
Effective Differences between 2D and 3D Planned Brachytherapy in Lung Cancer: An Institutional Retrospective Study
 ,
,  , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Materials and Methods
- Patients older than 18 years and younger than 85 years.
- Patients with cytologically or histologically confirmed lung cancer of endobronchial localization in the trachea and main bronchi.
- Patients treated with brachytherapy alone or brachytherapy combined with external beam radiotherapy, cytotherapy, or a combination of both, and immunotherapy.
- Patients in whom the disease relapsed in the form of an endobronchial tumor after surgery.
- Patients with severe chronic obstructive pulmonary disease, decompensated cardiomyopathy or malignant arrhythmia, and coagulopathy.
- Patients with ECOG PS 3 or 4.
- Patients with more severe psychiatric diseases in terms of uncooperativeness for performing bronchoscopy.
- Patients with brachytherapy probe displacement.
2.1. Treatment Details
2.2. Statistical Analysis
3. Results
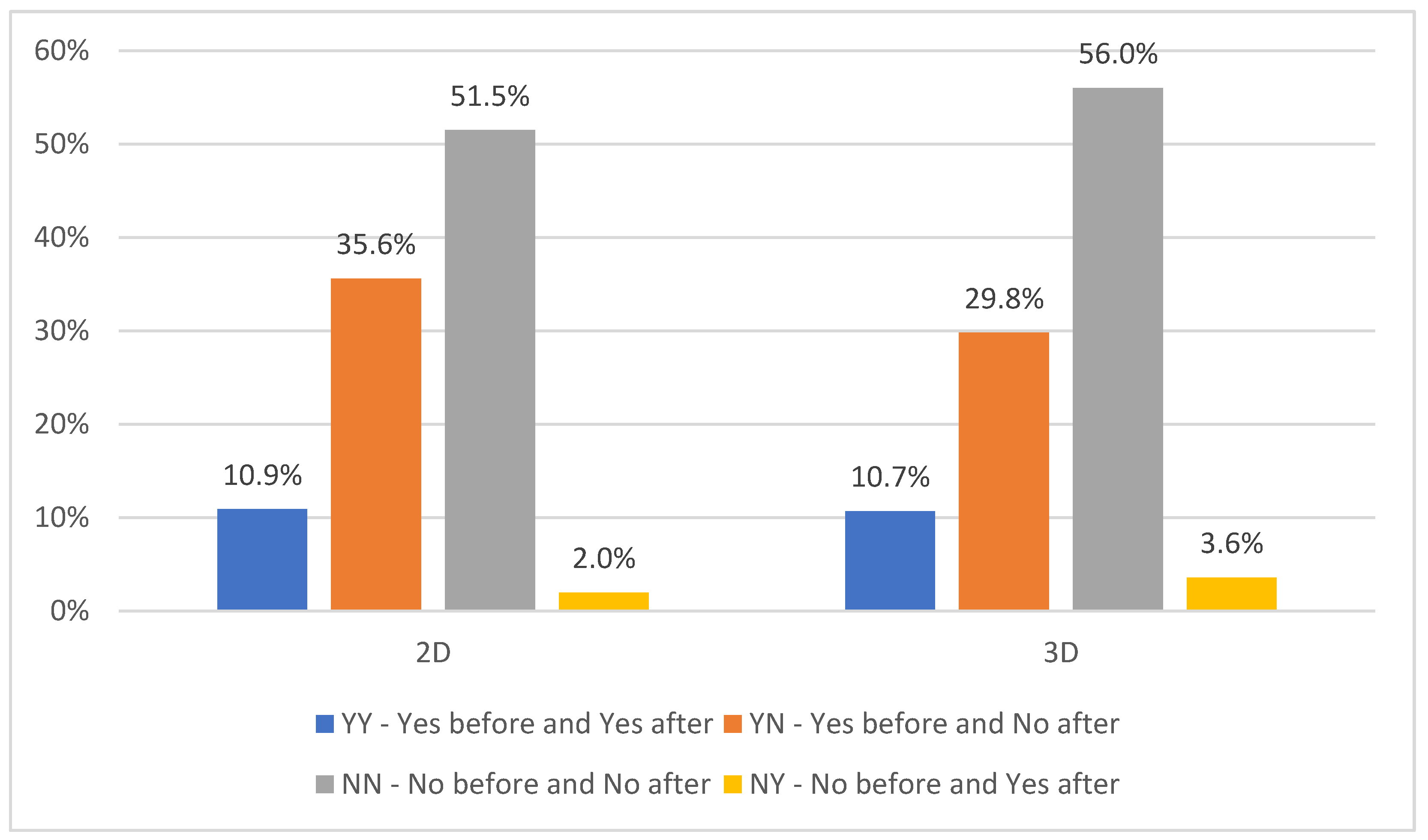
3.1. Palliation Rate and Clinical Response
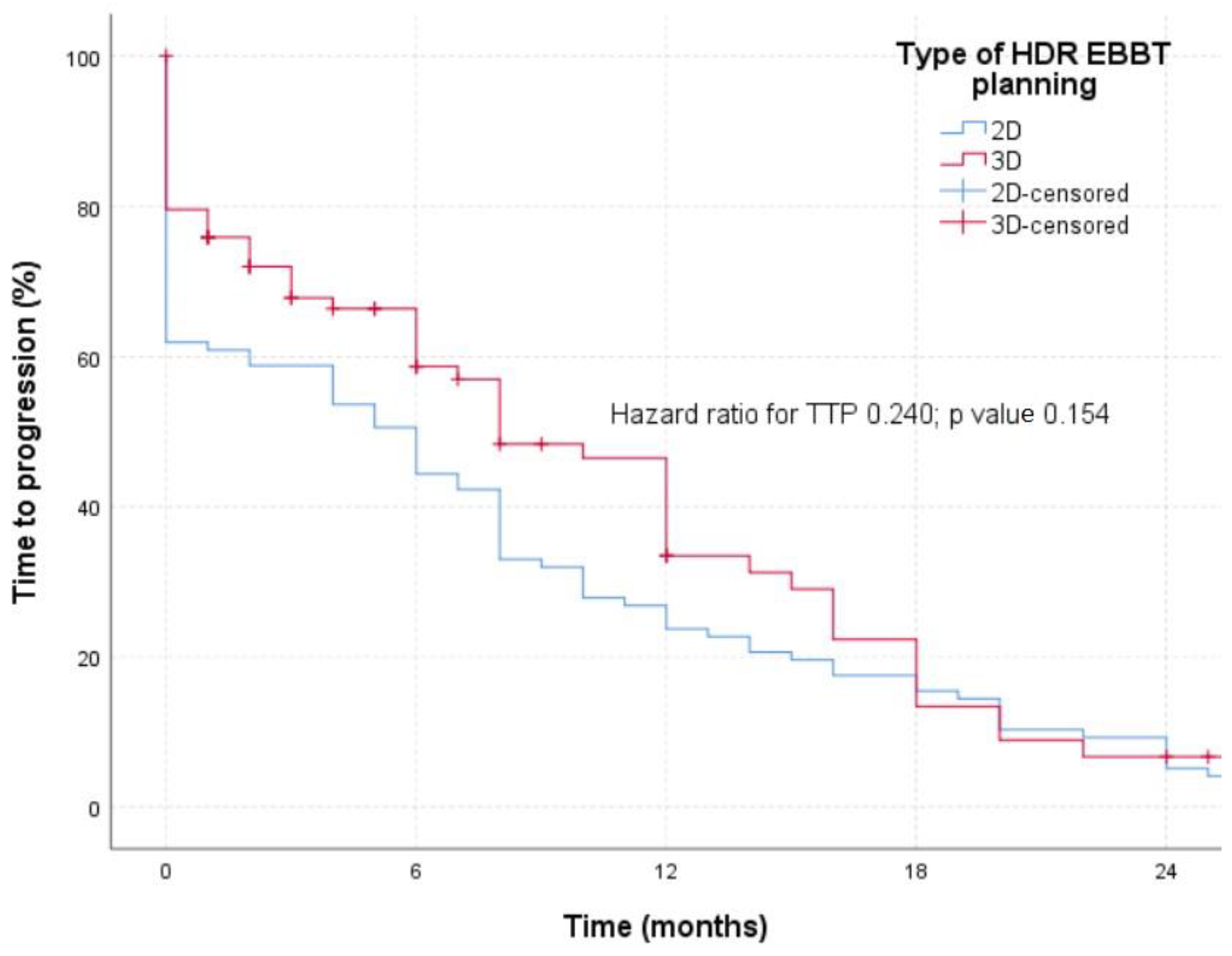
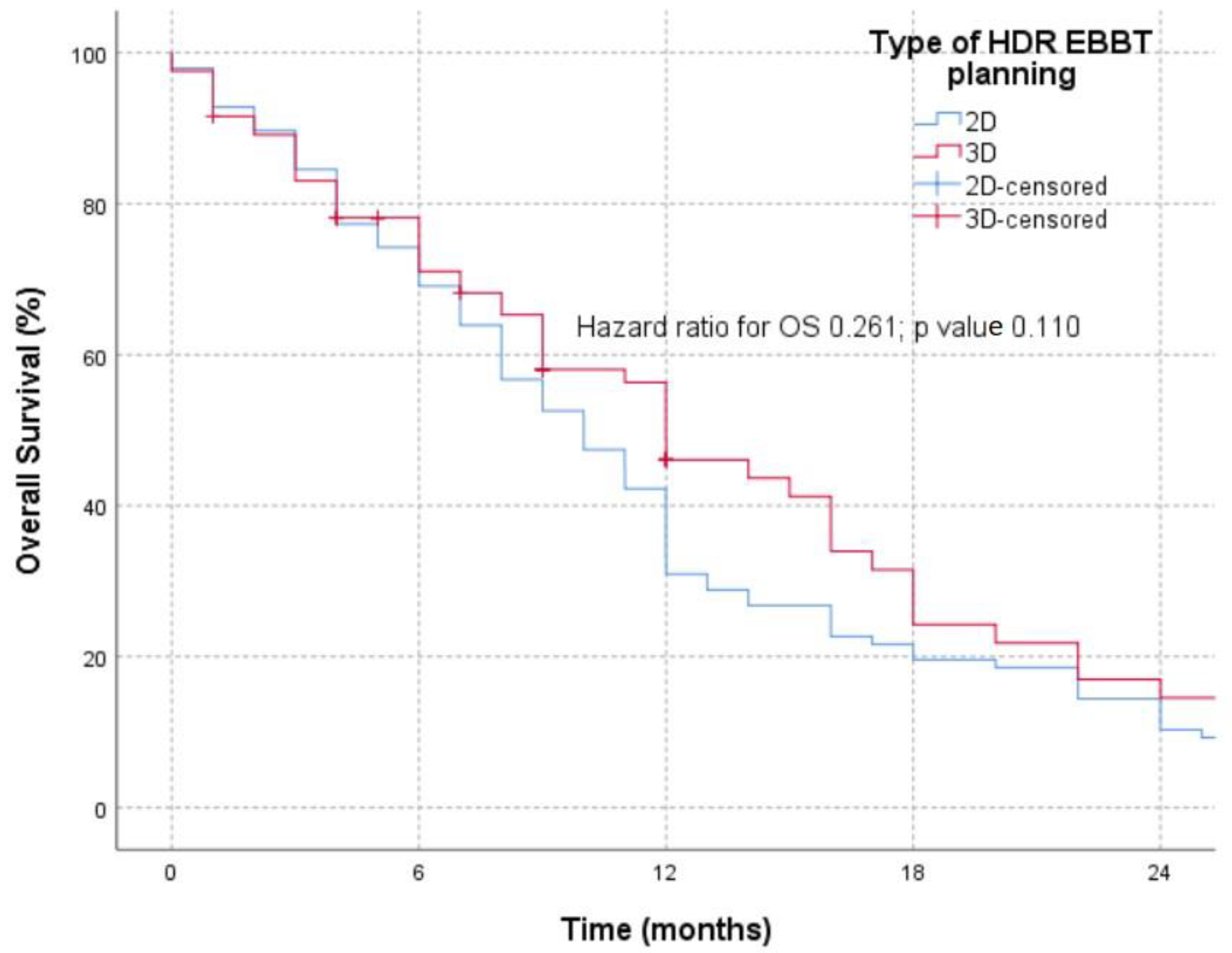
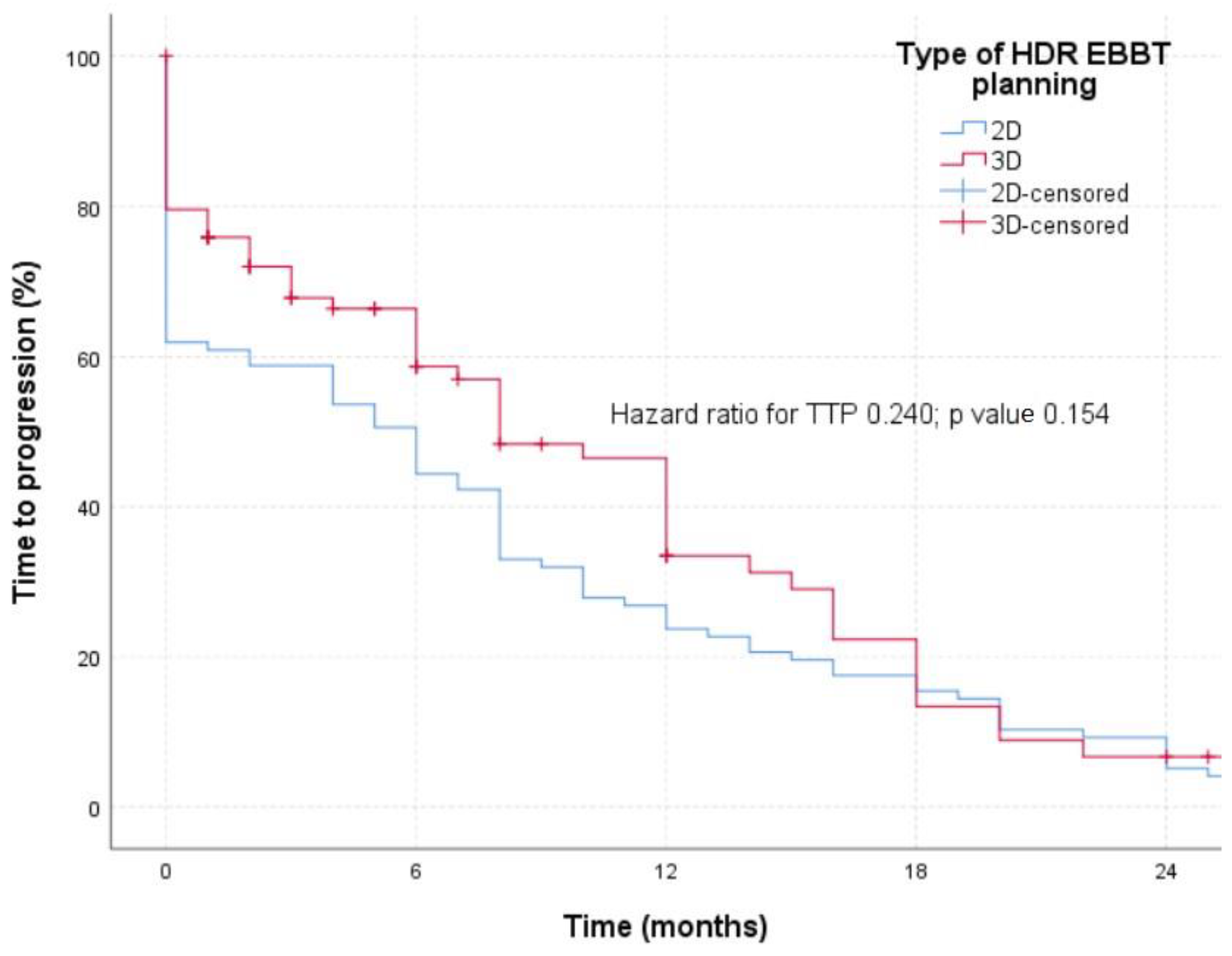
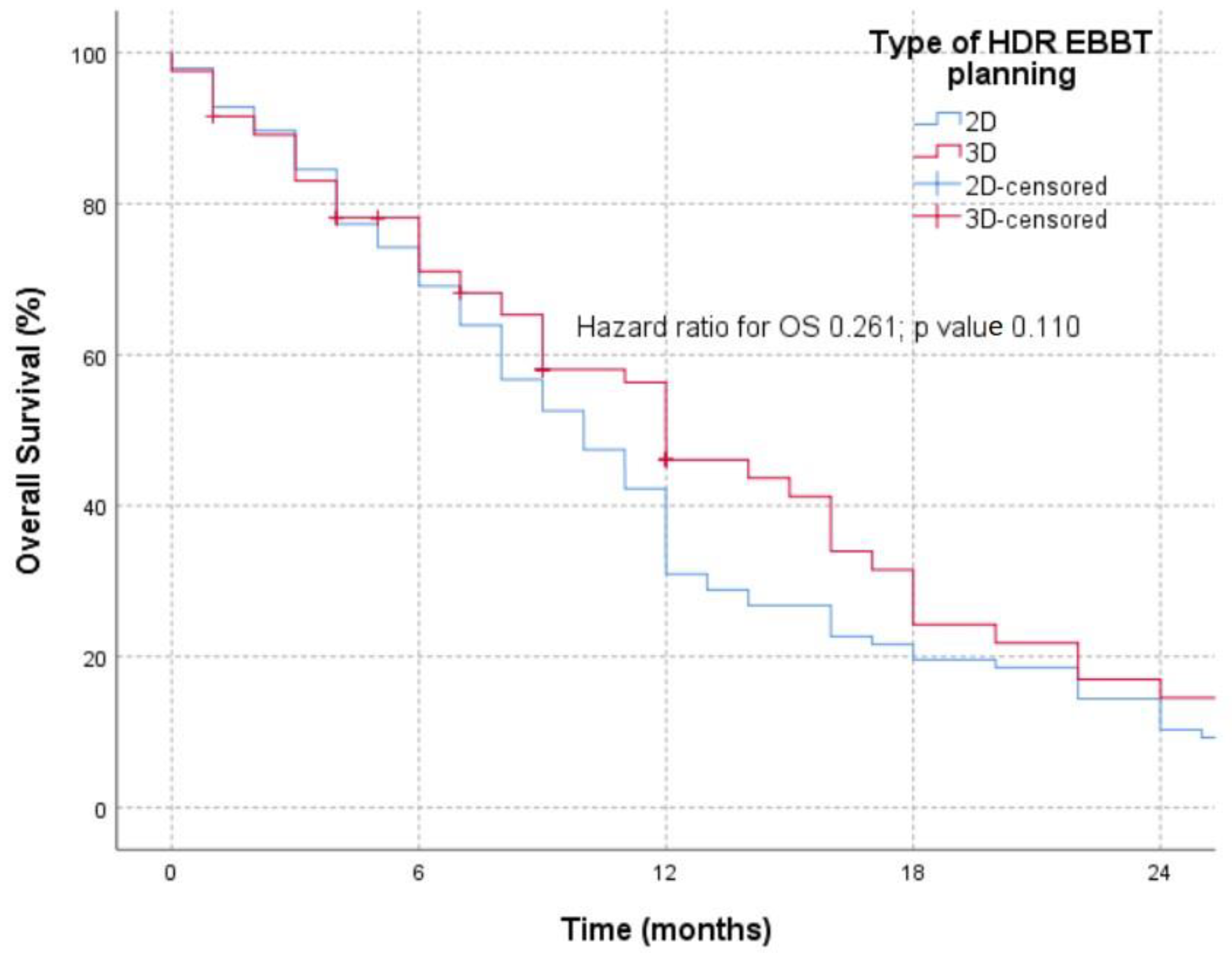
3.2. Time to Progression and Overall Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; DeCamp, M.; et al. NCCN Guidelines® Insights: Non-Small Cell Lung Cancer, Version 2.2023. J. Natl. Compr. Cancer Netw. 2023, 21, 340–350. [Google Scholar] [CrossRef]
- Howlader, N.; Noone, A.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.; et al. SEER Cancer Statistics Review, 1975–2017, National Cancer Institute. Available online: https://seer.cancer.gov/csr/1975_2017/index.html (accessed on 15 February 2024).
