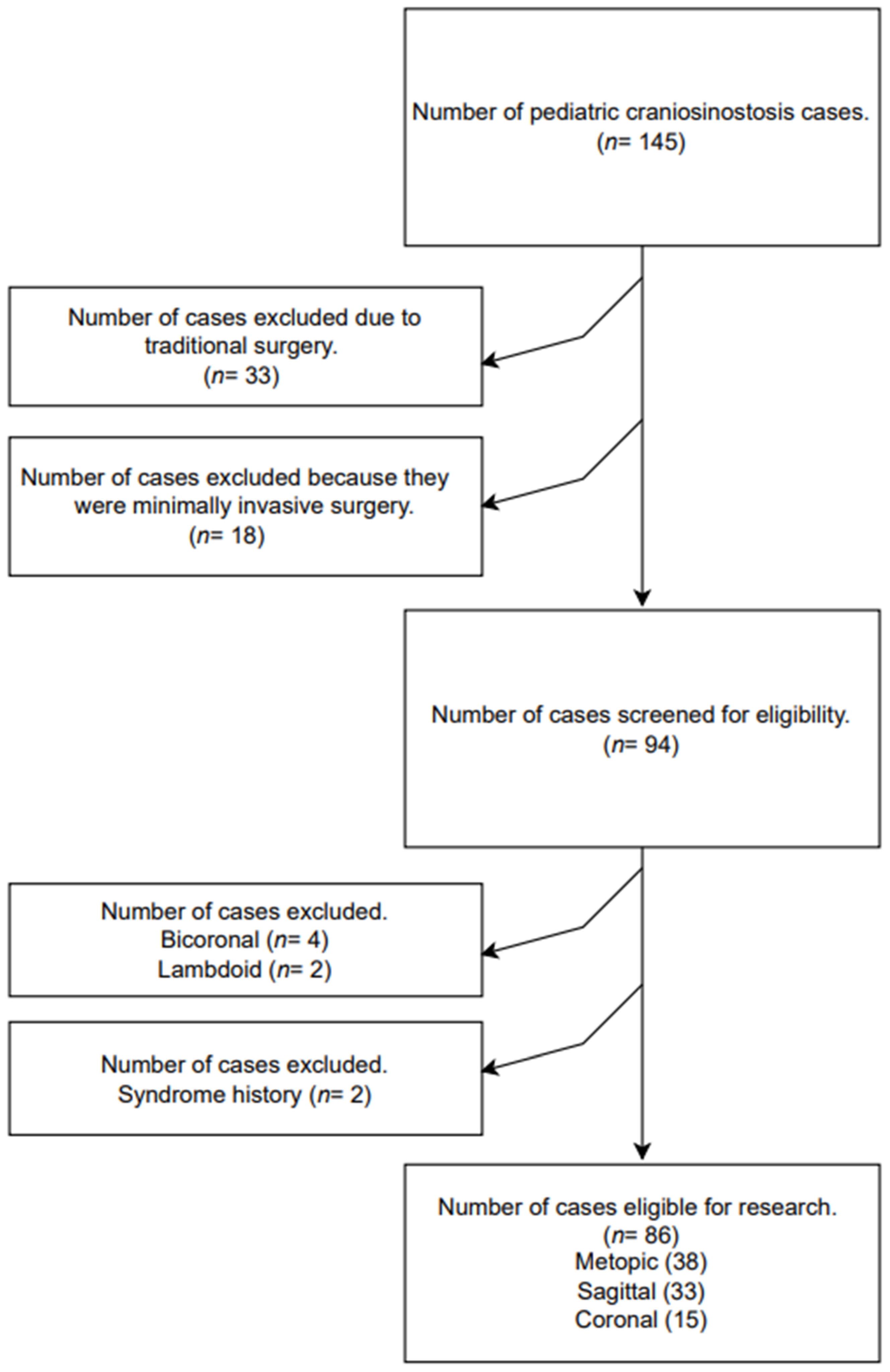
A total of 145 pediatric cases of craniosynostosis were evaluated in this study. In total, 33 patients who underwent open surgery and 18 who underwent minimally invasive surgery were excluded from this study. Out of 94 patients, 4 bi-Coronal, 2 lambdoid, and 2 syndromic patients were excluded, and a total of 86 patients were included in this study. The patients were divided into three groups: Metopic (n = 38), Sagittal (n = 33), and Coronal (n = 15) (Figure 1).
