
The Levels of Serum Serotonin Can Be Related to Skin and Pulmonary Manifestations of Systemic Sclerosis

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
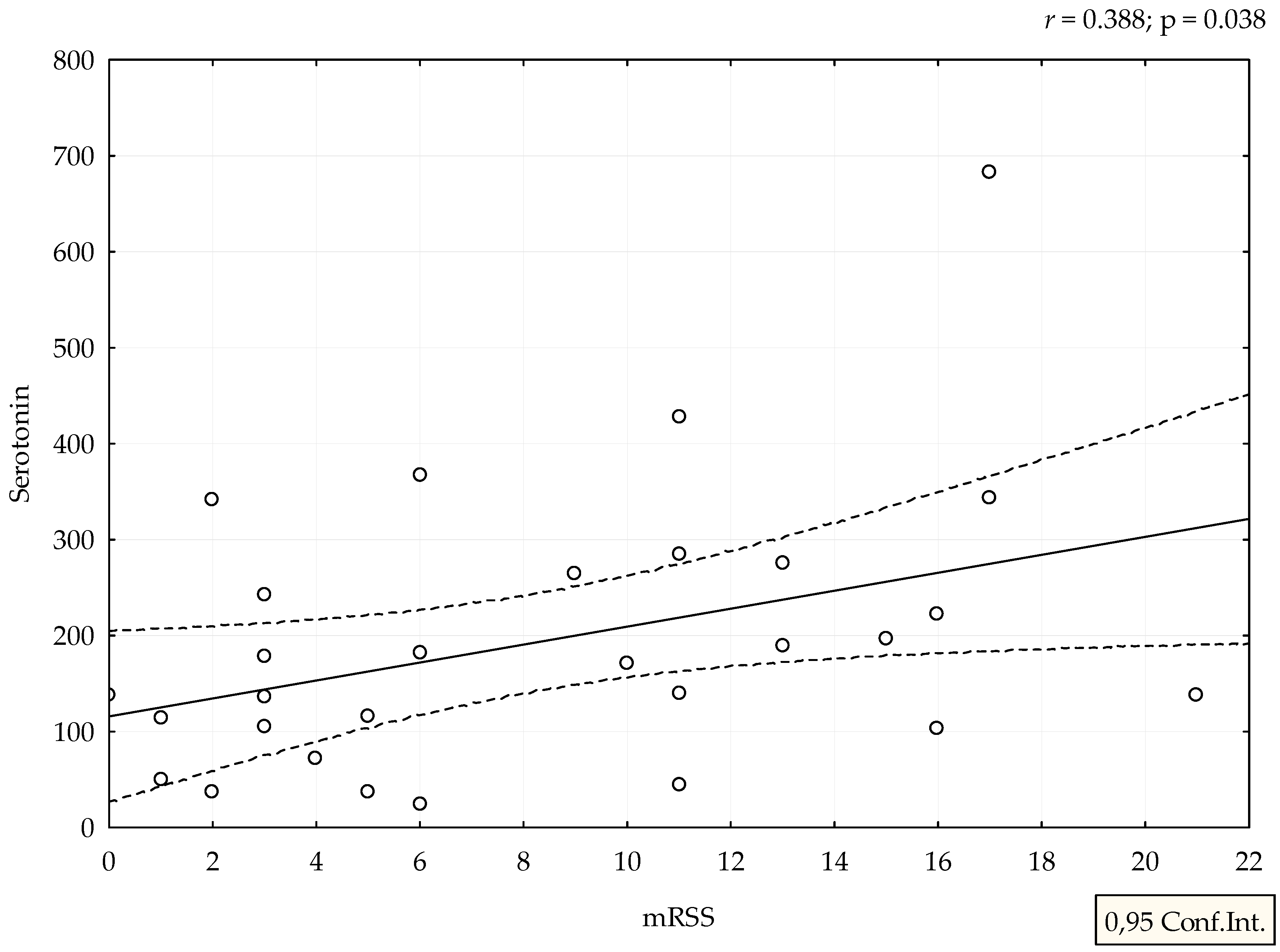
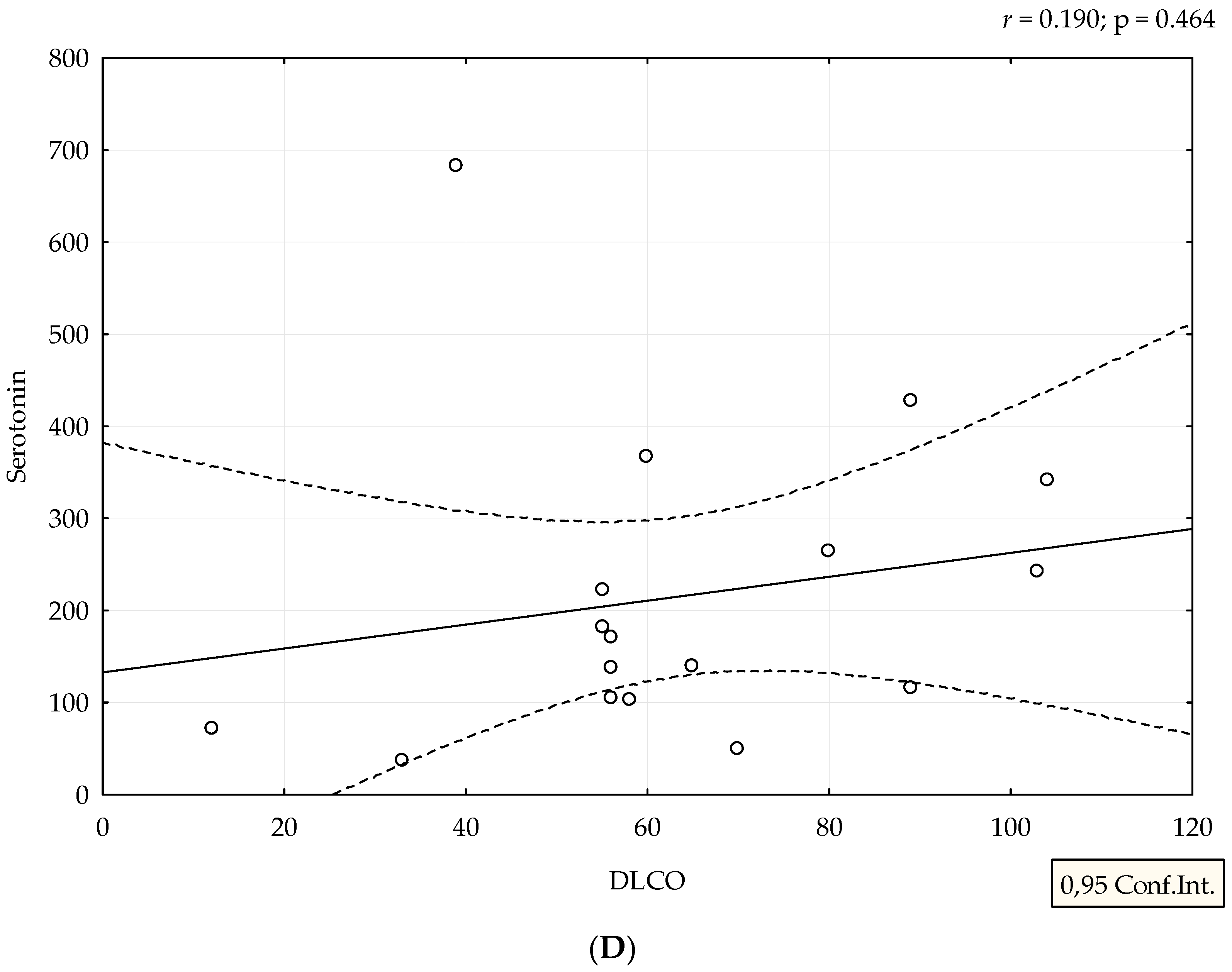
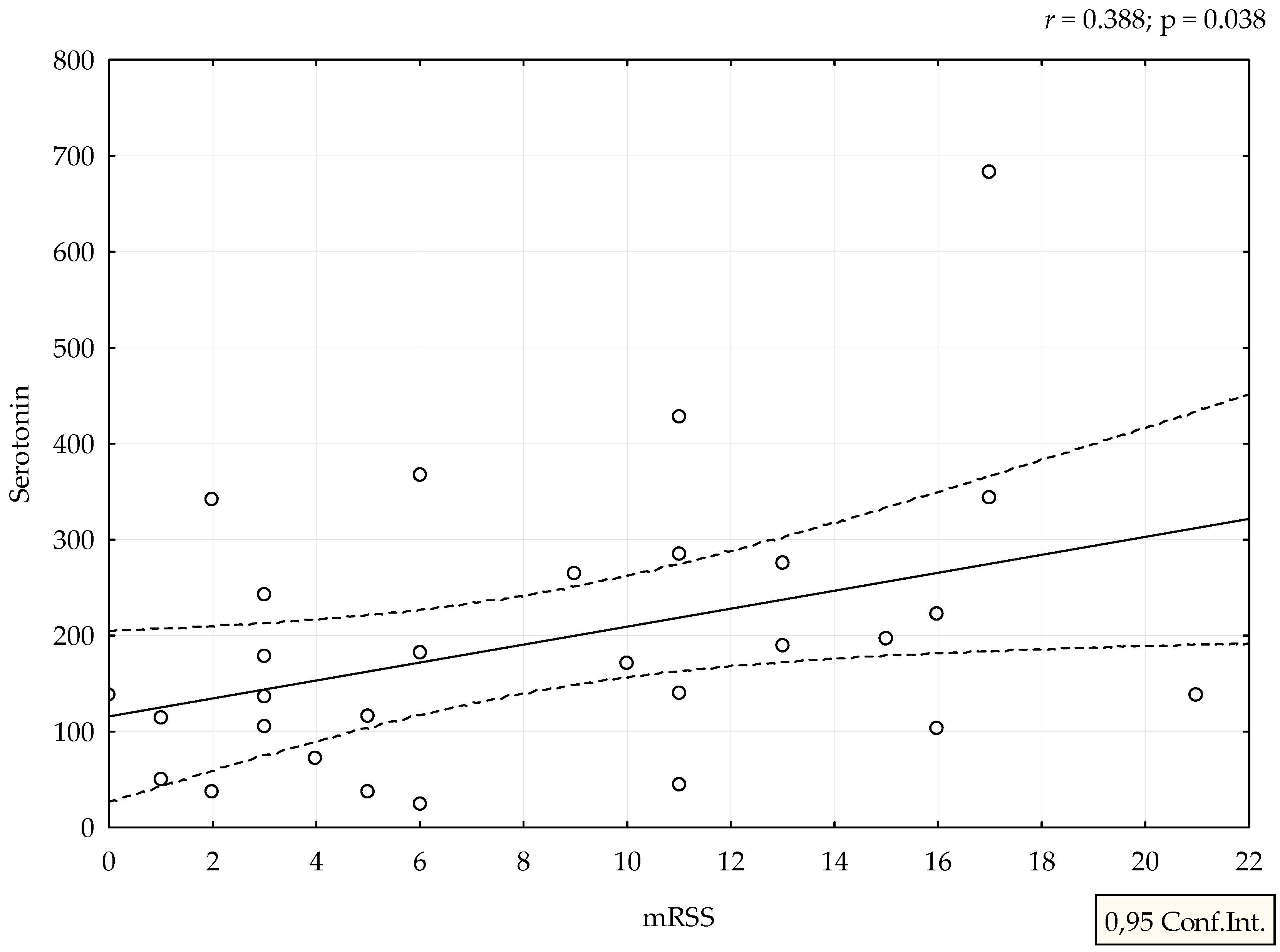
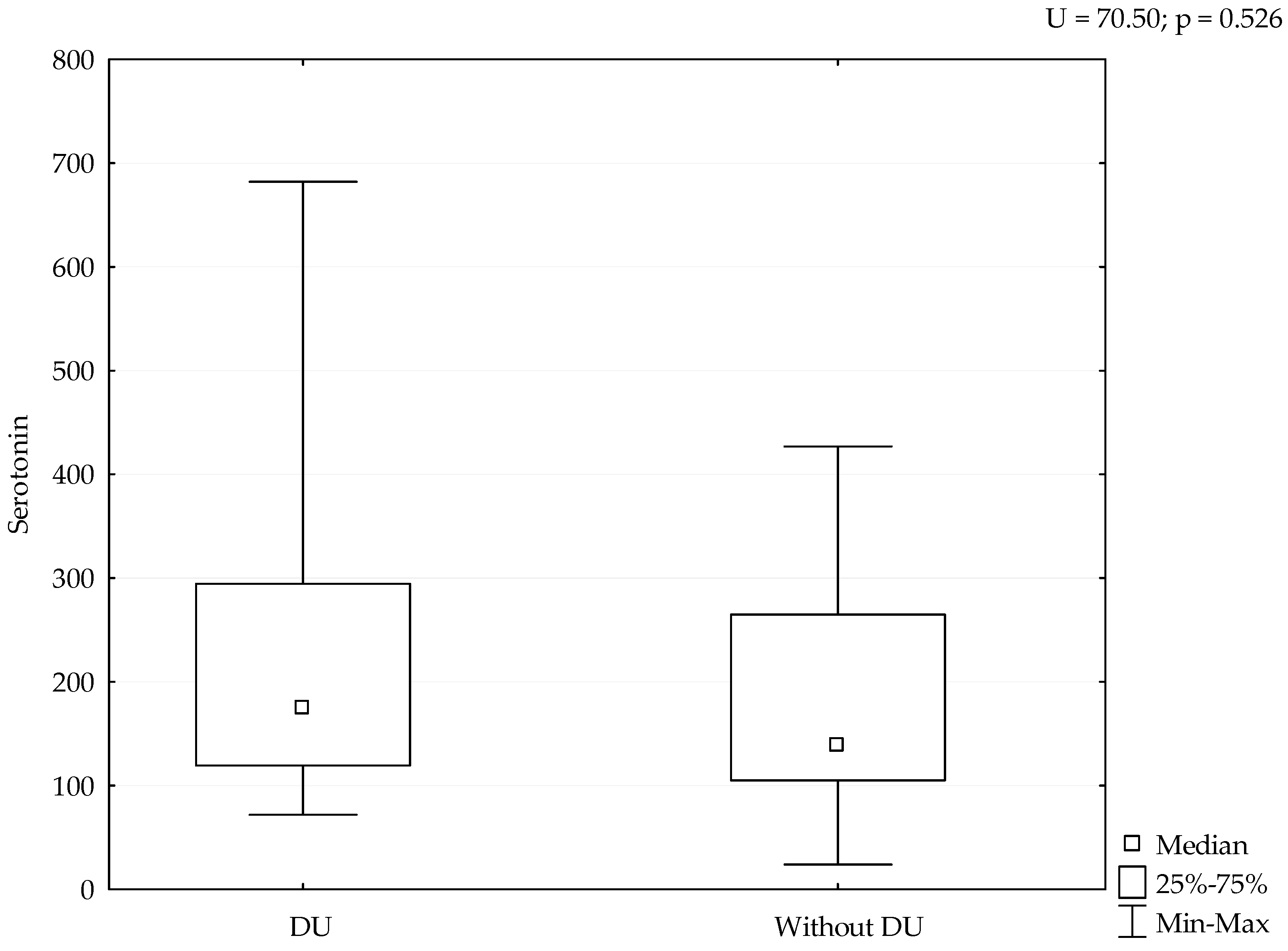
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sakkas, L.I. New developments in the pathogenesis of systemic sclerosis. Autoimmunity 2005, 38, 113–116. [Google Scholar] [CrossRef]
- Stern, E.P.; Denton, C.P. The Pathogenesis of Systemic Sclerosis. Rheum. Dis. Clin. N. Am. 2015, 41, 367–382. [Google Scholar] [CrossRef] [PubMed]
