
Uptake of COVID-19 Booster Dose among Saudi Arabian Population

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Measurements
2.3. Data Analysis
2.4. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, F.; Yuan, Y.; Deng, Z.; Yin, D.; Shen, Q.; Zeng, J.; Xie, Y.; Xu, M.; Yang, M.; Jiang, S.; et al. Acceptance of COVID-19 Booster Vaccination Based on the Protection Motivation Theory: A Cross-sectional Study in China. J. Med. Virol. 2022, 94, 4115–4124. [Google Scholar] [CrossRef] [PubMed]
- Lai, X.; Zhu, H.; Wang, J.; Huang, Y.; Jing, R.; Lyu, Y.; Zhang, H.; Feng, H.; Guo, J.; Fang, H. Public Perceptions and Acceptance of COVID-19 Booster Vaccination in China: A Cross-Sectional Study. Vaccines 2021, 9, 1461. [Google Scholar] [CrossRef] [PubMed]
- Interim Statement on Booster Doses for COVID-19 Vaccination. Available online: https://www.who.int/news/item/22-12-2021-interim-statement-on-booster-doses-for-covid-19-vaccination---update-22-december-2021 (accessed on 8 February 2022).
- Yadete, T.; Batra, K.; Netski, D.M.; Antonio, S.; Patros, M.J.; Bester, J.C. Assessing Acceptability of COVID-19 Vaccine Booster Dose among Adult Americans: A Cross-Sectional Study. Vaccines 2021, 9, 1424. [Google Scholar] [CrossRef] [PubMed]
- WHO—COVID-19 Vaccine Tracker. Available online: https://covid19.trackvaccines.org/agency/who/ (accessed on 8 February 2022).
- Kuhlmann, C.; Mayer, C.K.; Claassen, M.; Maponga, T.; Burgers, W.A.; Keeton, R.; Riou, C.; Sutherland, A.D.; Suliman, T.; Shaw, M.L.; et al. Breakthrough Infections with SARS-CoV-2 Omicron despite MRNA Vaccine Booster Dose. Lancet 2022, 399, 625–626. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against COVID-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine Hesitancy: The next Challenge in the Fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- Obregon, R.; Mosquera, M.; Tomsa, S.; Chitnis, K. Vaccine Hesitancy and Demand for Immunization in Eastern Europe and Central Asia: Implications for the Region and Beyond. J. Health Commun. 2020, 25, 808–815. [Google Scholar] [CrossRef]
- Jairoun, A.A.; Al-Hemyari, S.S.; El-Dahiyat, F.; Jairoun, M.; Shahwan, M.; Al Ani, M.; Habeb, M.; Babar, Z.-U.-D. Assessing Public Knowledge, Attitudes and Determinants of Third COVID-19 Vaccine Booster Dose Acceptance: Current Scenario and Future Perspectives. J. Pharm Policy Pract. 2022, 15, 26. [Google Scholar] [CrossRef]
- Chenchula, S.; Karunakaran, P.; Sharma, S.; Chavan, M. Current Evidence on Efficacy of COVID-19 Booster Dose Vaccination against the Omicron Variant: A Systematic Review. J. Med. Virol. 2022, 94, 2969–2976. [Google Scholar] [CrossRef]
- Folcarelli, L.; Miraglia del Giudice, G.; Corea, F.; Angelillo, I.F. Intention to Receive the COVID-19 Vaccine Booster Dose in a University Community in Italy. Vaccines 2022, 10, 146. [Google Scholar] [CrossRef]
- Al-Hanawi, M.K.; Ahmad, K.; Haque, R.; Keramat, S.A. Willingness to Receive COVID-19 Vaccination among Adults with Chronic Diseases in the Kingdom of Saudi Arabia. J. Infect. Public Health 2021, 14, 1489–1496. [Google Scholar] [CrossRef]
- Coronavirus Disease (COVID-19) Outbreak. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/novel-coronavirus-2019-ncov (accessed on 8 February 2022).
