
The Influence of Guiding Concept on the Accuracy of Static Computer-Assisted Implant Surgery in Partially Edentulous Cases: An In Vitro Study


Abstract
1. Introduction
2. Materials and Methods
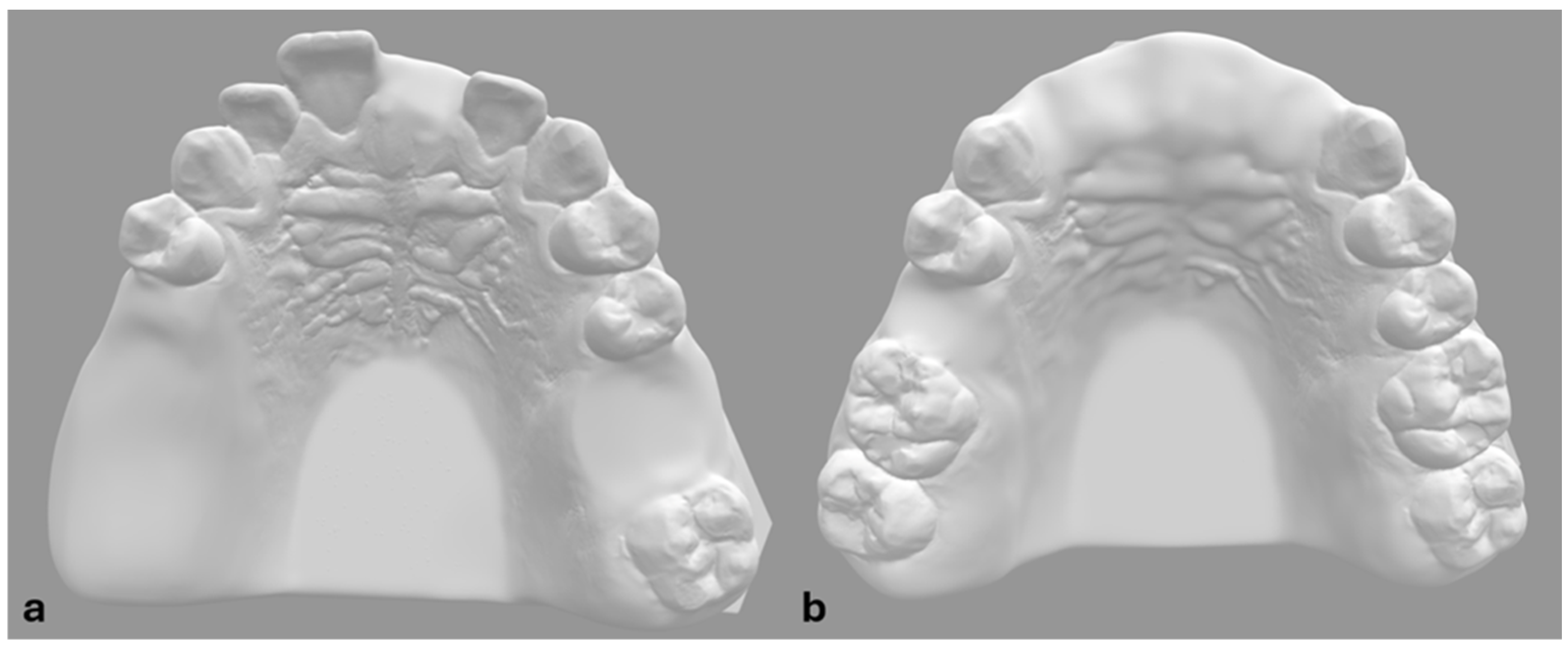
2.1. Study Groups
- Anterior single-tooth gap (AntSTG) at FDI 21 site (n = 10 implants);
- Anterior extended edentulous area (AntExt) at FDI 12 and 22 sites (n = 20 implants);
- Proximal posterior single-tooth gap (ProPosSTG) at FDI 15 site (n = 10 implants);
- Distal posterior single-tooth gap (DisPosSTG) at FDI 26 site (n = 10 implants);
- Proximal site of distal extension area (ProDE) at FDI 15 site (n = 10 implants);
- Distal site of distal extension area (DisDE) at FDI 17 site (n = 10 implants).
