
Ten-Year Change in Disorders of Consciousness: A Bibliometric Analysis


Abstract
1. Introduction
- (1)
- What is the knowledge structure of the current research system on DoC?
- (2)
- What is the focus of current research on DoC?
- (3)
- What are the possible directions for future research on DoC?
2. Materials and Methods
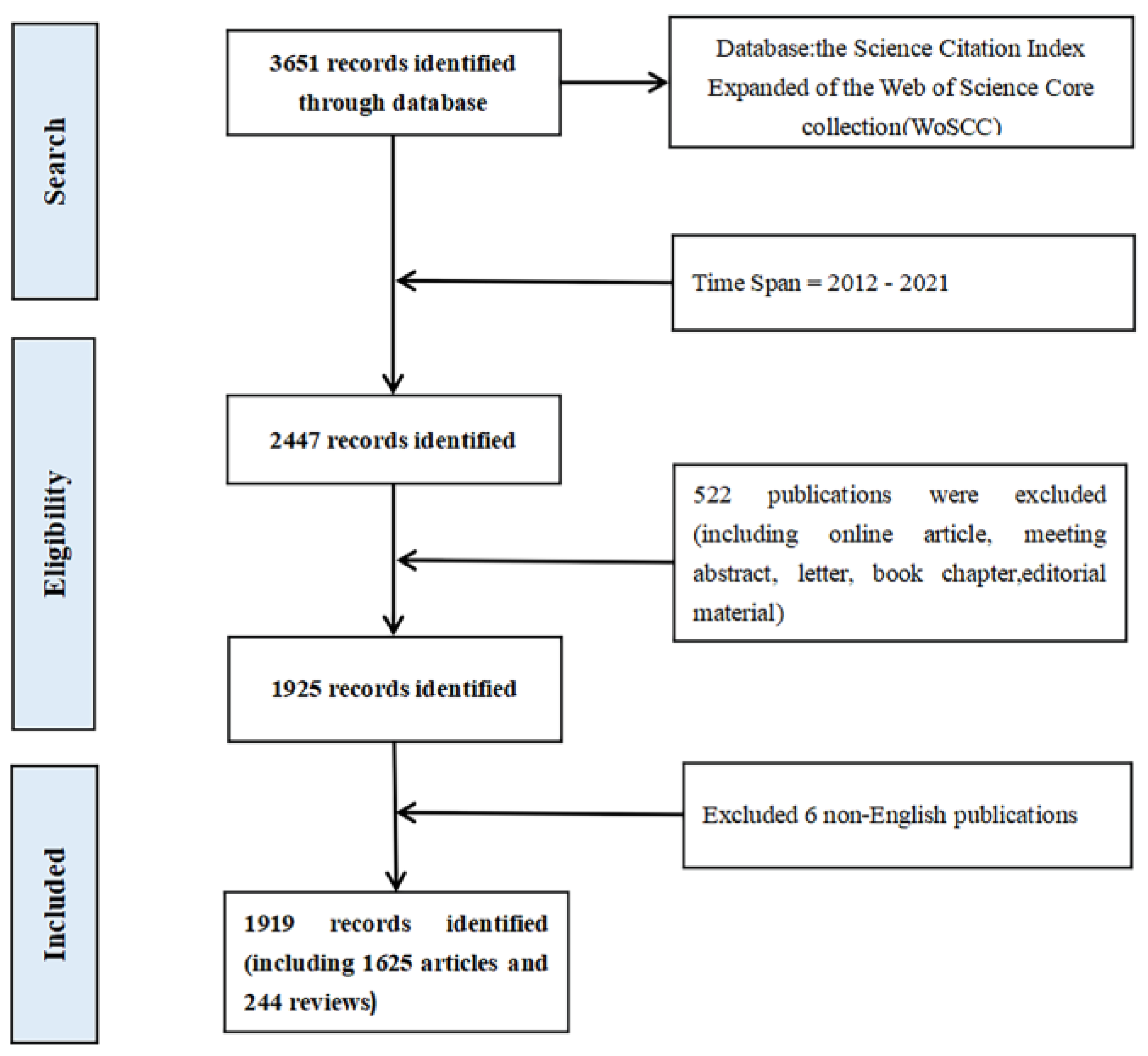
2.1. Data Collection
2.2. Inclusion Criteria
2.3. Analytical Methods
3. Result
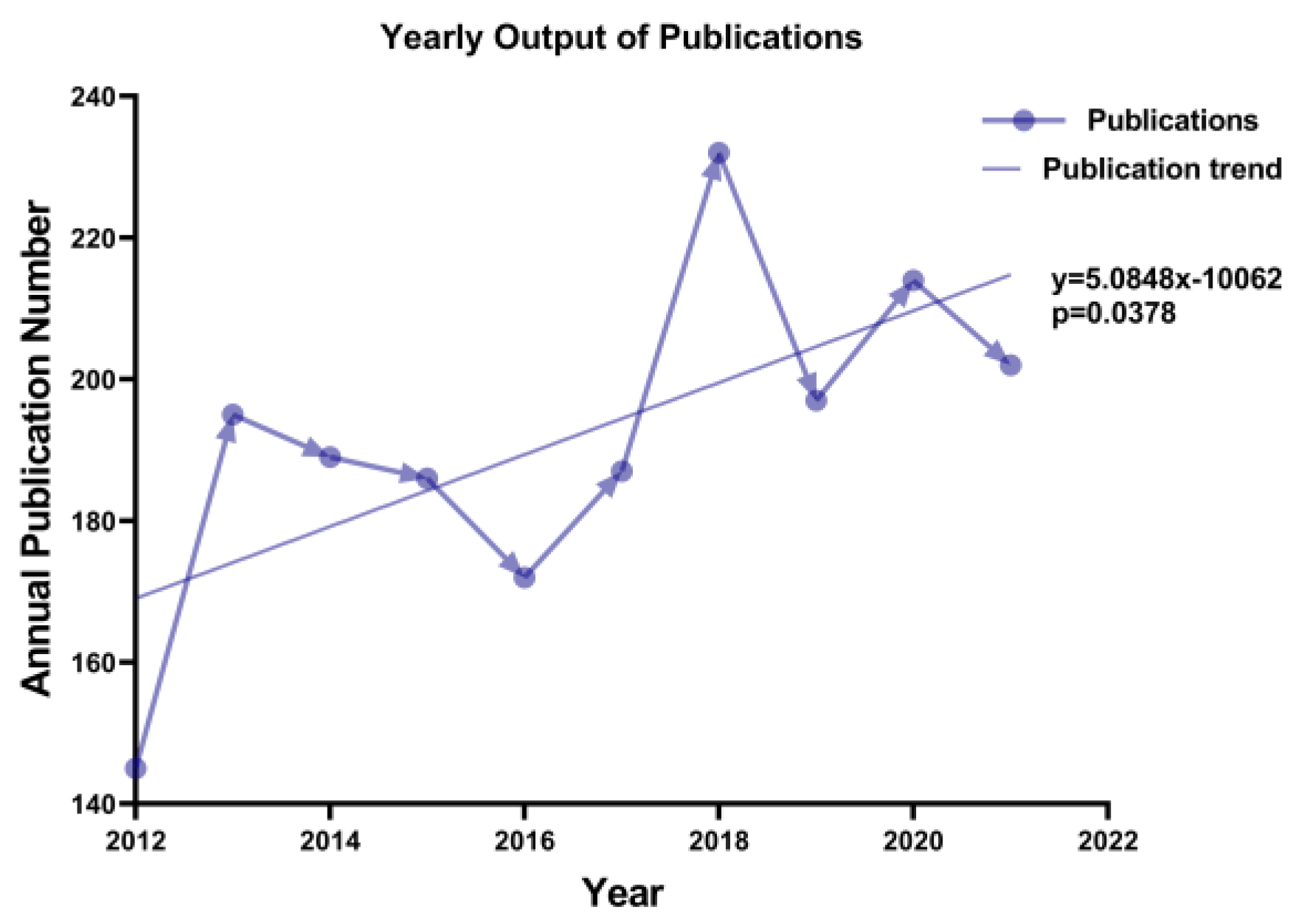
3.1. Publication Output and Time Trend
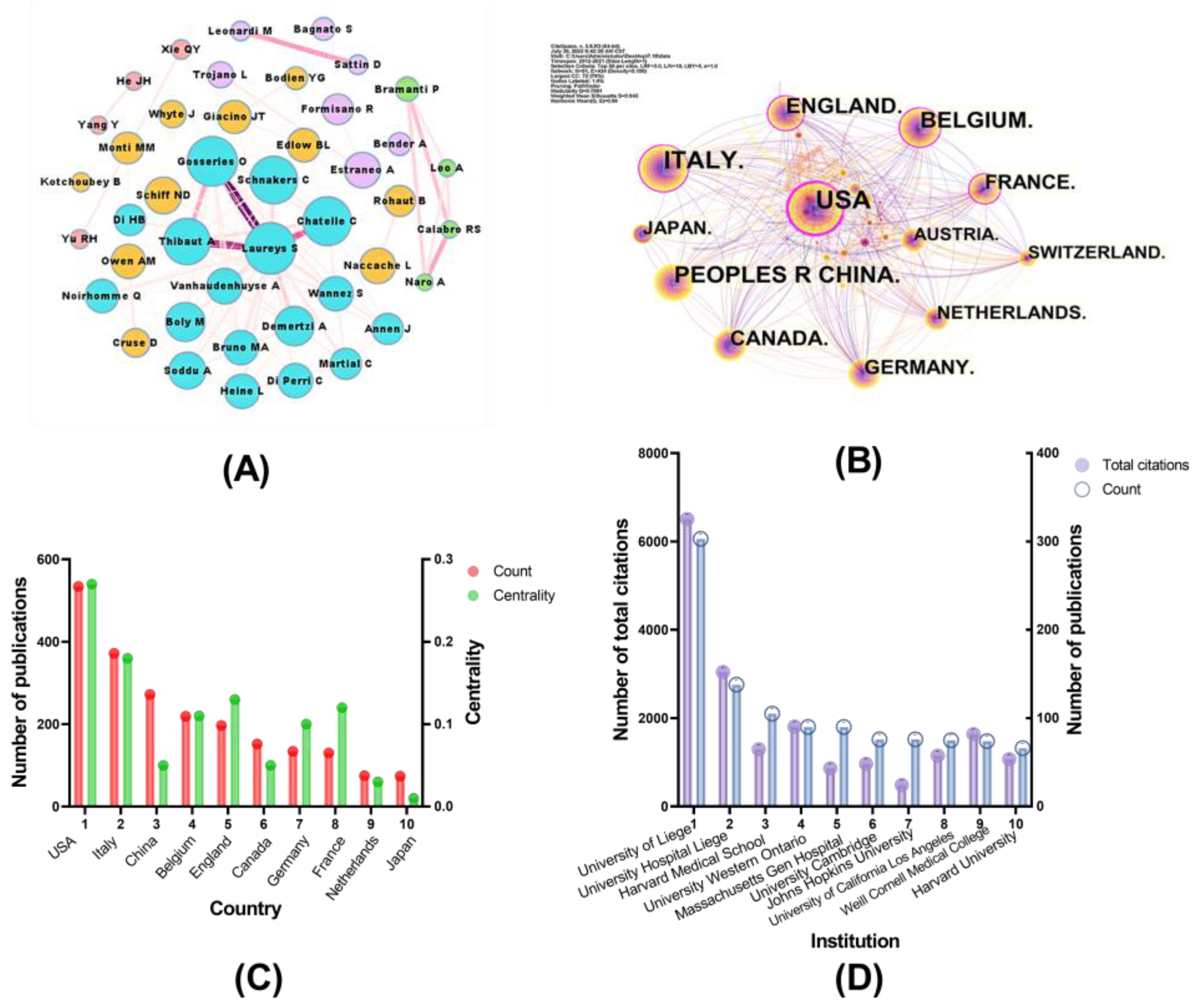
3.2. Author Cooperation and Co-Authors Analysis
3.3. Countries and Institutions Analysis
3.4. Journal Distribution and Co-Citation Analysis
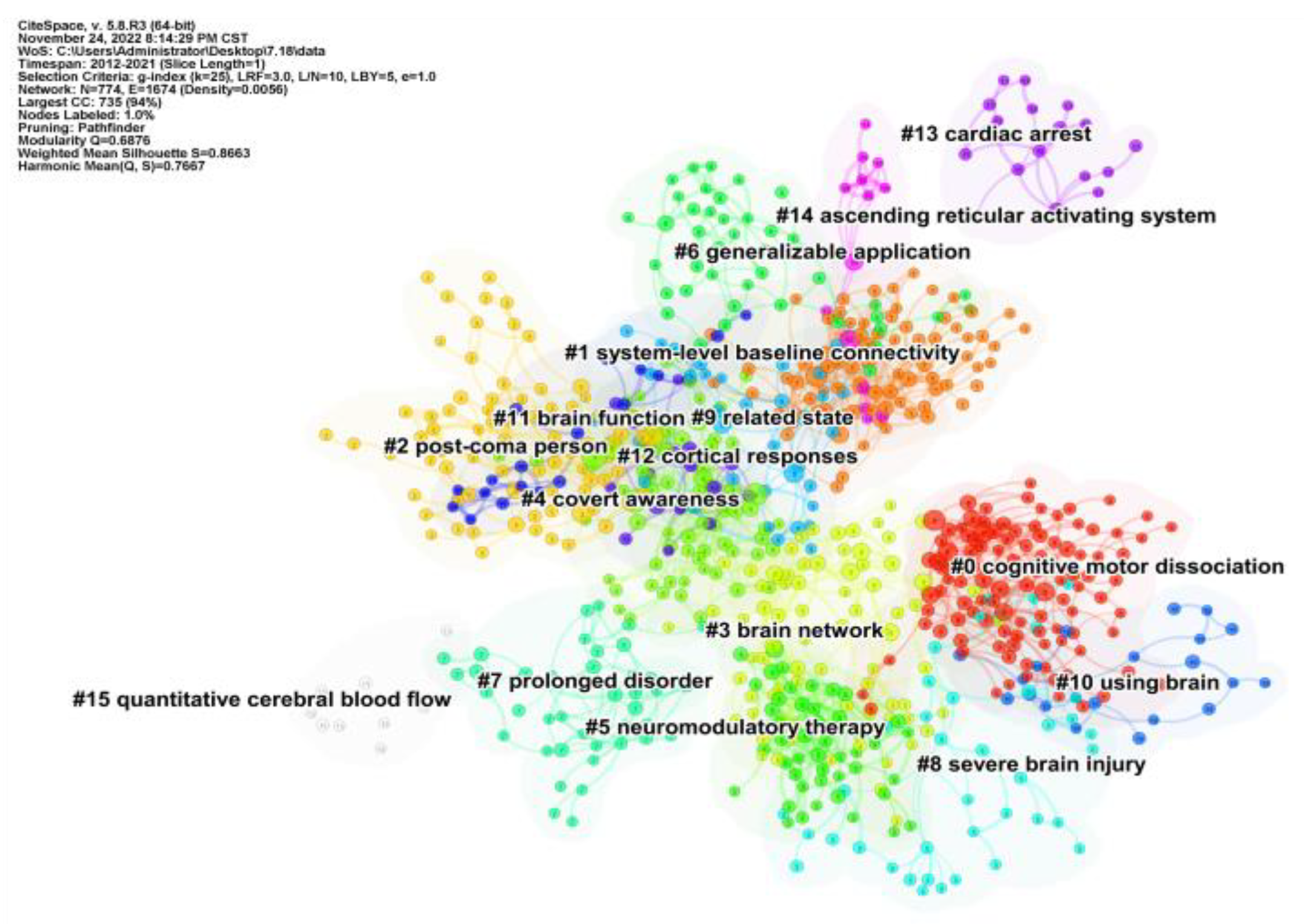
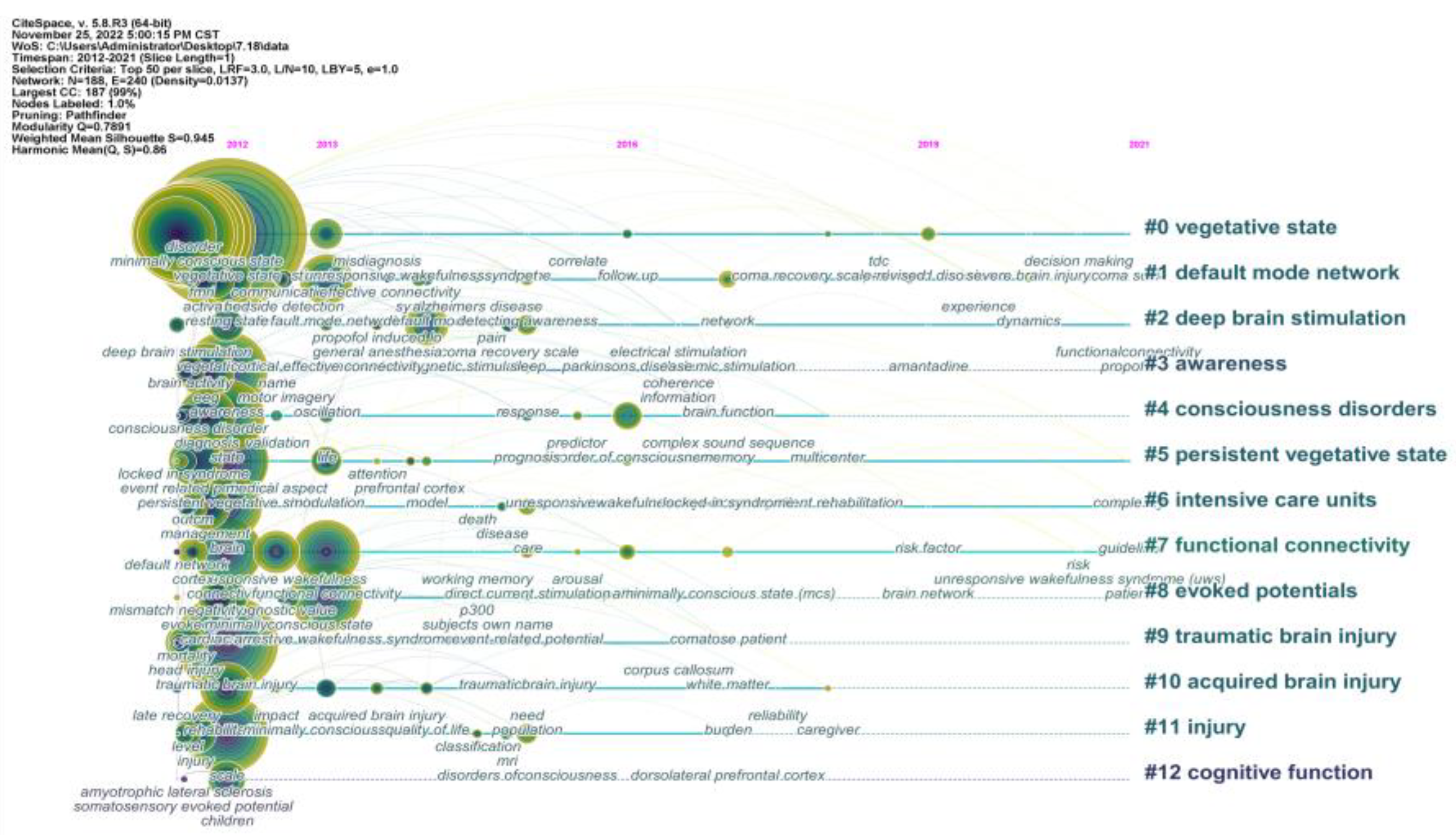
3.5. Reference Co-Citation Analysis
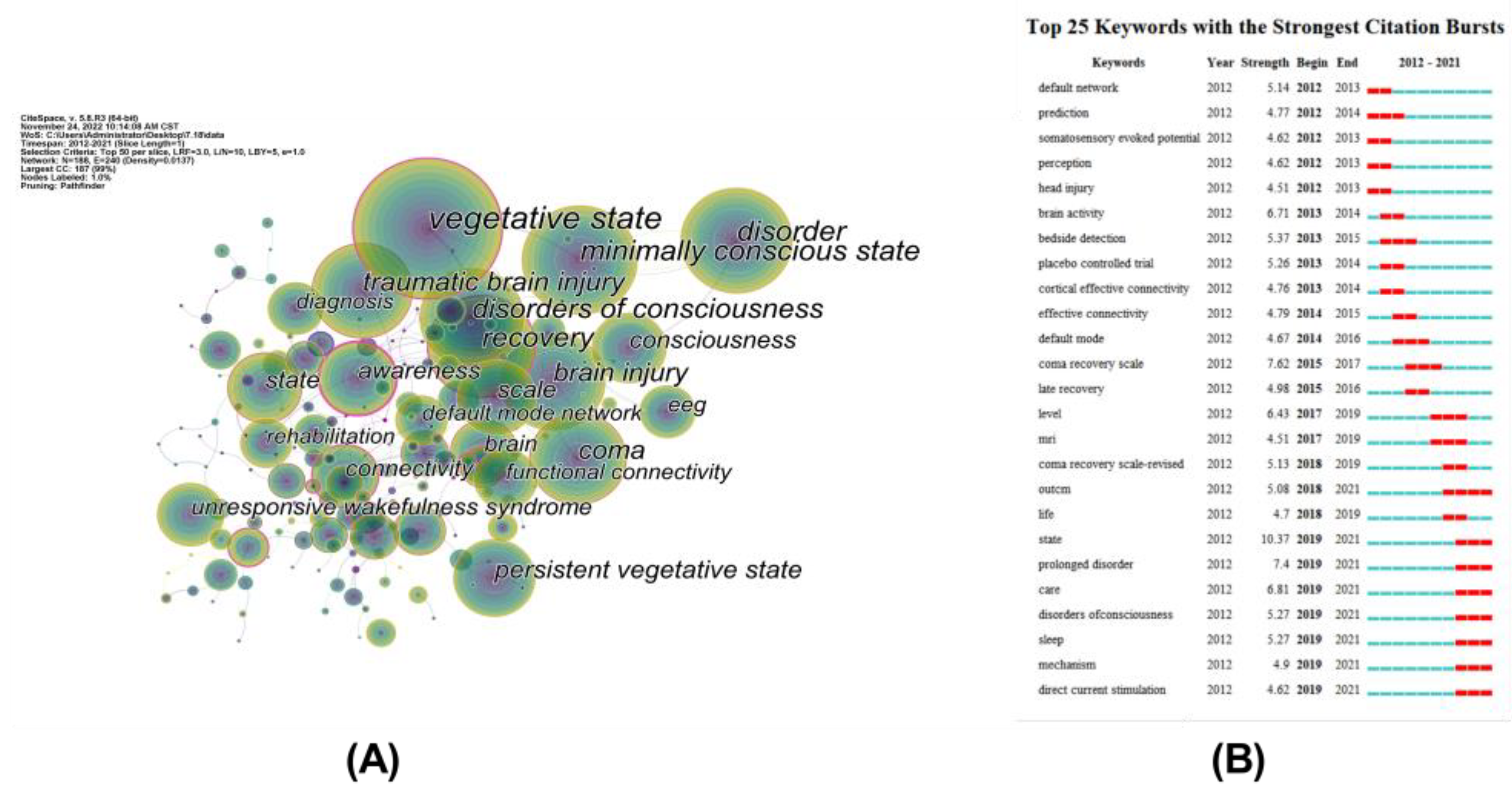
3.6. Keywords Co-Occurring Analysis and Citation Bursts
4. Discussion
4.1. Intellectual Structure of Publications on DoC
4.2. Recent Hot Issues in DoC Research
4.2.1. Diagnosing the Level of Consciousness in DoC Patients
4.2.2. Detecting Residual Awareness after Early Brain Injury at the ICU Bedside
4.3. Emerging Trends of DoC Research
4.3.1. Exploring the Mechanism of Consciousness Recovery
4.3.2. Neuromodulation Interventions for DoC Patients
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giacino, J.T.; Schnakers, C.; Rodriguez-Moreno, D.; Kalmar, K.; Schiff, N.; Hirsch, J. Behavioral Assessment in Patients with Disorders of Consciousness: Gold Standard or Fool’s Gold? In Progress in Brain Research; Laureys, S., Schiff, N.D., Owen, A.M., Eds.; Elsevier: Amsterdam, The Netherlands, 2009; Volume 177, pp. 33–48. [Google Scholar]
- Gosseries, O.; Bruno, M.-A.; Chatelle, C.; Vanhaudenhuyse, A.; Schnakers, C.; Soddu, A.; Laureys, S. Disorders of Consciousness: What’s in a Name? NeuroRehabilitation 2011, 28, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Giacino, J.T.; Fins, J.J.; Laureys, S.; Schiff, N.D. Disorders of Consciousness after Acquired Brain Injury: The State of the Science. Nat. Rev. Neurol. 2014, 10, 99–114. [Google Scholar] [CrossRef] [PubMed]
- Edlow, B.L.; Claassen, J.; Schiff, N.D.; Greer, D.M. Recovery from Disorders of Consciousness: Mechanisms, Prognosis and Emerging Therapies. Nat. Rev. Neurol. 2021, 17, 135–156. [Google Scholar] [CrossRef]
- Giacino, J.T.; Ashwal, S.; Childs, N.; Cranford, R.; Jennett, B.; Katz, D.I.; Kelly, J.P.; Rosenberg, J.H.; Whyte, J.; Zafonte, R.D.; et al. The Minimally Conscious State: Definition and Diagnostic Criteria. Neurology 2002, 58, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Schnakers, C.; Vanhaudenhuyse, A.; Giacino, J.; Ventura, M.; Boly, M.; Majerus, S.; Moonen, G.; Laureys, S. Diagnostic Accuracy of the Vegetative and Minimally Conscious State: Clinical Consensus versus Standardized Neurobehavioral Assessment. BMC Neurol. 2009, 9, 35. [Google Scholar] [CrossRef]