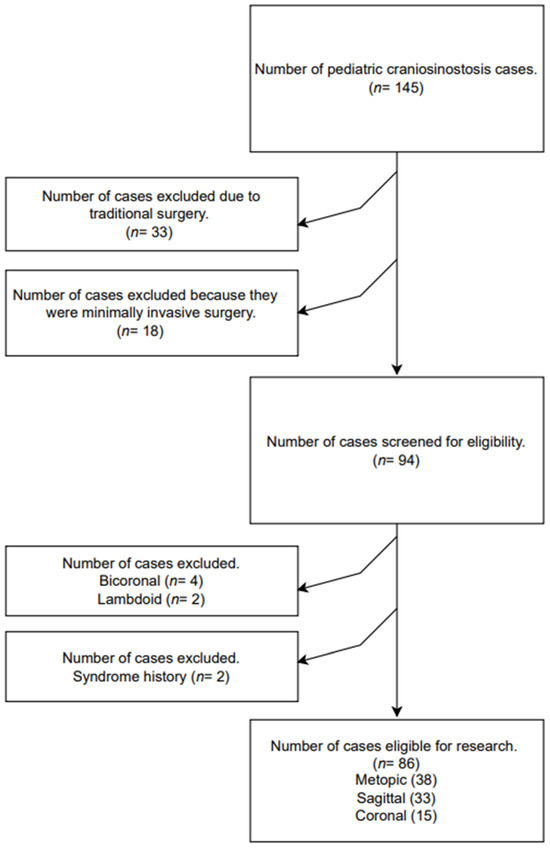
Figure 1.
Flowchart.
Our study examined the demographic and perioperative parameters in the Metopic, Sagittal, and Coronal groups (Table 2). In the Metopic group, 23.7% were female and 76.3% were male. In the Sagittal group, 21.2% were female and 78.8% were male. In the Coronal group, 46.7% were female and 53.3% were male. The mean age was 93.29 ± 17.98 days in the Metopic group, 89.61 ± 16.71 days in the Sagittal group, and 98.93 ± 21.26 days in the Coronal group. The mean weight was 5.47 ± 1.19 kg in the Metopic group, 5.32 ± 1.09 kg in the Sagittal group, and 5.47 ± 1.28 kg in the Coronal group.
Table 2.
Demographic and perioperative parameters according to Metopic, Sagittal, and Coronal groups.
ASA scores were found to be mostly ASA 1 with 94.7(%) in the Metopic group, ASA 1 with 84.8(%) in the Sagittal group, and ASA 1 with 80(%) in the Coronal group.
The mean duration of surgery was 58.89 ± 17.16 min in the Metopic group, 67.88 ± 32.26 min in the Sagittal group, and 57 ± 9.02 min in the Coronal group. The mean duration of general anesthesia was 182.89 ± 52.37 min in the Metopic group, 176.52 ± 46.85 min in the Sagittal group, and 168.33 ± 37.78 min in the Coronal group.
Intra-hospital death was observed in 1.36(%) of all patients, while no mortality was observed in the Coronal group.
The median of the delivered liquid amounts is 50.00 mL for Metopic, 55.00 mL for Sagittal, and 45.00 mL for Coronal. There was no statistical difference between age, weight, ASA score, the duration of surgery, the duration of general anesthesia, the amount of fluids given, the duration of intensive care, and hospital stay between all groups (p > 0.05). During the Intra-op period, the median is 50 mL in each group (range 40–60 mL). In the Post-op period, the median values are 22.5 mL (range 0–51.25 mL) for Metopic, 30 mL (range 0–50 mL) for Sagittal, and 30 mL (range 0–40 mL) for Coronal. The total transfusion amounts for the first 24th hour were measured as median values of 75 mL for Metopic and Coronal and 80 mL for Sagittal.
