

Clinical Implications of Ivabradine in the Contemporary Era


Abstract
1. Introduction: How Heart Rate Modulation Is Important
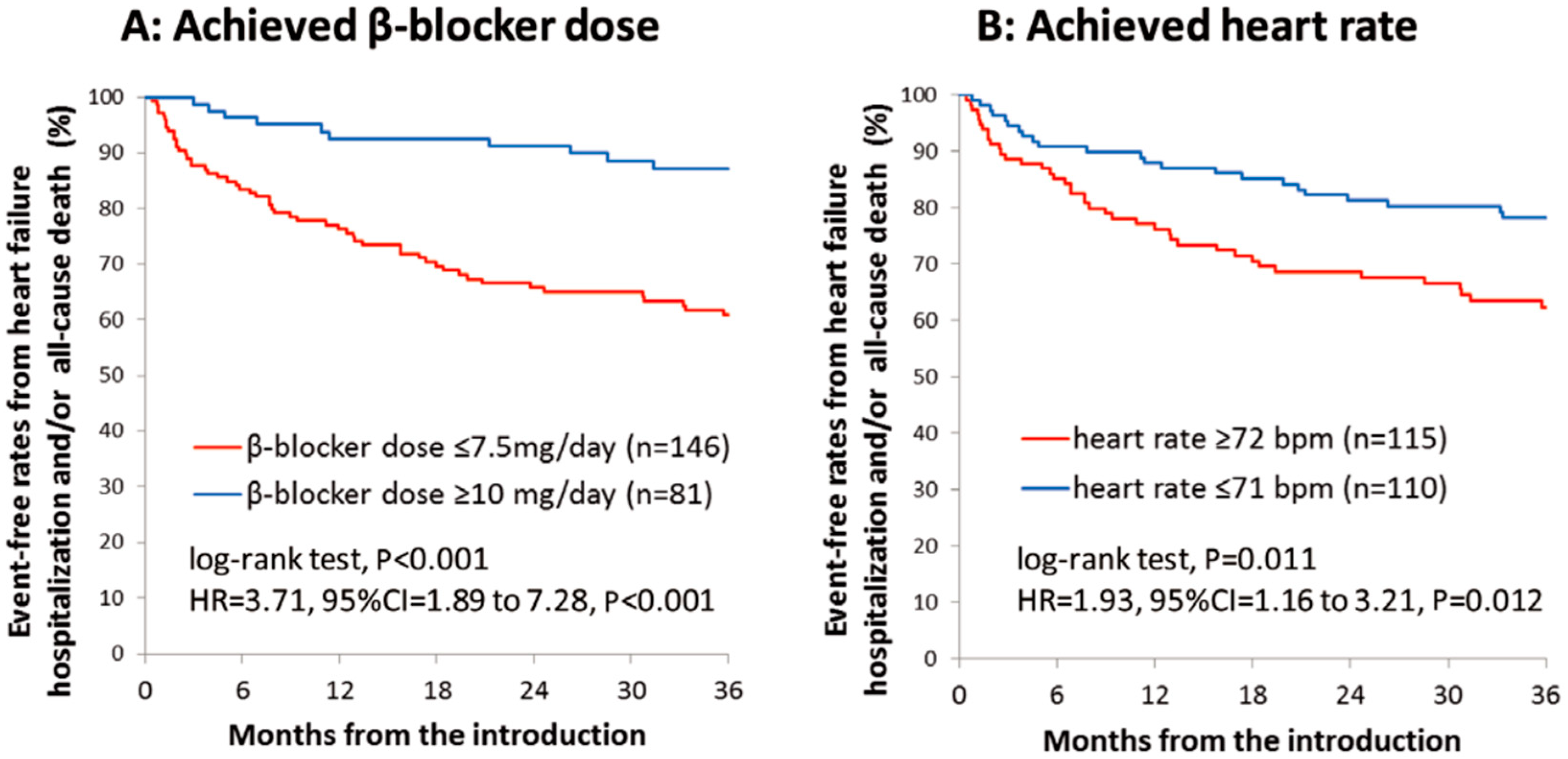
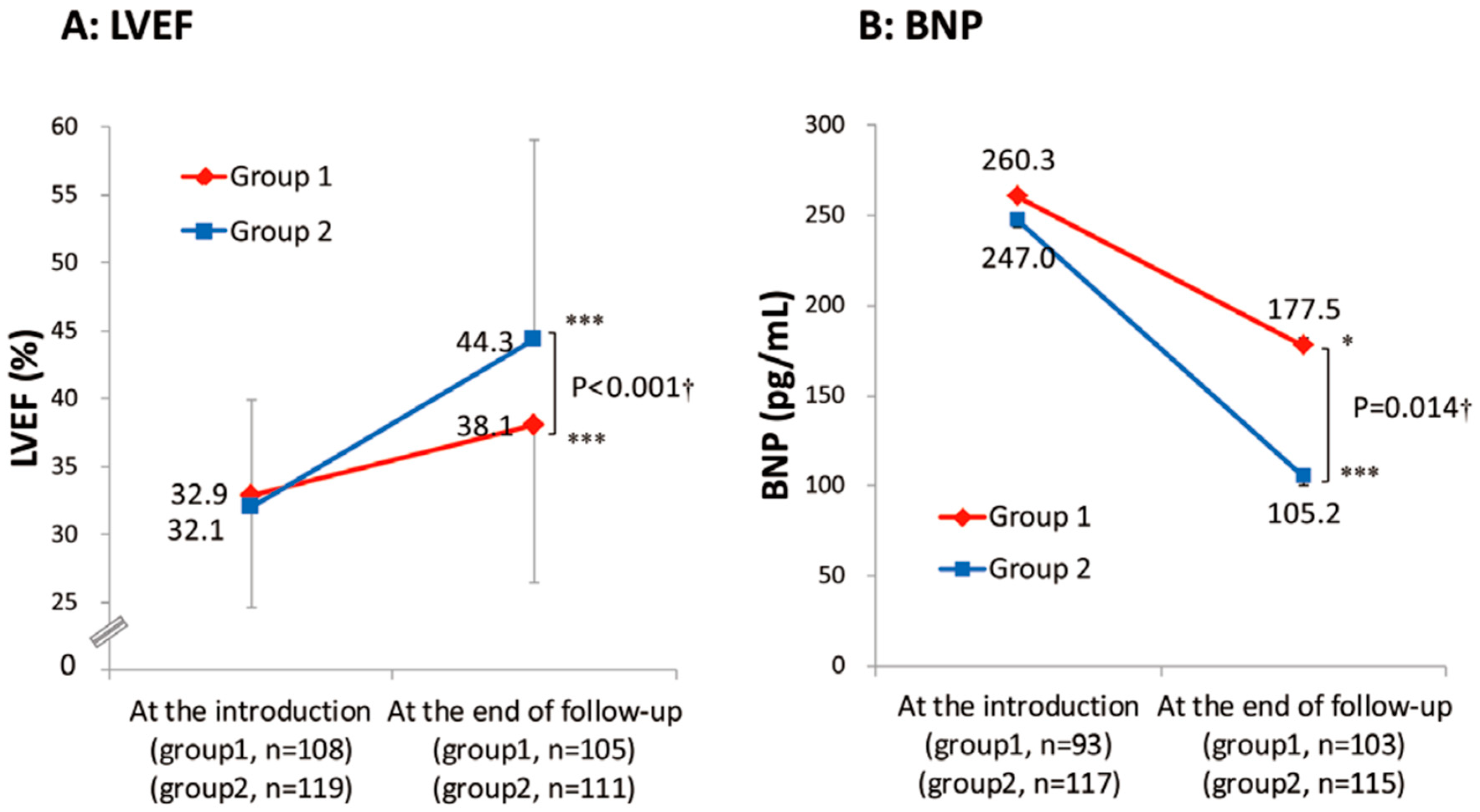
2. Beta-Blocker as a Mainstay for HFrEF and Challenges in Its Up-Titration
3. Indication for Ivabradine
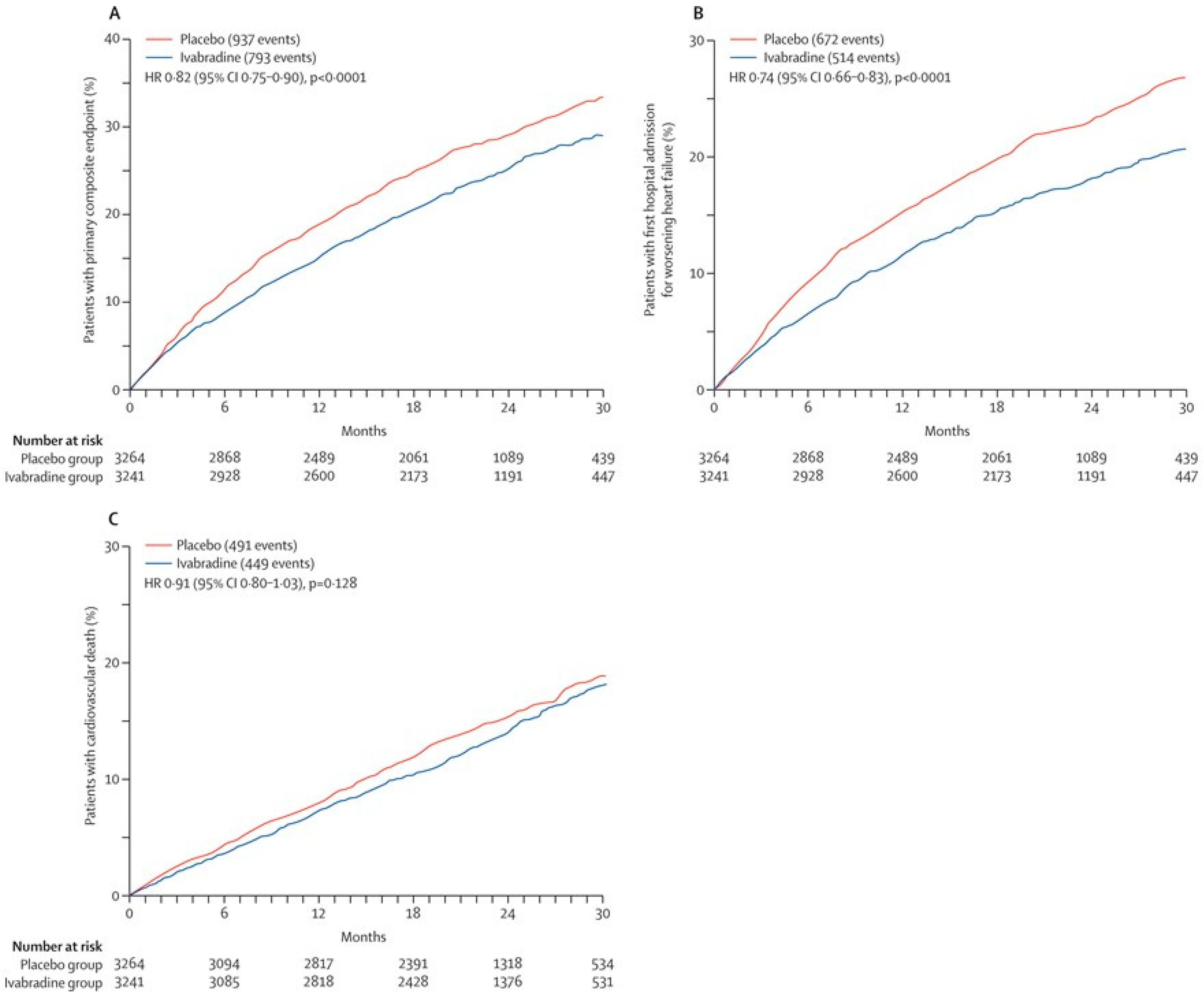
4. The SHIFT Trial: A Cornerstone Trial That Established the Current Indication of Ivabradine
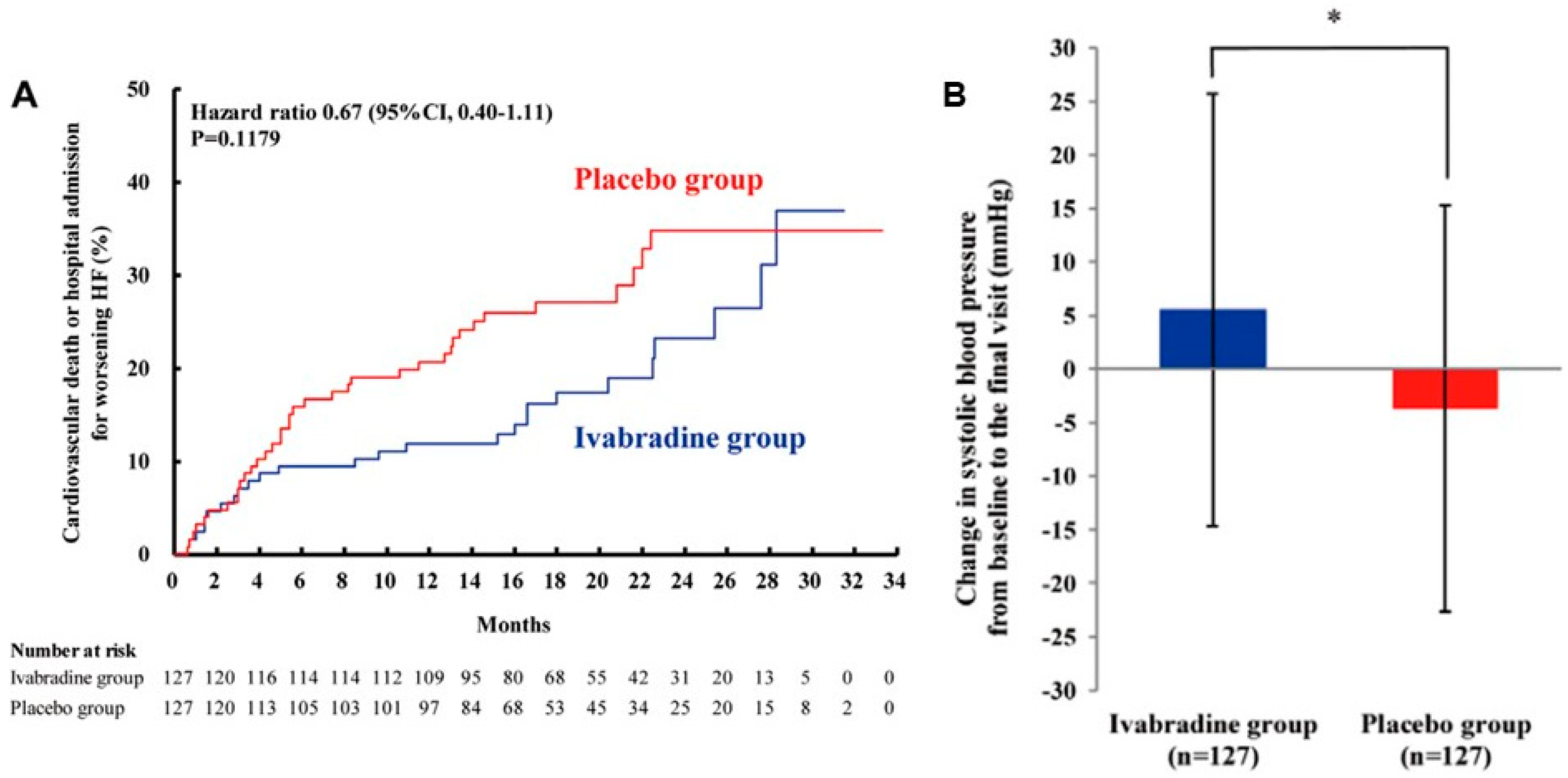
5. J-SHIFT Trial
6. Ivabradine and Cardiac Output
7. Lower Is Better?
8. How to Estimate Target Heart Rate
9. Generalization of the Formula to Diverse Clinical Scenarios with HFrEF
10. Optimal Heart Rate in HFpEF
11. Echocardiography-Guided Heart-Rate Modulation
12. Expanding Ivabradine Indications to Other Clinical Scenarios
13. Controversial Aspects of Ivabradine Indication
14. Future Considerations
15. Conclusions
Funding
Conflicts of Interest
References
- Tsutsui, H.; Ide, T.; Ito, H.; Kihara, Y.; Kinugawa, K.; Kinugawa, S.; Makaya, M.; Murohara, T.; Node, K.; Saito, Y.; et al. JCS/JHFS 2021 Guideline Focused Update on Diagnosis and Treatment of Acute and Chronic Heart Failure. J. Card. Fail. 2021, 27, 1404–1444. [Google Scholar] [CrossRef]
- Mcdonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Boehm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2023, 44, 3627–3639. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e263–e421. [Google Scholar] [CrossRef] [PubMed]
- Kotecha, D.; Flather, M.D.; Altman, D.G.; Holmes, J.; Rosano, G.; Wikstrand, J.; Packer, M.; Coats, A.J.; Manzano, L.; Böhm, M.; et al. Beta-Blockers in Heart Failure Collaborative G. Heart Rate and Rhythm and the Benefit of Beta-Blockers in Patients with Heart Failure. J. Am. Coll. Cardiol. 2017, 69, 2885–2896. [Google Scholar] [CrossRef] [PubMed]