- Manetti, M.; Romano, E.; Rosa, I.; Guiducci, S.; Bellando-Randone, S.; De Paulis, A.; Ibba-Manneschi, L.; Matucci-Cerinic, M. Endothelial-to-mesenchymal transition contributes to endothelial dysfunction and dermal fibrosis in systemic sclerosis. Ann. Rheum. Dis. 2017, 76, 924–934. [Google Scholar] [CrossRef]
- Guggino, G.; Lo Pizzo, M.; Di Liberto, D.; Rizzo, A.; Cipriani, P.; Ruscitti, P.; Candore, G.; Gambino, C.M.; Sireci, G.; Dieli, F.; et al. Interleukin-9 over-expression and T helper 9 polarization in systemic sclerosis patients. Clin. Exp. Immunol. 2017, 190, 208–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furue, M.; Mitoma, C.; Mitoma, H.; Tsuji, G.; Chiba, T.; Nakahara, T.; Uchi, H.; Kadono, T. Pathogenesis of systemic sclerosis-current concept and emerging treatments. Immunol. Res. 2017, 65, 790–797. [Google Scholar] [CrossRef]
- Postlethwaite, A.E.; Chiang, T.M. Platelet contributions to the pathogenesis of systemic sclerosis. Curr. Opin. Rheumatol. 2007, 19, 574–579. [Google Scholar] [CrossRef] [PubMed]
- Bellando-Randone, S.; Matucci-Cerinic, M. Very early systemic sclerosis. Best Pract. Res. Clin. Rheumatol. 2019, 33, 101428. [Google Scholar] [CrossRef]
- Devgire, V.; Hughes, M. Raynaud’s phenomenon. Br. J. Hosp. Med. (Lond.) 2019, 80, 658–664. [Google Scholar] [CrossRef]
