
Association of Periodontal Disease with Activity of Crohn’s Disease

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Assessment of Crohn’s Disease Activity
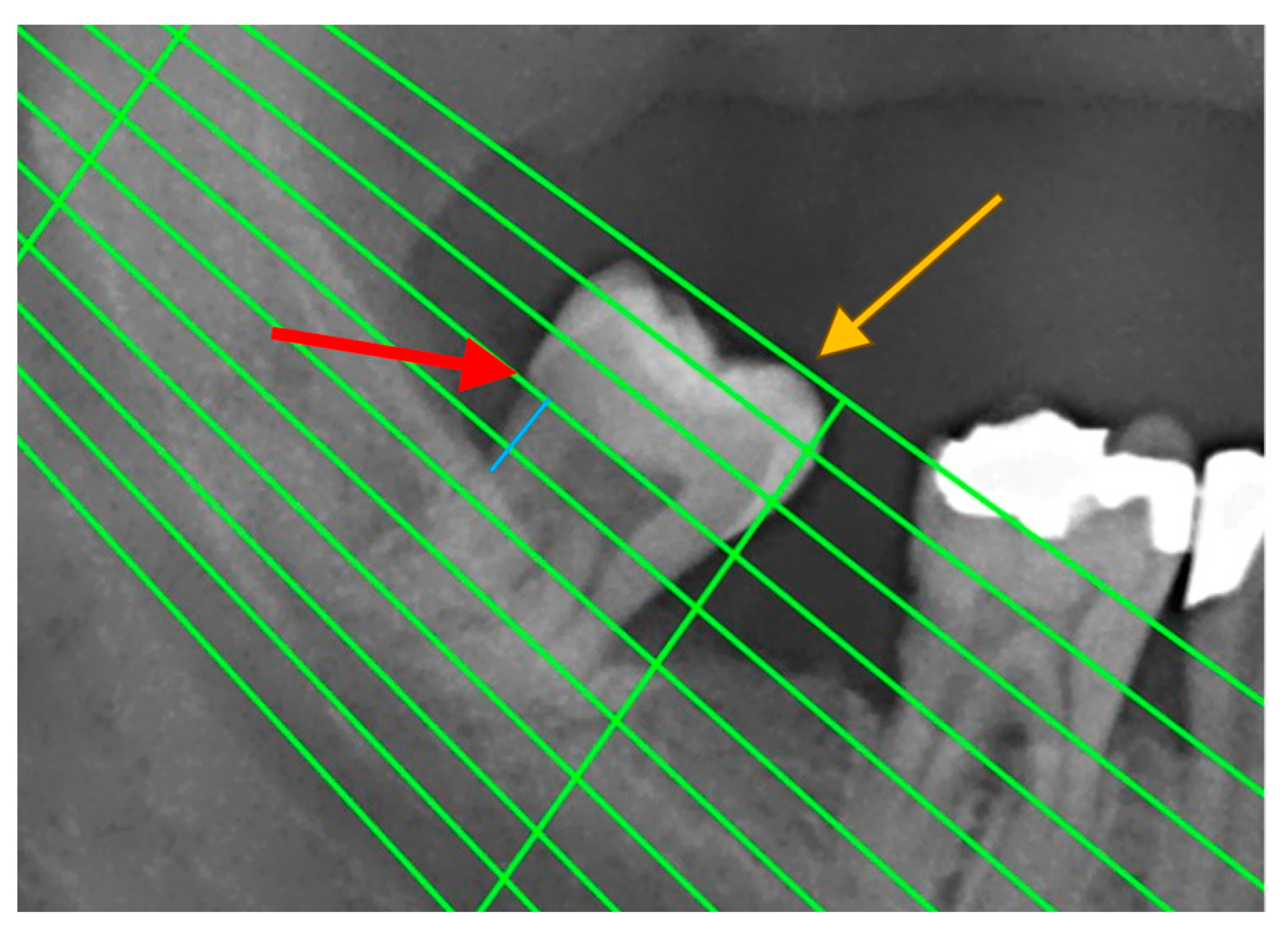
2.3. Assessment of Periodontal Disease
2.4. Statistics
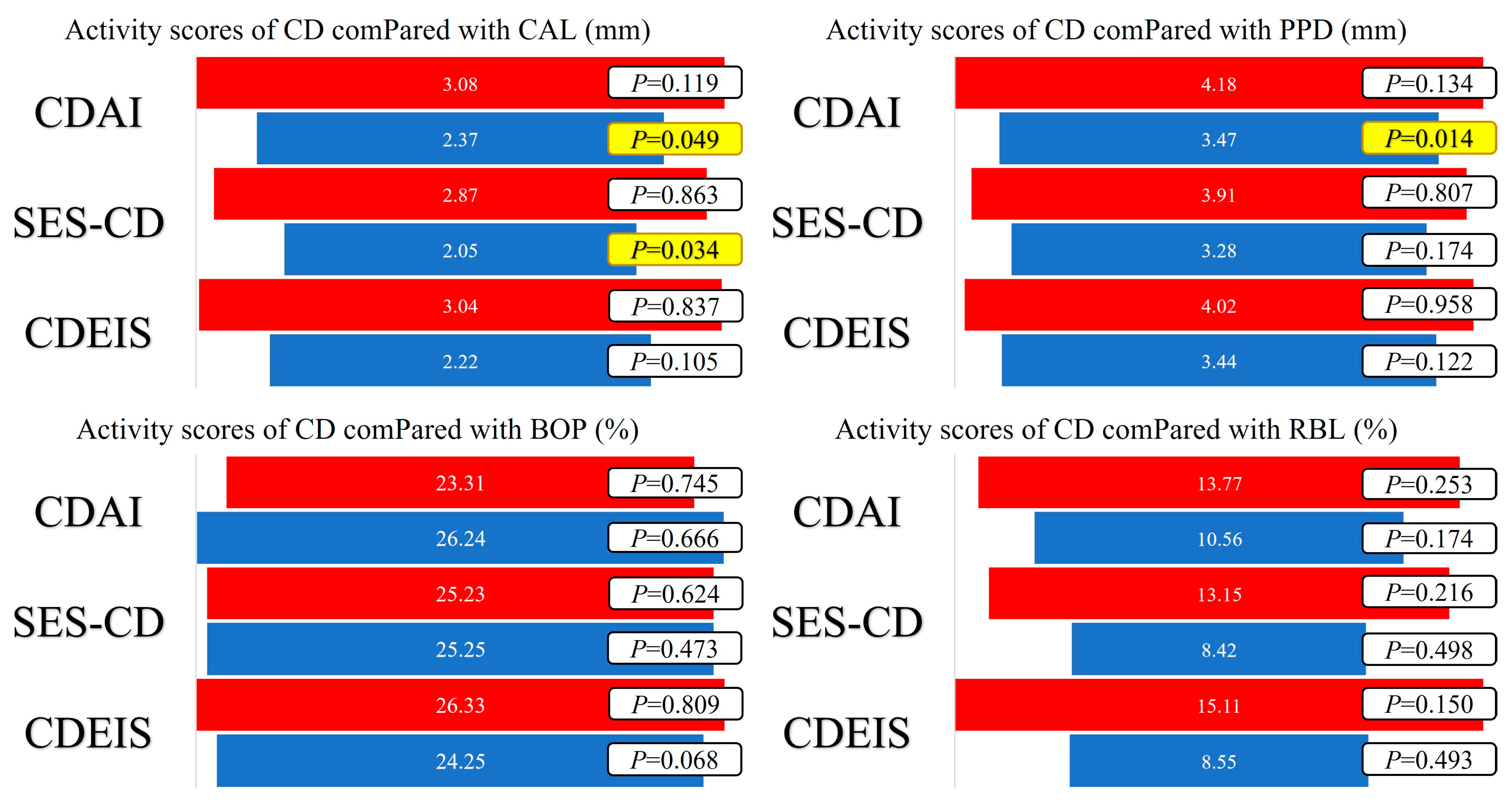
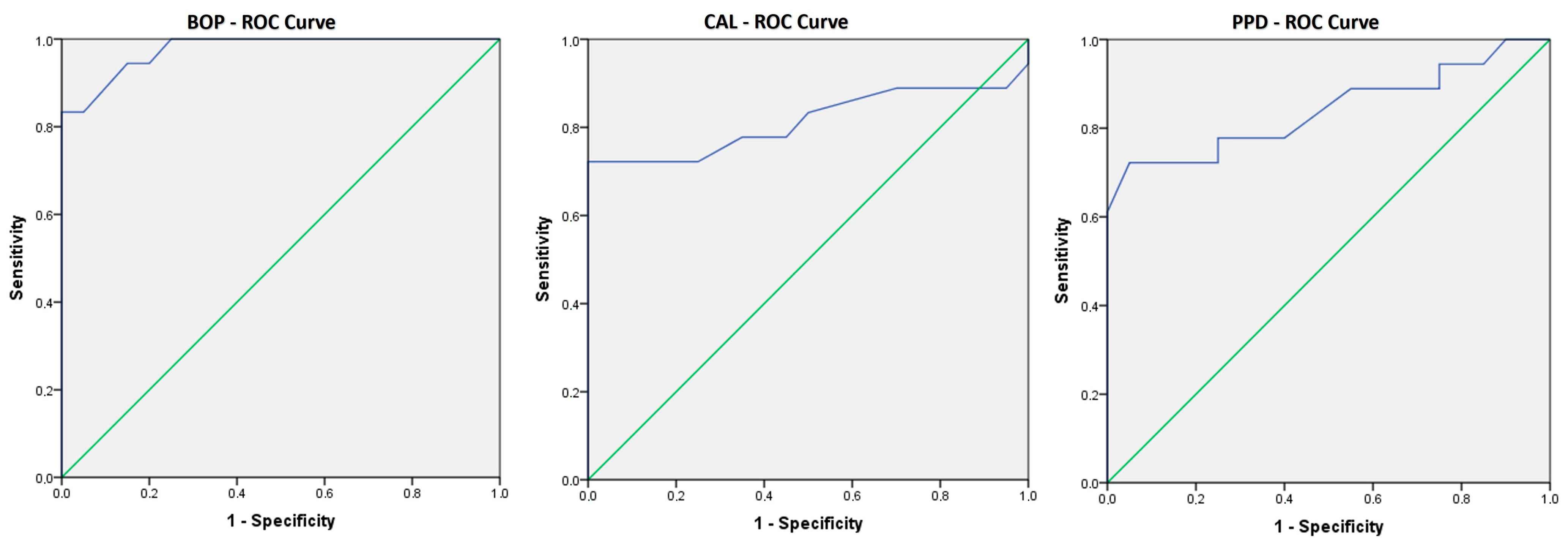
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Torres, J.; Mehandru, S.; Colombel, J.F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef] [PubMed]
- Baumgart, D.C.; Sandborn, W.J. Crohn’s disease. Lancet 2012, 380, 1590–1605. [Google Scholar] [CrossRef]
- Alvarado-Julio, A.; Chumacero-Palma, K.; Buenahora, M.R.; Parra-Izquierdo, V.; Monsalve, M.; Torres, A.M.; Chila-Moreno, L.; Flórez-Sarmiento, C.; Ramos-Casallas, A.; De Avila, J.; et al. Oral manifestations associated with inflammatory bowel disease and early endoscopic findings in patients with spondyloarthritis. BMC Oral Health 2022, 22, 477. [Google Scholar] [CrossRef]
- Matkowskyj, K.A.; Chen, Z.E.; Rao, M.S.; Yang, G.-Y. Dysplastic Lesions in Inflammatory Bowel Disease: Molecular Pathogenesis to Morphology. Arch. Pathol. Lab. Med. 2013, 137, 338–350. [Google Scholar] [CrossRef]
- Borowitz, S.M. The epidemiology of inflammatory bowel disease: Clues to pathogenesis? Front. Pediatr. 2023, 10, 1103713. [Google Scholar] [CrossRef] [PubMed]
- Festen, E.A.M.; Weersma, R.K. How will insights from genetics translate to clinical practice in inflammatory bowel disease? Best Pract. Res. Clin. Gastroenterol. 2014, 28, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Annese, V. Genetics and epigenetics of IBD. Pharmacol. Res. 2020, 159, 104892. [Google Scholar] [CrossRef]
- Brand, S. Moving the genetics of inflammatory bowel diseases from bench to bedside: First steps towards personalised medicine. Gut 2013, 62, 1531–1533. [Google Scholar] [CrossRef]