- Adams, S.H.; Schaub, J.P.; Nagata, J.M.; Park, M.J.; Brindis, C.D.; Irwin, C.E. Young Adult Perspectives on COVID-19 Vaccinations. J. Adolesc. Health 2021, 69, 511–514. [Google Scholar] [CrossRef]
- Abdul Salam, A.; Elsegaey, I.; Khraif, R.; Al-Mutairi, A. Population Distribution and Household Conditions in Saudi Arabia: Reflections from the 2010 Census. SpringerPlus 2014, 3, 530. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Fang, Y.; Yu, F.; Chan, P.S.; Chen, S.; Sun, F. Facilitators and Barriers to Take up a COVID-19 Vaccine Booster Dose among Community-Dwelling Older Adults in Hong Kong: A Population-Based Random Telephone Survey. Vaccines 2022, 10, 966. [Google Scholar] [CrossRef]
- Bardosh, K.; de Figueiredo, A.; Gur-Arie, R.; Jamrozik, E.; Doidge, J.; Lemmens, T.; Keshavjee, S.; Graham, J.E.; Baral, S. The Unintended Consequences of COVID-19 Vaccine Policy: Why Mandates, Passports and Restrictions May Cause More Harm than Good. BMJ Glob. Health 2022, 7, e008684. [Google Scholar] [CrossRef]
- Zhang, K.; Fang, Y.; Chan, P.S.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.; Zhou, X.; Wang, Z. Behavioral Intention to Get a Booster Dose of COVID-19 Vaccine among Chinese Factory Workers. Int. J. Environ. Res. Public Health 2022, 19, 5245. [Google Scholar] [CrossRef]
- Hodge, T.R.; Orzach, R.; Silberman, J. Higher Education Decision on COVID-19 Vaccine Mandate. Appl. Econ. Lett. 2022, 1–5. [Google Scholar] [CrossRef]
- Meo, S.A.; Bukhari, I.A.; Akram, J.; Meo, A.S.; Klonoff, D.C. COVID-19 Vaccines: Comparison of Biological, Pharmacological Characteristics and Adverse Effects of Pfizer/BioNTech and Moderna Vaccines. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1663–1669. [Google Scholar] [CrossRef]
- Ganesan, S.; Al Ketbi, L.M.B.; Al Kaabi, N.; Al Mansoori, M.; Al Maskari, N.N.; Al Shamsi, M.S.; Alderei, A.S.; El Eissaee, H.N.; Al Ketbi, R.M.; Al Shamsi, N.S.; et al. Vaccine Side Effects Following COVID-19 Vaccination Among the Residents of the UAE—An Observational Study. Front. Public Health 2022, 10, 876336. [Google Scholar] [CrossRef]
- Singh, A.; Khillan, R.; Mishra, Y.; Khurana, S. The Safety Profile of COVID-19 Vaccinations in the United States. Am. J. Infect. Control. 2022, 50, 15–19. [Google Scholar] [CrossRef]
- Taryam, M.; Alawadhi, D.; Aburayya, A.; Mubarak, S.; Aljasmi, M.; Salloum, S.A.; Mouzaek, T. Factors Affecting the Uptake of COVID-19 Vaccine among Dubai Airport’s Professionals. South East. Eur. J. Public Health SEEJPH 2022, 17, 1. [Google Scholar] [CrossRef]
- Antonelli, M.; Penfold, R.S.; Merino, J.; Sudre, C.H.; Molteni, E.; Berry, S.; Canas, L.S.; Graham, M.S.; Klaser, K.; Modat, M.; et al. Risk Factors and Disease Profile of Post-Vaccination SARS-CoV-2 Infection in UK Users of the COVID Symptom Study App: A Prospective, Community-Based, Nested, Case-Control Study. Lancet Infect. Dis. 2022, 22, 43–55. [Google Scholar] [CrossRef]
