
Delays in Time to Head and Neck Cancer Treatment: A South Australian Perspective



Abstract
1. Introduction
2. Materials and Methods
3. Results
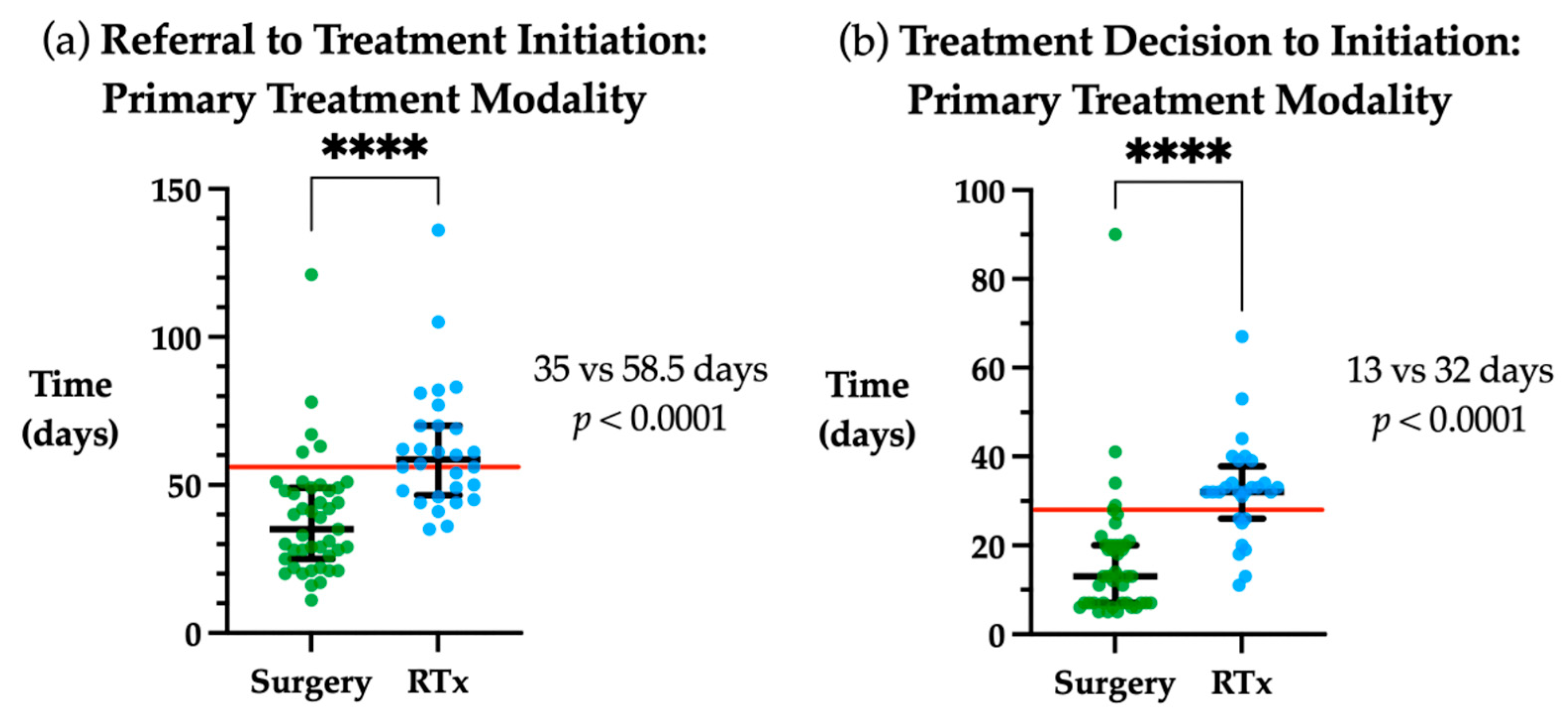
3.1. Timeframes to Treatment Initiation
3.2. Identification of Factors Associated with Time to Treatment Initiation
3.3. Identifying Factors Predictive of Exceeding the Referral to Treatment Initiation Timeframe
3.4. Mortality and Recurrence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Schutte, H.W.; Heutink, F.; Wellenstein, D.J.; van den Broek, G.B.; van den Hoogen, F.J.; Marres, H.A.; van Herpen, C.M.; Kaanders, J.H.; Merkx, T.M.; Takes, R.P. Impact of time to diagnosis and treatment in head and neck cancer: A systematic review. Otolaryngol. Head Neck Surg. 2020, 162, 446–457. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.T.; Galloway, T.J.; Handorf, E.A.; Egleston, B.L.; Wang, L.S.; Mehra, R.; Flieder, D.B.; Ridge, J.A. Survival impact of increasing time to treatment initiation for patients with head and neck cancer in the United States. J. Clin. Oncol. 2016, 34, 169. [Google Scholar] [CrossRef]
- Optimal Care Pathway for People with Head and Neck Cancer. Available online: https://www.cancer.org.au/assets/pdf/head-and-neck-cancers-optimal-cancer-care-pathway (accessed on 13 October 2021).
