
Beneficial Effects of IABP in Anterior Myocardial Infarction Complicated by Cardiogenic Shock

 ,
,  ,
, 
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Characteristics of Patients with Cardiogenic Shock
3.2. Mortality Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the Management of Acute Myocardial Infarction in Patients Presenting with ST-Segment Elevation. Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef]
- Hochman, J.S.; Sleeper, L.A.; Webb, J.G.; Sanborn, T.A.; White, H.D.; Talley, J.D.; Buller, C.E.; Jacobs, A.K.; Slater, J.N.; Col, J.; et al. Early Revascularization in Acute Myocardial Infarction Complicated by Cardiogenic Shock. N. Engl. J. Med. 1999, 341, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Panteleev, O.O.; Vyshlov, E.V.; Kercheva, M.A.; Ryabov, V.V. Analysis of results from intra-aortic balloon pump counterpulsation in patients with myocardial infarction and cardiogenic shock. Sib. J. Clin. Exp. Med. 2022, 37, 21–27. [Google Scholar] [CrossRef]
- Kimman, J.R.; Van Mieghem, N.M.; Endeman, H.; Brugts, J.J.; Constantinescu, A.A.; Manintveld, O.C.; Dubois, E.A.; den Uil, C.A. Mechanical support in early cardiogenic shock: What is the role of intra-aortic balloon counterpulsation? Curr. Heart Fail. Rep. 2020, 17, 247–260. [Google Scholar] [CrossRef]
- Babaev, A.; Frederick, P.D.; Pasta, D.J.; Every, N.; Sichrovsky, T.; Hochman, J.S.; NRMI Investigators. Trends in Management and Outcomes of Patients With Acute Myocardial Infarction Complicated by Cardiogenic Shock. JAMA 2005, 294, 448. [Google Scholar] [CrossRef]
- Mandawat, A.; Rao, S.V. Percutaneous Mechanical Circulatory Support Devices in Cardiogenic Shock. Circ. Cardiovasc. Interv. 2017, 10, 4337. [Google Scholar] [CrossRef]
- Cosentino, N.; Resta, M.L.; Somaschini, A.; Campodonico, J.; D’aleo, G.; Di Stefano, G.; Lucci, C.; Moltrasio, M.; Bonomi, A.; Cornara, S.; et al. ST-Segment Elevation Acute Myocardial Infarction Complicated by Cardiogenic Shock: Early Predictors of Very Long-Term Mortality. J. Clin. Med. 2021, 10, 2237. [Google Scholar] [CrossRef]
- Rossini, R.; Valente, S.; Colivicchi, F.; Baldi, C.; Caldarola, P.; Chiappetta, D.; Cipriani, M.; Ferlini, M.; Gasparetto, N.; Gilardi, R.; et al. ANMCO POSITION PAPER: Role of Intra-Aortic Balloon Pump in Patients with Acute Advanced Heart Failure and Cardiogenic Shock. Eur. Heart J. Suppl. 2021, 23, C204–C220. [Google Scholar] [CrossRef]
