
The Association of Acetabulum Fracture and Mechanism of Injury with BMI, Days Spent in Hospital, Blood Loss, and Surgery Time: A Retrospective Analysis of 67 Patients

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. General Characteristics
2.2. Inclusion Criteria
2.3. Ethics
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Morgan, O.; Davenport, D.; Enright, K. Pelvic injury is not just pelvic fracture. BMJ Case Rep. 2019, 12, e232622. [Google Scholar] [CrossRef] [PubMed]
- Dunn, E.L.; Berry, P.H.; Connally, J.D. Computed Tomography of the Pelvis in Patients with Multiple Injuries. J. Trauma Acute Care Surg. 1983, 23, 378. [Google Scholar] [CrossRef]
- Chaumoître, K.; Portier, F.; Petit, P.; Merrot, T.; Guillon, P.O.; Panuel, M. CT imaging of pelvic injuries in polytrauma patients. J. Radiol. 2000, 81, 111–120. [Google Scholar] [PubMed]
- Davis, D.D.; Foris, L.A.; Kane, S.M.; Waseem, M. Pelvic Fracture. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Holstein, J.H.; Culemann, U.; Pohlemann, T. What are Predictors of Mortality in Patients with Pelvic Fractures? Clin. Orthop. Relat. Res. 2012, 470, 2090–2097. [Google Scholar] [CrossRef] [PubMed]
- Kobziff, L. Traumatic pelvic fractures. Orthop. Nurs. 2006, 25, 235–241; quiz 242–243. [Google Scholar] [CrossRef]
- Skitch, S.; Engels, P.T. Acute Management of the Traumatically Injured Pelvis. Emerg. Med. Clin. N. Am. 2018, 36, 161–179. [Google Scholar] [CrossRef]
- Guerado, E.; Medina, A.; Mata, M.I.; Galvan, J.M.; Bertrand, M.L. Protocols for massive blood transfusion: When and why, and potential complications. Eur. J. Trauma Emerg. Surg. 2016, 42, 283–295. [Google Scholar] [CrossRef]
- Coppola, P.T.; Coppola, M. Emergency department evaluation and treatment of pelvic fractures. Emerg. Med. Clin. N. Am. 2000, 18, 1–27. [Google Scholar] [CrossRef]