- Buie, M.J.; Quan, J.; Windsor, J.W.; Coward, S.; Hansen, T.M.; King, J.A.; Kotze, P.G.; Gearry, R.B.; Ng, S.C.; Mak, J.W.; et al. Global Hospitalization Trends for Crohn’s Disease and Ulcerative Colitis in the 21st Century: A Systematic Review with Temporal Analyses. Clin. Gastroenterol. Hepatol. 2023, 21, 2211–2221. [Google Scholar] [CrossRef]
- Meurman, J.; Bascones-Martinez, A. Oral Infections and Systemic Health—More than Just Links to Cardiovascular Diseases. Oral Health Prev. Dent. 2021, 19, 441–448. [Google Scholar]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Primers 2017, 3, 17038. [Google Scholar] [CrossRef]
- Papageorgiou, S.N.; Hagner, M.; Nogueira, A.V.B.; Franke, A.; Jäger, A.; Deschner, J. Inflammatory bowel disease and oral health: Systematic review and a meta-analysis. J. Clin. Periodontol. 2017, 44, 382–393. [Google Scholar] [CrossRef]
- She, Y.Y.; Kong, X.B.; Ge, Y.P.; Liu, Z.Y.; Chen, J.Y.; Jiang, J.W.; Jiang, H.B.; Fang, S.L. Periodontitis and inflammatory bowel disease: A meta-analysis. BMC Oral Health 2020, 20, 67. [Google Scholar] [CrossRef] [PubMed]
- Best, W.R.; Becktel, J.M.; Singleton, J.W.; Kern, F. Development of a Crohn’s disease activity index. Natl. Coop. Crohn’s Dis. Study Gastroenterol. 1976, 70, 439–444. [Google Scholar] [CrossRef]
- Harvey, R.F.; Bradshaw, J.M. A Simple Index of Crohn’s-Disease Activity. Lancet 1980, 315, 514. [Google Scholar] [CrossRef]
- Van Hees, P.A.; Van Elteren, P.H.; Van Lier, H.J.; Van Tongeren, J.H. An index of inflammatory activity in patients with Crohn’s disease. Gut 1980, 21, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Mary, J.Y.; Modigliani, R. Development and validation of an endoscopic index of the severity for Crohn’s disease: A prospective multicentre study. Groupe d’Etudes Therapeutiques des Affections Inflammatoires du Tube Digestif (GETAID). Gut 1989, 30, 983–989. [Google Scholar] [CrossRef]
