
Oligoclonal Band Status and Features of Radiological and Clinical Findings in Patients with Multiple Sclerosis in Lithuania


Abstract
1. Introduction
2. Materials and Methods
3. Results
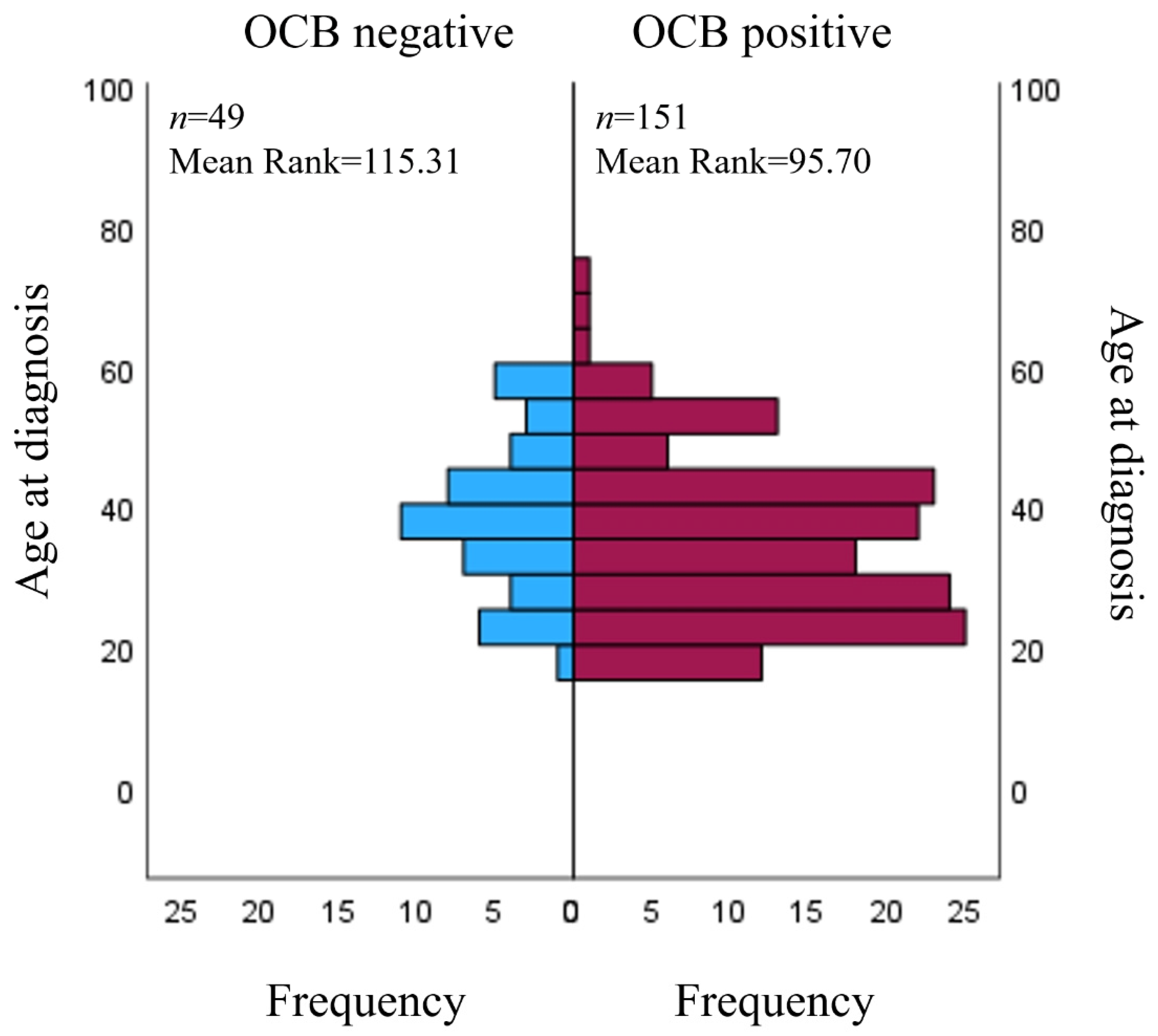
3.1. CSF OCBs and Their Relation to Disease Characteristics
3.2. Features of Radiological Findings and Their Relation to Disease Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walton, C.; King, R.; Rechtman, L.; Kaye, W.; Leray, E.; Marrie, R.A.; Robertson, N.; La Rocca, N.; Uitdehaag, B.; Van Der Mei, I.; et al. Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of MS, third edition. Mult. Scler. J. 2020, 26, 1816–1821. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, F.; Copetti, M.; Sormani, M.P.; Bovis, F.; de Moor, C.; Debray, T.P.; Kieseier, B.C. Predicting disability progression in multiple sclerosis: Insights from advanced statistical modeling. Mult. Scler. J. 2019, 26, 1828–1836. [Google Scholar] [CrossRef] [PubMed]
- Garg, N.; Smith, T.W. An update on immunopathogenesis, diagnosis, and treatment of multiple sclerosis. Brain Behav. 2015, 5, e00362. [Google Scholar] [CrossRef] [PubMed]
- Rival, M.; Galoppin, M.; Thouvenot, E. Biological Markers in Early Multiple Sclerosis: The Paved Way for Radiologically Isolated Syndrome. Front. Immunol. 2022, 13, 866092. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Balnytė, R.; Matijošaitis, V.; Čelpačenko, I.; Malciūtė, M.; Stankevičiūtė, R.; Laucius, O. Factors Related to the Progression of Clinically Isolated Syndrome to Multiple Sclerosis: A Retrospective Study in Lithuania. Medicina 2022, 58, 1178. [Google Scholar] [CrossRef]
- Dobson, R.; Ramagopalan, S.; Davis, A.; Giovannoni, G. Cerebrospinal fluid oligoclonal bands in multiple sclerosis and clinically isolated syndromes: A meta-analysis of prevalence, prognosis and effect of latitude. J. Neurol. Neurosurg. Psychiatry 2013, 84, 909–914. [Google Scholar] [CrossRef]
- Von Glehn, F.; Farias, A.S.; De Oliveira, A.C.P.; Damasceno, A.; Longhini, A.L.F.; Oliveira, E.C.; Damasceno, B.P.; Santos, L.M.B.; Brandão, C.O. Disappearance of cerebrospinal fluid oligoclonal bands after natalizumab treatment of multiple sclerosis patients. Mult. Scler. 2012, 18, 1038–1041. [Google Scholar] [CrossRef]
- Hemond, C.C.; Bakshi, R. Magnetic resonance imaging in multiple sclerosis. Cold Spring Harb. Perspect. Med. 2018, 8, a028969. [Google Scholar] [CrossRef]
- Filippi, M.; Preziosa, P.; Banwell, B.L.; Barkhof, F.; Ciccarelli, O.; De Stefano, N.; Geurts, J.J.G.; Paul, F.; Reich, D.S.; Toosy, A.T.; et al. Assessment of lesions on magnetic resonance imaging in multiple sclerosis: Practical guidelines. Brain 2019, 142, 1858–1875. [Google Scholar] [CrossRef]