- Cuthbert, R.; Walters, S.; Ferguson, D.; Karam, E.; Ward, J.; Arshad, H.; Culpan, P.; Bates, P. Epidemiology of pelvic and acetabular fractures across 12-mo at a level-1 trauma centre. World J. Orthop. 2022, 13, 744–752. [Google Scholar] [CrossRef]
- Rondanelli, A.M.; Gómez-Sierra, M.A.; Ossa, A.A.; Hernández, R.D.; Torres, M. Damage control in orthopaedical and traumatology. Colomb. Med. 2021, 52, e4184802. [Google Scholar] [CrossRef]
- Trainham, L.; Rizzolo, D.; Diwan, A.; Lucas, T. Emergency management of high-energy pelvic trauma. JAAPA 2015, 28, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Rommens, P.M. Focus on high energy pelvic trauma. Eur. J. Trauma Emerg. Surg. 2018, 44, 153–154. [Google Scholar] [CrossRef]
- Atif, M.; Hasan, O.; Baloch, N.; Umer, M. A comprehensive basic understanding of pelvis and acetabular fractures after high-energy trauma with associated injuries: Narrative review of targeted literature. J. Pak. Med. Assoc. 2020, 70 (Suppl. S1), S70–S75. [Google Scholar]
- Karunakar, M.A.; Shah, S.N.; Jerabek, S. Body mass index as a predictor of complications after operative treatment of acetabular fractures. J. Bone Jt. Surg. Am. 2005, 87, 1498–1502. [Google Scholar] [CrossRef]
- Abdelrahman, H.; El-Menyar, A.; Keil, H.; Alhammoud, A.; Ghouri, S.I.; Babikir, E.; Asim, M.; Muenzberg, M.; Al-Thani, H. Patterns, management, and outcomes of traumatic pelvic fracture: Insights from a multicenter study. J. Orthop. Surg. Res. 2020, 15, 249. [Google Scholar] [CrossRef] [PubMed]
- Buller, L.T.; Best, M.J.; Quinnan, S.M. A Nationwide Analysis of Pelvic Ring Fractures: Incidence and Trends in Treatment, Length of Stay, and Mortality. Geriatr. Orthop. Surg. Rehabil. 2016, 7, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Aggarwal, S.; Kumar, V.; Patel, S.; Kumar, P. Epidemiology of pelvic fractures in adults: Our experience at a tertiary hospital. Chin. J. Traumatol. 2019, 22, 138–141. [Google Scholar] [CrossRef]