- Daperno, M.; D’Haens, G.; Van Assche, G.; Baert, F.; Bulois, P.; Maunoury, V.; Sostegni, R.; Rocca, R.; Pera, A.; Gevers, A.; et al. Development validation of a new simplified endoscopic activity score for Crohn’s disease: The SES-CD. Gastrointest. Endosc. 2004, 60, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89, S159–S172. [Google Scholar] [CrossRef]
- Trombelli, L.; Farina, R.; Silva, C.O.; Tatakis, D.N. Plaque-induced gingivitis: Case definition and diagnostic considerations. J. Periodontol. 2018, 89, S46–S73. [Google Scholar] [CrossRef]
- Chapple, I.L.C.; Mealey, B.L.; Van Dyke, T.E.; Bartold, P.M.; Dommisch, H.; Eickholz, P.; Geisinger, M.L.; Genco, R.J.; Glogauer, M.; Goldstein, M.; et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S74–S84. [Google Scholar] [CrossRef]
- Shaker, Z.M.H.; Parsa, A.; Moharamzadeh, K. Development of a Radiographic Index for Periodontitis. Dent. J. 2021, 9, 19. [Google Scholar] [CrossRef] [PubMed]
- Ertaş, K.; Pence, I.; Cesmeli, M.S.; Ay, Z.Y. Determination of the stage and grade of periodontitis according to the current classification of periodontal and peri-implant diseases and conditions (2018) using machine learning algorithms. J. Periodontal Implant. Sci. 2023, 53, 38–53. [Google Scholar] [CrossRef] [PubMed]
- Sedghi, L.M.; Bacino, M.; Kapila, Y.L. Periodontal Disease: The Good, The Bad, and The Unknown. Front. Cell Infect. Microbiol. 2021, 11, 766944. [Google Scholar] [CrossRef]
- Lauritano, D.; Boccalari, E.; Di Stasio, D.; Della Vella, F.; Carinci, F.; Lucchese, A.; Petruzzi, M. Prevalence of Oral Lesions and Correlation with Intestinal Symptoms of Inflammatory Bowel Disease: A Systematic Review. Diagnostics 2019, 9, 77. [Google Scholar] [CrossRef] [PubMed]
- Lankarani, K.B.; Sivandzadeh, G.R.; Hassanpour, S. Oral manifestation in inflammatory bowel disease: A review. World J. Gastroenterol. 2013, 19, 8571. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.X.W. Oral manifestations of Crohn’s disease. Ned. Tijdschr. Tandheelkd. 2018, 125, 15–20. [Google Scholar] [CrossRef]