2.2. Accuracy Measurements
2.3. Statistical Analysis
3. Results
Different Sites of Implantation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 3D | Three Dimensional |
| CBCT | Cone Beam Computed Tomography |
| DLP | Digital Light Processing |
| FDI | Federal Dentaire Internationale |
| sCAIS | Static Computer-Assisted Implant Surgery |
| SLS | Selective Laser Sintering |
| STG | Single-tooth gap |
| STL | Standard Tessellation Language |
References
- D’haese, J.; Ackhurst, J.; Wismeijer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontol. 2000 2017, 73, 121–133. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Sennerby, L.; De Bruyn, H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. Periodontol. 2000 2017, 73, 7–21. [Google Scholar] [CrossRef]
- Van Assche, N.; Vercruyssen, M.; Coucke, W.; Teughels, W.; Jacobs, R.; Quirynen, M. Accuracy of computer-aided implant placement. Clin. Oral Implant. Res. 2012, 23 (Suppl. S6), 112–123. [Google Scholar] [CrossRef]
- Joda, T.; Derksen, W.; Wittneben, J.G.; Kuehl, S. Static computer-aided implant surgery (s-CAIS) analysing patient-reported outcome measures (PROMs), economics and surgical complications: A systematic review. Clin. Oral Implant. Res. 2018, 29 (Suppl. S16), 359–373. [Google Scholar] [CrossRef]
- Graf, T.; Keul, C.; Wismeijer, D.; Güth, J.F. Time and costs related to computer-assisted versus non-computer-assisted implant planning and surgery. A systematic review. Clin. Oral Implant. Res. 2021, 32 (Suppl. S21), 303–317. [Google Scholar] [CrossRef]
- Schnitman, P.A.; Hayashi, C.; Han, R.K. Why guided when freehand is easier, quicker, and less costly? J. Oral Implantol. 2014, 40, 670–678. [Google Scholar] [CrossRef] [PubMed]
- Varga, E., Jr.; Antal, M.; Major, L.; Kiscsatári, R.; Braunitzer, G.; Piffkó, J. Guidance means accuracy: A randomized clinical trial on freehand versus guided dental implantation. Clin. Oral Implant. Res. 2020, 31, 417–430. [Google Scholar] [CrossRef]
- Smitkarn, P.; Subbalekha, K.; Mattheos, N.; Pimkhaokham, A. The accuracy of single-tooth implants placed using fully digital-guided surgery and freehand implant surgery. J. Clin. Periodontol. 2019, 46, 949–957. [Google Scholar] [CrossRef]
- Younes, F.; Eghbali, A.; De Bruyckere, T.; Cleymae, R.; Cosyn, J. A randomized controlled trial on the efficiency of free-handed, pilot-drill guided and fully guided implant surgery in partially edentulous patients. Clin. Oral Implant. Res. 2019, 30, 131–138. [Google Scholar] [CrossRef]
- Gallardo, Y.R.; Bohner, L.; Tortamano, P.; Pigozzo, M.N.; Laganá, D.C.; Sesma, N. Patient outcomes and procedure working time for digital versus conventional impressions: A systematic review. J. Prosthet. Dent. 2018, 119, 214–219. [Google Scholar] [CrossRef]
- Vercruyssen, M.; De Laat, A.; Coucke, W.; Quirynen, M. An RCT comparing patient-centred outcome variables of guided surgery (bone or mucosa supported) with conventional implant placement. J. Clin. Periodontol. 2014, 41, 724–732. [Google Scholar] [CrossRef]
- Colombo, M.; Mangano, C.; Mijiritsky, E.; Krebs, M.; Hauschild, U.; Fortin, T. Clinical applications and effectiveness of guided implant surgery: A critical review based on randomized controlled trials. BMC Oral Health 2017, 17, 150. [Google Scholar] [CrossRef]
- Su, C.-Y.; Fu, J.-H.; Wang, H.-L. The Role of Implant Position on Long-Term Success. Clin. Adv. Periodontics 2014, 4, 187–193. [Google Scholar] [CrossRef]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S286–S291. [Google Scholar] [CrossRef] [PubMed]