- Chen, C.; Dubin, R.; Kim, M.C. Emerging Trends and New Developments in Regenerative Medicine: A Scientometric Update (2000–2014). Expert Opin. Biol. Ther. 2014, 14, 1295–1317. [Google Scholar] [CrossRef] [PubMed]
- Garnett, A.; Lee, G.; Illes, J. Publication Trends in Neuroimaging of Minimally Conscious States. PeerJ 2013, 1, e155. [Google Scholar] [CrossRef] [PubMed]
- Chen, C. CiteSpace II: Detecting and Visualizing Emerging Trends and Transient Patterns in Scientific Literature. J. Am. Soc. Inf. Sci. Technol. 2006, 57, 359–377. [Google Scholar] [CrossRef]
- Chen, C. CiteSpace: A Practical Guide for Mapping Scientific Literature; Nova Science Publishers: New York, NY, USA, 2016; ISBN 978-1-5361-0280-2. [Google Scholar]
- Monti, M.M.; Vanhaudenhuyse, A.; Coleman, M.R.; Boly, M.; Pickard, J.D.; Tshibanda, L.; Owen, A.M.; Laureys, S. Willful Modulation of Brain Activity in Disorders of Consciousness. N. Engl. J. Med. 2010, 362, 579–589. [Google Scholar] [CrossRef]
- Laureys, S.; Celesia, G.G.; Cohadon, F.; Lavrijsen, J.; León-Carrión, J.; Sannita, W.G.; Sazbon, L.; Schmutzhard, E.; von Wild, K.R.; Zemen, A.; et al. Unresponsive Wakefulness Syndrome: A New Name for the Vegetative State or Apallic Syndrome. BMC Med. 2010, 8, 68. [Google Scholar] [CrossRef]
- Cruse, D.; Chennu, S.; Chatelle, C.; Bekinschtein, T.A.; Fernández-Espejo, D.; Pickard, J.D.; Laureys, S.; Owen, A.M. Bedside Detection of Awareness in the Vegetative State: A Cohort Study. Lancet 2011, 378, 2088–2094. [Google Scholar] [CrossRef]
- Stender, J.; Gosseries, O.; Bruno, M.-A.; Charland-Verville, V.; Vanhaudenhuyse, A.; Demertzi, A.; Chatelle, C.; Thonnard, M.; Thibaut, A.; Heine, L.; et al. Diagnostic Precision of PET Imaging and Functional MRI in Disorders of Consciousness: A Clinical Validation Study. Lancet 2014, 384, 514–522. [Google Scholar] [CrossRef]
- Vanhaudenhuyse, A.; Noirhomme, Q.; Tshibanda, L.J.-F.; Bruno, M.-A.; Boveroux, P.; Schnakers, C.; Soddu, A.; Perlbarg, V.; Ledoux, D.; Brichant, J.-F.; et al. Default Network Connectivity Reflects the Level of Consciousness in Non-Communicative Brain-Damaged Patients. Brain 2010, 133, 161–171. [Google Scholar] [CrossRef]
- Wannez, S.; Heine, L.; Thonnard, M.; Gosseries, O.; Laureys, S.; Collaborators, C.S.G. The Repetition of Behavioral Assessments in Diagnosis of Disorders of Consciousness. Ann. Neurol. 2017, 81, 883–889. [Google Scholar] [CrossRef]
