
Effectiveness of the Cooled Radiofrequency Ablation of Genicular Nerves in Patients with Chronic Knee Pain Due to Osteoarthritis: A Double-Blind, Randomized, Controlled Study


Abstract
1. Introduction
2. Materials and Methods
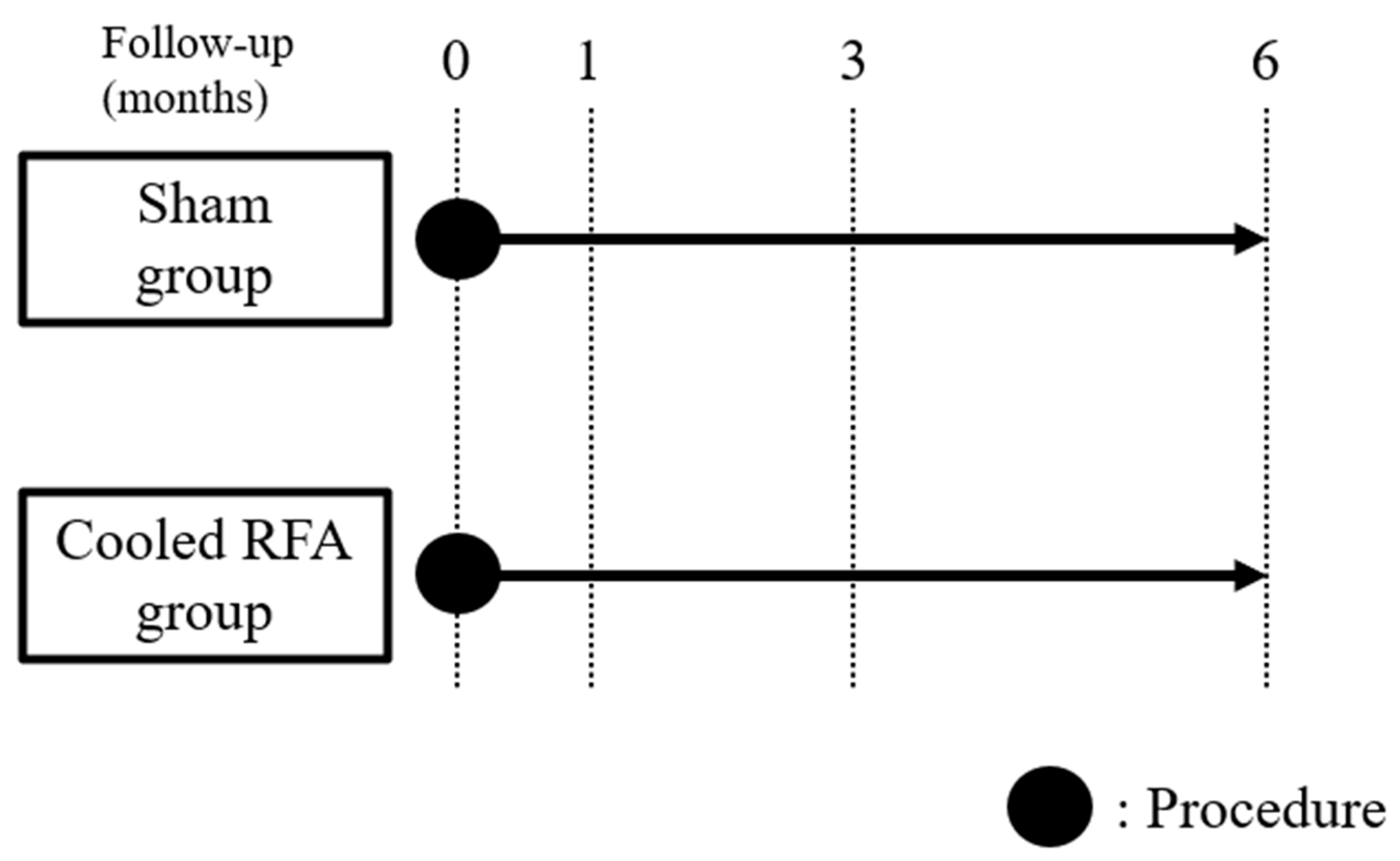
2.1. Study Design and Participants
2.2. Participants
2.3. Randomization and Blinding
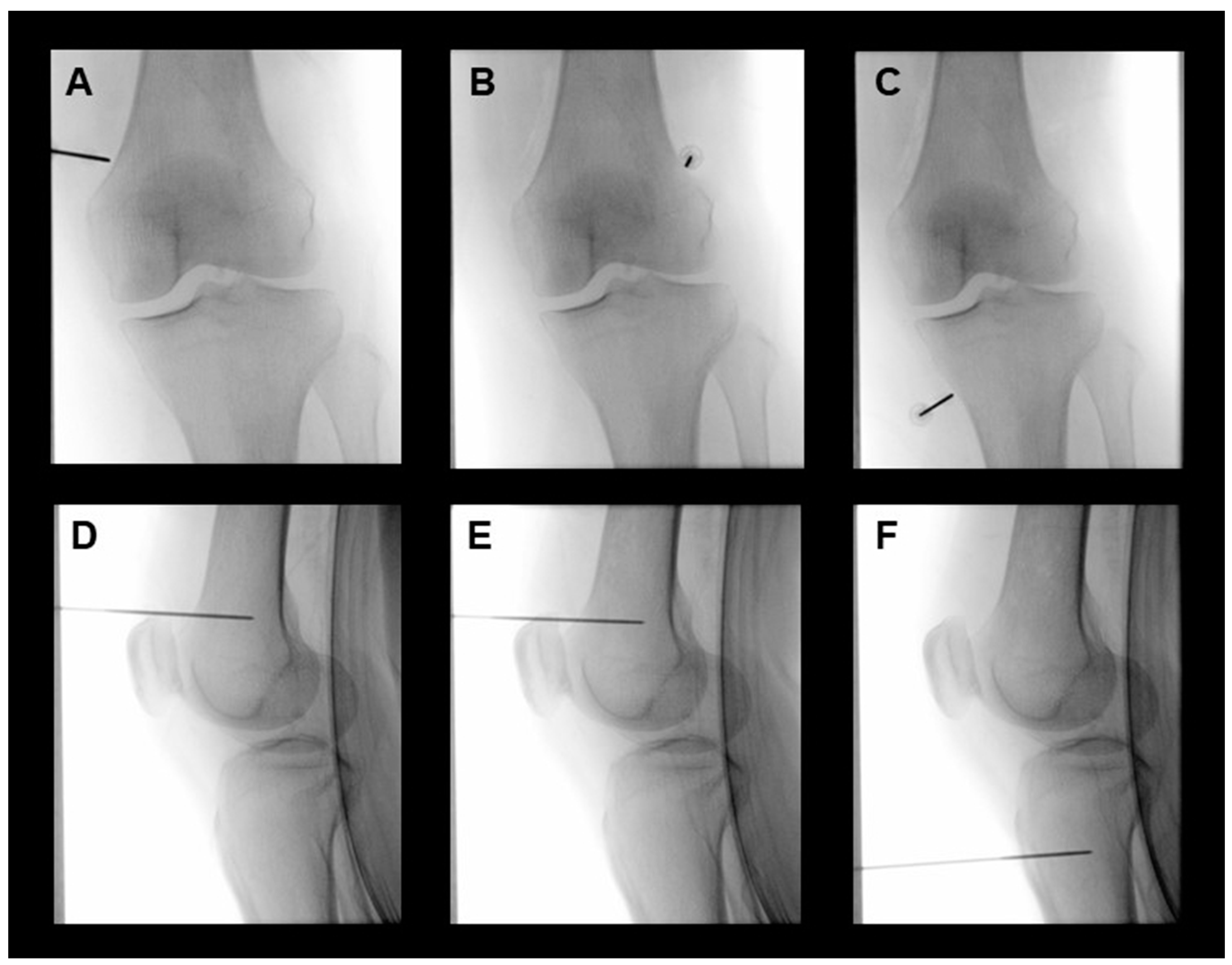
2.4. Intervention
2.5. Outcome Measures and Data Collection
2.6. Statistical Analysis
3. Results
3.1. Study Population
3.2. Primary and Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sharma, L. Osteoarthritis of the Knee. N. Engl. J. Med. 2021, 384, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, U.S.; Zhang, Y.; Zhu, Y.; Niu, J.; Zhang, B.; Felson, D.T. Increasing prevalence of knee pain and symptomatic knee osteoarthritis: Survey and cohort data. Ann. Intern. Med. 2011, 155, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Vanneste, T.; Belba, A.; Kallewaard, J.W.; van Kuijk, S.M.J.; Gelissen, M.; Emans, P.; Bellemans, J.; Smeets, K.; Terwiel, C.; Van Boxem, K.; et al. Comparison of cooled versus conventional radiofrequency treatment of the genicular nerves for chronic knee pain: A multicenter non-inferiority randomized pilot trial (COCOGEN trial). Reg. Anesth. Pain Med. 2023, 48, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.J.; Hwang, S.J.; Song, J.G.; Leem, J.G.; Kang, Y.U.; Park, P.H.; Shin, J.W. Radiofrequency treatment relieves chronic knee osteoarthritis pain: A double-blind randomized controlled trial. Pain 2011, 152, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Hagedorn, J.M.; Wooster, B.M.; Hunt, C.L.; Moeschler, S.M.; Orhurhu, V.; Trousdale, R.T. Beyond Revision Surgery: Work-Up and Interventional Treatments for the Painful Total Knee Arthroplasty. Pain Pract. 2020, 20, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Kapural, L.; Deering, J.P. A technological overview of cooled radiofrequency ablation and its effectiveness in the management of chronic knee pain. Pain Manag. 2020, 10, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Oladeji, L.O.; Cook, J.L. Cooled Radio Frequency Ablation for the Treatment of Osteoarthritis-Related Knee Pain: Evidence, Indications, and Outcomes. J. Knee Surg. 2019, 32, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Karm, M.-H.; Kwon, H.-J.; Kim, C.-S.; Kim, D.-H.; Shin, J.-W.; Choi, S.-S. Cooled radiofrequency ablation of genicular nerves for knee osteoarthritis. Korean J. Pain 2024, 37, 13–25. [Google Scholar] [CrossRef]