- Khanna, D.; Furst, D.E.; Clements, P.J.; Allanore, Y.; Baron, M.; Czirjak, L.; Distler, O.; Foeldvari, I.; Kuwana, M.; Matucci-Cerinic, M.; et al. Standardization of the modified Rodnan skin score for use in clinical trials of systemic sclerosis. J. Scleroderma Relat. Disord. 2017, 2, 11–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furst, D.E.; Clements, P.J.; Steen, V.D.; Medsger, T.A., Jr.; Masi, A.T.; D’Angelo, W.A. The modified Rodnan skin score is an accurate reflection of skin biopsy thickness in systemic sclerosis. J. Rheumatol. 1998, 25, 84–88. [Google Scholar]
- Ntelis, K.; Solomou, E.E.; Sakkas, L.; Liossis, S.N.; Daoussis, D. The role of platelets in autoimmunity, vasculopathy, and fibrosis: Implications for systemic sclerosis. Semin. Arthritis Rheum. 2017, 47, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, O.; Smith, J.R.; Purdy, R.E. Serotonin and vasoconstrictor synergism. Life Sci. 1998, 62, 1723–1732. [Google Scholar] [CrossRef]
- Soslau, G. Cardiovascular serotonergic system: Evolution, receptors, transporter, and function. J. Exp. Zool. Part A-Ecol. Integr. Physiol. 2021. Available online: https://www.webofscience.com/wos/woscc/full-record/WOS:000708131600001 (accessed on 17 January 2022).
