Remitting Seronegative Symmetrical Synovitis with Pitting Edema Syndrome Worsen after the Administration of Dulaglutide

 ,
,
Abstract
1. Introduction
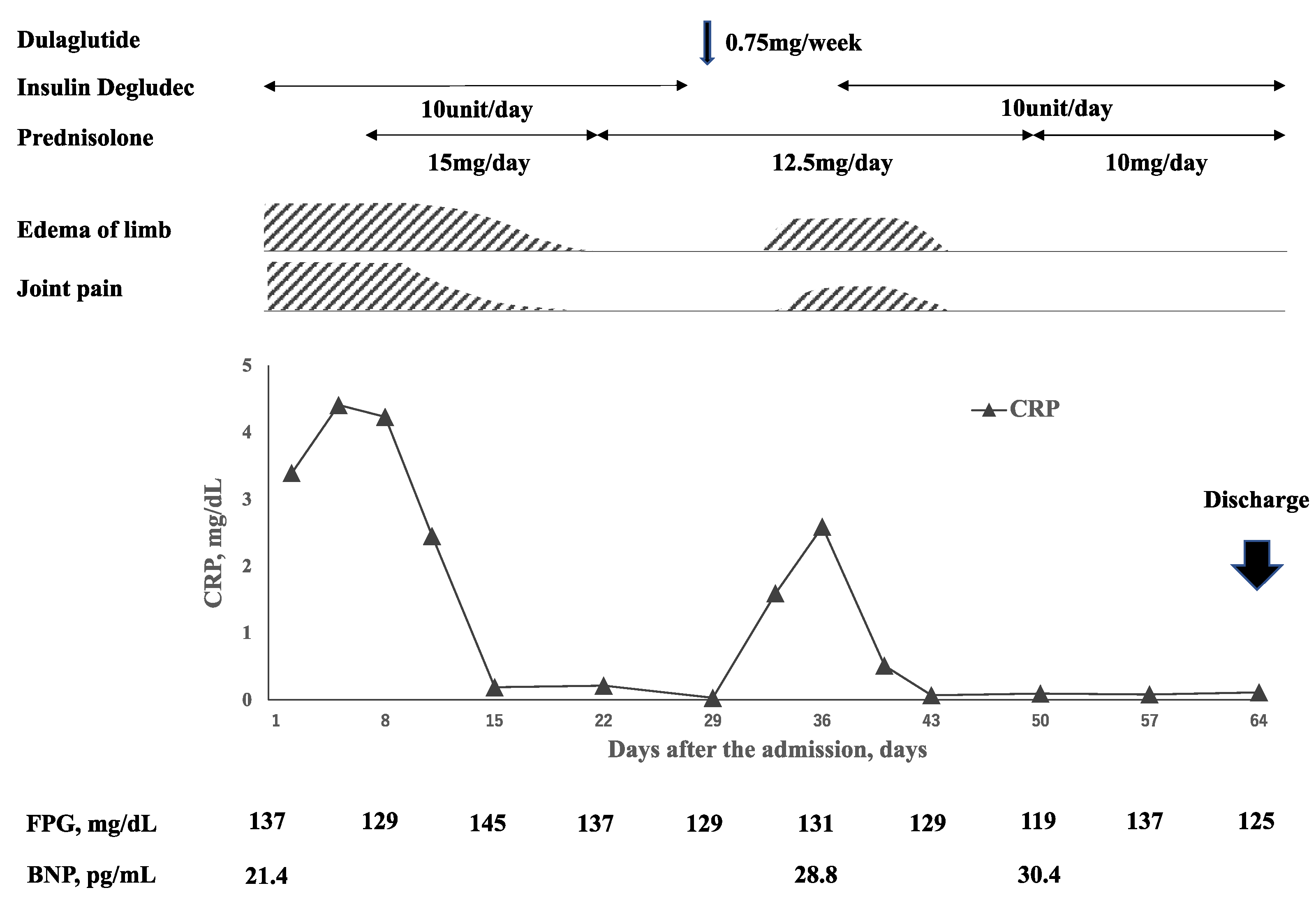
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Olivé, A.; Del Blanco, J.; Pons, M.; Vaquero, M.; Tena, X. The clinical spectrum of remitting seronegative symmetrical synovitis with pitting edema. The Catalán Group for the Study of RS3PE. J. Rheumatol. 1997, 24, 333–336. [Google Scholar] [PubMed]
- Yamauchi, K.; Sato, Y.; Yamashita, K.; Funase, Y.; Kaneko, T.; Hashimoto, T.; Aizawa, T. RS3PE Association with Dipeptidyl Pep-tidase-4 Inhibitor: Report of Two Cases. Diabetes Care 2012, 35, e7. [Google Scholar] [CrossRef] [PubMed]
- Yao, Q.; Su, X.; Altman, R.D. Is remitting seronegative symmetrical synovitis with pitting edema (RS3PE) a subset of rheumatoid arthritis? Semin. Arthritis Rheum. 2010, 40, 89–94. [Google Scholar] [CrossRef] [PubMed]
- George, D.L.; Mainali, N.R.; Schmidt, T.R.; Alweis, R. Novel Development of Remitting Seronegative Symmetrical Synovitis with Pitting Edema (RS3PE) Syndrome due to Insulin Therapy. Am. J. Case Rep. 2014, 15, 119–122. [Google Scholar] [CrossRef]
- World Health Organization (WHO)-Uppsala Monitoring Centre. The Use of the WHO-UMC System for Standardized Case Causality Assessment. Available online: http://www.who-umc.org/Graphics/24734.pdf (accessed on 10 January 2022).
- Fadini, G.P.; Boscaro, E.; Albiero, M.; Menegazzo, L.; Frison, V.; de Kreutzenberg, S.; Agostini, C.; Tiengo, A.; Avogaro, A. The oral dipeptidyl peptidase-4 inhibitor sitagliptin increases circulating endothelial progenitor cells in patients with type 2 diabetes: Possible role of stromal-derived factor-1alpha. Diabetes Care 2010, 33, 1607–1609. [Google Scholar] [CrossRef] [PubMed]