- Bruno, M.-A.; Vanhaudenhuyse, A.; Thibaut, A.; Moonen, G.; Laureys, S. From Unresponsive Wakefulness to Minimally Conscious PLUS and Functional Locked-in Syndromes: Recent Advances in Our Understanding of Disorders of Consciousness. J. Neurol. 2011, 258, 1373–1384. [Google Scholar] [CrossRef]
- Giacino, J.T.; Katz, D.I.; Schiff, N.D.; Whyte, J.; Ashman, E.J.; Ashwal, S.; Barbano, R.; Hammond, F.M.; Laureys, S.; Ling, G.S.F.; et al. Practice Guideline Update Recommendations Summary: Disorders of Consciousness: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology; the American Congress of Rehabilitation Medicine; and the National Institute on Disability, Independent Living, and Rehabilitation Research. Arch. Phys. Med. Rehabil. 2018, 99, 1699–1709. [Google Scholar] [CrossRef]
- Kondziella, D.; Friberg, C.K.; Frokjaer, V.G.; Fabricius, M.; Møller, K. Preserved Consciousness in Vegetative and Minimal Conscious States: Systematic Review and Meta-Analysis. J. Neurol. Neurosurg. Psychiatry 2016, 87, 485–492. [Google Scholar] [CrossRef]
- Zhang, Y.; You, X.; Huang, S.; Wang, M.; Dong, J. Knowledge Atlas on the Relationship between Water Management and Constructed Wetlands—A Bibliometric Analysis Based on CiteSpace. Sustainability 2022, 14, 8288. [Google Scholar] [CrossRef]
- Chen, X.; Zhou, J.; Wang, J.; Wang, D.; Liu, J.; Shi, D.; Yang, D.; Pan, Q. Visualizing Status, Hotspots, and Future Trends in Mathematical Literacy Research via Knowledge Graph. Sustainability 2022, 14, 13842. [Google Scholar] [CrossRef]
- Seel, R.T.; Sherer, M.; Whyte, J.; Katz, D.I.; Giacino, J.T.; Rosenbaum, A.M.; Hammond, F.M.; Kalmar, K.; Pape, T.L.-B.; Zafonte, R.; et al. Assessment Scales for Disorders of Consciousness: Evidence-Based Recommendations for Clinical Practice and Research. Arch. Phys. Med. Rehabil. 2010, 91, 1795–1813. [Google Scholar] [CrossRef]
- Giacino, J.T.; Kezmarsky, M.A.; DeLuca, J.; Cicerone, K.D. Monitoring Rate of Recovery to Predict Outcome in Minimally Responsive Patients. Arch. Phys. Med. Rehabil. 1991, 72, 897–901. [Google Scholar] [CrossRef] [PubMed]
- Giacino, J.T.; Kalmar, K.; Whyte, J. The JFK Coma Recovery Scale-Revised: Measurement Characteristics and Diagnostic Utility1. Arch. Phys. Med. Rehabil. 2004, 85, 2020–2029. [Google Scholar] [CrossRef] [PubMed]
- Kondziella, D.; Bender, A.; Diserens, K.; van Erp, W.; Estraneo, A.; Formisano, R.; Laureys, S.; Naccache, L.; Ozturk, S.; Rohaut, B.; et al. European Academy of Neurology Guideline on the Diagnosis of Coma and Other Disorders of Consciousness. Eur. J. Neurol. 2020, 27, 741–756. [Google Scholar] [CrossRef] [PubMed]