- Kahaleh, M.B.; Osborn, I.; Leroy, E.C. Elevated levels of circulating platelet aggregates and beta-thromboglobulin in scleroderma. Ann. Intern. Med. 1982, 96, 610–613. [Google Scholar] [CrossRef]
- Van den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A.; Carreira, P.E.; et al. 2013 classification criteria for systemic sclerosis: An American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis Rheum. 2013, 65, 2737–2747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brand, T.; Anderson, G.M. The measurement of platelet-poor plasma serotonin: A systematic review of prior reports and recommendations for improved analysis. Clin. Chem. 2011, 57, 1376–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dees, C.; Akhmetshina, A.; Zerr, P.; Reich, N.; Palumbo, K.; Horn, A.; Jüngel, A.; Beyer, C.; Krönke, G.; Zwerina, J.; et al. Platelet-derived serotonin links vascular disease and tissue fibrosis. J. Exp. Med. 2011, 208, 961–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klimiuk, P.S.; Grennan, A.; Weinkove, C.; Jayson, M.I. Platelet serotonin in systemic sclerosis. Ann. Rheum. Dis. 1989, 48, 586–589. [Google Scholar] [CrossRef] [Green Version]
- Fries, J.F.; Lindgren, J.A.; Bull, J.M. Scleroderma-like lesions and the carcinoid syndrome. Arch. Intern. Med. 1973, 131, 550–553. [Google Scholar] [CrossRef]
- Macdonald, R.A.; Robbins, S.L.; Mallory, G.K. Dermal fibrosis following subcutaneous injections of serotonin creatinine sulphate. Proc. Soc. Exp. Biol. Med. 1958, 97, 334–337. [Google Scholar] [CrossRef]
- Van Neuten, J.M.; Janssens, W.J.; Vanhoutte, P.M. Serotonin and vascular reactivity. Pharmacol. Res. Commun. 1985, 17, 585–608. [Google Scholar] [CrossRef]
- Biondi, M.L.; Marasini, B.; Bianchi, E.; Agostoni, A. Plasma free and intraplatelet serotonin in patients with Raynaud’s phenomenon. Int. J. Cardiol. 1988, 19, 335–339. [Google Scholar] [CrossRef]
- Wipff, J.; Bonnet, P.; Ruiz, B.; Dieude, P.; Avouac, J.; Tiev, K.; Hachulla, E.; Cracowski, J.L.; Diot, E.; Sibilia, J.; et al. Association study of serotonin transporter gene (SLC6A4) in systemic sclerosis in European Caucasian populations. J. Rheumatol. 2010, 37, 1164–1167. [Google Scholar] [CrossRef] [PubMed]
- Beretta, L.; Cossu, M.; Marchini, M.; Cappiello, F.; Artoni, A.; Motta, G.; Scorza, R. A polymorphism in the human serotonin 5-HT2A receptor gene may protect against systemic sclerosis by reducing platelet aggregation. Arthritis Res. Ther. 2008, 10, R103. [Google Scholar] [CrossRef] [Green Version]
- Kirsten, H.; Burkhardt, J.; Hantmann, H.; Hunzelmann, N.; Vaith, P.; Ahnert, P.; Melchers, I. 5HT2A polymorphism His452Tyr in a German Caucasian systemic sclerosis population. Arthritis Res. Ther. 2009, 11, 403. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Gong, Q.; Huang, C.; Li, G. Relationships between serotoninergic system and skin fibrotic. Antiinflamm. Antiallergy Agents Med. Chem. 2014, 13, 9–16. [Google Scholar] [CrossRef]
- Mann, D.A.; Oakley, F. Serotonin paracrine signaling in tissue fibrosis. Biochim. Biophys Acta 2013, 1832, 905–910. [Google Scholar] [CrossRef] [Green Version]
- Cooke, J.P.; Marshall, J.M. Mechanisms of Raynaud’s disease. Vasc. Med. 2005, 10, 293–307. [Google Scholar] [CrossRef] [Green Version]
- Pereira, P.R.; Oliveira-Junior, M.C.; Mackenzie, B.; Chiovatto, J.E.; Matos, Y.; Greiffo, F.R.; Rigonato-Oliveira, N.C.; Brugemman, T.R.; Delle, H.; Idzko, M.; et al. Exercise Reduces Lung Fibrosis Involving Serotonin/Akt Signaling. Med. Sci. Sports Exerc. 2016, 48, 1276–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, W.; Schymura, Y.; Novoyatleva, T.; Kojonazarov, B.; Boehm, M.; Wietelmann, A.; Luitel, H.; Murmann, K.; Krompiec, D.R.; Tretyn, A.; et al. 5-HT2B receptor antagonists inhibit fibrosis and protect from RV heart failure. BioMed Res. Int. 2015, 2015, 438403. [Google Scholar] [CrossRef]