- Villanacci, V.; Reggiani-Bonetti, L.; Salviato, T.; Leoncini, G.; Cadei, M.; Albarello, L.; Caputo, A.; Aquilano, M.C.; Battista, S.; Parente, P. Histopathology of IBD Colitis. A practical approach from the pathologists of the Italian Group for the study of the gastrointestinal tract (GIPAD). Pathologica 2021, 113, 39–53. [Google Scholar] [CrossRef]
- Habashneh, R.A.; Khader, Y.S.; Alhumouz, M.K.; Jadallah, K.; Ajlouni, Y. The association between inflammatory bowel disease and periodontitis among Jordanians: A case-control study: Inflammatory bowel disease and periodontitis. J. Periodontal Res. 2012, 47, 293–298. [Google Scholar] [CrossRef]
- Zhang, Y.; Qiao, D.; Chen, R.; Zhu, F.; Gong, J.; Yan, F. The Association between Periodontitis and Inflammatory Bowel Disease: A Systematic Review and Meta-analysis. BioMed Res. Int. 2021, 2021, 6692420. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 89, S1–S8. [Google Scholar]
- Stein, J.M.; Lammert, F.; Zimmer, V.; Granzow, M.; Reichert, S.; Schulz, S.; Ocklenburg, C.; Conrads, G. Clinical Periodontal and Microbiologic Parameters in Patients with Crohn’s Disease with Consideration of the CARD15 Genotype. J. Periodontol. 2010, 81, 535–545. [Google Scholar] [CrossRef]
- Zhang, L.; Gao, X.; Zhou, J.; Chen, S.; Zhang, J.; Zhang, Y.; Chen, B.; Yang, J. Increased risks of dental caries and periodontal disease in Chinese patients with inflammatory bowel disease. Int. Dent. J. 2020, 70, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Grossner-Schreiber, B.; Fetter, T.; Hedderich, J.; Kocher, T.; Schreiber, S.; Jepsen, S. Prevalence of dental caries and periodontal disease in patients with inflammatory bowel disease: A case-control study. J. Clin. Periodontol. 2006, 33, 478–484. [Google Scholar] [CrossRef]
