
Long-Term Outcomes of Perinatal Hypoxia and Asphyxia at an Early School Age

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Evaluation of Neurological Condition during the Neonatal Period
2.2. Mental Development at the Age of 1 Year
2.3. Assessment of Intellectual Abilities at an Early School Age
2.4. Clinical Neurological Examination and Evaluation of the Motor Function at an Early School Age
2.5. Evaluation of Health-Related Quality of Life (HRQL) at an Early School Age
2.6. Statistical Methods of Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ahearne, C.E.; Boylan, G.B.; Murray, D.M. Short and long-term prognosis in perinatal asphyxia: An update. World J. Clin. Pediatr. 2016, 5, 67–74. [Google Scholar] [CrossRef]
- Laptook, A.R.; Shankaran, S.; Tyson, J.E.; Munoz, B.; Bell, E.; Goldberg, R.N.; Parikh, N.A.; Ambalavanan, N.; Pedroza, C.; Pappas, A.; et al. Effect of Therapeutic Hypothermia Initiated after 6 h of Age on Death or Disability Among Newborns With Hypoxic-Ischemic Encephalopathy: A Randomized Clinical Trial. JAMA 2017, 318, 1550–1560. [Google Scholar] [CrossRef]
- Shankaran, S.; Laptook, A.R.; Pappas, A.; McDonald, S.A.; Das, A.; Tyson, J.E.; Poindexter, B.B.; Schibler, K.; Bell, E.F.; Heyne, R.J.; et al. Effect of Depth and Duration of Cooling on Death or Disability at Age 18 Months Among Neonates with Hypoxic-Ischemic Encephalopathy: A Randomized Clinical Trial. JAMA 2017, 318, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, C.J.; Helps, S.K.; Hart, D.; Zatorska, A.; Gupta, N.; Cianfaglione RVollmer, B. Minor neurological signs and behavioural function at age 2 years in neonatal hypoxic ischemic encephalopathy (HIE). Eur. J. Paediatr. Neurol. 2020, 27, 78–85. [Google Scholar] [CrossRef]
- Chin, E.M.; Jayakumar, S.; Ramos, E.; Gerner, G.; Soares, B.P.; Cristofalo, E.; Leppert, M.; Allen, M.; Parkinson, C.; Johnston, M.; et al. Preschool Language Outcomes following Perinatal Hypoxic-Ischemic Encephalopathy in the Age of Therapeutic Hypothermia. Dev. Neurosci. 2018, 40, 627–637. [Google Scholar] [CrossRef]