- Kim, D.H.; Choi, S.S.; Yoon, S.H.; Lee, S.H.; Seo, D.K.; Lee, I.G.; Choi, W.J.; Shin, J.W. Ultrasound-Guided Genicular Nerve Block for Knee Osteoarthritis: A Double-Blind, Randomized Controlled Trial of Local Anesthetic Alone or in Combination with Corticosteroid. Pain Physician 2018, 21, 41–51. [Google Scholar]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Gallizzi, M.; Gagnon, C.; Harden, R.N.; Stanos, S.; Khan, A. Medication Quantification Scale Version III: Internal validation of detriment weights using a chronic pain population. Pain Pract. 2008, 8, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.J.; Kim, D.H.; Cho, S.S.; Jeon, B.; Karm, M.H.; Choi, S.S. Comparison of Adjuvant Hypertonic Saline and Normal Saline for Epidural Block in Patients with Postherpetic Neuralgia: A Double-Blind, Randomized Trial. Pain Res. Manag. 2022, 2022, 8081443. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; Turk, D.C.; Wyrwich, K.W.; Beaton, D.; Cleeland, C.S.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Kerns, R.D.; Ader, D.N.; et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J. Pain 2008, 9, 105–121. [Google Scholar] [CrossRef] [PubMed]
- Menzies, R.D.; Hawkins, J.K. Analgesia and Improved Performance in a Patient Treated by Cooled Radiofrequency for Pain and Dysfunction Postbilateral Total Knee Replacement. Pain Pract. 2015, 15, E54–E58. [Google Scholar] [CrossRef] [PubMed]
- Davis, T.; Loudermilk, E.; DePalma, M.; Hunter, C.; Lindley, D.A.; Patel, N.; Choi, D.; Soloman, M.; Gupta, A.; Desai, M.; et al. Twelve-month analgesia and rescue, by cooled radiofrequency ablation treatment of osteoarthritic knee pain: Results from a prospective, multicenter, randomized, cross-over trial. Reg. Anesth. Pain Med. 2019, 44, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Caragea, M.; Woodworth, T.; Curtis, T.; Blatt, M.; Cheney, C.; Brown, T.; Carson, D.; Kuo, K.T.; Randall, D.; Huang, E.Y.; et al. Genicular Nerve Radiofrequency Ablation for the Treatment of Chronic Knee Joint Pain: A Real-world Cohort Study with Evaluation of Prognostic Factors. Pain Med. 2023, 24, 1332–1340. [Google Scholar] [CrossRef] [PubMed]