- Sormani, M.P.; Bruzzi, P. MRI lesions as a surrogate for relapses in multiple sclerosis: A meta-analysis of randomised trials. Lancet Neurol. 2013, 12, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Elliott, C.; Belachew, S.; Wolinsky, J.S.; Hauser, S.L.; Kappos, L.; Barkhof, F.; Bernasconi, C.; Fecker, J.; Model, F.; Wei, W.; et al. Chronic white matter lesion activity predicts clinical progression in primary progressive multiple sclerosis. Brain 2019, 142, 2787–2799. [Google Scholar] [CrossRef] [PubMed]
- Ammitzbøll, C.; Dyrby, T.; Lyksborg, M.; Schreiber, K.; Ratzer, R.; Christensen, J.R.; Iversen, P.; Magyari, M.; Garde, E.; Sørensen, P.; et al. Disability in progressive MS is associated with T2 lesion changes. Mult. Scler. Relat. Disord. 2018, 20, 73–77. [Google Scholar] [CrossRef]
- Koch, M.W.; Mostert, J.; Repovic, P.; Bowen, J.D.; Strijbis, E.; Uitdehaag, B.; Cutter, G. MRI brain volume loss, lesion burden, and clinical outcome in secondary progressive multiple sclerosis. Mult. Scler. J. 2022, 28, 561–572. [Google Scholar] [CrossRef]
- Radue, E.-W.; Barkhof, F.; Kappos, L.; Sprenger, T.; Häring, D.A.; de Vera, A.; von Rosenstiel, P.; Bright, J.R.; Francis, G.; Cohen, J.A. Correlation between brain volume loss and clinical and MRI outcomes in multiple sclerosis. Neurology 2015, 84, 784–793. [Google Scholar] [CrossRef] [PubMed]
- Charil, A.; Zijdenbos, A.P.; Taylor, J.; Boelman, C.; Worsley, K.J.; Evans, A.C.; Dagher, A. Statistical mapping analysis of lesion location and neurological disability in multiple sclerosis: Application to 452 patient data sets. Neuroimage 2003, 19, 532–544. [Google Scholar] [CrossRef]
- Graner, M.; Pointon, T.; Manton, S.; Green, M.; Dennison, K.; Davis, M.; Braiotta, G.; Craft, J.; Edwards, T.; Polonsky, B.; et al. Oligoclonal IgG antibodies in multiple sclerosis target patient-specific peptides. PLoS ONE 2020, 15, e0228883. [Google Scholar] [CrossRef]
- Leray, E.; Moreau, T.; Fromont, A.; Edan, G. Epidemiology of multiple sclerosis. Rev. Neurol. 2016, 172, 3–13. [Google Scholar] [CrossRef]
- Orton, S.-M.; Herrera, B.M.; Yee, I.M.; Valdar, W.; Ramagopalan, S.V.; Sadovnick, A.D.; Ebers, G.C.; Canadian Collaborative Study Group. Sex ratio of multiple sclerosis in Canada: A longitudinal study. Lancet Neurol. 2006, 5, 932–936. [Google Scholar] [CrossRef]
- Koch-Henriksen, N.; Sørensen, P.S. The changing demographic pattern of multiple sclerosis epidemiology. Lancet Neurol. 2010, 9, 520–532. [Google Scholar] [CrossRef]
- Wandall-Holm, M.F.; Andersen, M.A.; Buron, M.D.; Magyari, M. Aging With Multiple Sclerosis: Age-Related Factors and Socioeconomic Risks. Front. Neurol. 2022, 13, 818652. [Google Scholar] [CrossRef] [PubMed]
- Kaya Tutar, N.; Söylemez, E.; Ömerhoca, S.; Kale İçen, N. The Effect of Oligoclonal Bands in Patients with Multiple Sclerosis. Turk. J. Neurol. 2023, 28, 217–222. [Google Scholar] [CrossRef]
