
Evaluation of the Risk Factors for Cellulitis among Patients with Peripheral Artery Disease

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
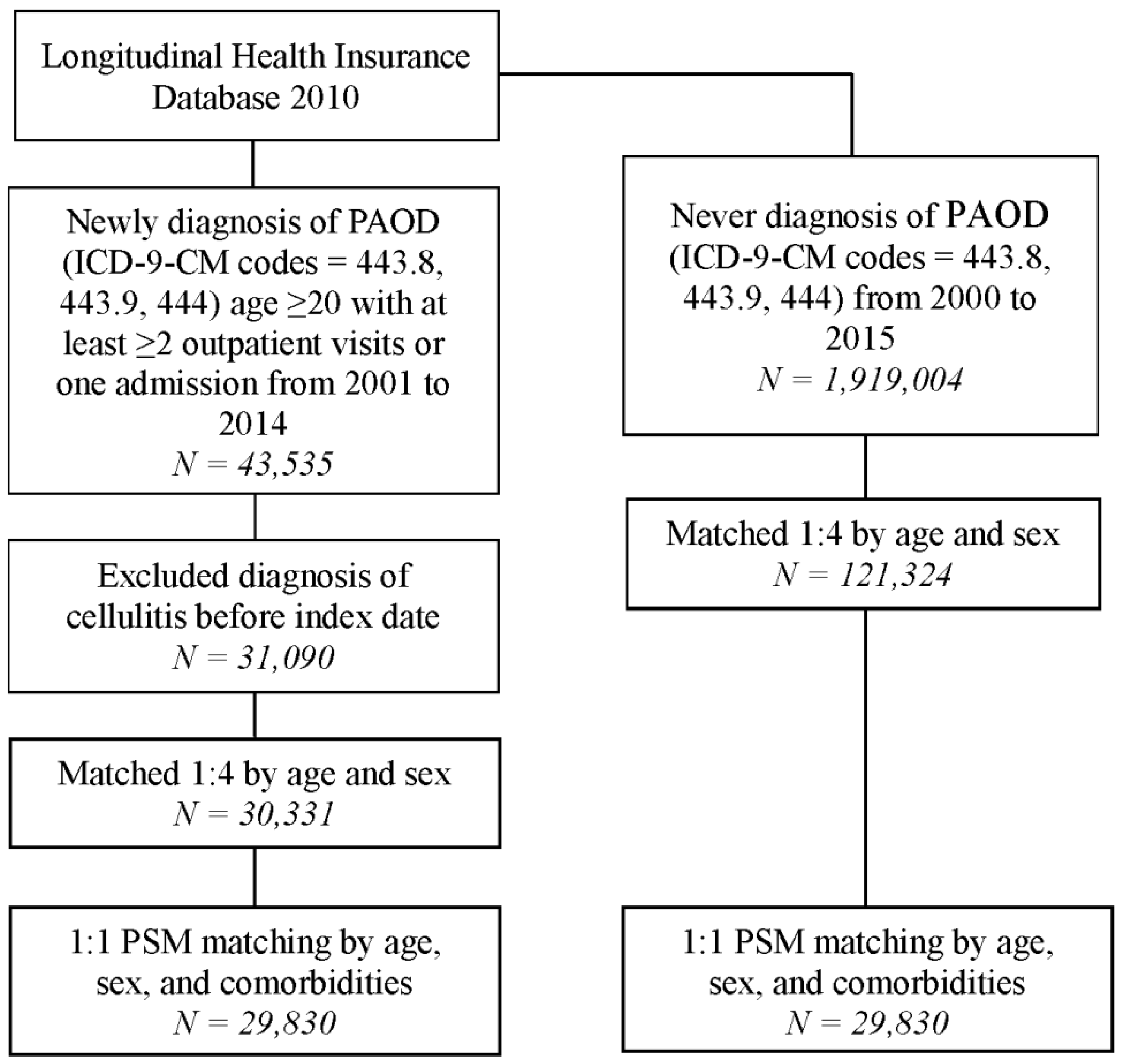
2.2. Patient Selection and Outcome
2.3. Covariates and Matching
2.4. Sensitivity Analysis
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
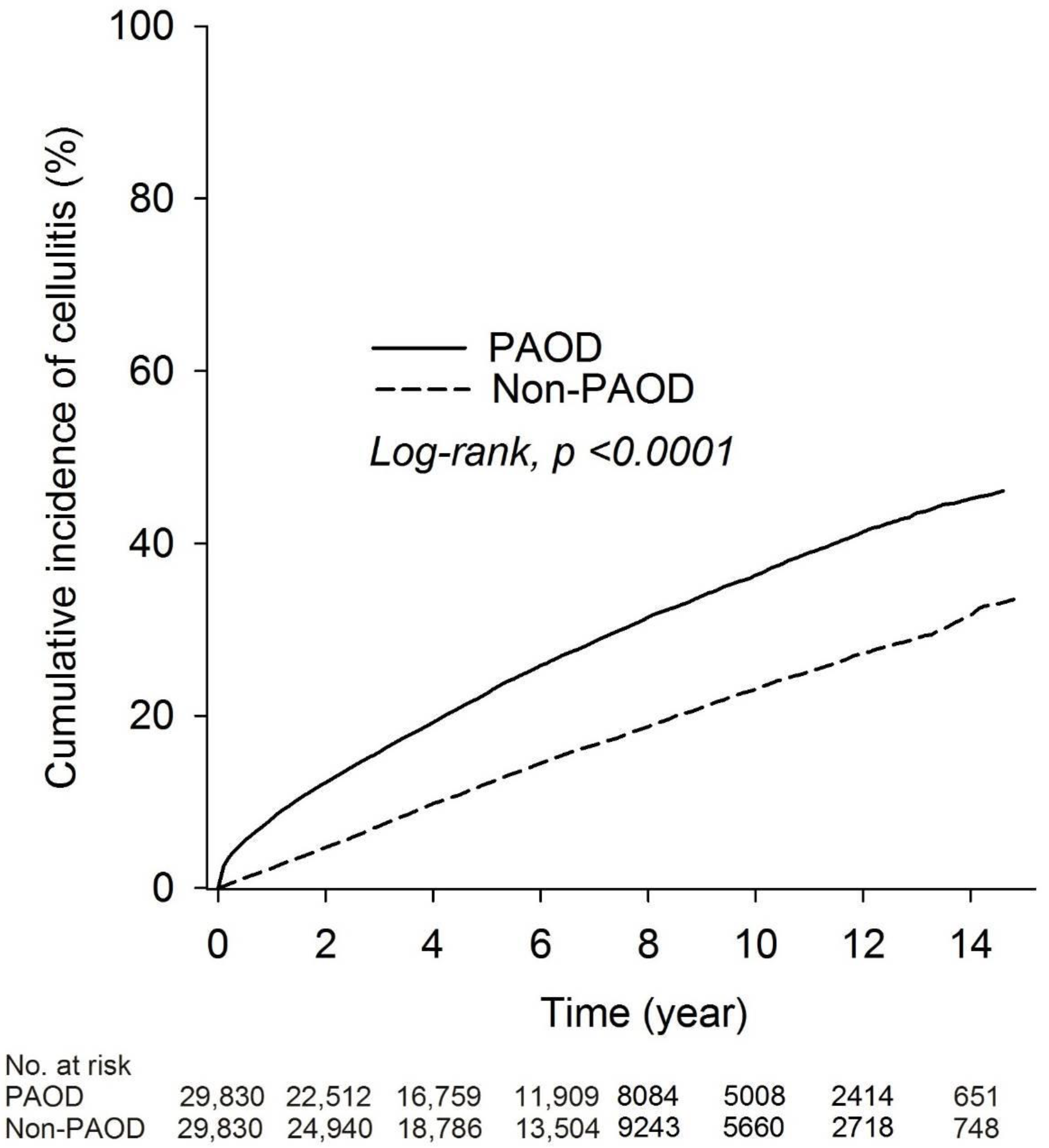
3.2. Risk of Cellulitis between PAOD and Non-PAOD Groups
3.3. Comparison of the Risk of Cellulitis between PAOD and Non-PAOD Groups
3.4. Subgroup Analysis of Cellulitis Risk in the PAOD Group Relative to the Non-PAOD Group after Propensity Score Matching
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yeh, Y.T.; Tseng, Y.S.; Wu, Y.L.; Yang, S.F.; Wang, B.Y.; Wang, Y.H.; Yeh, L.T.; Yeh, Y.T.; Chan, C.H. Risk of Peripheral Arterial Occlusive Disease with Periodontitis and Dental Scaling: A Nationwide Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 10057. [Google Scholar] [CrossRef] [PubMed]
- Binaghi, F.; Fronteddu, P.F.; Cannas, F.; Caredda, E.; Uras, A.; Garau, P.; Pitzus, F. Prevalence of peripheral arterial occlusive disease and associated risk factors in a sample of southern Sardinian population. Int. Angiol. 1994, 13, 233–245. [Google Scholar]
- Hiatt, W.R.; Hoag, S.; Hamman, R.F. Effect of diagnostic criteria on the prevalence of peripheral arterial disease. The San Luis Valley Diabetes Study. Circulation 1995, 91, 1472–1479. [Google Scholar] [CrossRef] [PubMed]
- Hooi, J.D.; Stoffers, H.E.; Kester, A.D.; Rinkens, P.E.; Kaiser, V.; van Ree, J.W.; Knottnerus, J.A. Risk factors and cardiovascular diseases associated with asymptomatic peripheral arterial occlusive disease: The Limburg PAOD Study. Scand. J. Prim. Health Care 1998, 16, 177–182. [Google Scholar] [CrossRef]
- Fowkes, F.G.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.; Williams, L.J.; Mensah, G.A.; et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef] [PubMed]
- Criqui, M.H.; Aboyans, V. Epidemiology of peripheral artery disease. Circ. Res. 2015, 116, 1509–1526. [Google Scholar] [CrossRef]
- Joosten, M.M.; Pai, J.K.; Bertoia, M.L.; Rimm, E.B.; Spiegelman, D.; Mittleman, M.A.; Mukamal, K.J. Associations between conventional cardiovascular risk factors and risk of peripheral artery disease in men. JAMA 2012, 308, 1660–1667. [Google Scholar] [CrossRef]