- Licitra, L.; Keilholz, U.; Tahara, M.; Lin, J.-C.; Chomette, P.; Ceruse, P.; Harrington, K.; Mesia, R. Evaluation of the benefit and use of multidisciplinary teams in the treatment of head and neck cancer. Oral Oncol. 2016, 59, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.L.; Jackson, J.E.; Hickey, B.E.; Szallasi, F.G.; Bond, C.A. Multidisciplinary clinic care improves adherence to best practice in head and neck cancer. Am. J. Otolaryngol. 2013, 34, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Schoonbeek, R.C.; Zwertbroek, J.; Plaat, B.E.C.; Takes, R.P.; Ridge, J.A.; Strojan, P.; Ferlito, A.; van Dijk, B.A.C.; Halmos, G.B. Determinants of delay and association with outcome in head and neck cancer: A systematic review. Eur. J. Surg. Oncol. 2021, 47, 1816–1827. [Google Scholar] [CrossRef] [PubMed]
- Liao, D.Z.; Schlecht, N.F.; Rosenblatt, G.; Kinkhabwala, C.M.; Leonard, J.A.; Ference, R.S.; Prystowsky, M.B.; Ow, T.J.; Schiff, B.A.; Smith, R.V.; et al. Association of delayed time to treatment initiation with overall survival and recurrence among patients with head and neck squamous cell carcinoma in an underserved urban population. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 1001–1009. [Google Scholar] [CrossRef] [PubMed]
- Fortin, A.; Bairati, I.; Albert, M.; Moore, L.; Allard, J.; Couture, C. Effect of treatment delay on outcome of patients with early-stage head-and-neck carcinoma receiving radical radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2002, 52, 929–936. [Google Scholar] [CrossRef]
- Polesel, J.; Furlan, C.; Birri, S.; Giacomarra, V.; Vaccher, E.; Grando, G.; Gobitti, C.; Navarria, F.; Schioppa, O.; Minatel, E.; et al. The impact of time to treatment initiation on survival from head and neck cancer in north-eastern Italy. Oral Oncol. 2017, 67, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Delivering Cancer Waiting Times: A Good Practice Guide. Available online: https://www.england.nhs.uk/wp-content/uploads/2015/03/delivering-cancer-wait-times.pdf (accessed on 27 October 2021).