- Tallarico, M.; Meloni, S.M. Retrospective Analysis on Survival Rate, Template-Related Complications, and Prevalence of Peri-implantitis of 694 Anodized Implants Placed Using Computer-Guided Surgery: Results Between 1 and 10 Years of Follow-Up. Int. J. Oral Maxillofac. Implant. 2017, 32, 1162–1171. [Google Scholar] [CrossRef]
- Gargallo-Albiol, J.; Barootchi, S.; Marqués-Guasch, J.; Wang, H.L. Fully Guided Versus Half-Guided and Freehand Implant Placement: Systematic Review and Meta-analysis. Int. J. Oral Maxillofac. Implant. 2020, 35, 1159–1169. [Google Scholar] [CrossRef]
- Tahmaseb, A.; Wismeijer, D.; Coucke, W.; Derksen, W. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 25–42. [Google Scholar] [CrossRef]
- Kasradze, D.; Segalyte, E.; Kubilius, R. Influence of clinical and technical parameters on accuracy of guided implant placement. Systematic review and meta-analysis. J. Osseointegr. 2021, 13, 198–219. [Google Scholar] [CrossRef]
- Koop, R.; Vercruyssen, M.; Vermeulen, K.; Quirynen, M. Tolerance within the sleeve inserts of different surgical guides for guided implant surgery. Clin. Oral Impl. Res. 2013, 24, 630–634. [Google Scholar] [CrossRef]
- Cassetta, M.; Di Mambro, A.; Di Giorgio, G.; Stefanelli, L.V.; Barbato, E. The Influence of the Tolerance between Mechanical Components on the Accuracy of Implants Inserted with a Stereolithographic Surgical Guide: A Retrospective Clinical Study. Clin. Implant. Dent. Relat. Res. 2015, 17, 580–588. [Google Scholar] [CrossRef]
- Schneider, D.; Schober, F.; Grohmann, P.; Hammerle, C.H.; Jung, R.E. In-vitro evaluation of the tolerance of surgical instruments in templates for computer-assisted guided implantology produced by 3-D printing. Clin. Oral Implant. Res. 2015, 26, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Guentsch, A.; Bjork, J.; Saxe, R.; Han, S.; Dentino, A.R. An In-Vitro analysis of the accuracy of different guided surgery systems —They are not all the same. Clin. Oral Implant. Res. 2023, 34, 531–541. [Google Scholar] [CrossRef]
- Raabe, C.; Schuetz, T.S.; Chappuis, V.; Yilmaz, B.; Abou-Ayash, S.; Couso-Queiruga, E. Accuracy of keyless vs drill-key implant systems for static computer-assisted implant surgery using two guide-hole designs compared to freehand implant placement: An in vitro study. Int. J. Implant. Dent. 2023, 9, 4. [Google Scholar] [CrossRef]
- Sittikornpaiboon, P.; Arunjaroensuk, S.; Kaboosaya, B.; Subbalekha, K.; Mattheos, N.; Pimkhaokham, A. Comparison of the accuracy of implant placement using different drilling systems for static computer-assisted implant surgery: A simulation-based experimental study. Clin. Implant. Dent. Relat. Res. 2021, 23, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Gourdache, I.; Salomó-Coll, O.; Hernández-Alfaro, F.; Gargallo-Albiol, J. Dental Implant Positioning Accuracy Using a Key or Keyless Static Fully Guided Surgical System: A Prospective Systematic Review and Meta-analysis. Int. J. Prosthodont. 2024, 37, 199–209. [Google Scholar] [CrossRef] [PubMed]
- El Kholy, K.; Janner, S.F.M.; Schimmel, M.; Buser, D. The influence of guided sleeve height, drilling distance, and drilling key length on the accuracy of static Computer-Assisted Implant Surgery. Clin. Implant. Dent. Relat. Res. 2019, 21, 101–107. [Google Scholar] [CrossRef]
- ISO 5725-1:2023(en); Accuracy (Trueness and Precision) of Measurement Methods and Results—Part 1: General Principles and Definitions. International Organization for Standardization: Geneva, Switzerland, 2023.