- Rihal, C.S.; Naidu, S.S.; Givertz, M.M.; Szeto, W.Y.; Burke, J.A.; Kapur, N.K.; Kern, M.; Garratt, K.N.; Goldstein, J.A.; Dimas, V.; et al. 2015 SCAI/ACC/HFSA/STS Clinical Expert Consensus Statement on the Use of Percutaneous Mechanical Circulatory Support Devices in Cardiovascular Care. J. Am. Coll. Cardiol. 2015, 65, e7–e26. [Google Scholar] [CrossRef]
- Kantrowitz, A.; Tjønneland, S.; Freed, P.S.; Phillips, S.J.; Butner, A.N.; Sherman, J.L. Initial Clinical Experience With Intraaortic Balloon Pumping in Cardiogenic Shock. JAMA J. Am. Med. Assoc. 1968, 203, 113–118. [Google Scholar] [CrossRef]
- Sjauw, K.D.; Engström, A.E.; Vis, M.M.; Van Der Schaaf, R.J.; Baan, J.; Koch, K.T.; De Winter, R.J.; Piek, J.J.; Tijssen, J.G.P.; Henriques, J.P.S. A Systematic Review and Meta-Analysis of Intra-Aortic Balloon Pump Therapy in ST-Elevation Myocardial Infarction: Should We Change the Guidelines? Eur. Heart J. 2009, 30, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Zeymer, U.; Neumann, F.J.; Ferenc, M.; Olbrich, H.G.; Hausleiter, J.; Richardt, G.; Hennersdorf, M.; Empen, K.; Fuernau, G.; et al. Intraaortic Balloon Support for Myocardial Infarction with Cardiogenic Shock. N. Engl. J. Med. 2012, 367, 1287–1296. [Google Scholar] [CrossRef]
- Combes, A.; Price, S.; Slutsky, A.S.; Brodie, D. Temporary Circulatory Support for Cardiogenic Shock. Lancet 2020, 396, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, Y.; Sen, S.; Shun-Shin, M.J.; Ouyang, J.; Finegold, J.A.; Al-Lamee, R.K.; Davies, J.E.R.; Cole, G.D.; Francis, D.P. Intra-Aortic Balloon Pump Therapy for Acute Myocardial Infarction: A Meta-Analysis. JAMA Intern. Med. 2015, 175, 931–939. [Google Scholar] [CrossRef] [PubMed]
- Gelsomino, S.; Johnson, D.M.; Lorusso, R. Intra-Aortic Balloon Pump: Is the Tide Turning? Crit. Care 2018, 18, 345. [Google Scholar] [CrossRef] [PubMed]
- Hawranek, M.; Gierlotka, M.; Pres, D.; Zembala, M.; Ga, M. Nonroutine Use of Intra-Aortic Balloon Pump in Cardiogenic Shock Complicating Myocardial Infarction With Successful and Unsuccessful Primary Percutaneous Coronary Intervention. JACC Cardiovasc. Interv. 2018, 11, 1885–1893. [Google Scholar] [CrossRef] [PubMed]
- Gul, B.; Bellumkonda, L. Usefulness of Intra-Aortic Balloon Pump in Patients With Cardiogenic Shock. Am. J. Cardiol. 2019, 123, 750–756. [Google Scholar] [CrossRef]
- van Nunen, L.X.; van ’t Veer, M.; Schampaert, S.; Rutten, M.C.M.; van de Vosse, F.N.; Patel, M.R.; Pijls, N.H.J. Intra-Aortic Balloon Counterpulsation Reduces Mortality in Large Anterior Myocardial Infarction Complicated by Persistent Ischaemia: A CRISP-AMI Substudy. EuroIntervention 2015, 11, 286–292. [Google Scholar] [CrossRef]