- Karrenbauer, V.D.; Bedri, S.K.; Hillert, J.; Manouchehrinia, A. Cerebrospinal fluid oligoclonal immunoglobulin gamma bands and long-term disability progression in multiple sclerosis: A retrospective cohort study. Sci. Rep. 2021, 11, 14987. [Google Scholar] [CrossRef] [PubMed]
- Lu, T.; Zhao, L.; Sun, X.; Au, C.; Huang, Y.; Yang, Y.; Bao, J.; Wu, A.; Kermode, A.G.; Qiu, W.; et al. Comparison of multiple sclerosis patients with and without oligoclonal IgG bands in South China. J. Clin. Neurosci. 2019, 66, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Simonsen, C.S.; Flemmen, H.; Lauritzen, T.; Berg-Hansen, P.; Moen, S.M.; Celius, E.G. The diagnostic value of IgG index versus oligoclonal bands in cerebrospinal fluid of patients with multiple sclerosis. Mult. Scler. J. Exp. Transl. Clin. 2020, 6, 2055217319901291. [Google Scholar] [CrossRef] [PubMed]
- Lourenco, P.; Shirani, A.; Saeedi, J.; Oger, J.; Schreiber, W.E.; Tremlett, H. Oligoclonal bands and cerebrospinal fluid markers in multiple sclerosis: Associations with disease course and progression. Mult. Scler. J. 2013, 19, 577–584. [Google Scholar] [CrossRef]
- Coll-Martinez, C.; Quintana, E.; Buxó, M.; Salavedra-Pont, J.; Gasull-Vicens, L.; Quiroga-Varela, A.; Costa-Frossard, L.; Villar, L.M.; Fernández-Díaz, E.; Gracia, J.; et al. Oligoclonal IgM bands are a promising biomarker for long-term cognitive outcomes in multiple sclerosis. Mult. Scler. Relat. Disord. 2022, 68, 104397. [Google Scholar] [CrossRef]
- Ellidag, H.Y.; Eren, E.; Erdogan, N.; Ture, S.; Yilmaz, N. Comparison of neurophysiological and mri findings of patients with multiple sclerosis using oligoclonal band technique. Ann. Neurosci. 2013, 20, 149–154. [Google Scholar] [CrossRef]
- Zhao, L.; Abrigo, J.; Chen, Q.; Au, C.; Ng, A.; Fan, P.; Mok, V.; Qiu, W.; Kermode, A.G.; Lau, A.Y. Advanced MRI features in relapsing multiple sclerosis patients with and without CSF oligoclonal IgG bands. Sci. Rep. 2020, 10, 13703. [Google Scholar] [CrossRef]
- Sirbu, C.A.; Mezei, R.-M.; Falup-Pecurariu, C.; Bratu, O.G.; Sirbu, A.M.; Ghinescu, M.C.; Radu, F.I. Autonomic dysfunctions in multiple sclerosis: Challenges of clinical practice (Review). Exp. Ther. Med. 2020, 20, 196. [Google Scholar] [CrossRef]
- Rzepiński, Ł.; Zawadka-Kunikowska, M.; Newton, J.L.; Zalewski, P. Cardiac Autonomic Dysfunction in Myasthenia Gravis and Relapsing-Remitting Multiple Sclerosis—A Pilot Study. J. Clin. Med. 2021, 10, 2173. [Google Scholar] [CrossRef] [PubMed]
- Ben Noon, G.; Vigiser, I.; Shiner, T.; Kolb, H.; Karni, A.; Regev, K. Reinforcing the evidence of oligoclonal bands as a prognostic factor in patients with Multiple sclerosis. Mult. Scler. Relat. Disord. 2021, 56, 103220. [Google Scholar] [CrossRef] [PubMed]
- Dekker, I.; Sombekke, M.H.; Balk, L.J.; Moraal, B.; Geurts, J.J.G.; Barkhof, F.; Uitdehaag, B.M.J.; Killestein, J.; Wattjes, M.P. Infratentorial and spinal cord lesions: Cumulative predictors of long-term disability? Mult Scler. 2020, 26, 1381. [Google Scholar] [CrossRef]