- Magnussen, R.A.; Tressler, M.A.; Obremskey, W.T.; Kregor, P.J. Predicting Blood Loss in Isolated Pelvic and Acetabular High-Energy Trauma. J. Orthop. Trauma 2007, 21, 603–607. [Google Scholar] [CrossRef]
- Frisch, N.; Wessell, N.M.; Charters, M.; Peterson, E.; Cann, B.; Greenstein, A.; Silverton, C.D. Effect of Body Mass Index on Blood Transfusion in Total Hip and Knee Arthroplasty. Orthopedics 2016, 39, e844–e849. [Google Scholar] [CrossRef]
- Cao, G.; Yang, X.; Yue, C.; Tan, H.; Xu, H.; Huang, Z.; Quan, S.; Yang, M.; Pei, F. The effect of body mass index on blood loss and complications in simultaneous bilateral total hip arthroplasty: A multicenter retrospective study. J. Orthop. Surg. 2021, 29, 23094990211061210. [Google Scholar] [CrossRef]
- Cao, G.; Chen, G.; Yang, X.; Huang, Q.; Huang, Z.; Xu, H.; Alexander, P.G.; Zhou, Z.; Pei, F. Obesity does not increase blood loss or incidence of immediate postoperative complications during simultaneous total knee arthroplasty: A multicenter study. Knee 2020, 27, 963–969. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, V.A.; Sambandam, S.; Wukich, D. The Impact of Obesity on Total Hip Arthroplasty Outcomes: A Retrospective Matched Cohort Study. Cureus 2022, 14, e27450. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, V.A.; Sambandam, S.N.; Wukich, D.K. The impact of obesity on total knee arthroplasty outcomes: A retrospective matched cohort study. J. Clin. Orthop. Trauma 2022, 33, 101987. [Google Scholar] [CrossRef]
- Waseem, S.; Lenihan, J.; Davies, B.M.; Rawal, J.; Hull, P.; Carrothers, A.; Chou, D. Low body mass index is associated with increased mortality in patients with pelvic and acetabular fractures. Injury 2021, 52, 2322–2326. [Google Scholar] [CrossRef]