- Li, S.J.; Sartipy, U.; Lund, L.H.; Dahlstrom, U.; Adiels, M.; Petzold, M.; Fu, M. Prognostic Significance of Resting Heart Rate and Use of beta-Blockers in Atrial Fibrillation and Sinus Rhythm in Patients with Heart Failure and Reduced Ejection Fraction: Findings from the Swedish Heart Failure Registry. Circ. Heart Fail. 2015, 8, 871–879. [Google Scholar] [CrossRef] [PubMed]
- Alpert, N.R.; Leavitt, B.J.; Ittleman, F.P.; Hasenfuss, G.; Pieske, B.; Mulieri, L.A. A mechanistic analysis of the force-frequency relation in non-failing and progressively failing human myocardium. Basic Res. Cardiol. 1998, 93 (Suppl. S1), 23–32. [Google Scholar] [CrossRef] [PubMed]
- Koruth, J.S.; Lala, A.; Pinney, S.; Reddy, V.Y.; Dukkipati, S.R. The Clinical Use of Ivabradine. J. Am. Coll. Cardiol. 2017, 70, 1777–1784. [Google Scholar] [CrossRef] [PubMed]
- Swedberg, K.; Komajda, M.; Böhm, M.; Borer, J.S.; Ford, I.; Dubost-Brama, A.; Lerebours, G.; Tavazzi, L.; on behalf of the SHIFT Investigators. Ivabradine and outcomes in chronic heart failure (SHIFT): A randomised placebo-controlled study. Lancet 2010, 376, 875–885. [Google Scholar] [CrossRef]
- Böhm, M.; Swedberg, K.; Komajda, M.; Borer, J.S.; Ford, I.; Dubost-Brama, A.; Lerebours, G.; Tavazzi, L. Heart rate as a risk factor in chronic heart failure (SHIFT): The association between heart rate and outcomes in a randomised placebo-controlled trial. Lancet 2010, 376, 886–894. [Google Scholar] [CrossRef]
- Bohm, M.; Borer, J.; Ford, I.; Gonzalez-Juanatey, J.R.; Komajda, M.; Lopez-Sendon, J.; Reil, J.C.; Swedberg, K.; Tavazzi, L. Heart rate at baseline influences the effect of ivabradine on cardiovascular outcomes in chronic heart failure: Analysis from the SHIFT study. Clin. Res. Cardiol. 2013, 102, 11–22. [Google Scholar] [CrossRef]
- Izumida, T.; Imamura, T.; Nakamura, M.; Fukuda, N.; Kinugawa, K. How to consider target heart rate in patients with systolic heart failure. ESC Heart Fail. 2020, 7, 3231–3234. [Google Scholar] [CrossRef] [PubMed]
- Izumida, T.; Imamura, T.; Fukui, T.; Koi, T.; Ueno, Y.; Hori, M.; Nakagaito, M.; Tanaka, S.; Kataoka, N.; Ushijima, R.; et al. How to Estimate the Optimal Heart Rate in Patients with Heart Failure with Preserved Ejection Fraction. Int. Heart J. 2021, 62, 816–820. [Google Scholar] [CrossRef] [PubMed]