- Mohseni Afshar, Z.; Barary, M.; Hosseinzadeh, R.; Alijanpour, A.; Hosseinzadeh, D.; Ebrahimpour, S.; Nazary, K.; Sio, T.T.; Sullman, M.J.M.; Carson-Chahhoud, K.; et al. Breakthrough SARS-CoV-2 Infections after Vaccination: A Critical Review. Hum. Vaccines Immunother. 2022, 18, 2051412. [Google Scholar] [CrossRef]
- Ejaz, W.; Ittefaq, M.; Seo, H.; Naz, F. Factors Associated with the Belief in COVID-19 Related Conspiracy Theories in Pakistan. Health Risk Soc. 2021, 23, 162–178. [Google Scholar] [CrossRef]
- Dohle, S.; Wingen, T.; Schreiber, M. Acceptance and Adoption of Protective Measures during the COVID-19 Pandemic: The Role of Trust in Politics and Trust in Science. Soc. Psychol. Bull. 2020, 15, e4315. [Google Scholar] [CrossRef]
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. A Global Database of COVID-19 Vaccinations. Our World Data 2021, 5, 947–953. [Google Scholar]
- Alper, S.; Bayrak, F.; Yilmaz, O. Psychological Correlates of COVID-19 Conspiracy Beliefs and Preventive Measures: Evidence from Turkey. Curr. Psychol. 2021, 40, 5708–5717. [Google Scholar] [CrossRef]
- Zeng, Z.; Ding, Y.; Zhang, Y.; Guo, Y. What Breeds Conspiracy Theories in COVID-19? The Role of Risk Perception in the Belief in COVID-19 Conspiracy. Int. J. Environ. Res. Public Health 2022, 19, 5396. [Google Scholar] [CrossRef]
- Vraga, E.K.; Bode, L. Addressing COVID-19 Misinformation on Social Media Preemptively and Responsively. Emerg. Infect. Dis. 2021, 27, 396–403. [Google Scholar] [CrossRef]
- Tabong, P.T.-N.; Segtub, M. Misconceptions, Misinformation and Politics of COVID-19 on Social Media: A Multi-Level Analysis in Ghana. Front. Commun. 2021, 6, 613794. [Google Scholar] [CrossRef]

{kind=link}
| Got COVID-19 Booster Dose | ||||||||
|---|---|---|---|---|---|---|---|---|
| No (n = 1805) | Yes (n = 527) | Total (n = 2332) | p-Value | |||||
| N | % | N | % | N | % | |||
| Age in years | 18–25 | 986 | (86.1%) | 159 | (13.9%) | 1145 | 49.1% | <0.01 * |
| 26–35 | 457 | (73.2%) | 167 | (26.8%) | 624 | 26.8% | ||
| 36–45 | 227 | (65.8%) | 118 | (34.2%) | 345 | 14.8% | ||
| 46–54 | 103 | (65.6%) | 54 | (34.4%) | 157 | 6.7% | ||
| 55 and more | 32 | (52.5%) | 29 | (47.5%) | 61 | 2.6% | ||
| Gender | Male | 874 | (73.5%) | 315 | (26.5%) | 1189 | 51.0% | <0.01 * |
| Female | 931 | (81.5%) | 212 | (18.5%) | 1143 | 49.0% | ||
| Marital status | Single | 1181 | (82.5%) | 250 | (17.5%) | 1431 | 61.4% | <0.01 * |
| Married | 624 | (69.3%) | 277 | (30.7%) | 901 | 38.6% | ||
| Region of living | Northern | 241 | (87.6%) | 34 | (12.4%) | 275 | 11.8% | <0.01 * |