- Sems, S.A.; Johnson, M.; Cole, P.A.; Byrd, C.T.; Templeman, D.C.; Minnesota Orthopaedic Trauma Group. Elevated body mass index increases early complications of surgical treatment of pelvic ring injuries. J. Orthop. Trauma 2010, 24, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Morris, B.J.; Richards, J.E.; Guillamondegui, O.D.; Sweeney, K.R.; Mir, H.R.; Obremskey, W.T.; Kregor, P.J. Obesity Increases Early Complications After High-Energy Pelvic and Acetabular Fractures. Orthopedics 2015, 38, e881–e887. [Google Scholar] [CrossRef]
- Fakru, N.; Faisham, W.; Hadizie, D.; Yahaya, S. Functional Outcome of Surgical Stabilisation of Acetabular Fractures. Malays. Orthop. J. 2021, 15, 129–135. [Google Scholar] [CrossRef]
- Trikha, V.; Ganesh, V.; Cabrera, D.; Bansal, H.; Mittal, S.; Sharma, V. Epidemiological assessment of acetabular fractures in a level one trauma centre: A 7-Year observational study. J. Clin. Orthop. Trauma 2020, 11, 1104–1109. [Google Scholar] [CrossRef]
- Vipulendran, K.; Kelly, J.; Rickman, M.; Chesser, T. Current concepts: Managing acetabular fractures in the elderly population. Eur. J. Orthop. Surg. Traumatol. 2021, 31, 807–816. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
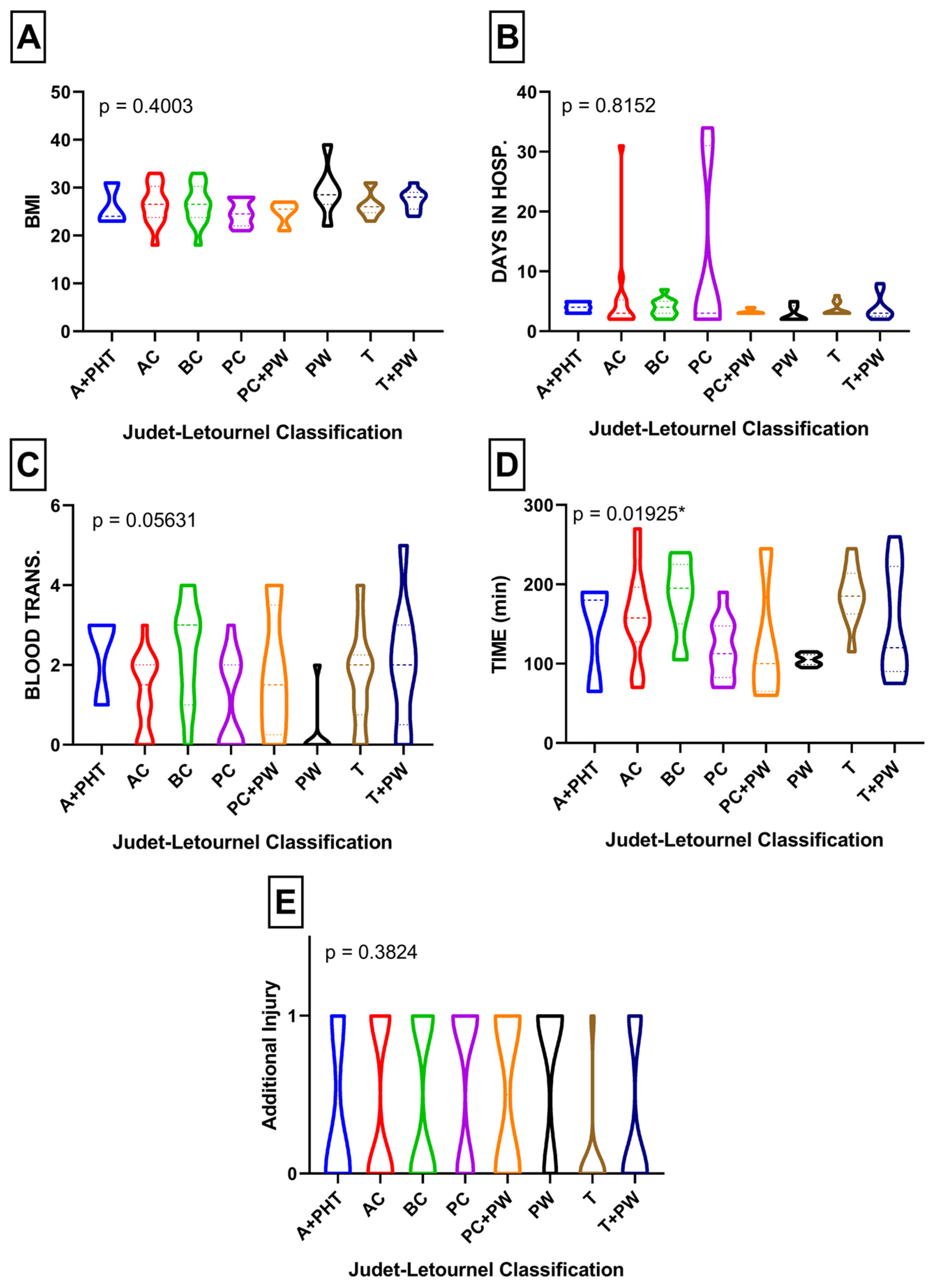
| A + T | AC | BC | PC | PC + W | PW | T | T+P | p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| Mean BMI (kg/cm2) | 26.0 | 26.5 | 26.5 | 24.8 | 24.8 | 29.5 | 26.4 | 27.4 | p = 0.4003 |
| Mean days in hospital (days) | 4.0 | 5.6 | 3.9 | 11.6 | 3.3 | 2.8 | 3.7 | 3.9 | p = 0.8152 |
| Mean blood transfusion (units) | 2.3 | 1.3 | 2.4 | 1.1 | 1.7 | 0.3 | 1.7 | 2.0 | p = 0.0563 |
| Mean time of surgery (minutes) | 145.0 | 159.6 | 183.6 | 119.5 | 126.3 | 105.0 | 186.5 | 152.8 | p = 0.0193 |
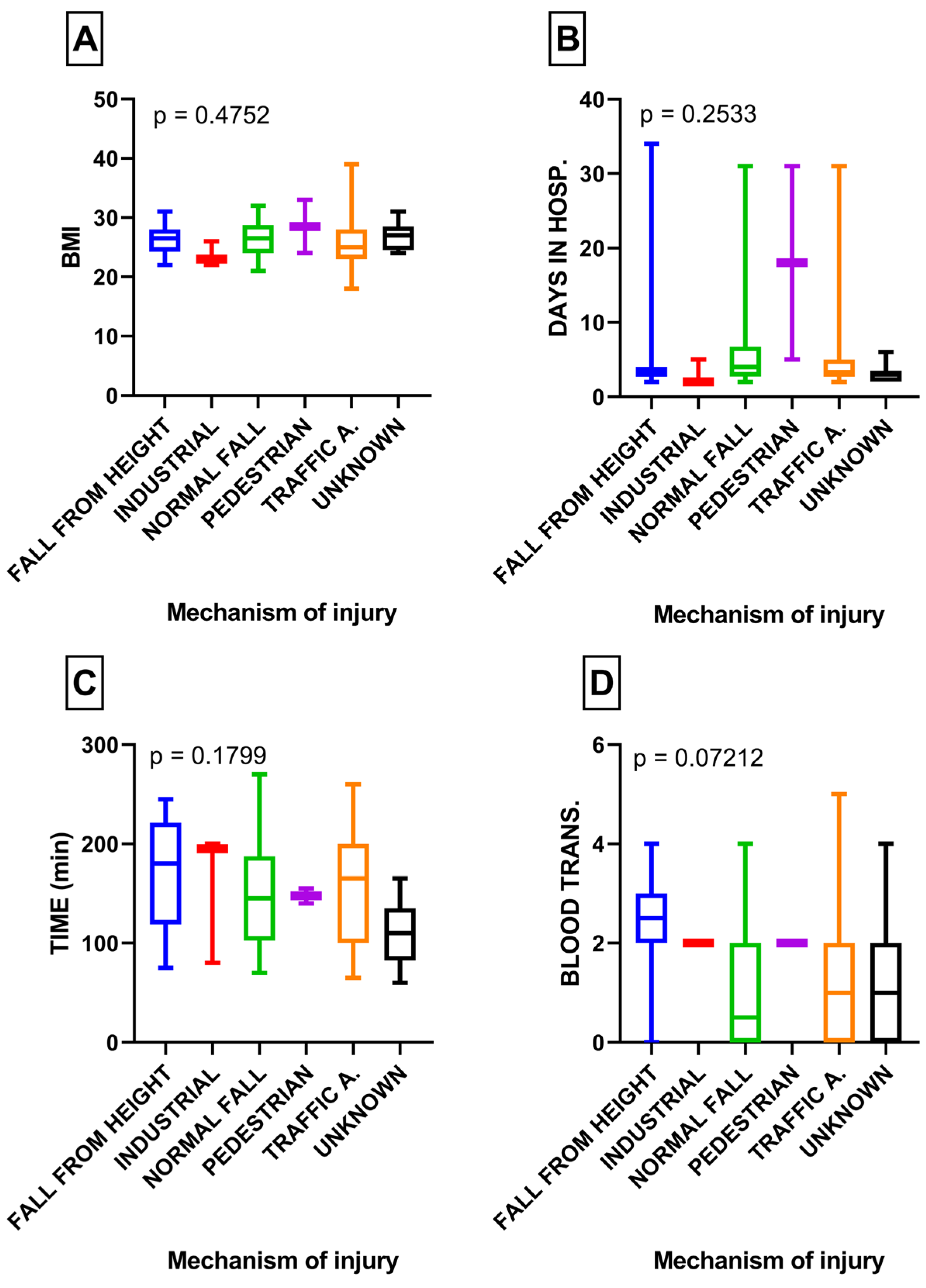
| Fall from Height | Industrial | Fall from Standing Height | Pedestrian | Traffic Accident | Unknown | p-Value | |
|---|---|---|---|---|---|---|---|