- Leguy, S.; Combès, B.; Bannier, E.; Kerbrat, A. Prognostic value of spinal cord MRI in multiple sclerosis patients. Rev. Neurol. 2021, 177, 571–581. [Google Scholar] [CrossRef] [PubMed]
- Kearney, H.; Miller, D.H.; Ciccarelli, O. Spinal cord MRI in multiple sclerosis—Diagnostic, prognostic and clinical value. Nat. Rev. Neurol. 2015, 11, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Pichiecchio, A.; Tavazzi, E.; Maccabelli, G.; Ponzio, M.; Romani, A.; Schiappacassa, R.; Poloni, G.U.; Franciotta, D.; Roccatagliata, L.; Bergamaschi, R.; et al. MR peri-CSF lesions and CSF oligoclonal bands in Italian multiple sclerosis patients. Acta Neurol. Scand. 2009, 120, 242–245. [Google Scholar] [CrossRef]
- Karrenbauer, V.D.; Prejs, R.; Masterman, T.; Hillert, J.; Glaser, A.; Imrell, K. Impact of cerebrospinal-fluid oligoclonal immunoglobulin bands and HLA-DRB1 risk alleles on brain magnetic-resonance-imaging lesion load in Swedish multiple sclerosis patients. J. Neuroimmunol. 2013, 254, 170–173. [Google Scholar] [CrossRef]
- Akaishi, T.; Takahashi, T.; Nakashima, I. Oligoclonal bands and periventricular lesions in multiple sclerosis will not increase blood-brain barrier permeability. J. Neurol. Sci. 2018, 387, 129–133. [Google Scholar] [CrossRef]
- Pareto, D.; Sastre-Garriga, J.; Auger, C.; Vives-Gilabert, Y.; Delgado, J.; Tintoré, M.; Montalban, X.; Rovira, A. Juxtacortical Lesions and Cortical Thinning in Multiple Sclerosis. Am. J. Neuroradiol. 2015, 36, 2270–2276. [Google Scholar] [CrossRef]
- Bermel, R.; Bakshi, R. The measurement and clinical relevance of brain atrophy in multiple sclerosis. Lancet Neurol. 2006, 5, 158–170. [Google Scholar] [CrossRef]
- Gueye, M.; Cacciaguerra, L.; Tedone, N.; Vizzino, C.; Mistri, D.; Pagani, E.; Filippi, M.; Rocca, M.A. Lesion Location Matters in Multiple Sclerosis: Clinical and Cognitive Correlates of Juxtacortical and Subventricular Zone Lesions (P1-1.Virtual). Neurology 2022, 98 (Suppl. 18), 1123. [Google Scholar]
- Kale, N.; Agaoglu, J.; Tanik, O. Electrophysiological and clinical correlates of corpus callosum atrophy in patients with multiple sclerosis. Neurol. Res. 2010, 32, 886–890. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | n (%) |
|---|---|
| Gender | |
| Male | 65 (32.5) |
| Female | 135 (67.5) |
| OCB status | |
| OCB positive | 151 (75.5) |
| OCB negative | 49 (24.5) |
| Course of the disease | |
| RR | 190 (95) |
| PP | 1 (0.5) |
| SP | 9 (4.5) |
| Lesion localization | |
| Periventricular | 184 (92) |
| C. callosum | 148 (74) |
| Brainstem | 100 (50) |
| Cerebellar | 94 (47) |
| Juxtacortical | 131 (66.2) |
| Spinal cord | 80 (56.7) |
| Changes in MRI | |
| Negative | 74 (37.4) |
| Stable/positive | 124 (62.6) |