- Daneshvar, C.; Falconer, W.E.; Ahmed, M.; Sibly, A.; Hindle, M.; Nicholson, T.W.; Aldik, G.; Telisinghe, L.A.; Riordan, R.D.; Marchbank, A.; et al. Prevalence and Outcome of Central Airway Obstruction in Patients with Lung Cancer. BMJ Open Respir. Res. 2019, 6, e000429. [Google Scholar] [CrossRef] [PubMed]
- Soror, T.; Kovács, G.; Fürschke, V.; Ismail, M.; Badakhshi, H. Salvage Treatment with Sole High-Dose-Rate Endobronchial Interventional Radiotherapy (Brachytherapy) for Isolated Endobronchial Tumor Recurrence in Non-Small-Cell Lung Cancer Patients: A 20-Year Experience. Brachytherapy 2019, 18, 727–732. [Google Scholar] [CrossRef]
- Powers, R.E.; Schwalk, A.J. Overview of Malignant Central Airway Obstruction. Mediastinum 2023, 7, 32. [Google Scholar] [CrossRef]
- Begnaud, A.; Connett, J.E.; Harwood, E.M.; Jantz, M.A.; Mehta, H.J. Measuring Central Airway Obstruction. What Do Bronchoscopists Do? Ann. Am. Thorac. Soc. 2015, 12, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Reveiz, L.; Rueda, J.-R.; Cardona, A.F. Palliative Endobronchial Brachytherapy for Non-Small Cell Lung Cancer. Cochrane Database Syst. Rev. 2012, 12, CD004284. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.Y.; Verma, V.; Li, M.; Zhang, W.; Komaki, R.; Lu, C.; Allen, P.K.; Liao, Z.; Welsh, J.; Lin, S.H.; et al. Proton Beam Radiotherapy and Concurrent Chemotherapy for Unresectable Stage III Non–Small Cell Lung Cancer. JAMA Oncol. 2017, 3, e172032. [Google Scholar] [CrossRef]
- Stewart, A.; Parashar, B.; Patel, M.; O’Farrell, D.; Biagioli, M.; Devlin, P.; Mutyala, S. American Brachytherapy Society Consensus Guidelines for Thoracic Brachytherapy for Lung Cancer. Brachytherapy 2016, 15, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sawicki, M.; Kazalski, D.; Lyczek, J.; Kowalik, L. The Evaluation of Treatment Plans in High-Dose-Rate Endobronchial Brachytherapy by Utilizing 2D and 3D Computed Tomography Imaging Methods. J. Contemp. Brachyther. 2014, 6, 289–292. [Google Scholar] [CrossRef]
- Shepherd, R.W.; Radchenko, C. Bronchoscopic Ablation Techniques in the Management of Lung Cancer. Ann. Transl. Med. 2019, 7, 362. [Google Scholar] [CrossRef]
- Sawicki, M. Treatment Planning in Brachytherapy HDR Based on Three-Dimensional Image. In Computed Tomography—Advanced Applications; Halefoglu, A.M., Ed.; InTech: Vienna, Austria, 2017; ISBN 978-953-51-3367-4. [Google Scholar]
- Bojović, M.; Lalić, N.; Bošković, T.; Ilić, M.; Ivanov, O.; Ličina, J.; Nikolin, B.; Kalember, S. High-Dose-Rate Endobronchial Brachytherapy in the Management of Advanced Lung Cancer—Comparison According to the Presence of Lung Atelectasis. Srp. Arh. Celok. Lek. 2021, 149, 696–701. [Google Scholar] [CrossRef]
- Qiu, B.; Jiang, P.; Ji, Z.; Huo, X.; Sun, H.; Wang, J. Brachytherapy for Lung Cancer. Brachytherapy 2021, 20, 454–466. [Google Scholar] [CrossRef]
- Marić, S.; Trokić, D. Radioterapija tumora pluća. In Radijaciona Onkologija; Medicinski Fakultet, Univerzitet u Banjoj Luci: Banja Luka, Bosnia and Herzegovina, 2020; pp. 236–259. ISBN 978-99976-26-39-4. [Google Scholar]
- Van Limbergen, E.; Skowronek, J.; Pötter, R. The GEC ESTRO Handbook of Brachytherapy. In Part II: Clinical Practice Version; European Society for Radiotherapy and Oncology: Bruxelles, Belgium, 2019; pp. 1–30. [Google Scholar]
- Nasim, F.; Sabath, B.F.; Eapen, G.A. Lung Cancer. Med. Clin. N. Am. 2019, 103, 463–473. [Google Scholar] [CrossRef]
- Scarlata, S.; Fuso, L.; Lucantoni, G.; Varone, F.; Magnini, D.; Antonelli Incalzi, R.; Galluccio, G. The Technique of Endoscopic Airway Tumor Treatment. J. Thorac. Dis. 2017, 9, 2619–2639. [Google Scholar] [CrossRef]
- Halperin, E.C.; Wazer, D.E.; Perez, C.A.; Brady, L.W. (Eds.) Perez and Brady’s Principles and Practice of Radiation Oncology, 7th ed.; Wolters Kluwer: Philadelphia, PA, USA; Baltimore, MD, USA; New York, NY, USA, 2019; ISBN 978-1-4963-8679-3. [Google Scholar]