- Tokuhisa, T.; Ibara, S.; Minakami, H.; Maede, Y.; Ishihara, C.; Matsui, T. Outcome of infants with hypoxic ischemic encephalopathy treated with brain hypothermia. J. Obstet. Gynaecol. Res. 2014, 41, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Grass, B.; Scheidegger, S.; Latal, B.; Hagmann, C.; Held, U.; Brotschi, B. Short-term neurological improvement in neonates with hypoxic-ischemic encephalopathy predicts neurodevelopmental outcome at 18–24 months. J. Perinat. Med. 2020, 48, 296–303. [Google Scholar] [CrossRef]
- Zubčević, S.; Heljić, S.; Catibusić, F.; Užičanin, S.; Sadiković, M.; Krdzalic, B. Neurodevelopmental Follow Up After Therapeutic Hypothermia for Perinatal Asphyxia. Med. Arch. 2015, 69, 362–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burton, V.J.; Gerner, G.; Cristofalo, E.A.; Chung, S.-E.; Jennings, J.M.; Parkinson, C.; Koehler, R.C.; Chavez-Valdez, R.; Johnston, M.V.; Northington, F.J.; et al. A pilot cohort study of cerebral autoregulation and 2-year neurodevelopmental outcomes in neonates with hypoxic-ischemic encephalopathy who received therapeutic hypothermia. BMC Neurol. 2015, 15, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monzani, A.; Cosi, G.; Genoni, G.; Lavrano, M.; Peruzzi, C.; Pomella, R.; Ferrero, F. Early instrumental predictors of long-term neurodevelopmental impairment in newborns with perinatal asphyxia treated with therapeutic hypothermia. Signa Vitae 2018, 14, 81–85. [Google Scholar] [CrossRef] [Green Version]
- Xu, M.; Su, W.; Ma, L.; Liu, X.; Zhang, R.; Liu, R. Predictors of neurodevelopmental outcomes at 12 months in term newborns with hypoxic ischemic encephalopathy. Int. J. Clin. Exp. Med. 2016, 9, 6605–6612. [Google Scholar]
- Reiss, J.; Sinha, M.; Gold, J.; Bykowski, J.; Lawrence, S.M. Outcomes of Infants with Mild Hypoxic Ischemic Encephalopathy Who Did Not Receive Therapeutic Hypothermia. Biomed. Hub 2019, 4, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Boldingh, A.M.; Solevåg, A.L.; Nakstad, B. Outcomes following neonatal cardiopulmonary resuscitation. Tidsskr. Den Nor. Legeforening 2018, 138. [Google Scholar] [CrossRef]
- Schreglmann, M.; Ground, A.; Vollmer, B.; Johnson, M.J. Systematic review: Long-term cognitive and behavioural outcomes of neonatal hypoxic–ischaemic encephalopathy in children without cerebral palsy. Acta Paediatr. 2019, 109, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Carrera, J.M. (Ed.) Recommendations and Guidelines for Perinatal Medicine; Matres Mundi: Barcelona, Spain, 2007; pp. 354–355. [Google Scholar]