- Turley, S.L.; Francis, K.E.; Lowe, D.K.; Cahoon, W.D. Emerging role of ivabradine for rate control in atrial fibrillation. Ther. Adv. Cardiovasc. Dis. 2016, 10, 348–352. [Google Scholar] [CrossRef] [PubMed]
- Bristow, M.R.; Gilbert, E.M.; Abraham, W.T.; Adams, K.F.; Fowler, M.B.; Hershberger, R.E.; Kubo, S.H.; Narahara, K.A.; Ingersoll, H.; Krueger, S.; et al. Carvedilol Produces Dose-Related Improvements in Left Ventricular Function and Survival in Subjects with Chronic Heart Failure. Circulation 1996, 94, 2807–2816. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, A.S.; DeVore, A.D.; DeWald, T.A.; Swedberg, K.; Mentz, R.J. Achieving a Maximally Tolerated beta-Blocker Dose in Heart Failure Patients: Is There Room for Improvement? J. Am. Coll. Cardiol. 2017, 69, 2542–2550. [Google Scholar] [CrossRef] [PubMed]
- Kato, N.; Kinugawa, K.; Imamura, T.; Muraoka, H.; Minatsuki, S.; Inaba, T.; Maki, H.; Shiga, T.; Hatano, M.; Yao, A.; et al. Trend of clinical outcome and surrogate markers during titration of beta-blocker in heart failure patients with reduced ejection fraction: Relevance of achieved heart rate and beta-blocker dose. Circ. J. 2013, 77, 1001–1008. [Google Scholar] [CrossRef]
- Greene, S.J.; Fonarow, G.C.; DeVore, A.D.; Sharma, P.P.; Vaduganathan, M.; Albert, N.M.; Duffy, C.I.; Hill, C.L.; McCague, K.; Patterson, J.H.; et al. Titration of Medical Therapy for Heart Failure with Reduced Ejection Fraction. J. Am. Coll. Cardiol. 2019, 73, 2365–2383. [Google Scholar] [CrossRef]
- Imamura, T.; Onoda, H.; Uchida, K.; Kinugawa, K. Implication of Ivabradine Therapy in Up-Titrating Beta-Blocker Dose in Patients with Systolic Dysfunction. Int. Heart J. 2021, 62, 1305–1309. [Google Scholar] [CrossRef]
- Swedberg, K.; Komajda, M.; Bohm, M.; Borer, J.S.; Ford, I.; Tavazzi, L. Rationale and design of a randomized, double-blind, placebo-controlled outcome trial of ivabradine in chronic heart failure: The Systolic Heart Failure Treatment with the I(f) Inhibitor Ivabradine Trial (SHIFT). Eur. J. Heart Fail. 2010, 12, 75–81. [Google Scholar] [CrossRef]