- Song, P.; Rudan, D.; Zhu, Y.; Fowkes, F.J.I.; Rahimi, K.; Fowkes, F.G.R.; Rudan, I. Global, regional, and national prevalence and risk factors for peripheral artery disease in 2015: An updated systematic review and analysis. Lancet Glob. Health 2019, 7, e1020–e1030. [Google Scholar] [CrossRef]
- Raff, A.B.; Kroshinsky, D. Cellulitis: A Review. JAMA 2016, 316, 325–337. [Google Scholar] [CrossRef]
- Ellis Simonsen, S.M.; van Orman, E.R.; Hatch, B.E.; Jones, S.S.; Gren, L.H.; Hegmann, K.T.; Lyon, J.L. Cellulitis incidence in a defined population. Epidemiol. Infect. 2006, 134, 293–299. [Google Scholar] [CrossRef]
- Cranendonk, D.R.; Lavrijsen, A.P.M.; Prins, J.M.; Wiersinga, W.J. Cellulitis: Current insights into pathophysiology and clinical management. Neth. J. Med. 2017, 75, 366–378. [Google Scholar] [PubMed]
- McCormick, A. Morbidity statistics from general practice. In Fourth National Study 1991–1992; Office of Population Censuses and Surveys: London, UK, 1995. [Google Scholar]
- Bhagat, T.S.; Kumar, L.; Garg, P.; Goel, A.; Aggarwal, A.; Gupta, S. To Study the Clinical Profile and Management of Cellulitis of Lower Limb in Northern India. Int. J. Low. Extrem. Wounds 2021, 22, 1534734620986679. [Google Scholar] [CrossRef] [PubMed]
- Roujeau, J.C.; Sigurgeirsson, B.; Korting, H.C.; Kerl, H.; Paul, C. Chronic dermatomycoses of the foot as risk factors for acute bacterial cellulitis of the leg: A case-control study. Dermatology 2004, 209, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Björnsdóttir, S.; Gottfredsson, M.; Thórisdóttir, A.S.; Gunnarsson, G.B.; Ríkardsdóttir, H.; Kristjánsson, M.; Hilmarsdóttir, I. Risk factors for acute cellulitis of the lower limb: A prospective case-control study. Clin. Infect. Dis. 2005, 41, 1416–1422. [Google Scholar] [CrossRef] [PubMed]
- Chambers, E.S.; Vukmanovic-Stejic, M. Skin barrier immunity and ageing. Immunology 2020, 160, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Chisari, G.; Chisari, E.M.; Borzì, A.M.; Grasso, A.; Chisari, C.G. Etiology of chronic skin lesions in subjects with peripheral arterial disease. Clin. Ter. 2018, 169, e51–e57. [Google Scholar] [CrossRef] [PubMed]
- Kujath, P.; Kujath, C. Complicated skin, skin structure and soft tissue infections—Are we threatened by multi-resistant pathogens? Eur. J. Med. Res. 2010, 15, 544–553. [Google Scholar] [CrossRef] [PubMed]