- Patel, M.R.; Smalling, R.W.; Thiele, H.; Barnhart, H.X.; Zhou, Y.; Chandra, P.; Chew, D.; Cohen, M.; French, J.; Perera, D.; et al. Intra-Aortic Balloon Counterpulsation and Infarct Size in Patients with Acute Anterior Myocardial Infarction without Shock: The CRISP AMI Randomized Trial. JAMA J. Am. Med. Assoc. 2011, 306, 1329–1337. [Google Scholar] [CrossRef]
- Marenzi, G.; Cosentino, N.; Moltrasio, M.; Rubino, M.; Crimi, G.; Buratti, S.; Grazi, M.; Milazzo, V.; Somaschini, A.; Camporotondo, R.; et al. Acute Kidney Injury Definition and In-Hospital Mortality in Patients Undergoing Primary Percutaneous Coronary Intervention for ST-Segment Elevation Myocardial Infarction. J. Am. Heart Assoc. 2016, 5, e003522. [Google Scholar] [CrossRef]
- Chesebro, J.H.; Knatterud, G.; Roberts, R.; Borer, J.; Cohen, L.S.; Dalen, J.; Dodge, H.T.; Francis, C.K.; Hillis, D.; Ludbrook, P.; et al. Thrombolysis in Myocardial Infarction (TIMI) Trial, Phase I: A Comparison between Intravenous Tissue Plasminogen Activator and Intravenous Streptokinase* Clinical Findings through Hospital Discharge. Circulation 1987, 76, 142–154. [Google Scholar] [CrossRef] [PubMed]
- van’t Hof, A.W.; ten Berg, J.; Heestermans, T.; Dill, T.; Funck, R.C.; van Werkum, W.; Dambrink, J.H.E.; Suryapranata, H.; van Houwelingen, G.; Ottervanger, J.P.; et al. Prehospital Initiation of Tirofiban in Patients with ST-Elevation Myocardial Infarction Undergoing Primary Angioplasty (On-TIME 2): A Multicentre, Double-Blind, Randomised Controlled Trial. Lancet 2008, 372, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Montalescot, G.; Van’t Hof, A.W.; Lapostolle, F.; Silvain, J.; Flensted Lassen, J.; Bolognese, L.; Cantor, W.J.; Cequier, Á.; Chettibi, M.; Goodman, S.G.; et al. Prehospital Ticagrelor in ST-Segment Elevation Myocardial Infarction. N. Engl. J. Med. 2014, 371, 1016–1043. [Google Scholar] [CrossRef]
- Somaschini, A.; Cornara, S.; Ferlini, M.; Crimi, G.; Camporotondo, R.; Gnecchi, M.; Ferrario Ormezzano, M.; Oltrona Visconti, L.; De Ferrari, G.M.; De Servi, S. Favorable Effect of Glycoprotein IIbIIIa Inhibitors among STEMI Patients Treated with Primary PCI and Incomplete ST Resolution. Platelets 2020, 31, 48–54. [Google Scholar] [CrossRef]
- Dhruva, S.S.; Ross, J.S.; Mortazavi, B.J.; Hurley, N.C.; Krumholz, H.M.; Curtis, J.P.; Berkowitz, A.; Masoudi, F.A.; Messenger, J.C.; Parzynski, C.S.; et al. Association of Use of an Intravascular Microaxial Left Ventricular Assist Device vs Intra-Aortic Balloon Pump with In-Hospital Mortality and Major Bleeding among Patients with Acute Myocardial Infarction Complicated by Cardiogenic Shock. JAMA J. Am. Med. Assoc. 2020, 323, 734–745. [Google Scholar] [CrossRef] [PubMed]