- Brito, F.; De Barros, F.C.; Zaltman, C.; Carvalho, A.T.P.; De Vasconcellos Carneiro, A.J.; Fischer, R.G.; Gustafsson, A.; De Silva Figueredo, C.M. Prevalence of periodontitis and DMFT index in patients with Crohn’s disease and ulcerative colitis. J. Clin. Periodontol. 2008, 35, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Menegat, J.S.B.; Lira-Junior, R.; Siqueira, M.A.; Brito, F.; Carvalho, A.T.; Fischer, R.G.; Figueredo, C.M. Cytokine expression in gingival and intestinal tissues of patients with periodontitis and inflammatory bowel disease: An exploratory study. Arch. Oral Biol. 2016, 66, 141–146. [Google Scholar] [CrossRef]
- Koutsochristou, V.; Zellos, A.; Dimakou, K.; Panayotou, I.; Siahanidou, S.; Roma-Giannikou, E.; Tsami, A. Dental Caries and Periodontal Disease in Children and Adolescents with Inflammatory Bowel Disease: A Case–Control Study. Inflamm. Bowel Dis. 2015, 21, 1839–1846. [Google Scholar] [CrossRef]
- Vavricka, S.R.; Manser, C.N.; Hediger, S.; Vögelin, M.; Scharl, M.; Biedermann, L.; Rogler, S.; Seibold, F.; Sanderink, R.; Attin, T.; et al. Periodontitis and Gingivitis in Inflammatory Bowel Disease: A Case–Control Study. Inflamm. Bowel Dis. 2013, 19, 2768–2777. [Google Scholar] [CrossRef]
- Imai, J.; Ichikawa, H.; Kitamoto, S.; Golob, J.L.; Kaneko, M.; Nagata, J.; Takahashi, M.; Gillilland, M.G.; Tanaka, R.; Nagao-Kitamoto, H.; et al. A potential pathogenic association between periodontal disease and Crohn’s disease. JCI Insight 2021, 6, e148543. [Google Scholar] [CrossRef]
- Yin, W.; Ludvigsson, J.F.; Liu, Z.; Roosaar, A.; Axéll, T.; Ye, W. Inverse Association between Poor Oral Health and Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2017, 15, 525–531. [Google Scholar] [CrossRef]