| Southern | 440 | (77.6%) | 127 | (22.4%) | 567 | 24.3% | ||
| Eastern | 180 | (66.4%) | 91 | (33.6%) | 271 | 11.6% | ||
| Western | 223 | (71.9%) | 87 | (28.1%) | 310 | 13.3% | ||
| Central | 721 | (79.3%) | 188 | (20.7%) | 909 | 39.0% | ||
| Education | Below secondary | 35 | (68.6%) | 16 | (31.4%) | 51 | 2.2% | <0.01 * |
| Secondary | 361 | (79.0%) | 96 | (21.0%) | 457 | 19.6% | ||
| Bachelor’s degree | 1308 | (79.2%) | 344 | (20.8%) | 1652 | 70.8% | ||
| Postgraduate degree | 101 | (58.7%) | 71 | (41.3%) | 172 | 7.4% | ||
| Employment | No | 1145 | (85.1%) | 201 | (14.9%) | 1346 | 57.7% | <0.01 * |
| Yes | 660 | (66.9%) | 326 | (33.1%) | 986 | 42.3% | ||
| Health worker | No | 1574 | (78.9%) | 420 | (21.1%) | 1994 | 85.5% | <0.01 * |
| Yes | 231 | (68.3%) | 107 | (31.7%) | 338 | 14.5% | ||
| Monthly income | Less than SAR 5000 | 1135 | (84.4%) | 209 | (15.6%) | 1344 | 57.6% | <0.01 * |
| SAR 5000–10,000 | 340 | (70.5%) | 142 | (29.5%) | 482 | 20.7% | ||
| More than SAR 10,000 | 330 | (65.2%) | 176 | (34.8%) | 506 | 21.7% | ||
| Obesity | No | 1606 | (78.3%) | 446 | (21.7%) | 2052 | 88.0% | 0.007 * |
| Yes | 199 | (71.1%) | 81 | (28.9%) | 280 | 12.0% | ||
| Smoker | No | 1505 | (78.8%) | 404 | (21.2%) | 1909 | 81.9% | <0.01 * |
| Yes | 300 | (70.9%) | 123 | (29.1%) | 423 | 18.1% | ||
| Got COVID-19 Booster Dose | ||||||||
|---|---|---|---|---|---|---|---|---|
| No (n = 1805) | Yes (n = 527) | Total | p-Value | |||||
| N | % | N | % | N | % | |||
| Influenza Vaccine | Never got before | 859 | 81.5% | 195 | 18.5% | 1054 | 45.2% | <0.01 * |
| In irregular intervals | 776 | 77.5% | 225 | 22.5% | 1001 | 42.9% | ||
| Annual intervals | 170 | 61.4% | 107 | 38.6% | 277 | 11.9% | ||
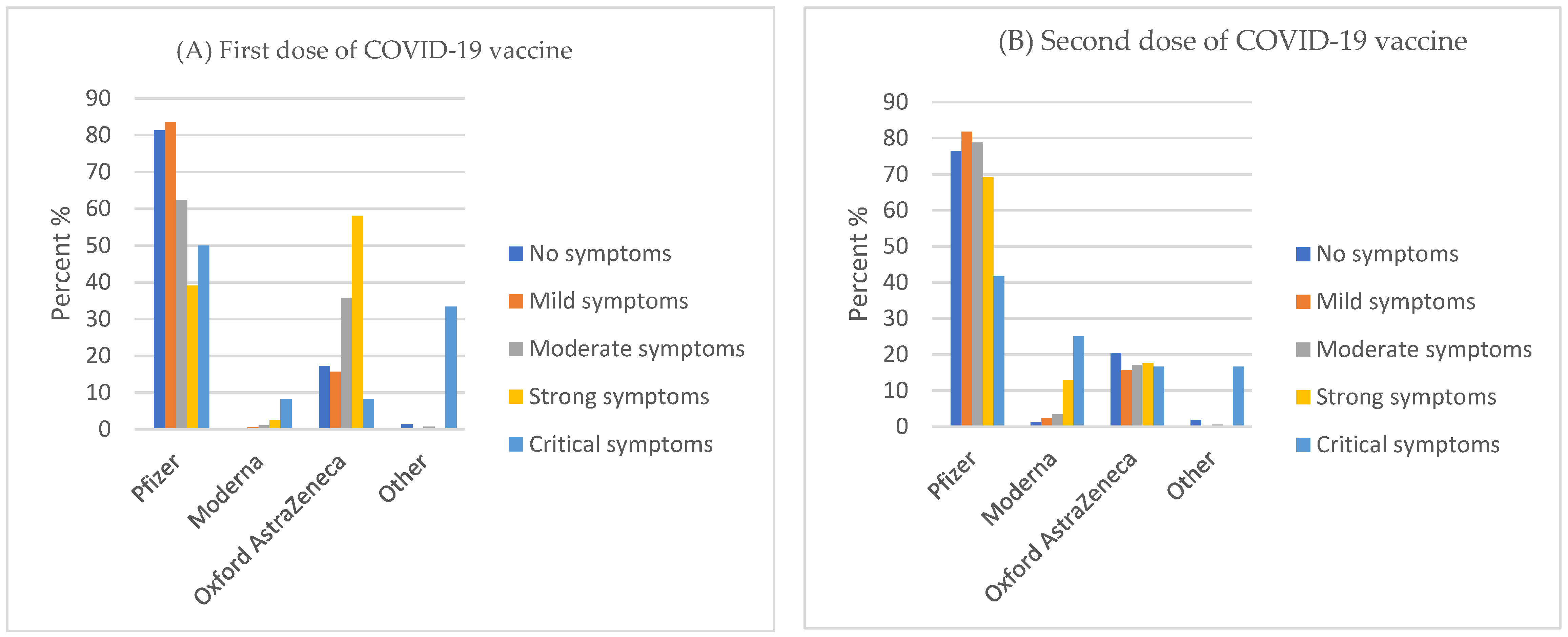
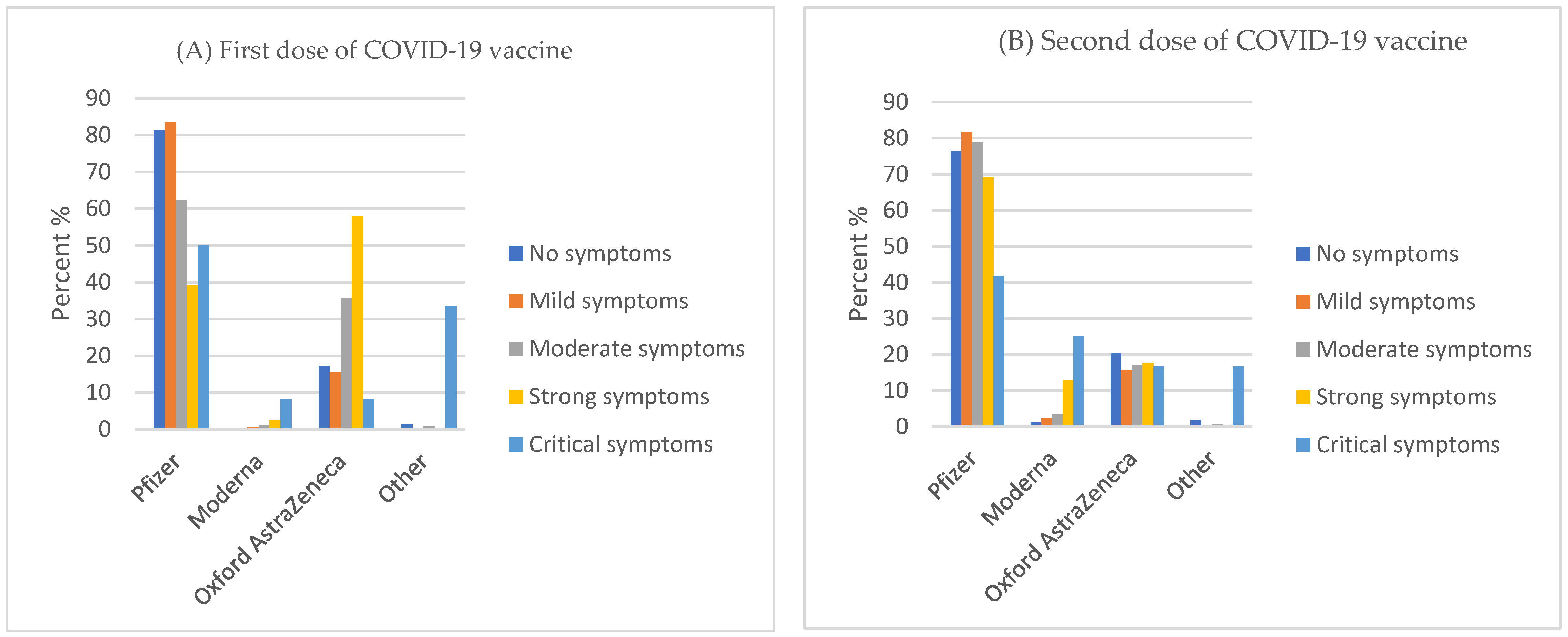
| Type of vaccines for first dose | Pfizer | 1341 | 80.1% | 334 | 19.9% | 1675 | 71.8% | <0.01 * |
| Moderna | 19 | 95.0% | 1 | 5.0% | 20 | 0.9% | ||
| Oxford AstraZeneca | 430 | 69.6% | 188 | 30.4% | 618 | 26.5% | ||
| Other | 15 | 78.9% | 4 | 21.1% | 19 | 0.8% | ||
| Type of vaccines for 2nd dose | Pfizer | 1383 | 76.6% | 423 | 23.4% | 1806 | 77.4% | <0.01 * |
| Moderna | 92 | 92.0% | 8 | 8.0% | 100 | 4.3% | ||
| Oxford AstraZeneca | 313 | 76.9% | 94 | 23.1% | 407 | 17.5% | ||
| Other | 17 | 89.5% | 2 | 10.5% | 19 | 0.8% | ||
| Side effect after first dose | No symptoms | 407 | 74.7% | 138 | 25.3% | 545 | 23.4% | 0.34 |
| Mild symptoms | 723 | 79.0% | 192 | 21.0% | 915 | 39.2% | ||
| Moderate symptoms | 413 | 76.5% | 127 | 23.5% | 540 | 23.2% | ||
| Strong symptoms | 252 | 78.8% | 68 | 21.3% | 320 | 13.7% | ||
| Critical symptoms | 10 | 83.3% | 2 | 16.7% | 12 | 0.5% | ||