There was no statistically significant difference between the groups according to Intra-op, Post-op, and total first 24th-hour Transfusion PRBC amounts (p > 0.05).
In our study, Post-Transfusion evaluation was performed between the Metopic, Sagittal, and Coronal groups. Within the group, the Post-Transfusion 1st-hour ERCM/Pre-Transfusion ERCM and Post-Transfusion 24th-hour Hourly ERCM/Pre-Transfusion ERCM ratios were evaluated (Table 3). The Post-Transfusion 1st-hour ERCM/Pre-Transfusion ERCM Ratios were found to have median values of 90.70(%) (93.6 ± 14.1) in the Metopic group, 91.61(%) (93.96 ± 14.84) in the Sagittal group, and 93.09(%) (97.28 ± 18.1) in the Coronal group.
Table 3.
Post-Transfusion in Metopic, Sagittal, and Coronal Groups 1st-hour ERCM/Pre-Transfusion ERCM vs Post-Transfusion 24th-hour ERCM/Comparison of Pre-Transfusion ERCM Rates.
The percentage of patients with an ERCM/Pre-Transfusion ERCM below 85(%) at the Post-Transfusion 1st-hour was 26.3(%) in the Metopic group, 25.2(%) in the Sagittal group, and 26.7(%) in the Coronal group. The ERCM/Preoperative ERCM at the 1st hour after surgery was between 85% and 115%; the percentage of patients was 63.2% in the Metopic group, 69.7% in the Sagittal group, and 60% in the Coronal group. The percentage of patients with a Post-op 1st hour ERCM/Pre-op ERCM above 115% was recorded as 10.5% in the Metopic group, 6.1% in the Sagittal group, and 13.2% in the Coronal group.
There was no significant difference between the ERCM/Pre-Transfusion ERCM Ratios between the groups and within the group at the Post-Transfusion 1st-hour (p = 0.921).
Post-Transfusion 24th-hour ERCM/Pre-Transfusion ERCM Ratios were found to be Median values of 94.05(%) (94.36 ± 12.67) in the Metopic group, 88.3(%) (90.45 ± 18.28) in the Sagittal group, and 87.08(%) (91.69 ± 18.1) in the Coronal group.
The percentage of patients with an ERCM/Pre-Transfusion ERCM below 85% at the Post-Transfusion 24th-hour was found to be 18.4% in the Metopic group, 36.4% in the Sagittal group, and 20% in the Coronal group. The percentage of patients with a Post-Transfusion 24th-hour ERCM/Pre-Transfusion ERCM between 85% and 115% was found to be 78.9% in the Metopic group, 54.5% in the Sagittal group, and 73.3% in the Coronal group.
There was no significant difference between the ERCM/Pre-Transfusion ERCM Ratios between the groups and within the group at the Post-Transfusion 24th-hour (p = 0.255).
Our study showed no difference between the groups when Pre-op Hb and Hct values were compared in the Metopic, Sagittal, and Coronal groups at the 1st hour and 24th hour Post-op (p > 0.05) (Table 4).
Table 4.
Comparison of Hb, Hct, and Plt Values in Metopic, Sagittal, and Coronal Groups at Pre-op and Post-op 1st and 24th hours.
In the Metopic groups, the decrease in Hb levels at the 1st hour Post-op (10.25 ± 1.56) and 24th hour Post-op (10.18 ± 1.14) was statistically significant (p = 0.002). In Sagittal groups, the decrease in Hb levels at the 1st hour Post-op (10.14 ± 1.19) and the 24th hour Post-op (9.9 ± 1.78) was statistically significant (p = 0.001). In the Coronal group, there was no significant decrease at 1 h Post-op (p = 0.222), and the decrease in Hb levels at 24 h (9.88 ± 1.68) was significant (p = 0.020).