- Jackson, D.J.; Akuthota, P.; Roufosse, F. Eosinophils and eosinophilic immune dysfunction in health and disease. Eur. Respir. Rev. 2022, 31, 210150. [Google Scholar] [CrossRef]
- Long, H.; Zhang, G.; Wang, L.; Lu, Q. Eosinophilic Skin Diseases: A Comprehensive Review. Clin. Rev. Allergy Immunol. 2016, 50, 189–213. [Google Scholar] [CrossRef]
- Quirke, M.; Ayoub, F.; McCabe, A.; Boland, F.; Smith, B.; O’Sullivan, R.; Wakai, A. Risk factors for nonpurulent leg cellulitis: A systematic review and meta-analysis. Br. J. Dermatol. 2017, 177, 382–394. [Google Scholar] [CrossRef]
- Hardman, R.L.; Jazaeri, O.; Yi, J.; Smith, M.; Gupta, R. Overview of classification systems in peripheral artery disease. Semin. Intervent. Radiol. 2014, 31, 378–388. [Google Scholar] [CrossRef] [PubMed]
- Kavurma, M.M.; Bursill, C.; Stanley, C.P.; Passam, F.; Cartland, S.P.; Patel, S.; Loa, J.; Figtree, G.A.; Golledge, J.; Aitken, S.; et al. Endothelial cell dysfunction: Implications for the pathogenesis of peripheral artery disease. Front. Cardiovasc. Med. 2022, 9, 1054576. [Google Scholar] [CrossRef] [PubMed]
- Gimbrone, M.A. Vascular Endothelium in Hemostasis and Thrombosis; Churchill Livingstone: London, UK, 1986; Volume 2. [Google Scholar]
- Majno, G. The Healing Hand: Man and Wound in the Ancient World; Harvard University Press: Cambridge, MA, USA, 1991. [Google Scholar]
- Lin, Z.; Natesan, V.; Shi, H.; Dong, F.; Kawanami, D.; Mahabeleshwar, G.H.; Atkins, G.B.; Nayak, L.; Cui, Y.; Finigan, J.H. Kruppel-like factor 2 regulates endothelial barrier function. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 1952–1959. [Google Scholar] [CrossRef] [PubMed]
- Hobbs, A.J.; Higgs, A.; Moncada, S. Inhibition of nitric oxide synthase as a potential therapeutic target. Annu. Rev. Pharmacol. Toxicol. 1999, 39, 191–220. [Google Scholar] [CrossRef]
- Pober, J.S.; Cotran, R.S. The role of endothelial cells in inflammation. Transplantation 1990, 50, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Jackson, S.P.; Darbousset, R.; Schoenwaelder, S.M. Thromboinflammation: Challenges of therapeutically targeting coagulation and other host defense mechanisms. Blood 2019, 133, 906–918. [Google Scholar] [CrossRef]
- Lin, S.; Lin, R.; Zhang, H.; Xu, Q.; He, Y. Peripheral vascular remodeling during ischemia. Front. Pharmacol. 2022, 13, 1078047. [Google Scholar] [CrossRef]