- Davis, T.; Loudermilk, E.; DePalma, M.; Hunter, C.; Lindley, D.; Patel, N.; Choi, D.; Soloman, M.; Gupta, A.; Desai, M.; et al. Prospective, Multicenter, Randomized, Crossover Clinical Trial Comparing the Safety and Effectiveness of Cooled Radiofrequency Ablation with Corticosteroid Injection in the Management of Knee Pain From Osteoarthritis. Reg. Anesth. Pain Med. 2018, 43, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.F.; Khalouf, F.; Zora, K.; DePalma, M.; Kohan, L.; Guirguis, M.; Beall, D.; Loudermilk, E.; Pingree, M.; Badiola, I.; et al. Cooled Radiofrequency Ablation Compared with a Single Injection of Hyaluronic Acid for Chronic Knee Pain A Multicenter, Randomized Clinical Trial Demonstrating Greater Efficacy and Equivalent Safety for Cooled Radiofrequency Ablation. J. Bone Jt. Surg. Am. Vol. 2020, 102, 1501–1510. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.P.; Grits, D.; Foorsov, V.; Xu, J.J.; Tankha, P.; Bolash, R.B. Cooled and traditional thermal radiofrequency ablation of genicular nerves in patients with chronic knee pain: A comparative outcomes analysis. Reg. Anesth. Pain Med. 2022, 47, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Kapural, L.; Minerali, A.; Sanders, M.; Matea, M.; Dua, S. Cooled Radiofrequency Ablation Provides Prolonged Pain Relief Compared to Traditional Radiofrequency Ablation: A Real-World, Large Retrospective Clinical Comparison from a Single Practice. J. Pain Res. 2022, 15, 2577–2586. [Google Scholar] [CrossRef]
- Tuttle, A.H.; Tohyama, S.; Ramsay, T.; Kimmelman, J.; Schweinhardt, P.; Bennett, G.J.; Mogil, J.S. Increasing placebo responses over time in U.S. clinical trials of neuropathic pain. Pain 2015, 156, 2616–2626. [Google Scholar] [CrossRef] [PubMed]
- Kapural, L.; Mekhail, N. Radiofrequency ablation for chronic pain control. Curr. Pain Headache Rep. 2001, 5, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Pritzlaff, S.; Jung, M.J.; Ghosh, P.; Hagedorn, J.M.; Tate, J.; Scarfo, K.; Strand, N.; Chakravarthy, K.; Sayed, D.; et al. Latest Evidence-Based Application for Radiofrequency Neurotomy (LEARN): Best Practice Guidelines from the American Society of Pain and Neuroscience (ASPN). J. Pain Res. 2021, 14, 2807–2831. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Huettner, D.P.; Dukewich, M. Comparative Effectiveness Review of Cooled Versus Pulsed Radiofrequency Ablation for the Treatment of Knee Osteoarthritis: A Systematic Review. Pain Physician 2017, 20, 155–171. [Google Scholar] [CrossRef] [PubMed]