The decrease in Hct values between the 1st hour Post-op (29.88 ± 3.96) and the 24th hour Post-op (30.08 ± 3.36) in the Metopic groups was statistically significant (p = 0.005, p = 0.007). The decrease in Hct values between the 1st hour Post-op (30.18 ± 3.34) and the 24th hour Post-op (29.02 ± 4.98) in the Sagittal groups was statistically significant (p = 0.001, p = 0.003, respectively). In the Coronal group, while no significance was found at the 1st hour Post-op (p = 0.233), the decrease in Hct levels at 24 h (29.13 ± 4.49) was significant (p = 0.011).
Our study compared Intra-op and total first 24 h CBL, Transfusion ERCM, transfusion amounts, and Transfusion EBV between the Metopic, Sagittal, and Coronal groups (Table 5).
Table 5.
A comparison of values of the Intra-op and total first 24 h CBL of the Metopic, Sagittal, and Coronal Groups; Transfusion ERCM; Transfusion PRBC; and Transfusion EBV.
The median values of CBL in the Intra-op period were found to be 34.87% (32.81 ± 14.08) in the Metopic group, 33.66% (31.81 ± 17.3) in the Sagittal group, and 29.72% (29.75 ± 15.63) in the Coronal group. In the first 24 h, these rates increased to 45.96% (45.94 ± 14.97) in the Metopic group, 51.3% (51.3 ± 23.78) in the Sagittal group, and 52.25% (47.21 ± 19.49) in the Coronal group. These increases were statistically significant in the Metopic (p < 0.001), Sagittal (p < 0.001), and Coronal (p = 0.005) groups.
The Intra-op Transfusion ERCM values were measured as 27.14% (26.46 ± 6.94) in the Metopic group, 25.48% (27.77 ± 6.7) in the Sagittal group, and 25.7% (27.03 ± 6.84) in the Coronal group. Total First 24 h Transfusion ERCM was determined to be 52.5% (54.8 ± 16.98) in the Metopic 56% (56.68 ± 19.06) in the Sagittal group, and 52.5% (53.67 ± 16.08) in the Coronal group. These increases were statistically significant in the Metopic (p < 0.001), Sagittal (p < 0.001), and Coronal (p = 0.001) groups.
Transfusion PRBC amounts in ml/kg were found to be 10 (9.62 ± 2.39) in the Metopic group, 9.52 (9.5 ± 2.88) in the Sagittal group, and 10 (9.6 ± 2.39) in the Coronal group during the Intra-op period. During the first 24 h, these values were found to be 13.33 (14.57 ± 4.47) in the Metopic group, 15 (15.47 ± 5.22) in the Sagittal group, and 14 (14.11 ± 3.23) in the Coronal group. These increases were statistically significant in the Metopic (p < 0.001), Sagittal (p < 0.001), and Coronal (p = 0.004) groups.
The Intra-op Transfusion EBV was measured as 12.5% in the Metopic and Coronal groups and 11.9% (11.87 ± 3.6) in the Sagittal group. The Transfusion EBV values were found to be 16.49% (18.3 ± 5.41) in the Metopic group, 18.15% (19.19 ± 6.55) in the Sagittal group, and 18.33% (18.3 ± 3.87) in the Coronal group in the first 24 h. These increases were statistically significant in the Metopic (p < 0.001), Sagittal (p < 0.001), and Coronal (p = 0.003) groups.
4. Discussion
Our study evaluated the adequacy of a liberal transfusion strategy in patients undergoing Metopic, Coronal, and Sagittal endoscopic craniosynostosis surgery using Pre- and Post-Transfusion ERCM ratios. The Median Post-Transfusion ERCM/Pre-Transfusion ERCM values were within the adequate transfusion range (85–115%) across all groups: Metopic (90.7% at 1 h, 94.1% at 24 h), Sagittal (91.6% at 1 h, 88.3% at 24 h), and Coronal (93.1% at 1 h, 87.1% at 24 h). Most patients received adequate transfusions (1st hour: Metopic 63.2%, Sagittal 69.7%, Coronal 60%; 24th hour: Metopic 78.7%, Sagittal 54.5%, Coronal 73.3%). The proportion of patients receiving insufficient transfusions was higher than those receiving excessive transfusions across all groups. At the 1st postoperative hour, insufficient transfusions were observed in 26.3% of the Metopic group, 25.2% of the Sagittal group, and 26.7% of the Coronal group. By the 24th hour, these rates shifted to 18.4%, 36.4%, and 20%, respectively. In contrast, excessive transfusions were the least common, occurring in 10.5% (Metopic), 6.1% (Sagittal), and 13.2% (Coronal) of patients at the 1st hour and decreasing to 2.6%, 9.1%, and 6.7%, respectively, at the 24th hour. However, contrary to our hypothesis, insufficient transfusions exceeded excessive transfusions, likely due to a transfusion trigger of Hb < 9 g/dL compared to studies using Hct < 30% as a threshold.