- Piras, V.; Usai, P.; Mezzena, S.; Susnik, M.; Ideo, F.; Schirru, E.; Cotti, E. Prevalence of Apical Periodontitis in Patients with Inflammatory Bowel Diseases: A Retrospective Clinical Study. J. Endod. 2017, 43, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Baima, G.; Muwalla, M.; Testa, G.; Mazza, F.; Bebars, A.; Perotto, S.; Vernero, M.; Massano, A.; Romano, F.; Ribaldone, D.G.; et al. Periodontitis prevalence and severity in inflammatory bowel disease: A case–control study. J. Periodontol. 2023, 94, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Tanwar, H.; Gnanasekaran, J.M.; Allison, D.; Chuang, L.S.; He, X.; Aimetti, M.; Baima, G.; Costalonga, M.; Cross, R.K.; Sears, C.; et al. Unraveling the Link between Periodontitis and Inflammatory Bowel Disease: Challenges and Outlook. arXiv 2023, arXiv:2308.10907v1. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Stage | Clinical Attachment Loss (CAL) | Radiographic Bone Loss (RBL) | Bleeding on Probing (BOP) | Probing Pocket Depth (PPD) |
|---|---|---|---|---|
| Healthy | 0–0.9 mm | None | 0–9% | 0–2.9 mm |
| I | 1–2.9 mm | <15% | <10% | 3–3.9 mm |
| II | 3–3.9 mm | 15–33% | 11–30% | 4–4.9 mm |
| III | 4–4.9 mm | 33–50% | 31–50% | 5–5.9 mm |
| IV | ≥5 mm | >50% | >50% | ≥6 mm |
| CD + PD Group (n = 18) | CD Group (n = 20) | p-Value | ||
|---|---|---|---|---|
| Age (years) | 42.50 (18.00) | 31.00 (22.50) | 0.021 | |
| Illness duration (years) | 7.50 (6.75) | 3.50 (11.25) | 0.212 | |
| Gender | Male (n) | 10 | 11 | |
| Female (n) | 8 | 9 | ||
| BMI | 26.42 ± 5.66 | 22.59 ± 4.21 | 0.026 | |
| CDAI score | 115.44 ± 75.06 | 114.80 ± 70.81 | 0.978 | |
| CDEIS score | 3.00 (8.25) | 2.00 (2.75) | 0.383 | |
| SES-CD score | 6.00 (9.75) | 3.00 (4.00) | 0.328 | |
| Vienna and Montreal classifications * | Class 3 in 72.22% | Class 3 in 50% | 0.484 | |
| Surgery (%) | 27.78 | 45 | / | |
| Rutgeerts | i0-22.2% i1-5.5% | i0-20% i1-25% | / | |
| BOP (%) | 34.61 ± 8.61 | 16.80 ± 5.49 | 0.000 | |
| PPD (mm) | 4.42 ± 1.11 | 3.07 ± 0.56 | 0.000 | |
| CAL (mm) | 3.15 ± 1.10 | 2.12 ± 0.40 | 0.001 | |
| RBL (%) | 22.00 (11.25) | 1.00 (2.00) | 0.000 | |
| Fecal calprotectin (ug/g) | 115.35 (934.20) | 104.60 (225.20) | 0.808 | |