- Seyfarth, M.; Sibbing, D.; Bauer, I.; Fröhlich, G.; Bott-Flügel, L.; Byrne, R.; Dirschinger, J.; Kastrati, A.; Schömig, A. A Randomized Clinical Trial to Evaluate the Safety and Efficacy of a Percutaneous Left Ventricular Assist Device Versus Intra-Aortic Balloon Pumping for Treatment of Cardiogenic Shock Caused by Myocardial Infarction. J. Am. Coll. Cardiol. 2008, 4, 1584–1588. [Google Scholar] [CrossRef] [PubMed]
- Schrage, B.; Ibrahim, K.; Loehn, T.; Werner, N.; Sinning, J.M.; Pappalardo, F.; Pieri, M.; Skurk, C.; Lauten, A.; Landmesser, U.; et al. Impella Support for Acute Myocardial Infarction Complicated by Cardiogenic Shock: Matched-Pair Iabp-Shock II Trial 30-Day Mortality Analysis. Circulation 2019, 139, 1249–1258. [Google Scholar] [CrossRef]
- Ouweneel, D.M.; Eriksen, E.; Seyfarth, M.; Henriques, J.P.S. Percutaneous Mechanical Circulatory Support Versus Intra-Aortic Balloon Pump for Treating Cardiogenic Shock: Meta-Analysis. J. Am. Coll. Cardiol. 2017, 24, 358–360. [Google Scholar] [CrossRef]
- Kuno, T.; Takagi, H.; Ando, T.; Kodaira, M.; Numasawa, Y.; Fox, J.; Bangalore, S. Safety and Efficacy of Mechanical Circulatory Support with Impella or intra-aortic Balloon Pump for high-risk Percutaneous Coronary Intervention and/or Cardiogenic Shock: Insights from a Network meta-analysis of Randomized Trials. Catheter. Cardiovasc. Interv. 2020, 97, E636–E645. [Google Scholar] [CrossRef]
- Thiele, H.; Zeymer, U.; Neumann, F.-J.; Ferenc, M.; Olbrich, H.-G.; Hausleiter, J.; de Waha, A.; Richardt, G.; Hennersdorf, M.; Empen, K.; et al. Intra-Aortic Balloon Counterpulsation in Acute Myocardial Infarction Complicated by Cardiogenic Shock (IABP-SHOCK II): Final 12 Month Results of a Randomised, Open-Label Trial. Lancet 2013, 382, 1638–1645. [Google Scholar] [CrossRef]
- Thiele, H.; Zeymer, U.; Thelemann, N.; Neumann, F.J.; Hausleiter, J.; Abdel-Wahab, M.; Meyer-Saraei, R.; Fuernau, G.; Eitel, I.; Hambrecht, R.; et al. Intraaortic Balloon Pump in Cardiogenic Shock Complicating Acute Myocardial Infarction: Long-Term 6-Year Outcome of the Randomized IABP-SHOCK II Trial. Circulation 2019, 139, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Hanlon-Pena, P.M.; Quaal, S.J. Intra-Aortic Balloon Pump Timing: Review of Evidence Supporting Current Practice. Am. J. Crit. Care 2011, 20, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Kapur, N.K.; Alkhouli, M.A.; DeMartini, T.J.; Faraz, H.; George, Z.H.; Goodwin, M.J.; Hernandez-Montfort, J.A.; Iyer, V.S.; Josephy, N.; Kalra, S.; et al. Unloading the Left Ventricle Before Reperfusion in Patients With Anterior ST-Segment–Elevation Myocardial Infarction. Circulation 2019, 139, 337–346. [Google Scholar] [CrossRef] [PubMed]
- De Silva, K.; Lumley, M.; Kailey, B.; Alastruey, J.; Guilcher, A.; Asrress, K.N.; Plein, S.; Marber, M.; Redwood, S.; Perera, D. Coronary and Microvascular Physiology during Intra-Aortic Balloon Counterpulsation. JACC Cardiovasc. Interv. 2014, 7, 631–640. [Google Scholar] [CrossRef]
- Fuernau, G.; Ledwoch, J.; Desch, S.; Eitel, I.; Thelemann, N.; Jung, C.; de Waha-Thiele, S.; Pöss, J.; Feistritzer, H.-J.; Freund, A.; et al. Impact of Timing of Intraaortic Balloon Counterpulsation on Mortality in Cardiogenic Shock—A Subanalysis of the IABP-SHOCK II Trial. Eur. Heart J. Acute Cardiovasc. Care 2020, 10, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.M.; van Leeuwen, M.A.H.; de Boer, S.P.M.; Wai, M.C.G.T.J.; den Uil, C.A.; Jewbali, L.S.D.; van Geuns, R.-J.; Kardys, I.; van Domburg, R.T.; Boersma, E.; et al. Impact of Intra-Aortic Balloon Pump Support Initiated before versus after Primary Percutaneous Coronary Intervention in Patients with Cardiogenic Shock from Acute Myocardial Infarction. Int. J. Cardiol. 2013, 168, 3758–3763. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Demographic Variables | STEMI (n = 2959) | STEMI + Cardiogenic Shock (n = 246) | p Value |
|---|---|---|---|
| Age (years; median (Q1–Q3)) | 63 (54–73) | 69.5 (60–77) | <0.001 |
| Age > 75 years (n, %) | 613 (20.4%) | 83 (33.7%) | <0.001 |
| Female sex (n, %) | 663 (22%) | 75 (30.5%) | <0.001 |
| Body mass index (kg/m2; median (Q1–Q3)) | 25.8 (23.4–28.7) | 24.2 (22.8–26.2) | <0.001 |
| CV risk factors | |||
| Smoke (n, %) | 1861 (63.1%) | 94 (38.5%) | <0.001 |
| Hypertension (n, %) | 1631 (55.3%) | 46 (60.1%) | <0.001 |
| Type II diabetes mellitus (n, %) | 496 (16.8%) | 46 (18.9%) | <0.001 |
| Dyslipidemia (n, %) | 1162 (39%) | 55 (22.6%) | <0.001 |
| Family history of cardiovascular disease (n, %) | 966 (32.8%) | 39 (16%) | <0.001 |
| Medical history | |||
| Peripheral arterial disease (n, %) | 312 (10.4%) | 47 (19.4%) | <0.001 |
| Previous myocardial infarction (n, %) | 392 (13.3%) | 40 (16.4%) | 0.056 |
| Previous percutaneous coronary intervention (n, %) | 357 (12.1%) | 33 (13.5%) | 0.199 |
| Previous coronary artery bypass grafting (n, %) | 53 (1.8%) | 8 (3.3%) | 0.712 |