- Tardif, J.-C.; O’Meara, E.; Komajda, M.; Böhm, M.; Borer, J.S.; Ford, I.; Tavazzi, L.; Swedberg, K. Effects of selective heart rate reduction with ivabradine on left ventricular remodelling and function: Results from the SHIFT echocardiography substudy. Eur. Heart J. 2011, 32, 2507–2515. [Google Scholar] [CrossRef]
- Tsutsui, H.; Momomura, S.-I.; Yamashina, A.; Shimokawa, H.; Kihara, Y.; Saito, Y.; Hagiwara, N.; Ito, H.; Yano, M.; Yamamoto, K.; et al. Efficacy and Safety of Ivabradine in Japanese Patients with Chronic Heart Failure—J-SHIFT Study—. Circ. J. 2019, 83, 2049–2060. [Google Scholar] [CrossRef] [PubMed]
- Salvi, P.; Palombo, C.; Salvi, G.M.; Labat, C.; Parati, G.; Benetos, A. Left ventricular ejection time, not heart rate, is an independent correlate of aortic pulse wave velocity. J. Appl. Physiol. 2013, 115, 1610–1617. [Google Scholar] [CrossRef] [PubMed]
- Bakkehaug, J.P.; Næsheim, T.; Engstad, E.T.; Kildal, A.B.; Myrmel, T.; How, O. Reversing dobutamine-induced tachycardia using ivabradine increases stroke volume with neutral effect on cardiac energetics in left ventricular post-ischaemia dysfunction. Acta Physiol. 2016, 218, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Lau, K.; Malik, A.; Foroutan, F.; Buchan, T.A.; Daza, J.F.; Sekercioglu, N.; Orchanian-Cheff, A.; Alba, A.C. Resting Heart Rate as an Important Predictor of Mortality and Morbidity in Ambulatory Patients with Heart Failure: A Systematic Review and Meta-Analysis. J. Card. Fail. 2021, 27, 349–363. [Google Scholar] [CrossRef] [PubMed]
- Writing, C.; Maddox, T.M.; Januzzi, J.L.; Allen, L.A., Jr.; Breathett, K.; Butler, J.; Davis, L.L.; Fonarow, G.C.; Ibrahim, N.E.; Lindenfeld, J.; et al. 2021 Update to the 2017 ACC Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure with Reduced Ejection Fraction: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2021, 77, 772–810. [Google Scholar]