- Fabre, A.; Marchal-Sommé, J.; Marchand-Adam, S.; Quesnel, C.; Borie, R.; Dehoux, M.; Ruffié, C.; Callebert, J.; Launay, J.M.; Hénin, D.; et al. Modulation of bleomycin-induced lung fibrosis by serotonin receptor antagonists in mice. Eur. Respir. J. 2008, 32, 426–436. [Google Scholar] [CrossRef] [Green Version]
- Löfdahl, A.; Tornling, G.; Wigén, J.; Larsson-Callerfelt, A.K.; Wenglén, C.; Westergren-Thorsson, G. Pathological Insight into 5-HT2B Receptor Activation in Fibrosing Interstitial Lung Diseases. Int. J. Mol. Sci. 2020, 22, 225. [Google Scholar] [CrossRef] [PubMed]
- Falkenberg, V.R.; Rajeevan, M.S. Identification of a potential molecular link between the glucocorticoid and serotonergic signaling systems. J. Mol. Neurosci. 2010, 41, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Guo, K.; Qu, W.; Han, Y.; Wang, S.; Lin, M.; An, S.; Li, X.; Ma, S.; Wang, T.; et al. Important role of 5-hydroxytryptamine in glucocorticoid-induced insulin resistance in liver and intra-abdominal adipose tissue of rats. J. Diabetes Investig. 2016, 7, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Hasni Ebou, M.; Singh-Estivalet, A.; Launay, J.M.; Callebert, J.; Tronche, F.; Ferré, P.; Gautier, J.F.; Guillemain, G.; Bréant, B.; Blondeau, B.; et al. Glucocorticoids Inhibit Basal and Hormone-Induced Serotonin Synthesis in Pancreatic Beta Cells. PLoS ONE 2016, 11, e0149343. [Google Scholar] [CrossRef] [Green Version]
- Kowal-Bielecka, O.; Fransen, J.; Avouac, J.; Becker, M.; Kulak, A.; Allanore, Y.; Distler, O.; Clements, P.; Cutolo, M.; Czirjak, L.; et al. Update of EULAR recommendations for the treatment of systemic sclerosis. Ann. Rheum. Dis. 2017, 76, 1327–1339. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SSc Patients (n = 29) | |
|---|---|
| Age (years), median (minimum-maximum) | 58 (41–80) |
| Disease duration (years), mean (S.D. 1) | 9 (6.4) |
| Raynoud phenomenon | 27 (93.1) |
| mRSS 2, mean (S.D.) | 8.3 (5.9) |
| DU 3 | 8 (27.6) |
| Interstitial lung disease verified by HRCT 4 | 15 (51.7) |
| Pulmonary artery hypertension verified by PCWP 5 | 4 (13.8) |
| ANA 6 positive | 26 (89.7) |
| Anti topo I positive | 16 (55.2) |
| ACA 7 positive | 3 (10) |
| SSc Patients (n = 19) | |
|---|---|
| FEV1 1 | 89 (28–114) |
| FVC 2 | 93 (54–132) |
| Tiffeneau index | 95 (50–108) |
| Opstructive pattern, n (%) | 1 (5.3) |
| Restrictive pattern, n (%) | 4 (21.1) |
| DLCO 3 | 60 (12–114) |
| Reduced diffusion capacity below 60%, n (%) | 9 (47.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrić, M.; Perković, D.; Božić, I.; Marasović Krstulović, D.; Martinović Kaliterna, D. The Levels of Serum Serotonin Can Be Related to Skin and Pulmonary Manifestations of Systemic Sclerosis. Medicina 2022, 58, 161. https://doi.org/10.3390/medicina58020161
Petrić M, Perković D, Božić I, Marasović Krstulović D, Martinović Kaliterna D. The Levels of Serum Serotonin Can Be Related to Skin and Pulmonary Manifestations of Systemic Sclerosis. Medicina. 2022; 58(2):161. https://doi.org/10.3390/medicina58020161
Chicago/Turabian StylePetrić, Marin, Dijana Perković, Ivona Božić, Daniela Marasović Krstulović, and Dušanka Martinović Kaliterna. 2022. "The Levels of Serum Serotonin Can Be Related to Skin and Pulmonary Manifestations of Systemic Sclerosis" Medicina 58, no. 2: 161. https://doi.org/10.3390/medicina58020161
APA StylePetrić, M., Perković, D., Božić, I., Marasović Krstulović, D., & Martinović Kaliterna, D. (2022). The Levels of Serum Serotonin Can Be Related to Skin and Pulmonary Manifestations of Systemic Sclerosis. Medicina, 58(2), 161. https://doi.org/10.3390/medicina58020161