| Chronic kidney disease (n, %) | 642 (21.4%) | 105 (52.8%) | <0.001 |
| Clinical and laboratory variables | |||
| Out of hospital cardiac arrest (n, %) | 284 (9.8%) | 92 (37.9%) | <0.001 |
| Anemia (n, %) | 528 (8.1%) | 106 (45.5%) | <0.001 |
| Heart rate (bpm; median (Q1–Q3)) | 75 (65–87) | 80 (67–99) | 0.001 |
| Left ventricular ejection fraction (median(Q1–Q3)) | 45 (38–50) | 35 (25–40) | <0.001 |
| Systolic arterial pressure (mmHg; median (Q1–Q3)) | 135 (120–150) | 90 (75–103) | <0.001 |
| Baseline blood sugar (mg/dL; median (Q1–Q3)) | 141 (120–176) | 175 (136–219) | <0.001 |
| Hyperglycemia (n,%) | 469 (16.5%) | 95 (43%) | <0.001 |
| Baseline hemoglobin (g/dL; median (Q1–Q3)) | 14.3 (13.5–15.3) | 13.6 (12–14.7) | <0.001 |
| Baseline white blood cells (n × 103/mcl; median (Q1–Q3)) | 11.2 (8.8–13.7) | 13.3 (9.5–20) | <0.001 |
| Troponin I peak (ng/dL; median (Q1–Q3)) | 80 (32–166) | 196 (81–355) | 0.001 |
| Creatine kinase peak (MU/L; median (Q1–Q3)) | 1.3 (0.6–2.4) | 2.8 (1.3–5.6) | <0.001 |
| Baseline creatinine (mg/dL; median (Q1–Q3)) | 0.9 (0.8–1.1) | 1 (0.8–1.3) | <0.001 |
| ECG | |||
| Anterior STEMI (n, %) | 1240 (46.5%) | 145 (59.7%) | <0.001 |
| ST resolution (n, %) | 1908 (69.9%) | 98 (49%) | <0.001 |
| Procedural data | |||
| Three-vessel disease (n, %) | 772 (26.4%) | 86 (36.3%) | 0.001 |
| Left main involvement (n, %) | 32 (1.1%) | 18 (8.1%) | <0.001 |
| Blood pressure ≤ 90 mmHg in the cath-lab (n,%) | 90 (3.1%) | 46 (20.3%) | <0.001 |
| Post-procedural TIMI flow <3 (n, %) | 278 (9.3%) | 56 (23.5%) | <0.001 |
| Length of stay | |||
| Coronary care unit (days; median (Q1–Q3)) | 4 (3–5) | 6 (2–10) | <0.001 |
| Hospital (days; median (Q1–Q3)) | 7 (6–9) | 9 (4–14) | <0.001 |
| Variables | Anterior STEMI | p-Value | |
|---|---|---|---|
| NO (n = 101) | YES (n = 145) | ||
| Age > 75 years (n, %) | 39 (39.8%) | 44 (30.1%) | 0.128 |
| Female sex (n, %) | 34 (34.7%) | 39 (26.9%) | 0.193 |
| Type II diabetes mellitus (n, %) | 21 (21.9%) | 25 (17.4%) | 0.348 |
| Heart rate (bpm; median (Q1–Q3)) | 73 (62–82) | 80 (68–88) | <0.001 |
| Anemia (n, %) | 43 (46.7%) | 61 (44.2%) | 0.075 |
| Out of hospital cardiac arrest (n, %) | 29 (30.2%) | 61 (42.4%) | 0.057 |
| Hyperglycemia (n, %) | 34 (39.5%) | 59 (44.7%) | 0.451 |
| Creatine kinase peak (Mu/L; median (Q1–Q3)) | 1.2 (0.6–2.1) | 1.7 (0.8–3) | <0.001 |
| Baseline white blood cells (n × 103/mcl; median (Q1–Q3)) | 10.8 (8.7–13.1) | 11.5 (9–14.2) | <0.001 |