| Hemoglobin (g/L) | 138.50 ± 25.55 | 133.05 ± 18.94 | 0.457 | |
| CRP (mg/L) | 4.45 (14.20) | 1.60 (7.65) | 0.149 | |
| Leucocytes (109/L) | 7.69 ± 3.68 | 7.44 ± 2.07 | 0.802 | |
| CD and PD Activity Parameters | Stages (Number of Patients) | ||||
|---|---|---|---|---|---|
| Stage I (n = 5) | Stage II (n = 9) | Stage III (n = 3) | Stage IV (n = 1) | p Value * | |
| CDAI (Median (IQR)) | 41 (74) | 137 (130.5) | 181 (/) | / | 0.062 |
| CDEIS (Median (IQR)) | 0 (3) | 2 (4.5) | 14 (/) | / | 0.017 |
| SES-CD (Median (IQR)) | 0 (6) | 3 (4.5) | 21 (/) | / | 0.016 |
| BOP (Median (IQR)) | 40 (15) | 30 (12.5) | 35 (/) | / | 0.332 |
| CAL (Median (IQR)) | 1.9 (1) | 3.2 (0.45) | 4.2 (/) | / | 0.001 |
| RBL (Median (IQR)) | 20 (8.5) | 23 (10) | 16 (/) | / | 0.618 |
| PPD (Median (IQR)) | 3.1 (0.6) | 4.7 (0.55) | 5.7 (/) | / | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Živić, M.; Zdravković, N.; Stojanović, B.; Milošević, B.; Todorović, Ž.; Adamović, M.; Zdravković, N. Association of Periodontal Disease with Activity of Crohn’s Disease. Medicina 2023, 59, 2154. https://doi.org/10.3390/medicina59122154
Živić M, Zdravković N, Stojanović B, Milošević B, Todorović Ž, Adamović M, Zdravković N. Association of Periodontal Disease with Activity of Crohn’s Disease. Medicina. 2023; 59(12):2154. https://doi.org/10.3390/medicina59122154
Chicago/Turabian StyleŽivić, Miloš, Nebojša Zdravković, Bojan Stojanović, Bojan Milošević, Željko Todorović, Miljan Adamović, and Nataša Zdravković. 2023. "Association of Periodontal Disease with Activity of Crohn’s Disease" Medicina 59, no. 12: 2154. https://doi.org/10.3390/medicina59122154
APA StyleŽivić, M., Zdravković, N., Stojanović, B., Milošević, B., Todorović, Ž., Adamović, M., & Zdravković, N. (2023). Association of Periodontal Disease with Activity of Crohn’s Disease. Medicina, 59(12), 2154. https://doi.org/10.3390/medicina59122154