| Side effect after second dose | No symptoms | 386 | 72.8% | 144 | 27.2% | 530 | 22.7% | <0.01 * |
| Mild symptoms | 578 | 74.4% | 199 | 25.6% | 777 | 33.3% | ||
| Moderate symptoms | 527 | 80.5% | 128 | 19.5% | 655 | 28.1% | ||
| Strong symptoms | 293 | 84.7% | 53 | 15.3% | 346 | 14.8% | ||
| Critical symptoms | 21 | 87.5% | 3 | 12.5% | 24 | 1.0% | ||
| Infected with COVID-19 | No | 1370 | 76.1% | 430 | 23.9% | 1800 | 77.2% | 0.006 * |
| Yes | 435 | 81.8% | 97 | 18.2% | 532 | 22.8% | ||
| Onset of infection | Before the first dose | 300 | 85.7% | 50 | 14.3% | 350 | 66.7% | <0.01* |
| After the first dose | 31 | 91.2% | 3 | 8.8% | 34 | 6.5% | ||
| After the second dose | 100 | 70.9% | 41 | 29.1% | 141 | 26.9% | ||
| Infection severity | No symptoms | 39 | 73.6% | 14 | 26.4% | 53 | 9.9% | <0.01 * |
| mild symptoms | 80 | 79.2% | 21 | 20.8% | 101 | 18.9% | ||
| moderate symptoms | 172 | 84.3% | 32 | 15.7% | 204 | 38.3% | ||
| Strong symptoms | 140 | 83.3% | 28 | 16.7% | 168 | 31.5% | ||
| critical symptoms | 5 | 71.4% | 2 | 28.6% | 7 | 1.3% | ||
| Symptoms | Fever | 327 | 83.2% | 66 | 16.8% | 393 | 75.0% | 0.028 * |
| cough | 246 | 84.2% | 46 | 15.8% | 292 | 55.7% | ||
| SOB ** | 142 | 80.2% | 35 | 19.8% | 177 | 33.8% | ||
| Fatigue | 361 | 82.4% | 77 | 17.6% | 438 | 83.6% | ||
| Myalgia | 325 | 82.1% | 71 | 17.9% | 396 | 75.6% | ||
| Headache | 347 | 83.4% | 69 | 16.6% | 416 | 79.4% | ||
| Anosmia | 323 | 81.8% | 72 | 18.2% | 395 | 75.4% | ||
| Pharyngitis | 236 | 84.3% | 44 | 15.7% | 280 | 53.4% | ||
| Congestion | 243 | 83.5% | 48 | 16.5% | 291 | 55.5% | ||
| Rhinitis | 165 | 83.8% | 32 | 16.2% | 197 | 37.6% | ||
| Nausea | 185 | 85.6% | 31 | 14.4% | 216 | 41.2% | ||
| Diarrhea | 145 | 84.3% | 27 | 15.7% | 172 | 32.8% | ||
| Vomiting | 75 | 84.3% | 14 | 15.7% | 89 | 17.0% | ||
| Got COVID-19 Booster Dose | ||||||||
|---|---|---|---|---|---|---|---|---|
| No (n = 1805) | Yes (n = 527) | Total (n = 2332) | p-Value | |||||
| N | % | N | % | N | % | |||
| I lost faith in the Saudi Ministry of Health | Disagree | 708 | 77.5% | 206 | 22.5% | 914 | 39.2% | <0.01 * |
| Agree | 582 | 82.2% | 126 | 17.8% | 708 | 30.4% | ||
| Neutral | 515 | 72.5% | 195 | 27.5% | 710 | 30.4% | ||
| I lost faith in the World Health Organization | Disagree | 1023 | 73.4% | 370 | 26.6% | 1393 | 59.7% | <0.01 * |
| Agree | 320 | 85.3% | 55 | 14.7% | 375 | 16.1% | ||
| Neutral | 462 | 81.9% | 102 | 18.1% | 564 | 24.2% | ||
| I lost my trust in healthcare practitioners | Disagree | 1094 | 74.4% | 377 | 25.6% | 1471 | 63.1% | <0.01 * |
| Agree | 275 | 82.1% | 60 | 17.9% | 335 | 14.4% | ||
| Neutral | 436 | 82.9% | 90 | 17.1% | 526 | 22.6% | ||
| I lost faith in the effectiveness of all vaccines “All vaccines are useless” | Disagree | 989 | 73.9% | 349 | 26.1% | 1338 | 57.4% | <0.01 * |