- Eisenbud, D.E. Oxygen in wound healing: Nutrient, antibiotic, signaling molecule, and therapeutic agent. Clin. Plast. Surg. 2012, 39, 293–310. [Google Scholar] [CrossRef]
- Wang, H.E.; Shapiro, N.I.; Griffin, R.; Safford, M.M.; Judd, S.; Howard, G. Chronic medical conditions and risk of sepsis. PLoS ONE 2012, 7, e48307. [Google Scholar] [CrossRef]
- Wang, B.Y.; Chou, Y.H.; Chung, C.T.; Yang, S.F.; Tzeng, S.L.; Wang, Y.H.; Chou, M.C.; Yeh, C.B.; Chan, C.H. Association of Peripheral Arterial Occlusive Disease and Deep Venous Thrombosis with Risk of Consequent Sepsis Event: A Retrospective Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 6710. [Google Scholar] [CrossRef]
- Smolderen, K.G.; Lee, M.; Arora, T.; Simonov, M.; Mena-Hurtado, C. Peripheral Artery Disease and COVID-19 Outcomes: Insights from the Yale DOM-CovX Registry. Curr. Probl. Cardiol. 2022, 47, 101007. [Google Scholar] [CrossRef]
- Mok, Y.; Ishigami, J.; Lutsey, P.L.; Tanaka, H.; Meyer, M.L.; Heiss, G.; Matsushita, K. Peripheral Artery Disease and Subsequent Risk of Infectious Disease in Older Individuals: The ARIC Study. Mayo Clin. Proc. 2022, 97, 2065–2075. [Google Scholar] [CrossRef]
- Daryapeyma, A.; Östlund, O.; Wahlgren, C.M. Healthcare-associated infections after lower extremity revascularization. Eur. J. Vasc. Endovasc. Surg. 2014, 48, 72–77. [Google Scholar] [CrossRef]
- Abu Dabrh, A.M.; Steffen, M.W.; Undavalli, C.; Asi, N.; Wang, Z.; Elamin, M.B.; Conte, M.S.; Murad, M.H. The natural history of untreated severe or critical limb ischemia. J. Vasc. Surg. 2015, 62, 1642–1651.e1643. [Google Scholar] [CrossRef] [PubMed]
- Duff, S.; Mafilios, M.S.; Bhounsule, P.; Hasegawa, J.T. The burden of critical limb ischemia: A review of recent literature. Vasc. Health Risk Manag. 2019, 15, 187–208. [Google Scholar] [CrossRef] [PubMed]
- Norgren, L.; Hiatt, W.R.; Dormandy, J.A.; Nehler, M.R.; Harris, K.A.; Fowkes, F.G.; Rutherford, R.B. Inter-society consensus for the management of peripheral arterial disease. Int. Angiol. 2007, 26, 81–157. [Google Scholar]
- Polonsky, T.S.; McDermott, M.M. Lower Extremity Peripheral Artery Disease without Chronic Limb-Threatening Ischemia: A Review. JAMA 2021, 325, 2188–2198. [Google Scholar] [CrossRef] [PubMed]