- Krithikadatta, J.; Gopikrishna, V.; Datta, M. CRIS Guidelines (Checklist for Reporting In-vitro Studies): A concept note on the need for standardized guidelines for improving quality and transparency in reporting in-vitro studies in experimental dental research. J. Conserv. Dent. 2014, 17, 301–304. [Google Scholar] [CrossRef]
- Gargallo-Albiol, J.; Zilleruelo-Pozo, M.J.; Lucas-Taulé, E.; Muñoz-Peñalver, J.; Paternostro-Betancourt, D.; Hernandez-Alfaro, F. Accuracy of static fully guided implant placement in the posterior area of partially edentulous jaws: A cohort prospective study. Clin. Oral Investig. 2022, 26, 2783–2791. [Google Scholar] [CrossRef]
- Tahmaseb, A.; Wu, V.; Wismeijer, D.; Coucke, W.; Evans, C. The accuracy of static computer-aided implant surgery: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29 (Suppl. S16), 416–435. [Google Scholar] [CrossRef]
- Bover-Ramos, F.; Vina-Almunia, J.; Cervera-Ballester, J.; Penarrocha-Diago, M.; Garcia-Mira, B. Accuracy of implant placement with computer-guided surgery: A systematic review and meta-analysis comparing cadaver, clinical, and in vitro studies. Int. J. Oral Maxillofac. Implant. 2018, 33, 101–115. [Google Scholar] [CrossRef]
- Kessler, A.; Le, V.; Folwaczny, M. Influence of the tooth position, guided sleeve height, supporting length, manufacturing methods, and resin E-modulus on the in vitro accuracy of surgical implant guides in a free-end situation. Clin. Oral Implant. Res. 2021, 32, 1097–1104. [Google Scholar] [CrossRef]
- Cassetta, M.; Di Mambro, A.; Giansanti, M.; Stefanelli, L.V.; Barbato, E. Is it possible to improve the accuracy of implants inserted with a stereolithographic surgical guide by reducing the tolerance between mechanical components? Int. J. Oral Maxillofac. Surg. 2013, 42, 887–890. [Google Scholar] [CrossRef] [PubMed]
- Van Assche, N.; Quirynen, M. Tolerance within a surgical guide. Clin. Oral Implant. Res. 2010, 21, 455–458. [Google Scholar] [CrossRef] [PubMed]
- Dulla, F.A.; Couso-Queiruga, E.; Chappuis, V.; Yilmaz, B.; Abou-Ayash, S.; Raabe, C. Influence of alveolar ridge morphology and guide-hole design on the accuracy of static Computer-Assisted Implant Surgery with two implant macro-designs: An In Vitro study. J. Dent. 2023, 130, 104426. [Google Scholar] [CrossRef]
- Adams, C.R.; Ammoun, R.; Deeb, G.R.; Bencharit, S. Influence of Metal Guide Sleeves on the Accuracy and Precision of Dental Implant Placement Using Guided Implant Surgery: An In Vitro Study. J. Prosthodont. 2023, 32, 62–70. [Google Scholar] [CrossRef]
- El Kholy, K.; Lazarin, R.; Janner, S.F.M.; Faerber, K.; Buser, R.; Buser, D. Influence of surgical guide support and implant site location on accuracy of static Computer-Assisted Implant Surgery. Clin. Oral Implant. Res. 2019, 30, 1067–1075. [Google Scholar] [CrossRef] [PubMed]
- Pessoa, R.; Siqueira, R.; Li, J.; Saleh, I.; Meneghetti, P.; Bezerra, F.; Wang, H.L.; Mendonça, G. The Impact of Surgical Guide Fixation and Implant Location on Accuracy of Static Computer-Assisted Implant Surgery. J. Prosthodont. 2022, 31, 155–164. [Google Scholar] [CrossRef]