| Agree | 365 | 85.7% | 61 | 14.3% | 426 | 18.3% | ||
| Neutral | 451 | 79.4% | 117 | 20.6% | 568 | 24.4% | ||
| I lost faith in COVID-19 vaccines | Disagree | 988 | 74.1% | 346 | 25.9% | 1334 | 57.2% | <0.01 * |
| Agree | 380 | 84.3% | 71 | 15.7% | 451 | 19.3% | ||
| Neutral | 437 | 79.9% | 110 | 20.1% | 547 | 23.5% | ||
| I was not satisfied with the previous doses | Disagree | 978 | 74.4% | 337 | 25.6% | 1315 | 56.4% | <0.01 * |
| Agree | 443 | 84.2% | 83 | 15.8% | 526 | 22.6% | ||
| Neutral | 384 | 78.2% | 107 | 21.8% | 491 | 21.1% | ||
| Traveling forced me to get vaccinated (Health Passport) | Disagree | 1022 | 75.8% | 327 | 24.2% | 1349 | 57.8% | 0.084 |
| Agree | 413 | 79.9% | 104 | 20.1% | 517 | 22.2% | ||
| Neutral | 370 | 79.4% | 96 | 20.6% | 466 | 20.0% | ||
| The desire to shop and go to malls forced me to get vaccinated | Disagree | 944 | 75.2% | 311 | 24.8% | 1255 | 53.8% | 0.020 * |
| Agree | 531 | 80.6% | 128 | 19.4% | 659 | 28.3% | ||
| Neutral | 330 | 78.9% | 88 | 21.1% | 418 | 17.9% | ||
| Entertainment activities forced me to get vaccinated | Disagree | 1002 | 75.6% | 324 | 24.4% | 1326 | 56.9% | 0.048 * |
| Agree | 442 | 79.4% | 115 | 20.6% | 557 | 23.9% | ||
| Neutral | 361 | 80.4% | 88 | 19.6% | 449 | 19.3% | ||
| I do not wear a mask anymore | Disagree | 1016 | 75.9% | 322 | 24.1% | 1338 | 57.4% | 0.12 |
| Agree | 427 | 80.1% | 106 | 19.9% | 533 | 22.9% | ||
| Neutral | 362 | 78.5% | 99 | 21.5% | 461 | 19.8% | ||
| I no longer sanitize hands | Disagree | 923 | 75.7% | 296 | 24.3% | 1219 | 52.3% | 0.069 |
| Agree | 491 | 80.5% | 119 | 19.5% | 610 | 26.2% | ||
| Neutral | 391 | 77.7% | 112 | 22.3% | 503 | 21.6% | ||
| I am no longer afraid of COVID-19 and its variants | Disagree | 844 | 77.1% | 250 | 22.9% | 1094 | 46.9% | 0.63 |
| Agree | 540 | 78.6% | 147 | 21.4% | 687 | 29.5% | ||
| Neutral | 421 | 76.4% | 130 | 23.6% | 551 | 23.6% | ||
| I do not follow the news of COVID-19 in my country | Disagree | 903 | 76.2% | 282 | 23.8% | 1185 | 50.8% | 0.167 |
| Agree | 491 | 80.1% | 122 | 19.9% | 613 | 26.3% | ||
| Neutral | 411 | 77.0% | 123 | 23.0% | 534 | 22.9% | ||
| I do not follow the news of COVID-19 in the world | Disagree | 836 | 75.5% | 272 | 24.5% | 1108 | 47.5% | 0.038 * |
| Agree | 550 | 80.6% | 132 | 19.4% | 682 | 29.2% | ||
| Neutral | 419 | 77.3% | 123 | 22.7% | 542 | 23.2% | ||
| Chronic Disease | Got COVID-19 Booster Dose | |||||
|---|---|---|---|---|---|---|
| No | Yes | Total (N = 501) | ||||
| N | % | N | % | N | p-Value | |
| DM | 55 | 53.40% | 48 | 46.60% | 103 | <0.01 * |
| HTN | 64 | 62.70% | 38 | 37.30% | 102 | |
| Cancer | 6 | 46.20% | 7 | 53.80% | 13 | |
| CVS | 24 | 63.20% | 14 | 36.80% | 38 | |