- Sarnat, H.B.; Sarnat, M.S. Neonatal encephalopathy following fetal distress. A clinical and electroencephalographic study. Arch. Neurol. 1976, 33, 696–705. [Google Scholar] [CrossRef] [PubMed]
- Bayley, N. The Bayley Scales of Infant Development II; New York Psychological Corporation: New York, NY, USA, 1993. [Google Scholar]
- Woolger, C. Wechsler Intelligence Scale for Children-Third Edition. In Understanding Psychological Assessment. Perspectives on Individual Differences; Dorfman, W.I., Hersen, M., Eds.; Springer: Boston, MA, USA, 2001. [Google Scholar] [CrossRef]
- Rosenbaum, P.L.; Palisano, R.J.; Bartlett, D.J.; Galuppi, B.E.; Russell, D.J. Development of the Gross Motor Function Classification System for cerebral palsy. Dev. Med. Child Neurol. 2008, 50, 249–253. [Google Scholar] [CrossRef]
- Horsman, J.; Furlong, W.; Feeny, D.; Torrance, G. The Health Utilities Index (HUI): Concepts, measurement properties and applications. Health Qual. Life Outcomes 2003, 1, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, H.; Eddama, O.; Azzopardi, D.; Edwards, A.D.; Strohm, B.; Rivero-Arias, O. Hypothermia for perinatal asphyxia: Trial-based quality of life at 6–7 years. Arch. Dis. Child. 2018, 103, 654–659. [Google Scholar] [CrossRef]
- Liu, X.; Jary, S.; Cowan, F.; Thoresen, M. Reduced infancy and childhood epilepsy following hypothermia-treated neonatal encephalopathy. Epilepsia 2017, 58, 1902–1911. [Google Scholar] [CrossRef] [PubMed]
- Perez, A.; Ritter, S.; Brotschi, B.; Werner, H.; Caflisch, J.; Martin, E.; Latal, B. Long-Term Neurodevelopmental Outcome with Hypoxic-Ischemic Encephalopathy. J. Pediatr. 2013, 163, 454–459.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azzopardi, D.; Strohm, B.; Marlow, N.; Brocklehurst, P.; Deierl, A.; Eddama, O.; Goodwin, J.; Halliday, H.; Juszczak, E.; Kapellou, O.; et al. Effects of Hypothermia for Perinatal Asphyxia on Childhood Outcomes. N. Engl. J. Med. 2014, 371, 140–149. [Google Scholar] [CrossRef] [Green Version]