- Wu, Q.; Lou, Y.; Sun, J.; Xie, C.; Wu, J.; Yu, H. Accuracy of the novel digital non-cross-arch surgical guides with integration of tooth undercut retention and screw-bone support for implant placement in mandibular free-end. BMC Oral Health 2024, 24, 550. [Google Scholar] [CrossRef]
- Thanasrisuebwong, P.; Pimkhaokham, A.; Jirajariyavej, B.; Bencharit, S. Influence of the Residual Ridge Widths and Implant Thread Designs on Implant Positioning Using Static Implant Guided Surgery. J. Prosthodont. 2023, 32, 340–346. [Google Scholar] [CrossRef]
- El Kholy, K.; Ebenezer, S.; Wittneben, J.G.; Lazarin, R.; Rousso, D.; Buser, D. Influence of implant macrodesign and insertion connection technology on the accuracy of static computer-assisted implant surgery. Clin. Implant. Dent. Relat. Res. 2019, 21, 1073–1079. [Google Scholar] [CrossRef]
- Kernen, F.; Schlager, S.; Seidel Alvarez, V.; Mehrhof, J.; Vach, K.; Kohal, R.; Nelson, K.; Flügge, T. Accuracy of intraoral scans: An in vivo study of different scanning devices. J. Prosthet. Dent. 2022, 128, 1303–1309. [Google Scholar] [CrossRef] [PubMed]
- Tatakis, D.N.; Chien, H.H.; Parashis, A.O. Guided implant surgery risks and their prevention. Periodontol. 2000 2019, 81, 194–208. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Guiding System | Site of Implantation | Min | Q1 | Median | Q3 | Max | Mean | SD |
|---|---|---|---|---|---|---|---|---|
| 3D Deviation at crest (mm) | ||||||||
| DK | AntExt | 0.11 | 0.32 | 0.37 | 0.51 | 0.79 | 0.41 | 0.17 |
| DK | AntSTG | 0.47 | 0.66 | 0.83 | 0.87 | 0.91 | 0.77 | 0.14 |
| DK | ProPosSTG | 0.53 | 0.58 | 0.72 | 0.79 | 0.90 | 0.70 | 0.13 |
| DK | DisPosSTG | 0.70 | 0.99 | 1.10 | 1.13 | 1.15 | 1.03 | 0.16 |
| DK | ProDE | 0.64 | 0.72 | 0.86 | 0.98 | 1.23 | 0.87 | 0.18 |
| DK | DisDE | 0.51 | 0.62 | 0.77 | 0.89 | 0.94 | 0.75 | 0.15 |
| I KL | AntExt | 0.43 | 0.64 | 0.89 | 1.03 | 1.29 | 0.84 | 0.26 |
| KL | AntSTG | 0.50 | 0.74 | 0.95 | 1.26 | 1.39 | 0.96 | 0.29 |
| KL | ProPosSTG | 0.54 | 0.80 | 0.97 | 1.15 | 1.33 | 0.96 | 0.26 |
| KL | DisPosSTG | 0.52 | 0.68 | 0.84 | 0.95 | 1.02 | 0.80 | 0.17 |
| KL | ProDE | 0.42 | 0.57 | 0.77 | 0.86 | 0.92 | 0.73 | 0.17 |
| KL | DisDE | 0.40 | 0.51 | 0.66 | 0.98 | 1.32 | 0.75 | 0.30 |
| DK | Overall | 0.11 | 0.52 | 0.72 | 0.89 | 1.23 | 0.71 | 0.26 |
| KL | Overall | 0.40 | 0.63 | 0.86 | 0.98 | 1.39 | 0.84 | 0.26 |
| 3D Deviation at apex (mm) | ||||||||
| DK | AntExt | 0.25 | 0.39 | 0.58 | 0.68 | 1.19 | 0.59 | 0.16 |
| DK | AntSTG | 0.61 | 0.79 | 1.13 | 1.26 | 1.43 | 1.07 | 0.27 |
| DK | ProPosSTG | 0.80 | 0.97 | 1.12 | 1.52 | 1.70 | 1.21 | 0.31 |
| DK | DisPosSTG | 1.14 | 1.29 | 1.62 | 1.74 | 2.05 | 1.57 | 0.28 |
| DK | ProDE | 0.70 | 0.80 | 1.09 | 1.22 | 1.51 | 1.05 | 0.26 |
| DK | DisDE | 0.95 | 1.19 | 1.55 | 1.67 | 2.05 | 1.49 | 0.32 |
| KL | AntExt | 0.65 | 1.24 | 1.54 | 1.86 | 2.17 | 1.50 | 0.43 |
| KL | AntSTG | 0.78 | 1.13 | 1.32 | 1.44 | 1.55 | 1.27 | 0.23 |
| KL | ProPosSTG | 0.76 | 1.11 | 1.60 | 1.90 | 2.36 | 1.56 | 0.48 |
| KL | DisPosSTG | 0.72 | 0.85 | 1.05 | 1.22 | 1.30 | 1.03 | 0.21 |
| KL | ProDE | 0.49 | 0.82 | 1.03 | 1.30 | 1.50 | 1.04 | 0.31 |