- Neuhaus, T.; Stier, S.; Totzke, G.; Gruenewald, E.; Fronhoffs, S.; Sachinidis, A.; Vetter, H.; Ko, Y.D. Stromal cell-derived factor 1α (SDF-1α) induces gene-expression of early growth response-1 (Egr-1) and VEGF in human arterial endothelial cells and enhances VEGF induced cell proliferation. Cell Prolif. 2003, 36, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Arima, K.; Origuchi, T.; Tamai, M.; Iwanaga, N.; Izumi, Y.; Huang, M.; Tanaka, F.; Kamachi, M.; Aratake, K.; Nakamura, H.; et al. RS3PE syndrome presenting as vascular endothelial growth factor associated disorder. Ann. Rheum. Dis. 2005, 64, 1653–1655. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.-Y.; Mo, Z.-H.; Chen, K.; He, H.-H.; Xie, Y.-H. Glucagon-like Peptide-1 improves proliferation and differentiation of endothelial progenitor cells via upregulating VEGF generation. Med. Sci. Monit. 2011, 17, BR35–BR41. [Google Scholar]
- Sato, K.; Kameda, M.; Yasuhara, T.; Agari, T.; Baba, T.; Wang, F.; Shinko, A.; Wakamori, T.; Toyoshima, A.; Takeuchi, H.; et al. Neuroprotective Effects of Liraglutide for Stroke Model of Rats. Int. J. Mol. Sci. 2013, 14, 21513–21524. [Google Scholar] [CrossRef] [PubMed]
- Chou, E.; Suzuma, I.; Way, K.J.; Opland, D.; Clermont, A.C.; Naruse, K.; Suzuma, K.; Bowling, N.L.; Vlahos, C.J.; Aiello, L.P.; et al. Decreased cardiac expression of vascular endothelial growth factor and its receptors in insulin-resistant and diabetic States: A possible explanation for impaired collateral formation in cardiac tissue. Circulation 2002, 105, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Hale, L.J.; Hurcombe, J.; Lay, A.; Santamaría, B.; Valverde, A.M.; Saleem, M.A.; Mathieson, P.W.; Welsh, G.I.; Coward, R.J. Insulin directly stimulates VEGF-A production in the glomerular podocyte. Am. J. Physiol. Physiol. 2013, 305, F182–F188. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Fang, W.; Ma, L.; Wang, Z.D.; Yang, Y.M.; Lu, Y.Q. VEGF levels in plasma in relation to metabolic control, inflammation, and microvascular complications in type-2 diabetes: A cohort study. Medicine 2018, 97, e0415. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Value | Normal Range |
|---|---|---|
| <Blood> | ||
| WBC count,/μL | 8100 | 4800–10,800 |
| RBC count, ×106/μL | 2.68 | 4.20–5.40 |
| Hemoglobin, g/dL | 8.6 | 12.0–16.0 |