- Porcaro, C.; Nemirovsky, I.E.; Riganello, F.; Mansour, Z.; Cerasa, A.; Tonin, P.; Stojanoski, B.; Soddu, A. Diagnostic Developments in Differentiating Unresponsive Wakefulness Syndrome and the Minimally Conscious State. Front. Neurol. 2022, 12, 778951. [Google Scholar] [CrossRef] [PubMed]
- Gosseries, O.; Sarasso, S.; Casarotto, S.; Boly, M.; Schnakers, C.; Napolitani, M.; Bruno, M.-A.; Ledoux, D.; Tshibanda, J.-F.; Massimini, M.; et al. On the Cerebral Origin of EEG Responses to TMS: Insights from Severe Cortical Lesions. Brain Stimul. Basic Transl. Clin. Res. Neuromodul. 2015, 8, 142–149. [Google Scholar] [CrossRef]
- Bodart, O.; Gosseries, O.; Wannez, S.; Thibaut, A.; Annen, J.; Boly, M.; Rosanova, M.; Casali, A.G.; Casarotto, S.; Tononi, G.; et al. Measures of Metabolism and Complexity in the Brain of Patients with Disorders of Consciousness. NeuroImage Clin. 2017, 14, 354–362. [Google Scholar] [CrossRef]
- Demertzi, A.; Antonopoulos, G.; Heine, L.; Voss, H.U.; Crone, J.S.; de Los Angeles, C.; Bahri, M.A.; Di Perri, C.; Vanhaudenhuyse, A.; Charland-Verville, V.; et al. Intrinsic Functional Connectivity Differentiates Minimally Conscious from Unresponsive Patients. Brain 2015, 138, 2619–2631. [Google Scholar] [CrossRef] [PubMed]
- Edlow, B.L.; Chatelle, C.; Spencer, C.A.; Chu, C.J.; Bodien, Y.G.; O’Connor, K.L.; Hirschberg, R.E.; Hochberg, L.R.; Giacino, J.T.; Rosenthal, E.S.; et al. Early Detection of Consciousness in Patients with Acute Severe Traumatic Brain Injury. Brain 2017, 140, 2399–2414. [Google Scholar] [CrossRef]
- Owen, A.M.; Coleman, M.R.; Boly, M.; Davis, M.H.; Laureys, S.; Pickard, J.D. Detecting Awareness in the Vegetative State. Science 2006, 313, 1402. [Google Scholar] [CrossRef]
- Claassen, J.; Doyle, K.; Matory, A.; Couch, C.; Burger, K.M.; Velazquez, A.; Okonkwo, J.U.; King, J.-R.; Park, S.; Agarwal, S.; et al. Detection of Brain Activation in Unresponsive Patients with Acute Brain Injury. N. Engl. J. Med. 2019, 380, 2497–2505. [Google Scholar] [CrossRef]
- Fernández-Espejo, D.; Rossit, S.; Owen, A.M. A Thalamocortical Mechanism for the Absence of Overt Motor Behavior in Covertly Aware Patients. JAMA Neurol. 2015, 72, 1442–1450. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Xie, Q.; Qin, P.; Chen, Y.; He, Y.; Huang, H.; Wang, F.; Ni, X.; Cichocki, A.; Yu, R.; et al. Prognosis for Patients with Cognitive Motor Dissociation Identified by Brain-Computer Interface. Brain 2020, 143, 1177–1189. [Google Scholar] [CrossRef] [PubMed]
- Jöhr, J.; Halimi, F.; Pasquier, J.; Pincherle, A.; Schiff, N.; Diserens, K. Recovery in Cognitive Motor Dissociation after Severe Brain Injury: A Cohort Study. PLoS ONE 2020, 15, e0228474. [Google Scholar] [CrossRef]