| Mean BMI (kg/cm2) | 26.6 | 23.6 | 26.6 | 28.5 | 25.8 | 26.7 | p = 0.4752 |
| Mean days in hospital (days) | 5.2 | 3.0 | 6.9 | 18.0 | 4.7 | 3.1 | p = 0.2533 |
| Mean blood transfusion (units) | 2.3 | 2.0 | 1.1 | 2.0 | 1.37 | 1.2 | p = 0.0721 |
| Mean time of surgery (minutes) | 172.8 | 158.3 | 148.0 | 147.5 | 157.6 | 110.0 | p = 0.1799 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wójcicki, R.; Pielak, T.; Walus, P.M.; Jaworski, Ł.; Małkowski, B.; Jasiewicz, P.; Gagat, M.; Łapaj, Ł.; Zabrzyński, J. The Association of Acetabulum Fracture and Mechanism of Injury with BMI, Days Spent in Hospital, Blood Loss, and Surgery Time: A Retrospective Analysis of 67 Patients. Medicina 2024, 60, 455. https://doi.org/10.3390/medicina60030455
Wójcicki R, Pielak T, Walus PM, Jaworski Ł, Małkowski B, Jasiewicz P, Gagat M, Łapaj Ł, Zabrzyński J. The Association of Acetabulum Fracture and Mechanism of Injury with BMI, Days Spent in Hospital, Blood Loss, and Surgery Time: A Retrospective Analysis of 67 Patients. Medicina. 2024; 60(3):455. https://doi.org/10.3390/medicina60030455
Chicago/Turabian StyleWójcicki, Rafał, Tomasz Pielak, Piotr Marcin Walus, Łukasz Jaworski, Bartłomiej Małkowski, Przemysław Jasiewicz, Maciej Gagat, Łukasz Łapaj, and Jan Zabrzyński. 2024. "The Association of Acetabulum Fracture and Mechanism of Injury with BMI, Days Spent in Hospital, Blood Loss, and Surgery Time: A Retrospective Analysis of 67 Patients" Medicina 60, no. 3: 455. https://doi.org/10.3390/medicina60030455
APA StyleWójcicki, R., Pielak, T., Walus, P. M., Jaworski, Ł., Małkowski, B., Jasiewicz, P., Gagat, M., Łapaj, Ł., & Zabrzyński, J. (2024). The Association of Acetabulum Fracture and Mechanism of Injury with BMI, Days Spent in Hospital, Blood Loss, and Surgery Time: A Retrospective Analysis of 67 Patients. Medicina, 60(3), 455. https://doi.org/10.3390/medicina60030455