- Soyoye, D.O.; Abiodun, O.O.; Ikem, R.T.; Kolawole, B.A.; Akintomide, A.O. Diabetes and peripheral artery disease: A review. World J. Diabetes 2021, 12, 827–838. [Google Scholar] [CrossRef]
- Dick, F.; Diehm, N.; Galimanis, A.; Husmann, M.; Schmidli, J.; Baumgartner, I. Surgical or endovascular revascularization in patients with critical limb ischemia: Influence of diabetes mellitus on clinical outcome. J. Vasc. Surg. 2007, 45, 751–761. [Google Scholar] [CrossRef]
- Federman, D.G.; Ladiiznski, B.; Dardik, A.; Kelly, M.; Shapshak, D.; Ueno, C.M.; Mostow, E.N.; Richmond, N.A.; Hopf, H.W. Wound Healing Society 2014 update on guidelines for arterial ulcers. Wound Repair Regen. 2016, 24, 127–135. [Google Scholar] [CrossRef]
- Korhonen, M.; Biancari, F.; Söderström, M.; Arvela, E.; Halmesmäki, K.; Albäck, A.; Lepäntalo, M.; Venermo, M. Femoropopliteal balloon angioplasty vs. bypass surgery for CLI: A propensity score analysis. Eur. J. Vasc. Endovasc. Surg. 2011, 41, 378–384. [Google Scholar] [CrossRef]
- Bray, C.; Bell, L.N.; Liang, H.; Haykal, R.; Kaiksow, F.; Mazza, J.J.; Yale, S.H. Erythrocyte Sedimentation Rate and C-reactive Protein Measurements and Their Relevance in Clinical Medicine. Wmj 2016, 115, 317–321. [Google Scholar] [PubMed]
- Dachun, X.; Jue, L.; Liling, Z.; Yawei, X.; Dayi, H.; Pagoto, S.L.; Yunsheng, M. Sensitivity and specificity of the ankle--brachial index to diagnose peripheral artery disease: A structured review. Vasc. Med. 2010, 15, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Watson, E.L.; Patel, B.; Katsogridakis, E.; Pepper, C.J.; Messeder, S.J.; Saratzis, A.; Zubair, M.; Nicholls, J.K.; Chung, E.; Bown, M.J. Selecting Portable Ankle/Toe Brachial Pressure Index Systems for a Peripheral Arterial Disease Population Screening Programme: A Systematic Review, Clinical Evaluation Exercise, and Consensus Process. Eur. J. Vasc. Endovasc. Surg. 2022, 64, 693–702. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Before PSM Matching | After PSM Matching | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Non-PAOD (N = 121,324) | PAOD (N = 30,331) | PAOD (N = 29,830) | Non-PAOD (N = 29,830) | |||||||
| n | % | n | % | ASD | n | % | n | % | ASD | |
| Age | <0.001 | <0.001 | ||||||||
| 20–40 | 8312 | 6.9 | 2078 | 6.9 | 1944 | 6.5 | 2050 | 6.9 | ||
| 40–60 | 54,332 | 44.8 | 13,583 | 44.8 | 13,146 | 44.1 | 13,255 | 44.4 | ||