| Respiratory ** | 19 | 63.30% | 11 | 36.70% | 30 | |
| Asthma | 125 | 77.60% | 36 | 22.40% | 161 | |
| Renal *** | 13 | 65.00% | 7 | 35.00% | 20 | |
| Immune deficiency disease | 27 | 79.40% | 7 | 20.60% | 34 | |
| p-Value | aOR | 95% C.I. | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Age in years | ||||
| 18–29 (ref) | ||||
| 26–35 | 0.001 * | 1.745 | 1.269 | 2.4 |
| 36–45 | <0.01 * | 2.478 | 1.621 | 3.787 |
| 46–54 | <0.01 * | 2.699 | 1.609 | 4.525 |
| 55 and more | <0.01 * | 5.415 | 2.719 | 10.783 |
| Gender | ||||
| Female (ref) | ||||
| Male | 0.644 | 0.941 | 0.728 | 1.217 |
| Marital status | ||||
| Unmarried (ref) | ||||
| Married | 0.403 | 0.875 | 0.639 | 1.197 |
| Region of living | ||||
| Northern (ref) | ||||
| Southern | 0.087 | 1.484 | 0.944 | 2.333 |
| Eastern | <0.01 * | 2.513 | 1.566 | 4.033 |
| Western | 0.004 * | 1.997 | 1.252 | 3.184 |
| Central | 0.06 | 1.495 | 0.983 | 2.272 |
| Education | ||||
| Below secondary (ref) | ||||
| Secondary | 0.567 | 0.816 | 0.406 | 1.638 |
| Bachelor’s degree | 0.435 | 0.765 | 0.39 | 1.5 |
| Postgraduates’ studies | 0.564 | 1.247 | 0.589 | 2.64 |
| Employment | ||||
| No (ref) | ||||
| Yes | <0.01 * | 1.729 | 1.281 | 2.332 |
| Health worker | ||||
| No (ref) | ||||
| Yes | 0.521 | 1.104 | 0.816 | 1.493 |
| Monthly income | ||||
| less than SAR 5000 (ref) | ||||
| Monthly income SAR 5000–10,000 | 0.675 | 1.072 | 0.773 | 1.488 |
| Monthly income more than SAR 10,000 | 0.908 | 1.022 | 0.704 | 1.484 |
| Obesity | ||||
| No (ref) | ||||
| Yes | 0.161 | 1.247 | 0.916 | 1.698 |
| Smoker | ||||
| No (ref) | ||||
| Yes | 0.474 | 1.109 | 0.835 | 1.472 |
| Influenza Vaccine | ||||
| “Never got before (ref)” | ||||
| “In irregular intervals” | 0.003 * | 1.437 | 1.134 | 1.821 |
| “Annual intervals” | <0.01 * | 2.387 | 1.73 | 3.293 |
| Type of vaccines for 1st dose | ||||
| “Pfizer” (ref) | ||||
| “Moderna” | <0.01 * | 1.324 | 1.16 | 1.51 |
| “Oxford AstraZeneca” | 0.383 | 0.381 | 0.045 | 0.304 |
| “Other” | 0.105 | 8.676 | 0.634 | 18.656 |
| Type of vaccines for 2nd dose | ||||
| “Pfizer” (ref) | ||||
| “Moderna” | 0.003 * | 0.794 | 0.683 | 0.922 |
| “Oxford AstraZeneca” | 0.018 * | 0.691 | 0.509 | 0.939 |
| “Other” | 0.077 | 0.066 | 0.003 | 1.348 |
| Side effect after 1st dose | ||||
| “No symptoms” (ref) | ||||
| “Mild symptoms” | 0.758 | 1.02 | 0.898 | 1.158 |
| “Moderate symptoms” | 0.257 | 0.965 | 0.712 | 1.309 |
| “Strong symptoms” | 0.725 | 0.927 | 0.609 | 1.411 |
| “Critical symptoms” | 0.942 | 1.083 | 0.124 | 9.419 |
| Side effect after 2nd dose | ||||
| “No symptoms” (ref) | ||||
| “Mild symptoms” | 0.877 | 0.976 | 0.723 | 1.318 |
| “Moderate symptoms” | 0.046 * | 0.71 | 0.507 | 0.9951 |
| “Strong symptoms” | 0.023 * | 0.615 | 0.404 | 0.935 |