- Tran, J.; Peng, P.W.H.; Lam, K.; Baig, E.; Agur, A.M.R.; Gofeld, M. Anatomical Study of the Innervation of Anterior Knee Joint Capsule: Implication for Image-Guided Intervention. Reg. Anesth. Pain Med. 2018, 43, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Conger, A.; Cushman, D.M.; Walker, K.; Petersen, R.; Walega, D.R.; Kendall, R.; McCormick, Z.L. A Novel Technical Protocol for Improved Capture of the Genicular Nerves by Radiofrequency Ablation. Pain Med. 2019, 20, 2208–2212. [Google Scholar] [CrossRef]
- McCormick, Z.L.; Cohen, S.P.; Walega, D.R.; Kohan, L. Technical considerations for genicular nerve radiofrequency ablation: Optimizing outcomes. Reg. Anesth. Pain Med. 2021, 46, 518–523. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Sham (n = 20) | Cooled RFA (n = 20) | p Value |
|---|---|---|---|
| Age (years) | 71.9 ± 6.0 | 69.1 ± 11.8 | 0.354 |
| Sex | 0.716 | ||
| Male | 4 (20%) | 6 (30%) | |
| Female | 16 (80%) | 14 (70%) | |
| Height (cm) | 157.2 ± 6.5 | 156.7 ± 7.6 | 0.824 |
| Weight (kg) | 66.2 ± 11.3 | 62.4 ± 8.6 | 0.243 |
| BMI (kg/m2) | 26.7 ± 4.0 | 25.4 ± 3.3 | 0.271 |
| Hypertension | 8 (40%) | 6 (30%) | 0.741 |
| Diabetes | 4 (20%) | 7 (35%) | 0.480 |
| PHQ-9 | 3.5 (1.5–13.5) | 3.5 (1.5–10.5) | 0.883 |
| Target knee | 0.205 | ||
| Right | 7 (35%) | 12 (60%) | |
| Left | 13 (65%) | 8 (40%) | |
| Pain intensity (NRS) | 6.3 ± 1.6 | 6.8 ± 1.6 | 0.283 |
| WOMAC | 56.2 ± 20.4 | 55.6 ± 21.1 | 0.922 |
| MQS | 4.6 (0.0–8.0) | 3.9 (0.0–7.6) | 0.638 |
| Responder * | Sham (n = 18) | Cooled RFA (n = 17) | p Value |
|---|---|---|---|
| 1 month | 7 (38.9%) | 13 (76.5%) | 0.041 |
| 3 months | 6 (33.3%) | 13 (76.5%) | 0.018 |
| 6 months | 5 (27.8%) | 13 (76.5%) | 0.007 |
| Variables | Time | Mean (95% CI) | Difference (95% CI) | p Value | |
|---|---|---|---|---|---|
| Sham | Cooled RFA | ||||
| Pain (NRS) | Baseline | 6.3 (5.6–7.1) | 6.9 (6.0–7.8) | −0.5 (−1.7 to 0.6) | 0.327 |
| 1 month | 3.9 (2.8–5.1) ** | 3.7 (2.8–4.6) *** | 0.2 (−1.2 to 1.6) | 0.733 | |
| 3 months | 4.8 (3.7–5.9) | 3.5 (2.7–4.4) *** | 1.2 (−0.1 to 2.6) | 0.063 | |