- Nagueh, S.F. Left Ventricular Diastolic Function: Understanding Pathophysiology, Diagnosis, and Prognosis with Echocardiography. JACC Cardiovasc. Imaging 2020, 13 Pt 2, 228–244. [Google Scholar] [CrossRef]
- Hori, M.; Imamura, T.; Narang, N.; Kinugawa, K. Implications of Doppler Echocardiography-guided Heart Rate Modulation Using Ivabradine. Intern. Med. 2021, 60, 3873–3877. [Google Scholar] [CrossRef]
- Izumida, T.; Imamura, T.; Ueno, Y.; Tanaka, S.; Kataoka, N.; Nakamura, M.; Kinugawa, K. Impact of optimal heart rate on left ventricular reverse remodeling and functional improvement in patients with systolic heart failure. Heart Vessels 2021, 36, 1688–1693. [Google Scholar] [CrossRef]
- Imamura, T.; Tanaka, S.; Ushijima, R.; Sobajima, M.; Fukuda, N.; Ueno, H.; Besser, S.; Kinugawa, K. The implication of optimal heart rate in patients with systolic dysfunction following TAVR. J. Card. Surg. 2021, 36, 1328–1333. [Google Scholar] [CrossRef]
- Mehra, M.R.; Goldstein, D.J.; Cleveland, J.C.; Cowger, J.A.; Hall, S.; Salerno, C.T.; Naka, Y.; Horstmanshof, D.; Chuang, J.; Wang, A.; et al. Five-Year Outcomes in Patients with Fully Magnetically Levitated vs Axial-Flow Left Ventricular Assist Devices in the MOMENTUM 3 Randomized Trial. JAMA 2022, 328, 1233–1242. [Google Scholar] [CrossRef]
- Burkhoff, D.; Topkara, V.K.; Sayer, G.; Uriel, N. Reverse Remodeling with Left Ventricular Assist Devices. Circ. Res. 2021, 128, 1594–1612. [Google Scholar] [CrossRef] [PubMed]
- Ambardekar, A.V.; Buttrick, P.M. Reverse remodeling with left ventricular assist devices: A review of clinical, cellular, and molecular effects. Circ. Heart Fail. 2011, 4, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Imamura, T.; Mehta, P.; Nguyen, A.; Chung, B.; Narang, N.; Rodgers, D.; Raikhelkar, J.; Smith, B.; Song, T.; Ota, T.; et al. Neurohormonal Blockade During Left Ventricular Assist Device Support. ASAIO J. 2020, 66, 881–885. [Google Scholar] [CrossRef] [PubMed]