| Left ventricular ejection fraction (%; median(Q1–Q3)) | 40 (30–47) | 27 (20–37.5) | <0.001 |
| Contrast-induced acute kidney injury (n, %) | 5 (5.4%) | 13 (9.3%) | <0.001 |
| Bleeding (n, %) | 9 (9.6%) | 22 (15.6%) | <0.001 |
| Three-vessel disease (n, %) | 33 (34.7%) | 53 (38.1%) | 0.597 |
| Left main involvement (n, %) | 1(1.2%) | 16 (11.9%) | 0.004 |
| Systolic blood pressure < 90 mmHg in the cath-lab (n, %) | 23 (25%) | 22 (16.7%) | 0.126 |
| Post-procedural TIMI flow <3 (n, %) | 23 (23.7%) | 32 (23.2%) | 0.926 |
| ST resolution (n, %) | 78 (78%) | 88 (61%) | <0.001 |
| Variables | IABP | p-Value | |
|---|---|---|---|
| NO (n = 58) | YES (n = 87) | ||
| Age (years; median (Q1–Q3)) | 74 (68–82) | 67 (58–74) | <0.001 |
| Age > 75 years (n, %) | 22 (39.3%) | 21 (24.1%) | 0.054 |
| Body mass index (kg/m2, median (Q1–Q3)) | 24.2 (22.8–26.9) | 24.5 (22.8–28.7) | 0.535 |
| Female sex (%) | 16 (28.6%) | 21 (24.1%) | 0.555 |
| Hypertension (%) | 35 (62.5%) | 44 (51.2%) | 0.184 |
| Type II diabetes mellitus (%) | 7 (12.5%) | 18 (20.9%) | 0.197 |
| Anemia (n, %) | 29 (55.8%) | 32 (37.6%) | 0.038 |
| Previous myocardial infarction (%) | 12 (21.4%) | 13 (14.9%) | 0.319 |
| Peripheral arterial disease (%) | 16 (27.8%) | 12 (14%) | 0.044 |
| Out of hospital cardiac arrest (%) | 19 (34.5%) | 40 (46.5%) | 0.178 |
| Heart rate (bpm; median (Q1–Q3)) | 80 (72–102) | 91 (69–109) | 0.706 |
| Baseline blood sugar (mg/dL; median (Q1–Q3)) | 141 (133–181) | 214 (176–263) | 0.005 |
| Left ventricular ejection fraction (median(Q1–Q3)) | 30 (25–40) | 25 (20–35) | 0.041 |
| Baseline hemoglobin (g/dL; median (Q1–Q3)) | 12.3 (11.4–15.1) | 13.9 (12.4–15.1) | 0.058 |
| Baseline platelets (Mu/L, median (Q1–Q3)) | 232 (206–266) | 246 (203–304) | 0.276 |
| Platelets nadir (Mu/L, median (Q1–Q3)) | 188 (159–228) | 137 (101–200) | <0.001 |
| Baseline white blood cells (n × 103/mcl; median (Q1–Q3)) | 12.49 (9.8–16.4) | 14.6 (11.4–21.3) | 0.013 |
| Hyperglycemia (n, %) | 16 (31.4%) | 42 (52.5%) | 0.018 |
| Creatine kinase peak (mg/dMU/L; median (Q1–Q3)) | 2.83 (1.04–4.34) | 4.06 (2.7–7.1) | 0.001 |
| Baseline eGFR * (mg/mL, median (Q1–Q3)) | 44 (36–74) | 65 (43–88) | 0.087 |
| Systolic blood pressure < 90 mmHg in the cath-lab (n, %) | 3 (5.4%) | 19 (25%) | 0.003 |
| Three-vessel disease (%) | 22 (40%) | 31 (37.3%) | 0.754 |
| Left main involvement (n, %) | 2 (3.7%) | 12 (15.2%) | 0.034 |
| ST resolution (%) | 17 (34.7%) | 32 (50%) | 0.104 |
| CI-AKI 0.5 (%) | 14 (26.4%) | 21 (25%) | 0.853 |
| Post-procedural TIMI flow <3 (%) | 13 (23.6%) | 18 (22%) | 0.817 |