- Lee-Kelland, R.; Jary, S.; Tonks, J.; Cowan, F.M.; Thoresen, M.; Chakkarapani, E. School-age outcomes of children without cerebral palsy cooled for neonatal hypoxic–ischaemic encephalopathy in 2008–2010. Arch. Dis. Child. Fetal Neonatal Ed. 2019, 105, 8–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pappas, A.; Shankaran, S.; McDonald, S.; Vohr, B.R.; Hintz, S.R.; Ehrenkranz, R.A.; Tyson, J.E.; Yolton, K.; Das, A.; Bara, R.; et al. Cognitive Outcomes After Neonatal Encephalopathy. Pediatrics 2015, 135, e624–e634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Schie, P.E.; Schijns, J.; Becher, J.G.; Barkhof, F.; van Weissenbruch, M.M.; Vermeulen, R.J. Long-term motor and behavioral outcome after perinatal hypoxic-ischemic encephalopathy. Eur. J. Paediatr. Neurol. 2015, 19, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Jary, S.; Lee-Kelland, R.; Tonks, J.; Cowan, F.M.; Thoresen, M.; Chakkarapani, E. Motor performance and cognitive correlates in children cooled for neonatal encephalopathy without cerebral palsy at school age. Acta Paediatr. 2019, 108, 1773–1780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, B.C.; Doherty, E.; Grehan, A.; Madigan, C.; McGarvey, C.; Mulvany, S.; Matthews, T.G.; King, M.D. Neurodevelopmental outcome in survivors of hypoxic ischemic encephalopathy without cerebral palsy. Eur. J. Pediatr. 2018, 177, 19–32. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
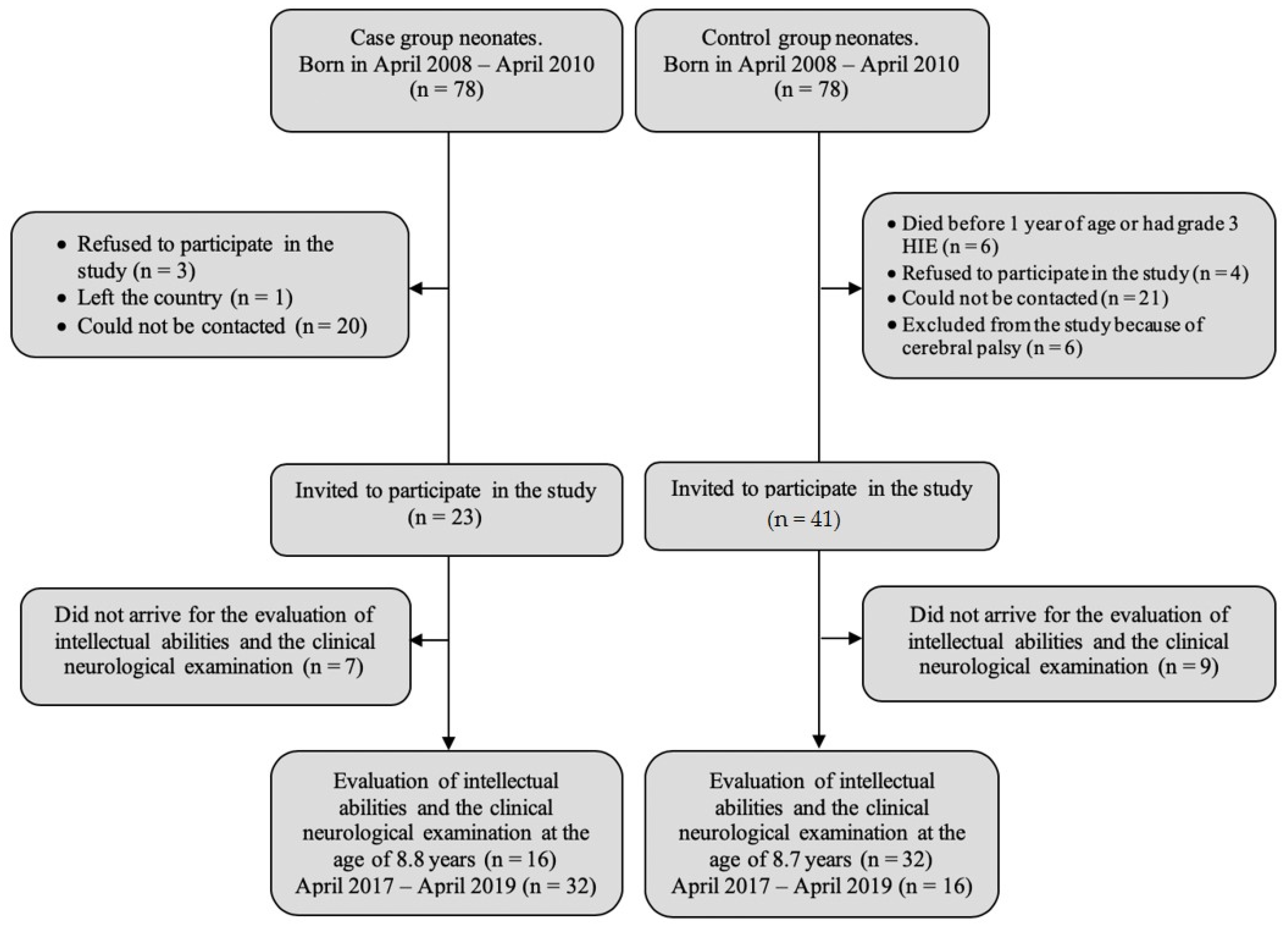
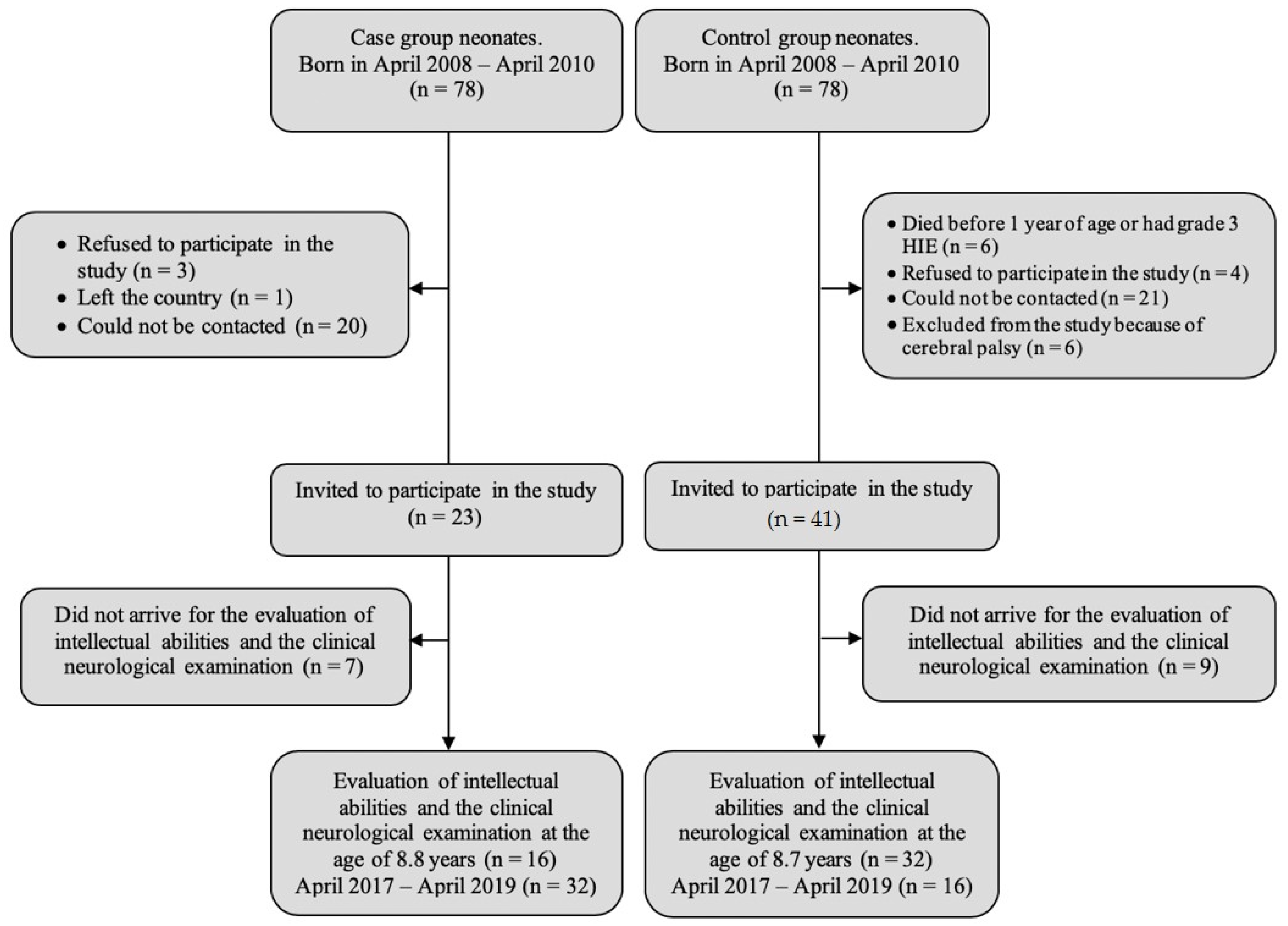
| Characteristics | Case Group | Control Group |
|---|---|---|
| n = 32 | n = 16 | |
| Sex, n (%) | ||
| boys | 13 (40.6) | 7 (43.8) |
| girls | 19 (59.4) | 9 (56.3) |
| Age (years) | ||
| Min. | 8.03 | 8.05 |
| Max. | 9.08 | 9.09 |
| M(SD) | 8.8 (0.417) | 8.7 (0.45) |
| Birth weight (g), n (%) | ||
| <3500 | 16 (50) | 5 (31.25) |
| >3501 | 16 (50) | 11 (68.75) |
| M(SD) | 33.3 (10.05) | 33.7 (8.12) |
| Gestational age at birth (weeks), n (%) | ||
| 37 | 2 (6.3) | 1 (6.3) |
| 38 | 3 (9.4) | 0 (0) |
| 39 | 8 (25.0) | 5 (31.3) |
| 40 | 13 (40.6) | 5 (31.3) |
| 41 | 6 (18.8) | 5 (31.3) |
| M(SD) | 39.56 (1.105) | 39.81 (1.109) |
| Apgar score at 1 min. | ||
| Min. | 0 | 8 |
| Max. | 7 | 10 |
| M (SD) | 4.3 (1.7) | 9.1 (0.6) |
| Apgar score at 5 min. | ||
| Min. | 4 | 9 |
| Max. | 9 | 10 |
| M (SD) | 6.94 (1.1) | 9.5 (0.5) |
| Extent of cardiopulmonary resuscitation after birth, (%) | ||
| No resuscitation measures applied | 0 (0) | 16 (100) |
| IS | 3 (6.3) | 0 (0) |