| ≥60 | 58,680 | 48.4 | 14,670 | 48.4 | 14,740 | 49.4 | 14,525 | 48.7 | ||
| Mean ± SD | 62.95 ± 14.48 | 62.95 ± 14.48 | <0.001 | 63.70 ± 13.98 | 62.96 ± 14.48 | 0.063 | ||||
| Sex | <0.001 | 0.003 | ||||||||
| Female | 63,468 | 52.3 | 15,867 | 52.3 | 15,700 | 52.6 | 15,653 | 52.5 | ||
| Male | 57,856 | 47.7 | 14,464 | 47.7 | 14,130 | 47.4 | 14,177 | 47.5 | ||
| Hypertension | 36,460 | 30.1 | 14,700 | 48.5 | 0.384 | 14,394 | 48.3 | 14,216 | 47.7 | 0.012 |
| Hyperlipidemia | 13,633 | 11.2 | 5863 | 19.3 | 0.226 | 5873 | 19.7 | 5742 | 19.2 | 0.011 |
| Diabetes | 14,823 | 12.2 | 8382 | 27.6 | 0.393 | 7908 | 26.5 | 7904 | 26.5 | <0.001 |
| Hyperthyroidism | 720 | 0.6 | 238 | 0.8 | 0.023 | 247 | 0.8 | 234 | 0.8 | 0.005 |
| Hypothyroidism | 511 | 0.4 | 172 | 0.6 | 0.021 | 170 | 0.6 | 165 | 0.6 | 0.002 |
| Rheumatoid arthritis | 668 | 0.6 | 356 | 1.2 | 0.067 | 350 | 1.2 | 344 | 1.2 | 0.002 |
| Systemic lupus erythematosus | 88 | 0.1 | 75 | 0.2 | 0.044 | 56 | 0.2 | 60 | 0.2 | 0.003 |
| Sjogren’s syndrome | 465 | 0.4 | 212 | 0.7 | 0.043 | 222 | 0.7 | 206 | 0.7 | 0.006 |
| Ankylosing spondylitis | 133 | 0.1 | 74 | 0.2 | 0.032 | 62 | 0.2 | 73 | 0.2 | 0.008 |
| Chronic pulmonary disease | 9898 | 8.2 | 3823 | 12.6 | 0.146 | 3863 | 13.0 | 3746 | 12.6 | 0.012 |
| Renal disease | 2625 | 2.2 | 2576 | 8.5 | 0.285 | 1973 | 6.6 | 2080 | 7.0 | 0.014 |
| Liver disease | 4946 | 4.1 | 2012 | 6.6 | 0.114 | 2042 | 6.8 | 1972 | 6.6 | 0.009 |
| Non-PAOD | PAOD | |
|---|---|---|
| N | 29,830 | 29,830 |
| Person-years | 180,947 | 162,677 |
| No. of cellulitis | 4713 | 7988 |
| ID (95% CI) | 26.05 (25.31–26.80) | 49.10 (48.04–50.19) |
| Relative risk (95% CI) | Reference | 1.89 (1.82–1.95) |
| Univariate | Multivariate † | |||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Group | ||||
| Non-PAOD | Reference | Reference | ||
| PAOD | 1.87 (1.81–1.94) | <0.001 | 1.94 (1.87–2.01) | <0.001 |
| Age | ||||
| 20–40 | Reference | Reference | ||
| 40–60 | 1.48 (1.36–1.61) | <0.001 | 1.30 (1.19–1.41) | <0.001 |
| ≥60 | 2.31 (2.12–2.51) | <0.001 | 1.84 (1.69–2.01) | <0.001 |
| Sex | ||||
| Female | Reference | Reference | ||
| Male | 1.16 (1.12–1.21) | <0.001 | 1.14 (1.10–1.18) | <0.001 |
| Hypertension | 1.42 (1.37–1.47) | <0.001 | 1.13 (1.09–1.17) | <0.001 |
| Hyperlipidemia | 1.12 (1.07–1.17) | <0.001 | 0.91 (0.87–0.95) | <0.001 |
| Diabetes | 1.74 (1.68–1.81) | <0.001 | 1.62 (1.56–1.69) | <0.001 |