- Fay, M.; Poole, C.M.; Pratt, G. Recent Advances in Radiotherapy for Thoracic Tumours. J. Thorac. Dis. 2013, 5 (Suppl. S5), S551–S555. [Google Scholar] [CrossRef]
- Mallow, C.; Hayes, M.; Semaan, R.; Smith, T.; Hales, R.; Brower, R.; Yarmus, L. Minimally Invasive Palliative Interventions in Advanced Lung Cancer. Expert Rev. Respir. Med. 2018, 12, 605–614. [Google Scholar] [CrossRef]
- Sawicki, M.; Łyczek, J.; Szutkowski, Z. Analysis of Dose Distribution between Contemporary and Standard Planning in High-Dose-Rate Endobronchial Brachytherapy Based on Three-Dimensional Imaging. J. Contemp. Brachyther. 2019, 11, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Marchioni, A.; Andrisani, D.; Tonelli, R.; Piro, R.; Andreani, A.; Cappiello, G.F.; Meschiari, E.; Dominici, M.; Bavieri, M.; Barbieri, F.; et al. Integrated interventional Bronchoscopy in the Treatment of Locally Advanced Non-Small Lung cancer with Central Malignant Airway Obstructions: A Multicentric REtrospective Study (EVERMORE). Lung Cancer 2020, 148, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Aumont-le Guilcher, M.; Prevost, B.; Sunyach, M.P.; Peiffert, D.; Maingon, P.; Thomas, L.; Williaume, D.; Begue, M.; Lerouge, D.; Campion, L.; et al. High-Dose-Rate Brachytherapy for Non-Small-Cell Lung Carcinoma: A Retrospective Study of 226 Patients. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 1112–1116. [Google Scholar] [CrossRef] [PubMed]
- Zorlu, A.F.; Selek, U.; Emri, S.; Gurkaynak, M.; Akyol, F.H. Second Line Palliative Endobronchial Radiotherapy with HDR Ir 192 in Recurrent Lung Carcinoma. Yonsei Med. J. 2008, 49, 620–624. [Google Scholar] [CrossRef] [PubMed]
- Macías-Lozano, M.J.; Díaz-Díaz, V.; Sayago-Gil, S.; García-Polo, C.; Jaén-Olasolo, J. High Dose Rate Endoluminal Brachytherapy in the Treatment of Endobronchial Lesions—Experience of a Single Institution and Literature Review. Support Care Cancer 2023, 31, 260. [Google Scholar] [CrossRef]
- Xie, X.; Li, X.; Tang, W.; Xie, P.; Tan, X. Primary Tumor Location in Lung Cancer: The Evaluation and Administration. Chin. Med. J. 2021, 135, 127–136. [Google Scholar] [CrossRef]
- Goldberg, M.; Timotin, E.; Farrell, T.; Puksa, S.; Donde, B.; Sur, R. A Prospective Analysis of High-Dose-Rate Endobronchial Brachytherapy in the Palliation of Obstructive Symptoms in Lung Cancer Patients: A Single-Institution Experience. Brachytherapy 2015, 14, 655–661. [Google Scholar] [CrossRef]
- Kniese, C.M.; Musani, A.I. Bronchoscopic Treatment of Inoperable Non-small Cell Lung Cancer. Eur. Respir. Rev. 2020, 29, 200035. [Google Scholar] [CrossRef]
- Youroukou, A.; Gkiozos, I.; Kalaitzi, Z.; Tsalafoutas, I.; Papalla, K.; Charpidou, A.; Kouloulias, V. The Potential Role of Brachytherapy in the Irradiation of Patients with Lung Cancer: A Systematic Review. Clin. Transl. Oncol. 2017, 19, 945–950. [Google Scholar] [CrossRef]
- Skowronek, J. Brachytherapy in the Treatment of Lung Cancer—A Valuable Solution. J. Contemp. Brachyther. 2015, 4, 297–311. [Google Scholar] [CrossRef]
- Mallick, I.; Sharma, S.C.; Behera, D.; Ghoshal, S.; Oinam, A.S. Optimization of Dose and Fractionation of Endobronchial Brachytherapy with or without External Radiation in the Palliative Management of Non-Small Cell Lung Cancer: A Prospective Randomized Study. J. Cancer Res. Ther. 2006, 2, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Speiser, B.L.; Spratling, L. Remote Afterloading Brachytherapy for the Local Control of Endobronchial Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 1993, 25, 579–587. [Google Scholar] [CrossRef]