- Schiff, N.D. Cognitive Motor Dissociation Following Severe Brain Injuries. JAMA Neurol. 2015, 72, 1413–1415. [Google Scholar] [CrossRef]
- Egbebike, J.; Shen, Q.; Doyle, K.; Der-Nigoghossian, C.A.; Panicker, L.; Gonzales, I.J.; Grobois, L.; Carmona, J.C.; Vrosgou, A.; Kaur, A.; et al. Cognitive-Motor Dissociation and Time to Functional Recovery in Patients with Acute Brain Injury in the USA: A Prospective Observational Cohort Study. Lancet Neurol. 2022, 21, 704–713. [Google Scholar] [CrossRef]
- Gibson, R.M.; Owen, A.M.; Cruse, D. Brain–Computer Interfaces for Patients with Disorders of Consciousness. In Progress in Brain Research; Coyle, D., Ed.; Elsevier: Amsterdam, The Netherlands, 2016; Volume 228, pp. 241–291. ISBN 978-0-12-804216-8. [Google Scholar]
- Seth, A.K.; Bayne, T. Theories of Consciousness. Nat. Rev. Neurosci. 2022, 23, 439–452. [Google Scholar] [CrossRef]
- Schiff, N.D. Recovery of Consciousness after Brain Injury: A Mesocircuit Hypothesis. Trends Neurosci. 2010, 33, 1–9. [Google Scholar] [CrossRef]
- Markowitsch, H.J.; Kessler, J. Massive Impairment in Executive Functions with Partial Preservation of Other Cognitive Functions: The Case of a Young Patient with Severe Degeneration of the Prefrontal Cortex. In Executive Control and the Frontal Lobe: Current Issues; Springer: Berlin/Heidelberg, Germany, 2000; pp. 94–102. [Google Scholar] [CrossRef]
- Boly, M.; Massimini, M.; Tsuchiya, N.; Postle, B.R.; Koch, C.; Tononi, G. Are the Neural Correlates of Consciousness in the Front or in the Back of the Cerebral Cortex? Clinical and Neuroimaging Evidence. J. Neurosci. 2017, 37, 9603–9613. [Google Scholar] [CrossRef]
- Bodien, Y.G.; Chatelle, C.; Edlow, B.L. Functional Networks in Disorders of Consciousness. Semin. Neurol. 2017, 37, 485–502. [Google Scholar] [CrossRef]
- Rosazza, C.; Andronache, A.; Sattin, D.; Bruzzone, M.G.; Marotta, G.; Nigri, A.; Ferraro, S.; Sebastiano, D.R.; Porcu, L.; Bersano, A.; et al. Multimodal Study of Default-Mode Network Integrity in Disorders of Consciousness. Ann. Neurol. 2016, 79, 841–853. [Google Scholar] [CrossRef] [PubMed]
- Fingelkurts, A.A.; Fingelkurts, A.A.; Bagnato, S.; Boccagni, C.; Galardi, G. DMN Operational Synchrony Relates to Self-Consciousness: Evidence from Patients in Vegetative and Minimally Conscious States. Open Neuroimaging J. 2012, 6, 55–68. [Google Scholar] [CrossRef] [PubMed]