Statistically significant reductions in Hemoglobin (Hb) and Hematocrit (Hct) levels were observed in the Metopic and Sagittal groups at both 1 h and 24 h postoperatively, while the Coronal group exhibited significant decreases at the 24 h mark. Additionally, the intraoperative blood loss percentage (CBL%) increased significantly across all groups within the first 24 h. The percentage of transfused estimated red cell mass (ERCM) also showed a notable increase in all groups by the 24 h mark. Correspondingly, intraoperative transfusion volumes, including Packed Red Blood Cells (PRBCs) and EBV, demonstrated significant increases across all groups within the same timeframe.
In perioperative transfusion management for patients undergoing craniosynostosis surgery, many studies have relied on EBV, ERCM, and EBL calculations [17,18,19]. However, recent research has moved away from using these calculations to assess transfusion adequacy. Older studies evaluated transfusion adequacy based on Pre-Transfusion/Post-Transfusion ERCM exchange rates. Kearney et al. reported that while 70% of intraoperative transfusions were managed correctly, only 29% were truly appropriate, leaving the majority of postoperative transfusions unnecessary [14]. Similarly, Kang et al. analyzed 43 patients who underwent primary craniosynostosis repair and found that, based on Pre-Transfusion/Post-Transfusion ERCM ratios, 18% received excessive transfusions, 70% had appropriate transfusions, and 12% were under-transfused [15]. In our study, adequate transfusion rates exceeded 60% across all groups, highlighting the effectiveness of our approach. However, the higher rates of excessive transfusion indicate a need for further optimization. The significant postoperative decrease in Hb and Hct levels, coupled with increased intraoperative blood loss (CBL%) and higher transfusion volumes (PRBC and EBV) within 24 h, underscores the critical importance of precise transfusion strategies.
Meier et al. reported an EBL of approximately 25% of the EBV during endoscopic procedures [20]. Similarly, Han et al. documented a median intraoperative transfusion volume of 36 mL in 140 patients with non-syndromic craniosynostosis, with an EBL-to-EBV ratio of 7.5% ± 5.3% [21].
The higher Calculated Blood Loss observed in our study compared to studies reporting 25% and 7.5% EBL-to-EBV ratios, respectively, may stem from our reliance on Calculated Blood Loss methods, which provide greater accuracy than subjective surgical estimates [20,21]. Some studies show that the Calculated Blood Loss method provides more accurate results than the Estimated Blood Loss of the surgical team in different surgical and age groups [7,16,22]. The literature also supports the idea that bleeding varies between surgeons in the same surgical group [23].
Sakar et al. documented a median total intraoperative and postoperative transfusion volume of 32 mL in a cohort of 31 patients [24]. Furthermore, Soobey et al. noted an average intraoperative blood transfusion volume of 3 mL/kg in 49 single-suture craniosynostosis cases, with postoperative Hematocrit values averaging 25.3% ± 3.3% and with an intraoperative crystalloid fluid use of 34 mL/kg [25]. Notably, our liberal transfusion strategy, with a trigger of Hb < 9 g/dL and a target of Hb 10 g/dL, likely contributed to higher transfusion volumes and reduced crystalloid fluid use compared to restrictive strategies reported in the literature.
Within the scope of this strategy, we think that determining the transfusion trigger threshold as Hb 9 g/dL and the target value as Hb 10 g/dL is effective in performing more PRBC transfusions and using less crystalloid fluid.