- Macha, H.N.; Wahlers, B.; Reichle, C.; von Zwehl, D. Endobronchial Radiation Therapy for Obstructing Malignancies: Ten Years’ Experience with Iridium-192 High-Dose Radiation Brachytherapy Afterloading Technique in 365 Patients. Lung 1995, 173, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.F.; Horvath, J.; Peyton, W.; Ling, S.S. High Dose Rate Afterloading Intraluminal Brachytherapy in Malignant Airway Obstruction of Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 1994, 28, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Kohek, P.; Pakisch, B.; Rehak, P. Nd-YAG Laser Debulking Combined with Ir 192 HDR Brachytherapy for Obstructing Cancer of the Central Bronchial Airways: Technique and Results. Activity 1990, (Suppl. S1), 45–47. [Google Scholar]
- Kelly, J.F.; Delclos, M.E.; Morice, R.C.; Huaringa, A.; Allen, P.K.; Komaki, R. High-Dose-Rate Endobronchial Brachytherapy Effectively Palliates Symptoms Due to Airway Tumors: The 10-Year M. D. Anderson Cancer Center Experience. Int. J. Radiat. Oncol. Biol. Phys. 2000, 48, 697–702. [Google Scholar] [CrossRef] [PubMed]
- Polanski, J.; Jankowska-Polanska, B.; Rosinczuk, J.; Chabowski, M.; Szymanska-Chabowska, A. Quality of Life of Patients with Lung Cancer. OncoTargets Ther. 2016, 9, 1023–1028. [Google Scholar] [CrossRef]
- Guarnaschelli, J.N.; Jose, B.O. Palliative High-Dose-Rate Endobronchial Brachytherapy for Recurrent Carcinoma: The University of Louisville Experience. J. Palliat. Med. 2010, 13, 981–989. [Google Scholar] [CrossRef]
- Marsiglia, H.; Baldeyrou, P.; Lartigau, E.; Briot, E.; Haie-Meder, C.; Le Chevalier, T.; Sasso, G.; Gerbaulet, A. High-Dose-Rate Brachytherapy as Sole Modality for Early-Stage Endobronchial Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2000, 47, 665–672. [Google Scholar] [CrossRef]
- Lorchel, F.; Spaeth, D.; Scheid, P.; Aletti, P.; Thariat, J.; Peiffert, D. High dose rate brachytherapy: A potentially curative treatment for small invasive T1N0 endobronchial carcinoma and carcinoma in situ. Rev. Mal. Respir. 2003, 20, 515–520. [Google Scholar]
- Harms, W.; Schraube, P.; Becker, H.; Latz, D.; Herth, F.; Fritz, P.; Wannenmacher, M. Effect and Toxicity of Endoluminal High-Dose-Rate (HDR) Brachytherapy in Centrally Located Tumors of the Upper Respiratory Tract. Strahlenther. Onkol. 2000, 176, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Rochet, N.; Hauswald, H.; Stoiber, E.M.; Hensley, F.W.; Becker, H.D.; Debus, J.; Lindel, K. Primary Radiotherapy with Endobronchial High-Dose-Rate Brachytherapy Boost for Inoperable Lung Cancer: Long-Term Results. Tumori 2013, 99, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Anacak, Y.; Mogulkoc, N.; Ozkok, S.; Goksel, T.; Haydaroglu, A.; Bayindir, U. High Dose Rate Endobronchial Brachytherapy in Combination with External Beam Radiotherapy for Stage III Non-Small Cell Lung Cancer. Lung Cancer 2001, 34, 253–259. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Type of EBBT Planning | |||||
|---|---|---|---|---|---|
| 2D | 3D | ∑ | p Value | ||
| Age | 63.8 (38–85) ± 8.03 | 67.36 (47–85) ± 7.11 | 65.42 (38–85) ± 7.81 | 0.001 a | |
| Gender | Male | 87 (86.1%) | 65 (78.3%) | 152 (82.6%) | 0.163 b |
| Female | 14 (13.9%) | 18 (21.7%) | 32 (17.4%) | ||
| Histological type | SCC | 71 (70.3%) | 56 (63.9%) | 124 (67.4%) | 0.052 c |
| ADC | 17 (16.8%) | 18 (21.7%) | 35 (19%) | ||
| SCLC | 5 (5%) | 1 (1.2%) | 6 (3.3%) | ||
| NSCLC/NOS | 4 (4%) | 2 (2.4%) | 6 (3.3%) | ||
| other | 4 (4%) | 9 (10.8%) | 13 (7.1%) | ||
| TNM | II | 7 (6.9%) | 1 (1.2%) | 8 (4.3%) | 0.004 c |
| IIIA | 16 (15.8%) | 6 (7.2%) | 22 (12%) | ||
| IIIB | 49 (48.5%) | 61 (73.5%) | 110 (59.8%) | ||
| IV | 29 (28.7%) | 15 (18.1%) | 44 (23.9%) | ||
| Other treatments | CTH | 67 (66.3%) | 41 (49.4%) | 108 (58.7%) | 0.024 b |
| EBRT | 49 (49%) | 50 (60.2%) | 99 (54.1%) | 0.139 b | |
| MTH | / | 5 (6%) | 5 (4.7%) | 0.593 c | |