- Flukes, S.; Garry, S.; Hinton-Bayre, A.; Lindsay, A. Pre-treatment wait time for head and neck cancer patients in Western Australia: Description of a new metric and examination of predictive factors. ANZ J. Surg. 2019, 89, 858–862. [Google Scholar] [CrossRef] [PubMed]
- Connell, J.T.; Sekhar, V.; Hodge, J.-C.; Krishnan, S.; Foreman, A. Delays to treatment initiation in the management of head and neck cancer. Aust. J. Otolaryngol. 2020, 3, 5. [Google Scholar] [CrossRef]
- Van Harten, M.C.; Hoebers, F.J.P.; Kross, K.W.; van Werkhoven, E.D.; van den Brekel, M.W.M.; van Dijk, B.A.C. Determinants of treatment waiting times for head and neck cancer in the Netherlands and their relation to survival. Oral Oncol. 2015, 51, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.T.; Galloway, T.J.; Handorf, E.A.; Wang, L.; Mehra, R.; Flieder, D.B.; Ridge, J.A. Increasing time to treatment initiation for head and neck cancer: An analysis of the National Cancer Database. Cancer 2015, 121, 1204–1213. [Google Scholar] [CrossRef] [PubMed]
- Castaldi, P.; Leccisotti, L.; Bussu, F.; Miccichè, F.; Rufini, V. Role of (18)F-FDG PET-CT in head and neck squamous cell carcinoma. Acta Otorhinolaryngol. Ital. 2013, 33, 1–8. [Google Scholar] [PubMed]
- Madhoun, M.F.; Blankenship, M.M.; Blankenship, D.M.; Krempl, G.A.; Tierney, W.M. Prophylactic PEG placement in head and neck cancer: How many feeding tubes are unused (and unnecessary)? World J. Gastroenterol. 2011, 17, 1004–1008. [Google Scholar] [CrossRef] [PubMed]
- McClelland, S., III; Andrews, J.Z.; Chaudhry, H.; Teckie, S.; Goenka, A. Prophylactic versus reactive gastrostomy tube placement in advanced head and neck cancer treated with definitive chemoradiotherapy: A systematic review. Oral Oncol. 2018, 87, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Baschnagel, A.M.; Yadav, S.; Marina, O.; Parzuchowski, A.; Lanni, T.B., Jr.; Warner, J.N.; Parzuchowski, J.S.; Ignatius, R.T.; Akervall, J.; Chen, P.Y.; et al. Toxicities and costs of placing prophylactic and reactive percutaneous gastrostomy tubes in patients with locally advanced head and neck cancers treated with chemoradiotherapy. Head Neck 2014, 36, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Kao, S.S.-T.; Marshall-Webb, M.; Dharmawardana, N.; Foreman, A.; Ooi, E.H. Gastrostomy tube insertion outcomes in South Australian head and neck cancer patients. Aust. J. Otolaryngol. 2018, 1, 21. [Google Scholar] [CrossRef][Green Version]
- Jawad, H.; Hodson, N.A.; Nixon, P.J. A review of dental treatment of head and neck cancer patients, before, during and after radiotherapy: Part 1. Br. Dent. J. 2015, 218, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Coca-Pelaz, A.; Takes, R.P.; Hutcheson, K.; Saba, N.F.; Haigentz, M.; Bradford, C.R.; de Bree, R.; Strojan, P.; Lund, V.J.; Mendenhall, W.M.; et al. Head and Neck Cancer: A Review of the Impact of Treatment Delay on Outcome. Adv. Ther. 2018, 35, 153–160. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Tumour Site | n | % |
|---|---|---|
| Oropharynx | 29 | 40.0 |
| Salivary gland | 12 | 16.7 |
| Unknown primary | 9 | 12.5 |
| Oral | 8 | 11.1 |
| Larynx | 6 | 8.3 |
| Skin | 3 | 4.2 |
| Hypopharynx | 2 | 2.8 |
| Nasopharynx | 1 | 1.4 |
| Thyroid | 1 | 1.4 |
| Sinonasal | 1 | 1.4 |
| Histopathology | ||