| 6 months | 4.8 (3.8–5.8) | 3.5 (2.6–4.4) *** | 1.4 (0.1 to 2.7) | 0.041 | |
| WOMAC | Baseline | 55.3 (45.2–65.4) | 59.0 (49.0–69.0) | −3.7 (−17.4 to 9.9) | 0.583 |
| 1 month | 37.6 (26.9–48.3) * | 45.4 (35.1–55.7) | −7.9 (−22.2 to 6.5) | 0.273 | |
| 3 months | 45.4 (36.3–54.5) | 47.6 (39.0–56.3) | −2.3 (−14.4 to 9.9) | 0.707 | |
| 6 months | 41.9 (31.8–52.1) | 49.1 (38.4–59.8) | −7.2 (−21.3 to 7.0) | 0.311 | |
| MQS | Baseline | 4.7 (2.4–7.0) | 5.8 (2.0–9.6) | −1.1 (−5.3 to 3.1) | 0.599 |
| 1 month | 5.0 (2.6–7.4) | 5.3 (1.8–8.8) | −0.3 (−4.3 to 3.7) | 0.889 | |
| 3 months | 5.1 (2.8–7.3) | 4.3 (1.0–7.5) | 0.8 (−3.0 to 4.6) | 0.666 | |
| 6 months | 5.1 (2.8–7.3) | 3.7 (0.8–6.6) | 1.4 (−2.2 to 4.9) | 0.431 | |
| GPES | 1 month | 5.1 (4.4–5.7) | 5.0 (4.2–5.9) | 0.1 (−1.0 to 1.1) | 0.914 |
| 3 months | 5.0 (4.3–5.7) | 5.4 (4.8–5.9) | −0.4 (−1.2 to 0.5) | 0.428 | |
| 6 months | 5.1 (4.3–5.9) | 4.9 (4.1–5.7) | 0.2 (−0.9 to 1.3) | 0.677 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, H.-J.; Kim, C.-S.; Kim, D.-H.; Shin, J.-W.; Choi, D.; Choi, S.-S. Effectiveness of the Cooled Radiofrequency Ablation of Genicular Nerves in Patients with Chronic Knee Pain Due to Osteoarthritis: A Double-Blind, Randomized, Controlled Study. Medicina 2024, 60, 857. https://doi.org/10.3390/medicina60060857
Kwon H-J, Kim C-S, Kim D-H, Shin J-W, Choi D, Choi S-S. Effectiveness of the Cooled Radiofrequency Ablation of Genicular Nerves in Patients with Chronic Knee Pain Due to Osteoarthritis: A Double-Blind, Randomized, Controlled Study. Medicina. 2024; 60(6):857. https://doi.org/10.3390/medicina60060857
Chicago/Turabian StyleKwon, Hyun-Jung, Chan-Sik Kim, Doo-Hwan Kim, Jin-Woo Shin, Daeyun Choi, and Seong-Soo Choi. 2024. "Effectiveness of the Cooled Radiofrequency Ablation of Genicular Nerves in Patients with Chronic Knee Pain Due to Osteoarthritis: A Double-Blind, Randomized, Controlled Study" Medicina 60, no. 6: 857. https://doi.org/10.3390/medicina60060857
APA StyleKwon, H.-J., Kim, C.-S., Kim, D.-H., Shin, J.-W., Choi, D., & Choi, S.-S. (2024). Effectiveness of the Cooled Radiofrequency Ablation of Genicular Nerves in Patients with Chronic Knee Pain Due to Osteoarthritis: A Double-Blind, Randomized, Controlled Study. Medicina, 60(6), 857. https://doi.org/10.3390/medicina60060857