| OP | 3 (3%) | / | 3 (1.6%) | 0.253 c | |
| MMT | 45 (44.6%) | 30 (36.1%) | 75 (40.8%) | 0.292 b | |
| ∑ | 101 (100%) | 83 (100%) | 184 (100%) | ||
| Type of EBBT Planning | |||||
|---|---|---|---|---|---|
| 2D | 3D | ∑ | p-Value | ||
| Location | Trachea | 16 (15.8%) | 13 (15.7%) | 29 (15.8%) | 0.076 c |
| RMB | 26 (25.7%) | 36 (43.4%) | 62 (33.7%) | ||
| IMB | 4 (4%) | 5 (6%) | 9 (4.9%) | ||
| RUB | 5 (5%) | / | 5 (2.7%) | ||
| RMdB | 3 (3%) | 1 (1.2%) | 4 (2.2%) | ||
| RLB | 4 (4%) | 1 (1.2%) | 5 (2.7%) | ||
| LMB | 29 (28.7%) | 23 (27.7%) | 52 (28.3%) | ||
| LUB | 4 (4%) | / | 4 (2.2%) | ||
| LLB | 4 (4%) | 2 (2.4%) | 6 (3.3%) | ||
| BMB | 6 (5.9%) | 2 (2.4%) | 8 (4.3%) | ||
| Number of fractions | I | 5 (5%) | 4 (4.8%) | 9 (4.9%) | 0.179 b |
| II | 95 (94.1%) | 74 (89.2%) | 169 (91.8%) | ||
| IV | 1 (1%) | 5 (6%) | 6 (3.3%) | ||
| Type of EBBT Planning | |||||
|---|---|---|---|---|---|
| 2D | 3D | ∑ | p-Value | ||
| Asymptomatic | YY | 62 (61.4%) | 37 (44.6%) | 53.8% | 0.038 b |
| YN | 38 (37.6%) | 41 (49.4%) | 42.9% | ||
| NN | 1 (1%) | 4 (4.8%) | 2.7% | ||
| NY | / | 1 (1.2%) | 0.5% | ||
| Cough | YY | 49 (48.5%) | 18 (21.4%) | 36.2% | <0.001 b |
| YN | 43 (42.6%) | 39 (46.4%) | 44.3% | ||
| NN | 5 (5%) | 22 (26.2%) | 14.6% | ||
| NY | 4 (4%) | 5 (6%) | 4.9% | ||
| Temperature | YY | 7 (6.9%) | 2 (2.4%) | 4.9% | 0.009 b |
| YN | 16 (15.8%) | 30 (35.7%) | 24.9% | ||
| NN | 72 (71.3%) | 50 (59.5%) | 65.9% | ||
| NY | 6 (5.9%) | 2 (2.4%) | 4.3% | ||
| Dyspnea | YY | 49 (48.5%) | 18 (21.4%) | 36.2% | <0.001 b |
| YN | 38 (37.6%) | 28 (33.3%) | 35.7% | ||
| NN | 13 (12.9%) | 30 (35.7%) | 23.2% | ||
| NY | 1 (1%) | 8 (9.5%) | 4.9% | ||
| Hemoptysis | YY | 5 (5%) | 2 (2.4%) | 3.8% | 0.490 b |
| YN | 15 (14.9%) | 12 (14.3%) | 14.6% | ||
| NN | 75 (74.3%) | 68 (81%) | 77.3% | ||
| NY | 6 (5.9%) | 2 (2.4%) | 4.3% | ||
| ECOG PS | Same | 45 (44.5%) | 34 (40.5%) | 42.7% | 0.847 b |
| Better | 53 (40.5%) | 47 (56%) | 54.1% | ||
| Worse | 3 (3%) | 3 (3.5%) | 3.2% | ||
| 101 (100%) | 84 (100%) | ||||
| Type of EBBT Planning | ||||
|---|---|---|---|---|
| 2D | 3D | ∑ | p Value | |
| Pneumothorax | 2 (2%) | 2 (2.4%) | 4 (2.2%) | 1 c |
| Hemoptisis | 7 (6.9%) | 5 (6%) | 12 (6.5%) | 1 c |
| Infective syndrome | 14 (13.9%) | 10 (12%) | 24 (13%) | 0.716 b |
| Need for PTH AB | 8 (7.9%) | 4 (4.8%) | 12 (6.5%) | 0.551 c |
| Pneumothorax cum drainage | 1 (1%) | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lalić, N.; Bojović, M.; Ivanov, O.; Ličina, J.; Popević, S.; Stjepanović, M.; Bursać, D.; Lalić, I.; Milić, R.; Tomić, S.; et al. Effective Differences between 2D and 3D Planned Brachytherapy in Lung Cancer: An Institutional Retrospective Study. Medicina 2024, 60, 452. https://doi.org/10.3390/medicina60030452
Lalić N, Bojović M, Ivanov O, Ličina J, Popević S, Stjepanović M, Bursać D, Lalić I, Milić R, Tomić S, et al. Effective Differences between 2D and 3D Planned Brachytherapy in Lung Cancer: An Institutional Retrospective Study. Medicina. 2024; 60(3):452. https://doi.org/10.3390/medicina60030452
Chicago/Turabian StyleLalić, Nensi, Marko Bojović, Olivera Ivanov, Jelena Ličina, Spasoje Popević, Mihailo Stjepanović, Daliborka Bursać, Ivica Lalić, Rade Milić, Sanja Tomić, and et al. 2024. "Effective Differences between 2D and 3D Planned Brachytherapy in Lung Cancer: An Institutional Retrospective Study" Medicina 60, no. 3: 452. https://doi.org/10.3390/medicina60030452
APA StyleLalić, N., Bojović, M., Ivanov, O., Ličina, J., Popević, S., Stjepanović, M., Bursać, D., Lalić, I., Milić, R., Tomić, S., Parapid, B., & Anđelković, A. (2024). Effective Differences between 2D and 3D Planned Brachytherapy in Lung Cancer: An Institutional Retrospective Study. Medicina, 60(3), 452. https://doi.org/10.3390/medicina60030452