- Imamura, T.; Kinugawa, K.; Narang, N.; Nishida, H.; Pinney, S.; Jeevanandam, V.; Ota, T. Implications of Heart Rate in Patients with Left Ventricular Assist Devices. Int. Heart J. 2022, 63, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Bristow, M.R.; Altman, N.L. Heart Rate in Preserved Ejection Fraction Heart Failure. JACC Heart Fail. 2017, 5, 792–794. [Google Scholar] [CrossRef] [PubMed]
- Imamura, T.; Narang, N.; Besser, S.; Kinugawa, K. Chronotropic Assessment in Patients with Constrictive Pericarditis. Int. Heart J. 2021, 62, 811–815. [Google Scholar] [CrossRef] [PubMed]
- Izumida, T.; Imamura, T.; Nakamura, M.; Kinugawa, K. Optimal Heart Rate and Prognosis in Patients with Cardiac Amyloidosis. J. Cardiovasc. Dev. Dis. 2021, 8, 182. [Google Scholar] [CrossRef] [PubMed]
- Izumida, T.; Imamura, T.; Kinugawa, K. Efficacy of Doppler echocardiography-guided ivabradine therapy. Heart Vessel 2023, 38, 49–55. [Google Scholar] [CrossRef]
- Abdin, A.; Komajda, M.; Borer, J.S.; Ford, I.; Tavazzi, L.; Batailler, C.; Swedberg, K.; Rosano, G.M.; Mahfoud, F.; Böhm, M.; et al. Efficacy of ivabradine in heart failure patients with a high-risk profile (analysis from the SHIFT trial). ESC Heart Fail. 2023, 10, 2895–2902. [Google Scholar] [CrossRef]
- Virmani, S.; Mallik, I.; Mohire, V.B.; Geelani, M.A.; Minhas, H.S. Effect of Preoperative Ivabradine on Hemodynamics during Elective Off-Pump CABG. Ann. Card. Anaesth. 2023, 26, 260–267. [Google Scholar] [CrossRef]
- Tóth, N.; Soós, A.; Váradi, A.; Hegyi, P.; Tinusz, B.; Vágvölgyi, A.; Orosz, A.; Solymár, M.; Polyák, A.; Varró, A.; et al. Effect of ivabradine in heart failure: A meta-analysis of heart failure patients with reduced versus preserved ejection fraction. Can. J. Physiol. Pharmacol. 2021, 99, 1159–1174. [Google Scholar] [CrossRef]
- Abdelnabi, M.; Benjanuwattra, J.; Saleh, Y.; Badran, H.; Ahmed, S.; Almaghraby, A. Ivabradine effects in hospitalized acute heart failure patients: A single center retrospective study. Am. J. Cardiovasc. Dis. 2023, 13, 177–182. [Google Scholar]