| Hyperthyroidism | 0.90 (0.74–1.11) | 0.324 | 0.97 (0.79–1.18) | 0.734 |
| Hypothyroidism | 0.99 (0.77–1.28) | 0.949 | 0.99 (0.77–1.27) | 0.923 |
| Rheumatoid arthritis | 1.43 (1.24–1.65) | <0.001 | 1.40 (1.21–1.62) | <0.001 |
| Systemic lupus erythematosus | 1.57 (1.13–2.18) | 0.007 | 1.78 (1.28–2.47) | <0.001 |
| Sjogren’s syndrome | 1.14 (0.92–1.40) | 0.227 | 1.05 (0.86–1.30) | 0.621 |
| Ankylosing spondylitis | 1.68 (1.24–2.26) | <0.001 | 1.70 (1.26–2.30) | <0.001 |
| Chronic pulmonary disease | 1.44 (1.37–1.51) | <0.001 | 1.26 (1.20–1.32) | <0.001 |
| Renal disease | 1.87 (1.75–1.99) | <0.001 | 1.59 (1.50–1.70) | <0.001 |
| Liver disease | 1.18 (1.10–1.26) | <0.001 | 1.10 (1.03–1.18) | 0.003 |
| Non-PAOD | PAOD | |||||
|---|---|---|---|---|---|---|
| N | No. of Cellulitis Cases | N | No. of Cellulitis Cases | HR (95% CI) | p Value | |
| Age 1 | ||||||
| 20–40 | 1944 | 210 | 2050 | 379 | 1.75 (1.48–2.08) | <0.001 |
| 40–60 | 13,146 | 1935 | 13,255 | 3172 | 1.79 (1.70–1.90) | <0.001 |
| ≥60 | 14,740 | 2568 | 14,525 | 4437 | 2.12 (2.02–2.23) | <0.001 |
| p for interaction < 0.001 | ||||||
| Sex 1 | ||||||
| Female | 15,700 | 2499 | 15,653 | 3997 | 1.84 (1.75–1.94) | <0.001 |
| Male | 14,130 | 2214 | 14,177 | 3991 | 2.12 (2.02–2.24) | <0.001 |
| p for interaction < 0.001 | ||||||
| Hypertension 1 | ||||||
| No | 15,436 | 2235 | 15,614 | 3791 | 1.91 (1.82–2.02) | <0.001 |
| Yes | 14,394 | 2478 | 14,216 | 4197 | 2.03 (1.93–2.13) | <0.001 |
| p for interaction = 0.0640 | ||||||
| Hyperlipidemia 1 | ||||||
| No | 23,957 | 3804 | 24,088 | 6428 | 1.97 (1.89–2.05) | <0.001 |
| Yes | 5873 | 909 | 5742 | 1560 | 2.01 (1.85–2.18) | <0.001 |
| p for interaction = 0.5347 | ||||||
| Diabetes 1 | ||||||
| No | 21,922 | 3308 | 21,926 | 5187 | 1.75 (1.68–1.83) | <0.001 |
| Yes | 7908 | 1405 | 7904 | 2801 | 2.49 (2.34–2.66) | <0.001 |
| p for interaction < 0.001 | ||||||
| Hyperthyroidism 2 | ||||||
| No | 29,583 | 4673 | 29,596 | 7935 | 1.98 (1.91–2.05) | <0.001 |
| Yes | 247 | 40 | 234 | 53 | 1.69 (1.11–2.56) | 0.015 |
| p for interaction = 0.4887 | ||||||
| Hypothyroidism 3 | ||||||
| No | 29,660 | 4689 | 29,665 | 7951 | 1.97 (1.90–2.05) | <0.001 |
| Yes | 170 | 24 | 165 | 37 | 2.04 (1.19–3.49) | 0.010 |
| p for interaction = 0.8925 | ||||||
| Rheumatoid arthritis 1 | ||||||