- Perri, C.D.; Bahri, M.A.; Amico, E.; Thibaut, A.; Heine, L.; Antonopoulos, G.; Charland-Verville, V.; Wannez, S.; Gomez, F.; Hustinx, R.; et al. Neural Correlates of Consciousness in Patients Who Have Emerged from a Minimally Conscious State: A Cross-Sectional Multimodal Imaging Study. Lancet Neurol. 2016, 15, 830–842. [Google Scholar] [CrossRef] [PubMed]
- Chennu, S.; Annen, J.; Wannez, S.; Thibaut, A.; Chatelle, C.; Cassol, H.; Martens, G.; Schnakers, C.; Gosseries, O.; Menon, D.; et al. Brain Networks Predict Metabolism, Diagnosis and Prognosis at the Bedside in Disorders of Consciousness. Brain 2017, 140, 2120–2132. [Google Scholar] [CrossRef] [PubMed]
- Rezai, A.R.; Sederberg, P.B.; Bogner, J.; Nielson, D.M.; Zhang, J.; Mysiw, W.J.; Knopp, M.V.; Corrigan, J.D. Improved Function After Deep Brain Stimulation for Chronic, Severe Traumatic Brain Injury. Neurosurgery 2016, 79, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Kundu, B.; Brock, A.A.; Englot, D.J.; Butson, C.R.; Rolston, J.D. Deep Brain Stimulation for the Treatment of Disorders of Consciousness and Cognition in Traumatic Brain Injury Patients: A Review. Neurosurg. Focus 2018, 45, E14. [Google Scholar] [CrossRef] [PubMed]
- Rezaei Haddad, A.; Lythe, V.; Green, A.L. Deep Brain Stimulation for Recovery of Consciousness in Minimally Conscious Patients After Traumatic Brain Injury: A Systematic Review. Neuromodul. Technol. Neural Interface 2019, 22, 373–379. [Google Scholar] [CrossRef]
- Vanhoecke, J.; Hariz, M. Deep Brain Stimulation for Disorders of Consciousness: Systematic Review of Cases and Ethics. Brain Stimul. 2017, 10, 1013–1023. [Google Scholar] [CrossRef]
- Redinbaugh, M.J.; Phillips, J.M.; Kambi, N.A.; Mohanta, S.; Andryk, S.; Dooley, G.L.; Afrasiabi, M.; Raz, A.; Saalmann, Y.B. Thalamus Modulates Consciousness via Layer-Specific Control of Cortex. Neuron 2020, 106, 66–75.e12. [Google Scholar] [CrossRef]
- Schiff, N.D.; Giacino, J.T.; Kalmar, K.; Victor, J.D.; Baker, K.; Gerber, M.; Fritz, B.; Eisenberg, B.; O’Connor, J.; Kobylarz, E.J.; et al. Behavioural Improvements with Thalamic Stimulation after Severe Traumatic Brain Injury. Nature 2007, 448, 600–603. [Google Scholar] [CrossRef]
- Manganotti, P.; Formaggio, E.; Storti, S.F.; Fiaschi, A.; Battistin, L.; Tonin, P.; Piccione, F.; Cavinato, M. Effect of High-Frequency Repetitive Transcranial Magnetic Stimulation on Brain Excitability in Severely Brain-Injured Patients in Minimally Conscious or Vegetative State. Brain Stimul. Basic Transl. Clin. Res. Neuromodul. 2013, 6, 913–921. [Google Scholar] [CrossRef]
- Thibaut, A.; Bruno, M.-A.; Ledoux, D.; Demertzi, A.; Laureys, S. TDCS in Patients with Disorders of Consciousness: Sham-Controlled Randomized Double-Blind Study. Neurology 2014, 82, 1112–1118. [Google Scholar] [CrossRef]