| “Critical symptoms” | 0.001 * | 0.814 | 0.72 | 0.92 |
| Infected with COVID-19 | ||||
| “No” (ref) | ||||
| “Yes” | 0.471 | 0.462 | 0.057 | 3.773 |
| I lost faith in the Saudi Ministry of Health | ||||
| “Disagree” (ref) | ||||
| “Agree” | 0.748 | 0.755 | 0.137 | 4.176 |
| “Natural” | 0.471 | 0.462 | 0.057 | 3.773 |
| I lost faith in COVID-19 vaccines | ||||
| “Disagree” (ref) | ||||
| “Agree” | 0.31 | 1.4 | 0.7334 | 2.685 |
| “Neutral” | 0.013 * | 2.426 | 1.207 | 4.863 |
| Cancer patient | ||||
| No (ref) | ||||
| Yes | 0.008 * | 2.161 | 1.218 | 3.879 |
| Got COVID-19 Booster Dose * | ||||||
|---|---|---|---|---|---|---|
| No | Yes | Total | ||||
| n | % | n | % | n | % | |
| Health practitioners | 364 | 72.50% | 138 | 27.50% | 502 | 65.50% |
| World Health Organization | 311 | 71.30% | 125 | 28.70% | 436 | 56.90% |
| Ministry of health | 499 | 72.40% | 190 | 27.60% | 689 | 89.90% |
| Research articles | 350 | 71.00% | 143 | 29.00% | 493 | 64.40% |
| Books | 202 | 72.70% | 76 | 27.30% | 278 | 36.30% |
| The schools and universities | 189 | 74.10% | 66 | 25.90% | 255 | 33.30% |
| Celebrity and Influencers | 46 | 75.40% | 15 | 24.60% | 61 | 8.00% |
| Friends | 148 | 77.50% | 43 | 22.50% | 191 | 24.90% |
| Family | 183 | 75.30% | 60 | 24.70% | 243 | 31.70% |
| Internet | 289 | 79.20% | 76 | 20.80% | 365 | 47.70% |
| Social media | 224 | 78.90% | 60 | 21.10% | 284 | 37.10% |
| TV | 226 | 72.00% | 88 | 28.00% | 314 | 41.00% |
| Radio | 111 | 72.10% | 43 | 27.90% | 154 | 20.10% |
| Mosque and religious pulpits | 147 | 73.50% | 53 | 26.50% | 200 | 26.10% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshahrani, N.Z.; Alsabaani, A.A.; Ridda, I.; Rashid, H.; Alzahrani, F.; Almutairi, T.H.; Alzahrani, B.A.S.; Albeshri, A.S.S. Uptake of COVID-19 Booster Dose among Saudi Arabian Population. Medicina 2022, 58, 972. https://doi.org/10.3390/medicina58070972
Alshahrani NZ, Alsabaani AA, Ridda I, Rashid H, Alzahrani F, Almutairi TH, Alzahrani BAS, Albeshri ASS. Uptake of COVID-19 Booster Dose among Saudi Arabian Population. Medicina. 2022; 58(7):972. https://doi.org/10.3390/medicina58070972
Chicago/Turabian StyleAlshahrani, Najim Z., Abdullah A. Alsabaani, Iman Ridda, Harunor Rashid, Faris Alzahrani, Talal Hamed Almutairi, Bader Ahmed S. Alzahrani, and Abdulelah Saleh Saeed Albeshri. 2022. "Uptake of COVID-19 Booster Dose among Saudi Arabian Population" Medicina 58, no. 7: 972. https://doi.org/10.3390/medicina58070972
APA StyleAlshahrani, N. Z., Alsabaani, A. A., Ridda, I., Rashid, H., Alzahrani, F., Almutairi, T. H., Alzahrani, B. A. S., & Albeshri, A. S. S. (2022). Uptake of COVID-19 Booster Dose among Saudi Arabian Population. Medicina, 58(7), 972. https://doi.org/10.3390/medicina58070972