| Platelet count, ×103/μL | 278 | 130–400 |
| TP, g/dL | 6.5 | 6.7–8.3 |
| Albumin, g/dL | 3.3 | 4.0–5.0 |
| γGTP, U/L | 12 | 10–47 |
| Total protein, g/dL | 6.5 | 6.7–8.3 |
| Albumin, g/dL | 3.3 | 4.0–5.0 |
| AST, U/L | 24 | 13–33 |
| ALT, U/L | 20 | 6–22 |
| γGTP, U/L | 12 | 10–47 |
| BUN, mg/dL | 13 | 8.0–22.0 |
| Creatinine, mg/dL | 0.71 | 0.50–0.80 |
| eGFR, mL/min/ | 57.0 | 60–90 |
| CRP, mg/dL | 3.39 | <0.3 |
| FPG, mg/dL | 114 | 69–109 |
| HbA1c, % | 6.7 | 4.6–6.2 |
| TSH, μIU/mL | 1.23 | 0.34–3.88 |
| FT4, ng/mL | 1.12 | 0.95–1.74 |
| BNP, pg/mL | 21.4 | <18.4 |
| D-Dimer, μg/mL | 0.5 | <1.0 |
| ESR, mm/h | 110 | <10 |
| MMP-3, ng/mL | 468 | 17.3–59.7 |
| RF, IU/mL | <3.0 | <15 |
| Anti-CCP antibody, U/mL | <4.5 | <4.5 |
| <Urine> | ||
| Protein | negative | negative |
| Occult blood | negative | negative |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sawamura, T.; Karashima, S.; Ohmori, A.; Sawada, K.; Kometani, M.; Takeda, Y.; Yoneda, T. Remitting Seronegative Symmetrical Synovitis with Pitting Edema Syndrome Worsen after the Administration of Dulaglutide. Medicina 2022, 58, 289. https://doi.org/10.3390/medicina58020289
Sawamura T, Karashima S, Ohmori A, Sawada K, Kometani M, Takeda Y, Yoneda T. Remitting Seronegative Symmetrical Synovitis with Pitting Edema Syndrome Worsen after the Administration of Dulaglutide. Medicina. 2022; 58(2):289. https://doi.org/10.3390/medicina58020289
Chicago/Turabian StyleSawamura, Toshitaka, Shigehiro Karashima, Ai Ohmori, Kei Sawada, Mitsuhiro Kometani, Yoshiyu Takeda, and Takashi Yoneda. 2022. "Remitting Seronegative Symmetrical Synovitis with Pitting Edema Syndrome Worsen after the Administration of Dulaglutide" Medicina 58, no. 2: 289. https://doi.org/10.3390/medicina58020289
APA StyleSawamura, T., Karashima, S., Ohmori, A., Sawada, K., Kometani, M., Takeda, Y., & Yoneda, T. (2022). Remitting Seronegative Symmetrical Synovitis with Pitting Edema Syndrome Worsen after the Administration of Dulaglutide. Medicina, 58(2), 289. https://doi.org/10.3390/medicina58020289