- Xia, X.; Bai, Y.; Zhou, Y.; Yang, Y.; Xu, R.; Gao, X.; Li, X.; He, J. Effects of 10 Hz Repetitive Transcranial Magnetic Stimulation of the Left Dorsolateral Prefrontal Cortex in Disorders of Consciousness. Front. Neurol. 2017, 8, 182. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Meng, F.; Gao, J.; Zhang, L.; Zhou, Z.; Pan, G.; Luo, B. Behavioral and Resting State Functional Connectivity Effects of High Frequency RTMS on Disorders of Consciousness: A Sham-Controlled Study. Front. Neurol. 2018, 9, 982. [Google Scholar] [CrossRef] [PubMed]
- Estraneo, A.; Pascarella, A.; Moretta, P.; Masotta, O.; Fiorenza, S.; Chirico, G.; Crispino, E.; Loreto, V.; Trojano, L. Repeated Transcranial Direct Current Stimulation in Prolonged Disorders of Consciousness: A Double-Blind Cross-over Study. J. Neurol. Sci. 2017, 375, 464–470. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Rank | Count | Author | H-Index | Country | Rank | Count | Co-Author | H-Index | Country |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 163 | Laureys S | 96 | Belgium | 1 | 1026 | Giacino JT | 50 | USA |
| 2 | 62 | Gosseries O | 41 | Belgium | 2 | 804 | Laureys S | 96 | Belgium |
| 3 | 56 | Owen AM | 85 | Canada | 3 | 568 | Schnakers C | 96 | USA |
| 4 | 53 | Chatelle C | 29 | Belgium | 4 | 482 | Monti MM | 22 | USA |
| 5 | 52 | Thibaut A | 26 | Belgium | 5 | 417 | Schiff ND | 44 | USA |
| 6 | 43 | Giacino JT | 50 | USA | 6 | 405 | Ashwal S | 61 | USA |
| 7 | 37 | Bramanti P | 52 | Italy | 7 | 400 | Boly M | 65 | USA |
| 8 | 37 | Calabro RS | 28 | Italy | 8 | 399 | Owen AM | 85 | Canada |
| 9 | 35 | Naro A | 23 | Italy | 9 | 343 | Bruno MA | 44 | Belgium |
| 10 | 33 | Schnakers C | 96 | USA | 10 | 337 | Jennett B | 48 | UK |
| Rank | Journal | Impact Factor (2021) | JCR (2021) | Count | Co-Journal | Impact Factor (2021) | JCR (2021) | Count |
|---|---|---|---|---|---|---|---|---|
| 1 | Brain Injury | 2.167 | Q2 | 101 | Neurology | 11.8 | Q1 | 1215 |
| 2 | Frontiers in Neurology | 4.086 | Q2 | 53 | New England Journal of Medicine | 176.079 | Q1 | 930 |
| 3 | Frontiers in Human Neuroscience | 3.473 | Q2 | 44 | Archives of Physical Medicine and Rehabilitation | 4.06 | Q1 | 911 |
| 4 | PloS One | 3.752 | Q2 | 39 | Lancet | 202.731 | Q1 | 879 |
| 5 | Archives of Physical Medicine and Rehabilitation | 4.06 | Q1 | 37 | Brain Injury | 2.167 | Q2 | 832 |
| 6 | Neuroimage-Clinical | 4.891 | Q2 | 37 | Brain | 15.255 | Q1 | 819 |
| 7 | Brain Sciences | 3.333 | Q3 | 36 | Neuroimage | 7.4 | Q1 | 714 |
| 8 | Clinical Neurophysiology | 4.861 | Q2 | 33 | Ann Neurol | 11.274 | Q1 | 623 |
| 9 | Journal of Neurotrauma | 4.869 | Q2 | 33 | J Neurol Neurosurg Ps | 13.654 | Q1 | 615 |