| Characteristic | Mean (min/max) |
| Age at first symptoms | 32.13 ± 10.8 (12/73) |
| Age at diagnosis | 36.4 ± 11.6 (18/74) |
| Time from first symptoms to diagnosis | 5.07 ± 9.35 (0/56) |
| EDSS1 | 2.28 ± 1.16 (0/7) |
| EDSS2 | 3.17 ± 1.77 (0/9.5) |
| EDSS2–EDSS1 | 0.86 ± 1.66 (−4.5/6.5) |
| Characteristic | OCB+ n(%) | OCB− n(%) | p Value | |
|---|---|---|---|---|
| Gender | Male | 51 (78.5) | 14 (21.5) | 0.499 |
| Female | 100 (74.1) | 35 (25.9) | ||
| Disease course | Relapsing–remitting | 143 (75.3) | 47 (24.7) | 0.837 |
| Primary progressive | 1 (100) | 0 (0) | ||
| Secondary progressive | 7 (77.8) | 2 (22.2) | ||
| MRI lesion localization | Periventricular lesions | 141 (76.6) | 43 (23.4) | 0.207 |
| C. callosum | 113 (76.4) | 35 (23.6) | 0.637 | |
| Brainstem | 81 (81) | 19 (19) | 0.071 | |
| Cerebellar | 74 (78.7) | 20 (21.3) | 0.318 | |
| Juxtacortical | 98 (74.8) | 33 (25.2) | 0.84 | |
| Spinal cord | 65 (81.3) | 15 (18.7) | 0.034 | |
| Changes in MRI (lesion count and size) | Negative | 57 (77) | 17 (23) | 0.655 |
| Stable/positive | 92 (74.2) | 32 (25.8) | ||
| Age at First Symptoms | Age at Diagnosis | Time from First Symptoms to Diagnosis | EDSS1 | EDSS2 | EDSS2-EDSS1 | |
|---|---|---|---|---|---|---|
| Periventricular | 0.247 | 0.502 | 0.226 | 0.685 | 0.372 | 0.424 |
| C. Callosum | 0.505 | 0.338 | 0.366 | 0.371 | 0.085 | 0.045 |
| Brainstem | 0.184 | 0.117 | 0.824 | 0.002 | 0.004 | 0.128 |
| Cerebellum | 0.243 | 0.577 | 0.805 | 0.145 | 0.362 | 0.926 |
| Juxtacortical | 0.921 | 0.241 | 0.002 | 0.320 | 0.090 | 0.075 |
| Spinal cord | 0.479 | 0.496 | 0.555 | 0.339 | 0.143 | 0.073 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aleksandravičiūtė, E.; Stankevičiūtė, R.; Balnytė, R.; Šaknys, L.; Ulozienė, I. Oligoclonal Band Status and Features of Radiological and Clinical Findings in Patients with Multiple Sclerosis in Lithuania. Medicina 2023, 59, 1028. https://doi.org/10.3390/medicina59061028
Aleksandravičiūtė E, Stankevičiūtė R, Balnytė R, Šaknys L, Ulozienė I. Oligoclonal Band Status and Features of Radiological and Clinical Findings in Patients with Multiple Sclerosis in Lithuania. Medicina. 2023; 59(6):1028. https://doi.org/10.3390/medicina59061028
Chicago/Turabian StyleAleksandravičiūtė, Emilija, Radvilė Stankevičiūtė, Renata Balnytė, Laurynas Šaknys, and Ingrida Ulozienė. 2023. "Oligoclonal Band Status and Features of Radiological and Clinical Findings in Patients with Multiple Sclerosis in Lithuania" Medicina 59, no. 6: 1028. https://doi.org/10.3390/medicina59061028
APA StyleAleksandravičiūtė, E., Stankevičiūtė, R., Balnytė, R., Šaknys, L., & Ulozienė, I. (2023). Oligoclonal Band Status and Features of Radiological and Clinical Findings in Patients with Multiple Sclerosis in Lithuania. Medicina, 59(6), 1028. https://doi.org/10.3390/medicina59061028