Our study’s strengths include the use of objective ERCM ratios, a homogeneous patient cohort, and a single-center, single-surgeon design, which minimizes variability and enhances data reliability. However, limitations include its retrospective design, single-center scope, and unequal subgroup sizes, which reduce generalizability and subgroup analysis strength. Variability in PRBC Hct values across institutions and the absence of a restrictive transfusion comparator group further limit this study’s applicability. Additionally, the lack of advanced techniques to reduce perioperative transfusion, such as blood recovery systems, may have influenced outcomes. In this study, transfusion-related clinical outcomes were not evaluated. To accurately assess transfusion-related clinical outcomes, it is essential to first demonstrate that sufficient and necessary transfusions have been performed.
Future studies should explore the use of laboratory and imaging methods to assess organ perfusion, adopt alternative transfusion thresholds, and evaluate blood conservation techniques, such as intraoperative blood recovery systems and pharmacologic interventions. Multi-center, prospective trials with larger patient cohorts are essential to validate and optimize transfusion protocols for endoscopic craniosynostosis surgery. These efforts will enable more individualized transfusion strategies that balance patient safety with resource utilization, ensuring optimal outcomes in this delicate pediatric population.
5. Conclusions
Using a liberal transfusion strategy, we observed that the Post-Transfusion 1st-hour and 24th-hour ERCM/Pre-Transfusion ERCM ratios remained within the 85–115% adequacy range. In intra-group analyses, most patients received adequate transfusions, followed by those with insufficient transfusions, while excessive transfusions were the least common. These patterns were consistent across all surgical groups. Our findings indicate that the liberal transfusion strategy effectively ensures adequate transfusion. However, the volume of transfusions in our study exceeded those reported in the literature, underscoring the need for more individualized, patient-centered approaches to refine transfusion decisions and improve their adequacy.
Author Contributions
Conceptualization, T.E., E.E., R.A., A.M.Y. and H.S.; methodology, T.E. and E.E.; software, T.E. and İ.Ç.; validation, T.E. and E.E.; formal analysis, T.E. and E.E.; investigation, T.E., E.E. and İ.Ç.; resources, T.E.; data curation, İ.Ç. and R.A.; writing—original draft preparation, T.E. and E.E.; writing—review and editing, T.E., E.E., B.A., İ.Ç., R.A., A.M.Y., S.İ., S.C. and H.S.; visualization, İ.Ç. and A.M.Y.; supervision, H.S.; project administration, T.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Non-Interventional Clinical Research of Pamukkale University (Date and Number of Approval: 10 January 2024, E.474199).
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare that they have no competing interests.
Abbreviations
| ASA | American Society of Anesthesiologists |
| CBL | Calculated Blood Loss |
| EACS | Endoscopy-Assisted Craniosynostosis Surgery |
| EBL | Estimated Blood Loss |
| EBV | Estimated Blood Volume |
| ERCM | Estimated Red Blood Cell Mass |
| Hb | Hemoglobin |
| Hct | Hematocrit |
| ICU | Intensive Care Unit |
| IQR | Interquartile Range |
| mL | Milliliters |
| mm3 | Cubic Millimeter |