- Yang, T.-Y.; Tsai, M.-S.; Jan, J.-Y.; Chang, J.-J.; Chung, C.-M.; Lin, M.-S.; Chen, H.-M.; Lin, Y.-S. Early administration of ivabradine in patients admitted for acute decompensated heart failure. Front. Cardiovasc. Med. 2022, 9, 1036418. [Google Scholar] [CrossRef] [PubMed]
- Diaz, A.; Bourassa, M.G.; Guertin, M.-C.; Tardif, J.-C. Long-term prognostic value of resting heart rate in patients with suspected or proven coronary artery disease. Eur. Heart J. 2005, 26, 967–974. [Google Scholar] [CrossRef]
- Tardif, J.C.; Ponikowski, P.; Kahan, T.; Investigators, A.S. Efficacy of the I(f) current inhibitor ivabradine in patients with chronic stable angina receiving beta-blocker therapy: A 4-month, randomized, placebo-controlled trial. Eur. Heart J. 2009, 30, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.; Ford, I.; Steg, P.G.; Tendera, M.; Ferrari, R. Ivabradine for patients with stable coronary artery disease and left-ventricular systolic dysfunction (BEAUTIFUL): A randomised, double-blind, placebo-controlled trial. Lancet 2008, 372, 807–816. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.; Ford, I.; Steg, P.G.; Tardif, J.C.; Tendera, M.; Ferrari, R.; Investigators, S. Ivabradine in stable coronary artery disease without clinical heart failure. N. Engl. J. Med. 2014, 371, 1091–1099. [Google Scholar] [CrossRef]
- Bedet, A.; Voiriot, G.; Ternacle, J.; Marcos, E.; Adnot, S.; Derumeaux, G.; Mekontso Dessap, A. Heart Rate Control during Experimental Sepsis in Mice: Comparison of Ivabradine and beta-Blockers. Anesthesiology 2020, 132, 321–329. [Google Scholar] [CrossRef]
- Datta, P.K.; Rewari, V.; Ramachandran, R.; Singh, P.M.; Ray, B.R.; Aravindan, A.; Seth, S.; Parakh, N.; Trikha, A. Effectiveness of enteral ivabradine for heart rate control in septic shock: A randomised controlled trial. Anaesth. Intensive Care 2021, 49, 366–378. [Google Scholar] [CrossRef]
- Moubarak, G.; Logeart, D.; Cazeau, S.; Cohen Solal, A. Might ivabradine be useful in permanent atrial fibrillation? Int. J. Cardiol. 2014, 175, 187–188. [Google Scholar] [CrossRef]