| Squamous cell carcinoma | 60 | 83.3 |
| Basal cell carcinoma | 2 | 2.8 |
| Mucoepidermoid carcinoma | 2 | 2.8 |
| Nasopharyngeal carcinoma | 1 | 1.4 |
| Adenoid cystic carcinoma | 1 | 1.4 |
| Basal cell adenocarcinoma | 1 | 1.4 |
| Salivary duct carcinoma | 1 | 1.4 |
| Secretory carcinoma | 1 | 1.4 |
| Alveolar soft part sarcoma | 1 | 1.4 |
| Acinic cell carcinoma | 1 | 1.4 |
| Merkel cell carcinoma | 1 | 1.4 |
| Stage (AJCC 8th Edition) | ||
| I | 25 | 34.7 |
| II | 9 | 12.5 |
| III | 15 | 20.9 |
| IV | 23 | 31.9 |
| Treatment Modality | ||
| Primary surgery | 43 | 59.7 |
| Surgery alone | 15 | 20.8 |
| Surgery + radiotherapy | 18 | 25.0 |
| Surgery + chemoradiotherapy | 9 | 12.5 |
| Surgery + chemotherapy | 1 | 1.4 |
| Primary radiotherapy | 29 | 40.3 |
| Radiotherapy alone | 4 | 5.6 |
| Chemoradiotherapy | 25 | 34.7 |
| Timeframe | Days Median (IQR) | Guideline Recommendation (Days) | Met Guideline n (%) |
|---|---|---|---|
| Referral to Head and Neck Clinic | 12.5 (3–20) | 14 | 40/72 (56%) |
| Head and Neck Clinic to MDT | 7 (3–14) | 14 | 56/72 (78%) |
| Treatment Decision to Initiation | 20 (11–32) | 28 | 48/72 (67%) |
| Treatment Decision to Primary Surgery | 13 (7–20) | 28 | 39/43 (91%) |
| Treatment Decision to Primary Radiotherapy | 32 (26–38) | 28 | 8/28 (29%) |
| Referral to Treatment Initiation | 45.5 (29–61) | 56 | 52/72 (72%) |
| Referral to Primary Surgery | 35 (25–49) | 56 | 38/43 (88%) |
| Referral to Primary Radiotherapy | 58.5 (47–70) | 56 | 13/28 (46%) |
| Primary Surgery to Adjuvant Radiotherapy | 42 (37–48) | 42 | 16/29 (55%) |
| Referral to Treatment Initiation (Median Days) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| PET Scan | Gastrostomy Tube | Special Needs Dental | |||||||
| No 1 | Yes | p Value | No | Yes | p Value | No | Yes | p Value | |
| Primary Surgery | 37.5 | 30 | 0.78 | 40 | 28.5 | 0.32 | 41 | 33 | 0.69 |
| Primary Radiotherapy | 56 | 62 | 0.28 | 55 | 61 | 0.52 | 41 | 61 | 0.002 |
| Odds Ratio (95% CI) | p Value | |
|---|---|---|
| Gender | 1.462 (0.484–4.410) | 0.501 |
| Histopathology 1 | 2.143 (0.426–10.779) | 0.355 |
| Residential Remoteness | 2.297 (0.586–9.006) | 0.233 |
| Stage 2 | 2.045 (0.716–5.846) | 0.1823 |
| PET | 2.741 (0.938–8.016) | 0.065 |
| Gastrostomy Tube | 3.088 (1.064–8.966) | 0.038 |
| Special Needs Dental | 2.519 (0.646–9.826) | 0.184 |
| Primary Treatment Modality | 8.769 (2.662–28.884) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cook, L.; Woods, C.; Nicholls, T.; Ooi, E.H. Delays in Time to Head and Neck Cancer Treatment: A South Australian Perspective. Medicina 2022, 58, 145. https://doi.org/10.3390/medicina58020145
Cook L, Woods C, Nicholls T, Ooi EH. Delays in Time to Head and Neck Cancer Treatment: A South Australian Perspective. Medicina. 2022; 58(2):145. https://doi.org/10.3390/medicina58020145
Chicago/Turabian StyleCook, Lachlan, Charmaine Woods, Tracey Nicholls, and Eng H. Ooi. 2022. "Delays in Time to Head and Neck Cancer Treatment: A South Australian Perspective" Medicina 58, no. 2: 145. https://doi.org/10.3390/medicina58020145
APA StyleCook, L., Woods, C., Nicholls, T., & Ooi, E. H. (2022). Delays in Time to Head and Neck Cancer Treatment: A South Australian Perspective. Medicina, 58(2), 145. https://doi.org/10.3390/medicina58020145