| KL | DisDE | 0.41 | 0.92 | 1.05 | 1.34 | 1.51 | 1.06 | 0.31 |
| DK | Overall | 0.25 | 0.70 | 1.13 | 1.45 | 2.05 | 1.08 | 0.45 |
| KL | Overall | 0.41 | 0.98 | 1.26 | 1.52 | 2.36 | 1.28 | 0.41 |
| Angular deviation (°) | ||||||||
| DK | AntExt | 0.24 | 1.12 | 1.52 | 2.11 | 3.47 | 1.02 | 0.73 |
| DK | AntSTG | 1.19 | 2.13 | 2.63 | 3.41 | 4.15 | 2.69 | 0.89 |
| DK | ProPosSTG | 1.96 | 2.59 | 3.52 | 4.96 | 5.20 | 3.56 | 1.18 |
| DK | DisPosSTG | 4.63 | 5.03 | 6.06 | 6.49 | 7.78 | 5.92 | 0.98 |
| DK | ProDE | 0.54 | 1.37 | 1.79 | 2.60 | 4.11 | 2.02 | 1.06 |
| DK | DisDE | 2.34 | 3.09 | 4.23 | 4.75 | 5.46 | 3.99 | 1.04 |
| KL | AntExt | 1.72 | 3.70 | 4.33 | 5.44 | 5.88 | 4.37 | 1.10 |
| KL | AntSTG | 1.29 | 2.25 | 2.72 | 3.18 | 3.58 | 2.65 | 0.67 |
| KL | ProPosSTG | 1.45 | 2.91 | 4.68 | 5.44 | 7.02 | 4.26 | 1.71 |
| KL | DisPosSTG | 1.55 | 1.88 | 2.36 | 3.30 | 4.28 | 2.56 | 0.87 |
| KL | ProDE | 1.56 | 1.81 | 2.64 | 4.22 | 5.43 | 2.97 | 1.32 |
| KL | DisDE | 0.36 | 1.59 | 2.63 | 3.41 | 4.16 | 2.43 | 1.24 |
| DK | Overall | 0.24 | 1.69 | 2.58 | 4.33 | 7.78 | 3.06 | 1.72 |
| KL | Overall | 0.36 | 2.25 | 3.22 | 4.41 | 7.02 | 3.37 | 1.43 |
| Vertical linear deviation (mm) | ||||||||
| DK | AntExt | 0.00 | 0.06 | 0.17 | 0.34 | 0.49 | 0.20 | 0.16 |
| DK | AntSTG | 0.40 | 0.55 | 0.62 | 0.73 | 0.82 | 0.62 | 0.12 |
| DK | ProPosSTG | 0.33 | 0.37 | 0.42 | 0.55 | 0.76 | 0.46 | 0.13 |
| DK | DisPosSTG | 0.67 | 0.89 | 1.01 | 1.04 | 1.07 | 0.95 | 0.15 |
| DK | ProDE | 0.33 | 0.50 | 0.65 | 0.80 | 0.94 | 0.64 | 0.20 |
| DK | DisDE | 0.00 | 0.01 | 0.05 | 0.08 | 0.13 | 0.05 | 0.04 |
| KL | AntExt | 0.00 | 0.18 | 0.29 | 0.39 | 0.57 | 0.29 | 0.15 |
| KL | AntSTG | 0.34 | 0.49 | 0.55 | 1.00 | 1.18 | 0.67 | 0.29 |
| KL | ProPosSTG | 0.08 | 0.38 | 0.53 | 0.63 | 0.75 | 0.48 | 0.22 |
| KL | DisPosSTG | 0.49 | 0.61 | 0.73 | 0.82 | 0.89 | 0.71 | 0.14 |
| KL | ProDE | 0.08 | 0.12 | 0.20 | 0.60 | 0.78 | 0.33 | 0.27 |
| KL | DisDE | 0.02 | 0.17 | 0.33 | 0.62 | 1.32 | 0.43 | 0.38 |
| DK | Overall | 0.00 | 0.13 | 0.45 | 0.67 | 1.07 | 0.45 | 0.33 |
| KL | Overall | 0.00 | 0.24 | 0.46 | 0.62 | 1.32 | 0.46 | 0.29 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kasradze, D.; Kubilius, R. The Influence of Guiding Concept on the Accuracy of Static Computer-Assisted Implant Surgery in Partially Edentulous Cases: An In Vitro Study. Medicina 2025, 61, 617. https://doi.org/10.3390/medicina61040617
Kasradze D, Kubilius R. The Influence of Guiding Concept on the Accuracy of Static Computer-Assisted Implant Surgery in Partially Edentulous Cases: An In Vitro Study. Medicina. 2025; 61(4):617. https://doi.org/10.3390/medicina61040617
Chicago/Turabian StyleKasradze, David, and Ričardas Kubilius. 2025. "The Influence of Guiding Concept on the Accuracy of Static Computer-Assisted Implant Surgery in Partially Edentulous Cases: An In Vitro Study" Medicina 61, no. 4: 617. https://doi.org/10.3390/medicina61040617
APA StyleKasradze, D., & Kubilius, R. (2025). The Influence of Guiding Concept on the Accuracy of Static Computer-Assisted Implant Surgery in Partially Edentulous Cases: An In Vitro Study. Medicina, 61(4), 617. https://doi.org/10.3390/medicina61040617