| 10 | Frontiers in Neuroscience | 5.152 | Q2 | 29 | Clin Neurophysiology | 4.861 | Q2 | 614 |
| Rank | Co-Cited References | Impact Factor (2021) | Count |
|---|---|---|---|
| 1 | Monti MM, 2010, NEW ENGL J MED, V362, P579, DOI 10.1056/NEJMoa0905370 [11] | 176.079 | 178 |
| 2 | Laureys S, 2010, BMC MED, V8, P0, DOI 10.1186/1741-7015-8-68 [12] | 11.15 | 139 |
| 3 | Schnakers C, 2009, BMC NEUROL, V9, P0, DOI 10.1186/1471-2377-9-35 [6] | 2.903 | 126 |
| 4 | Giacino JT, 2014, NAT REV NEUROL, V10, P99,DOI10.1038/nrneurol.2013.279 [3] | 0.29 | 124 |
| 5 | Cruse D, 2011, LANCET, V378, P2088, DOI 10.1016/S0140-6736(11)61224-5 [13] | 202.731 | 116 |
| 6 | Stender J, 2014, LANCET, V384, P514, DOI 10.1016/S0140-6736(14)60042-8 [14] | 202.731 | 98 |
| 7 | Vanhaudenhuyse A, 2010, BRAIN, V133, P161, DOI 10.1093/brain/awp313 [15] | 15.255 | 92 |
| 8 | Wannez S, 2017, ANN NEUROL, V81, P883, DOI 10.1002/ana.24962 [16] | 11.274 | 89 |
| 9 | Bruno MA, 2011, J NEUROL, V258, P1373, DOI 10.1007/s00415-011-6114-x [17] | 6.682 | 87 |
| 10 | Giacino JT, 2018, NEUROLOGY, V91, P450, DOI 10.1212/WNL.0000000000005926 [18] | 11.8 | 87 |
| Rank | Count | Keyword | Centrality | Keyword |
|---|---|---|---|---|
| 1 | 784 | vegetative state | 0.56 | awareness |
| 2 | 399 | minimally conscious state | 0.38 | connectivity |
| 3 | 369 | disorder | 0.37 | own name |
| 4 | 318 | disorders of consciousness | 0.29 | vegetative state |
| 5 | 307 | recovery | 0.28 | electrical stimulation |
| 6 | 255 | traumatic brain injury | 0.27 | prognostic value |
| 7 | 235 | brain injury | 0.26 | recovery |
| 8 | 233 | coma | 0.26 | complexity |
| 9 | 165 | persistent vegetative state | 0.23 | transcranial magnetic stimulation |
| 10 | 147 | awareness | 0.23 | modulation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, X.; Xu, C.; Li, S.; Wu, W.; Xiao, Q.; Xie, Q. Ten-Year Change in Disorders of Consciousness: A Bibliometric Analysis. Medicina 2023, 59, 78. https://doi.org/10.3390/medicina59010078
Zheng X, Xu C, Li S, Wu W, Xiao Q, Xie Q. Ten-Year Change in Disorders of Consciousness: A Bibliometric Analysis. Medicina. 2023; 59(1):78. https://doi.org/10.3390/medicina59010078
Chicago/Turabian StyleZheng, Xiaochun, Chengwei Xu, Shuiyan Li, Wanchun Wu, Qiuyi Xiao, and Qiuyou Xie. 2023. "Ten-Year Change in Disorders of Consciousness: A Bibliometric Analysis" Medicina 59, no. 1: 78. https://doi.org/10.3390/medicina59010078
APA StyleZheng, X., Xu, C., Li, S., Wu, W., Xiao, Q., & Xie, Q. (2023). Ten-Year Change in Disorders of Consciousness: A Bibliometric Analysis. Medicina, 59(1), 78. https://doi.org/10.3390/medicina59010078