| OR | Operating Room |
| PACU | Post-Anesthesia Care Unit |
| PRBC | Packed Red Blood Cells |
| SD | Standard Deviation |
| µg/kg/min | Micrograms per Kilogram per Minute |
| mg/kg | Milligrams per Kilogram |
| min | Minutes |
| g/dL | Grams per Deciliter |
References
- Kajdic, N.; Spazzapan, P.; Velnar, T. CCraniosynostosis—Recognition, clinical characteristics, and treatment. Bosn. J. Basic Med. Sci. 2018, 18, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Thomas, K.; Hughes, C.; Johnson, D.; Das, S. Anesthesia for surgery related to craniosynostosis: A review. Part 1. Paediatr. Anaesth. 2012, 22, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Gee, E.; Liu, C.A. Anesthesia for Innovative Pediatric Surgical Procedures. Anesthesiol. Clin. 2020, 38, 493–508. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, I.; Harrison, L.M.; Parsa, S.; Hallac, R.R.; Seaward, J.R.; Kane, A.A. Open Versus Minimally Invasive Approach for Craniosynostosis: Analysis of the National Surgical Quality Improvement Program-Pediatric. Cleft Palate Craniofacial J. 2023, 60, 804–809. [Google Scholar] [CrossRef]
- Michaëlsson, I.; Skoglund, T.; Hallén, T.; Olsson, R.; Maltese, G.; Tarnow, P.; Bhatti-Søfteland, M.; Zetterberg, H.; Blennow, K.; Kölby, L. Circulating Brain-Injury Markers After Surgery for Craniosynostosis. World Neurosurg. 2023, 173, e593–e599. [Google Scholar] [CrossRef]
- Hughes, C.; Thomas, K.; Johnson, D.; Das, S. Anesthesia for surgery related to craniosynostosis: A review. Part 2. Paediatr. Anaesth. 2013, 23, 22–27. [Google Scholar] [CrossRef]
- Seruya, M.; Oh, A.K.; Rogers, G.F.; Han, K.D.; Boyajian, M.J.; Myseros, J.S.; Yaun, A.L.; Keating, R.F. Blood loss estimation during fronto-orbital advancement: Implications for blood transfusion practice and hospital length of stay. J. Craniofacial Surg. 2012, 23, 1314–1317. [Google Scholar] [CrossRef]
- Lacroix, J.; Hébert, P.C.; Hutchison, J.S.; Hume, H.A.; Tucci, M.; Ducruet, T.; Gauvin, F.; Collet, J.-P.; Toledano, B.J.; Robillard, P.; et al. Transfusion strategies for patients in pediatric intensive care units. N. Engl. J. Med. 2007, 356, 1609–1619. [Google Scholar] [CrossRef]
- Kietaibl, S.; Ahmed, A.; Afshari, A.; Albaladejo, P.; Aldecoa, C.; Barauskas, G.; De Robertis, E.; Faraoni, D.; Filipescu, D.C.; Fries, D.; et al. Management of severe perioperative bleeding: Guidelines from the European Society of Anaesthesiology and Intensive Care: Second update 2022. Eur. J. Anaesthesiol. 2023, 40, 226–304. [Google Scholar] [CrossRef]
- Azam, F.; Neerukonda, S.V.; Smith, P.; Anand, S.; Mittal, S.; Bah, M.G.; Barrie, U.; Detchou, D.; Aoun, S.G.; Braga, B.P. Red blood cell transfusion threshold guidelines in pediatric neurosurgery. Neurosurg. Rev. 2024, 47, 555. [Google Scholar] [CrossRef]
- Rail, B.; Hicks, W.H.; Oduguwa, E.; Barrie, U.; Pernik, M.N.; Montgomery, E.; Tao, J.; Kenfack, Y.J.; Mofor, P.; Adeyemo, E.; et al. Transfusion Guidelines in Brain Tumor Surgery: A Systematic Review and Critical Summary of Currently Available Evidence. World Neurosurg. 2022, 165, 172–179.e2. [Google Scholar] [CrossRef] [PubMed]
- Downey, L.A.; Goobie, S.M. Perioperative Pediatric Erythrocyte Transfusions: Incorporating Hemoglobin Thresholds and Physiologic Parameters in Decision-making. Anesthesiology 2022, 137, 604–619. [Google Scholar] [CrossRef] [PubMed]