- Fontenla, A.; Villagraz, L.; de Juan, J.; Lozano, A.; Giacoman, S.; López-Gil, M. Ivabradine as an Alternative to AV Node Ablation in a Patient with Permanent Atrial Fibrillation. Rev. Esp. Cardiol. (Engl. Ed). 2017, 70, 1019–1020. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.-H.; Hai, J.-J.; Wong, C.-K.; Lau, C.-P.; Cheung, B.M.-Y.; Tse, H.-F. Ventricular rate control with ivabradine in patients with permanent atrial fibrillation. J. Interv. Card. Electrophysiol. 2022, 65, 597–599. [Google Scholar] [CrossRef] [PubMed]
- Fontenla, A.; Tamargo, J.; Salgado, R.; Lopez-Gil, M.; Mejia, E.; Matia, R.; Toquero, J.; Montilla, I.; Rajjoub, E.A.; Garcia-Fernandez, F.J.; et al. Ivabradine for controlling heart rate in permanent atrial fibrillation: A translational clinical trial. Heart Rhythm. 2023, 20, 822–830. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class | |
|---|---|
| JCS/JHFS guidelines [1] | |
| Resting heart rate ≥ 75 bpm with sinus rhythm, LVEF ≤ 35%, and refractory to optimal medical therapy | IIa |
| ESC guidelines [2] | |
| Resting heart rate ≥ 70 bpm with sinus rhythm, LVEF ≤ 35%, and refractory to optimal medical therapy | IIa |
| AHA/ACC/HFSA guidelines [3] | |
| Resting heart rate ≥ 70 bpm with sinus rhythm, LVEF ≤ 35%, and refractory to optimal medical therapy | IIa |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imamura, T. Clinical Implications of Ivabradine in the Contemporary Era. Medicina 2024, 60, 303. https://doi.org/10.3390/medicina60020303
Imamura T. Clinical Implications of Ivabradine in the Contemporary Era. Medicina. 2024; 60(2):303. https://doi.org/10.3390/medicina60020303
Chicago/Turabian StyleImamura, Teruhiko. 2024. "Clinical Implications of Ivabradine in the Contemporary Era" Medicina 60, no. 2: 303. https://doi.org/10.3390/medicina60020303
APA StyleImamura, T. (2024). Clinical Implications of Ivabradine in the Contemporary Era. Medicina, 60(2), 303. https://doi.org/10.3390/medicina60020303