| No | 29,480 | 4640 | 29,486 | 7869 | 1.97 (1.90–2.04) | <0.001 |
| Yes | 350 | 73 | 344 | 119 | 2.11 (1.57–2.84) | <0.001 |
| p for interaction = 0.4890 | ||||||
| Systemic lupus erythematosus 4 | ||||||
| No | 29,774 | 4698 | 29,770 | 7967 | 1.98 (1.91–2.05) | <0.001 |
| Yes | 56 | 15 | 60 | 21 | 1.56 (0.68–3.56) | 0.292 |
| p for interaction = 0.7374 | ||||||
| Sjogren’s syndrome 5 | ||||||
| No | 29,608 | 4672 | 29,624 | 7940 | 1.98 (1.91–2.05) | <0.001 |
| Yes | 222 | 41 | 206 | 48 | 1.61 (1.04–2.50) | 0.034 |
| p for interaction = 0.2626 | ||||||
| Ankylosing spondylitis 6 | ||||||
| No | 29,768 | 4691 | 29,757 | 7967 | 1.98 (1.91–2.05) | <0.001 |
| Yes | 62 | 22 | 73 | 21 | 1.15 (0.60–2.20) | 0.680 |
| p for interaction = 0.0161 | ||||||
| Chronic pulmonary disease 1 | ||||||
| No | 25,967 | 3973 | 26,084 | 6787 | 1.96 (1.88–2.04) | <0.001 |
| Yes | 3863 | 740 | 3746 | 1201 | 2.05 (1.87–2.25) | <0.001 |
| p for interaction = 0.2229 | ||||||
| Renal disease 1 | ||||||
| No | 27,857 | 4362 | 27,750 | 7278 | 1.92 (1.85–2.00) | <0.001 |
| Yes | 1973 | 351 | 2080 | 710 | 2.65 (2.33–3.02) | <0.001 |
| p for interaction <0.001 | ||||||
| Liver disease 1 | ||||||
| No | 27,788 | 4339 | 27,858 | 7387 | 1.98 (1.90–2.05) | <0.001 |
| Yes | 2042 | 374 | 1972 | 601 | 1.94 (1.71–2.21) | <0.001 |
| p for interaction = 0.8008 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, B.-Y.; Yang, S.-F.; Ting, K.-H.; Wang, Y.-H.; Chou, M.-C.; Yeh, C.-B. Evaluation of the Risk Factors for Cellulitis among Patients with Peripheral Artery Disease. Medicina 2023, 59, 933. https://doi.org/10.3390/medicina59050933
Wang B-Y, Yang S-F, Ting K-H, Wang Y-H, Chou M-C, Yeh C-B. Evaluation of the Risk Factors for Cellulitis among Patients with Peripheral Artery Disease. Medicina. 2023; 59(5):933. https://doi.org/10.3390/medicina59050933
Chicago/Turabian StyleWang, Bo-Yuan, Shun-Fa Yang, Ke-Hsin Ting, Yu-Hsun Wang, Ming-Chih Chou, and Chao-Bin Yeh. 2023. "Evaluation of the Risk Factors for Cellulitis among Patients with Peripheral Artery Disease" Medicina 59, no. 5: 933. https://doi.org/10.3390/medicina59050933
APA StyleWang, B.-Y., Yang, S.-F., Ting, K.-H., Wang, Y.-H., Chou, M.-C., & Yeh, C.-B. (2023). Evaluation of the Risk Factors for Cellulitis among Patients with Peripheral Artery Disease. Medicina, 59(5), 933. https://doi.org/10.3390/medicina59050933