| GP IIbIIIa—inhibitors use (%) | 19 (37.3%) | 43 (52.4%) | 0.088 |
| Days in Coronary Care Unit (days; median (Q1–Q3)) | 7 (4–10) | 6 (4–10) | 0.219 |
| Days in hospital (days; median (Q1–Q3)) | 8 (6–15) | 12 (8–19) | 0.003 |
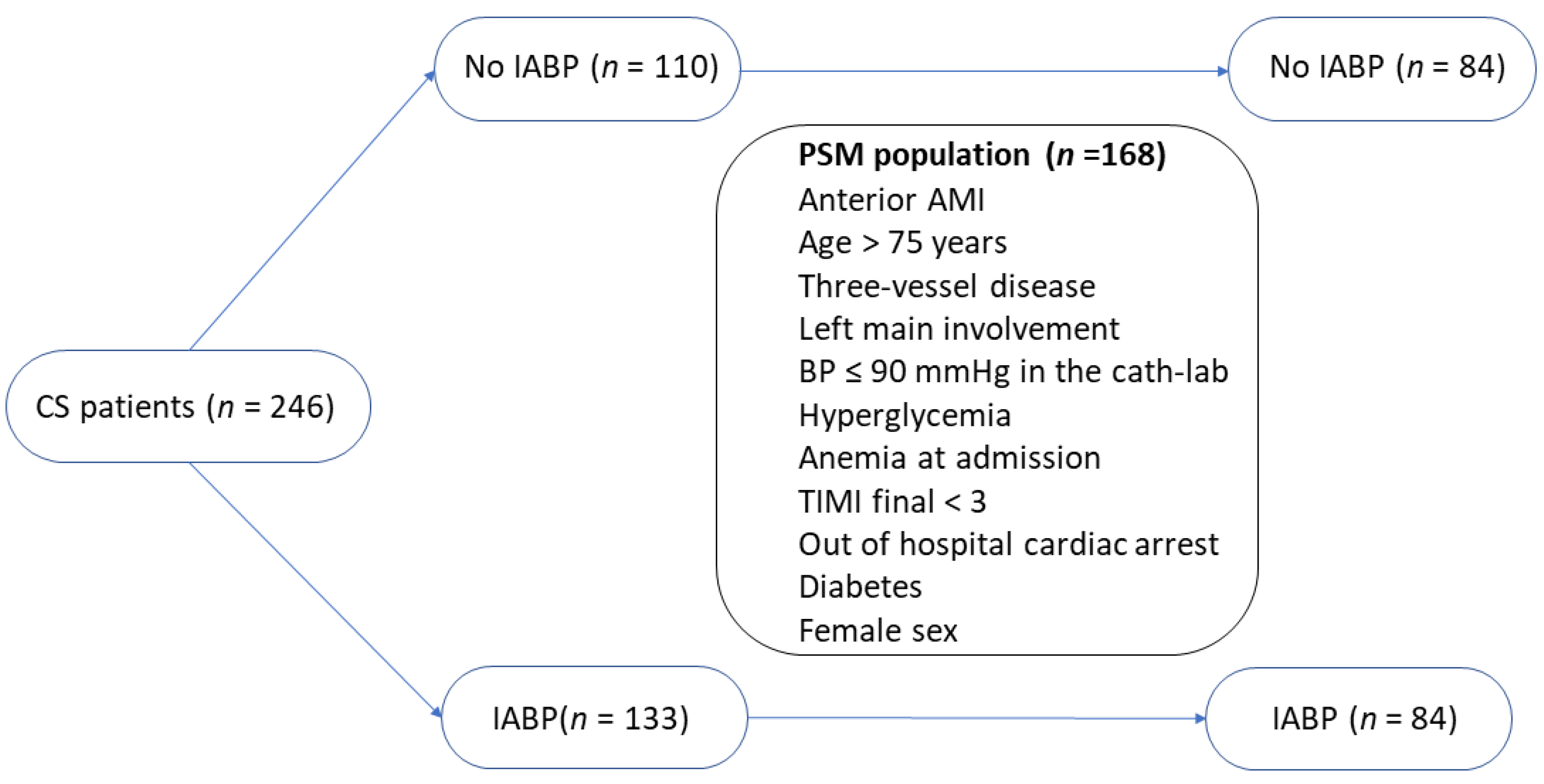
| Variables Included in the PMS | IABP | p-Value | |
|---|---|---|---|
| NO (n = 84) | YES (n = 84) | ||
| Age > 75 years (%) | 30 (37.5%) | 26 (29.5%) | 0.275 |
| Anterior myocardial infarction (%) | 46 (57.5%) | 56 (63.6%) | 0.416 |
| Three-vessel disease (%) | 26 (32.5%) | 32 (36.4%) | 0.599 |
| Left main involvement (%) | 2 (2.5%) | 6 (6.8%) | 0.189 |
| Systolic blood pressure < 90 mmHg in the cath-lab (n, %) | 60 (62.5%) | 66 (75%) | 0.080 |
| Hyperglycemia at admission (%) | 26 (32.5%) | 44 (50%) | 0.022 |
| Anemia at admission (%) | 41 (51.2%) | 34 (38.6%) | 0.100 |
| Post-procedural TIMI flow <3 (%) | 17 (21.3%) | 20 (22.7%) | 0.817 |
| Out of hospital cardiac arrest (%) | 23 (28.7%) | 18 (20.5%) | 0.211 |
| Type II diabetes mellitus (%) | 11 (13.8%) | 22 (25%) | 0.067 |
| Female sex (%) | 24 (30%) | 27 (30.7%) | 0.924 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Somaschini, A.; Cornara, S.; Leonardi, S.; Demarchi, A.; Mandurino-Mirizzi, A.; Fortuni, F.; Ferlini, M.; Crimi, G.; Camporotondo, R.; Gnecchi, M.; et al. Beneficial Effects of IABP in Anterior Myocardial Infarction Complicated by Cardiogenic Shock. Medicina 2023, 59, 1806. https://doi.org/10.3390/medicina59101806
Somaschini A, Cornara S, Leonardi S, Demarchi A, Mandurino-Mirizzi A, Fortuni F, Ferlini M, Crimi G, Camporotondo R, Gnecchi M, et al. Beneficial Effects of IABP in Anterior Myocardial Infarction Complicated by Cardiogenic Shock. Medicina. 2023; 59(10):1806. https://doi.org/10.3390/medicina59101806
Chicago/Turabian StyleSomaschini, Alberto, Stefano Cornara, Sergio Leonardi, Andrea Demarchi, Alessandro Mandurino-Mirizzi, Federico Fortuni, Marco Ferlini, Gabriele Crimi, Rita Camporotondo, Massimiliano Gnecchi, and et al. 2023. "Beneficial Effects of IABP in Anterior Myocardial Infarction Complicated by Cardiogenic Shock" Medicina 59, no. 10: 1806. https://doi.org/10.3390/medicina59101806
APA StyleSomaschini, A., Cornara, S., Leonardi, S., Demarchi, A., Mandurino-Mirizzi, A., Fortuni, F., Ferlini, M., Crimi, G., Camporotondo, R., Gnecchi, M., Oltrona Visconti, L., De Servi, S., & De Ferrari, G. M. (2023). Beneficial Effects of IABP in Anterior Myocardial Infarction Complicated by Cardiogenic Shock. Medicina, 59(10), 1806. https://doi.org/10.3390/medicina59101806