- Goobie, S.M.; Faraoni, D. Perioperative paediatric patient blood management: A narrative review. Br. J. Anaesth. 2024, 134, 168–179. [Google Scholar] [CrossRef]
- Kearney, R.A.; Rosales, J.K.; Howes, W.J. Craniosynostosis: An assessment of blood loss and transfusion practices. Can. J. Anaesth. 1989, 36, 473–477. [Google Scholar] [CrossRef]
- Kang, J.K.; Lee, S.W.; Baik, M.W.; Son, B.C.; Kil Hong, Y.; Jung, C.K.; Ryu, K.H. Perioperative specific management of blood volume loss in craniosynostosis surgery. Childs Nerv. Syst. 1998, 14, 297–301. [Google Scholar] [CrossRef]
- Lopez, M.M.; Lee, J.; Morrison, K.; Hoffman, C.; Souweidane, M.; Ascherman, J.A. Calculated Blood Loss and Transfusion Requirements in Primary Open Repair of Craniosynostosis. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2112. [Google Scholar] [CrossRef]
- Uslu, A.; Mogensen, S.; Lubenow, N.; Enblad, P.; Nilsson, P.; Nowinski, D.; Frykholm, P. A Transfusion Regimen With Same-donor Packed Red Blood Cells Reduces Exposure to Multiple Blood Donors in Craniosynostosis Surgery. J. Craniofacial Surg. 2024, 35, 1352–1355. [Google Scholar] [CrossRef]
- Eustache, G.; Nardi, N.; Rousseau, C.; Aouaissia, S.; Aillet, S.; Larralde, S.D.; Wodey, E.; Riffaud, L. Importance of tranexamic acid in pediatric monosutural craniosynostosis surgery. J. Neurosurg. Pediatr. 2021, 29, 412–418. [Google Scholar] [CrossRef]
- Borst, A.J.; Bonfield, C.M.; Deenadayalan, P.S.; Le, C.H.; Xu, M.; Sobey, J.H.; Reddy, S.K. ε-Aminocaproic acid versus tranexamic acid in children undergoing complex cranial vault reconstruction for repair of craniosynostosis. Pediatr. Blood Cancer 2021, 68, e29093. [Google Scholar] [CrossRef] [PubMed]
- Meier, P.M.; Goobie, S.M.; DiNardo, J.A.; Proctor, M.R.; Zurakowski, D.; Soriano, S.G. Endoscopic strip craniectomy in early infancy: The initial five years of anesthesia experience. Anesth. Analg. 2011, 112, 407–414. [Google Scholar] [CrossRef]
- Han, R.H.; Nguyen, D.C.; Bruck, B.S.; Skolnick, G.B.; Yarbrough, C.K.; Naidoo, S.D.; Patel, K.B.; Kane, A.A.; Woo, A.S.; Smyth, M.D. Characterization of complications associated with open and endoscopic craniosynostosis surgery at a single institution. J. Neurosurg. Pediatr. 2016, 17, 361–370. [Google Scholar] [CrossRef]
- Gluck, O.; Mizrachi, Y.; Kovo, M.; Divon, M.; Bar, J.; Weiner, E. Major underestimation and overestimation of visual blood loss during cesarean deliveries: Can they be predicted? Arch. Gynecol. Obstet. 2017, 296, 907–913. [Google Scholar] [CrossRef] [PubMed]
- van Uitert, A.; Megens, J.H.A.M.; Breugem, C.C.; Stubenitsky, B.M.; Han, K.S.; de Graaff, J.C. Factors influencing blood loss and allogeneic blood transfusion practice in craniosynostosis surgery. Paediatr. Anaesth. 2011, 21, 1192–1197. [Google Scholar] [CrossRef] [PubMed]
- Sakar, M.; Çevik, S.; Işık, S.; Haidar, H.; Şahin, Y.; Saçak, B.; Bayri, Y.; Dağçınar, A. Modified endoscopic strip craniectomy technique for sagittal craniosynostosis: Provides comparable results and avoids bony defects. Childs Nerv. Syst. 2022, 38, 1173–1180. [Google Scholar] [CrossRef]
- Sobey, J.H.; Menser, C.C.; Hartzog, A.J.; Hocking, K.M.; Niconchuk, J.A.; Bonfield, C.M.; Stricker, P.A.; Reddy, S.K.M. Antifibrinolytics Are Not Associated With Reduced Blood Loss in Minimally-Invasive Endoscopic-Assisted Craniectomy for Repair of Single-Suture Craniosynostosis. J. Craniofacial Surg. 2022, 33, 1312–1316. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).