| IS-PPV | 25 (52.1) | 0 (0) |
| IS-PPV-CC | 2 (4.2) | 0 (0) |
| IS-PPV-CC-M | 2 (4.2) | 0 (0) |
| HIE, n (%) | ||
| not detected | 5 (15.6) | 16 (100) |
| mild | 15 (46.9) | 0 (0) |
| moderate | 12 (37.5) | 0 (0) |
| Composite Score | Classification | Theoretical Normal Curve |
|---|---|---|
| 130 or above | Very superior | 2.2 |
| 120–129 | Superior | 6.7 |
| 110–119 | High average | 16.1 |
| 90–109 | Average | 50.0 |
| 80–89 | Low average | 16.1 |
| 70–79 | Borderline | 6.7 |
| 69 or below | Extremely low | 2.2 |
| Variable | Case Group (n = 32), Proc. (n) | Control Group (n = 16), Proc. (n) | p (χ2) |
|---|---|---|---|
| Abnormalities in neurological examination | 43.8 (14) | 25 (4) | 0.21 |
| Changes in cranial nerves | 0.0 (0) | 6.3 (1) | 0.15 |
| Changes in upper and lower limbs | 40.6 (13) | 12.5 (2) | 0.05 |
| Changes in cerebellar function | 15.6 (5) | 0.0 (0) | 0.1 |
| Gait disorders | 9.4 (3) | 0.0 (0) | 0.2 |
| Muscle tone disorders | 9.4 (3) | 0.0 (0) | 0.2 |
| Abnormalities detected during neurological examination (tics, myoclonus, tremor, muscle atrophy) | 18.8 (6) | 6.3 (1) | 0.21 |
| Epilepsy | 12.5 (4) | 0.0 (0) | 0.14 |
| Neuromotor function (GMFCS) | |||
| No abnormality | 75 (24) | 87.5 (14) | 0.55 |
| Level I | 21.9 (7) | 12.5 (2) | |
| Level II | 3.1 (1) | 0.0 (0) | |
| Level III | 0.0 (0) | 0.0 (0) | |
| Level IV | 0.0 (0) | 0.0 (0) | |
| Level V | 0.0 (0) | 0.0 (0) | |
| Health-related quality of life (HUI3) | |||
| Vision | |||
| Level 1 | 87.5 (28) | 87.5 (14) | 1.0 |
| Level 2 | 12.5 (4) | 12.5 (2) | |
| Level 3 | 0.0 (0) | 0.0 (0) | |
| Level 4 | 0.0 (0) | 0.0 (0) | |
| Level 5 | 0.0 (0) | 0.0 (0) | |
| Level 6 | 0.0 (0) | 0.0 (0) | |
| Hearing | |||
| Level 1 | 96.9 (31) | 100 (16) | 0.48 |
| Level 2 | 3.1 (1) | 0.0 (0) | |
| Level 3 | 0.0 (0) | 0.0 (0) | |
| Level 4 | 0.0 (0) | 0.0 (0) | |
| Level 5 | 0.0 (0) | 0.0 (0) | |
| Level 6 | 0.0 (0) | 0.0 (0) | |
| Speech | |||
| Level 1 | 93.8 (30) | 93.8 (15) | 1.0 |
| Level 2 | 6.3 (2) | 6.3 (1) | |
| Level 3 | 0.0 (0) | 0.0 (0) | |
| Level 4 | 0.0 (0) | 0.0 (0) | |
| Level 5 | 0.0 (0) | 0.0 (0) | |
| Level 6 | 0.0 (0) | 0.0 (0) | |
| Emotion | |||
| Level 1 | 100 (32) | 100 (16) | 1.0 |
| Level 2 | 0.0 (0) | 0.0 (0) | |
| Level 3 | 0.0 (0) | 0.0 (0) | |
| Level 4 | 0.0 (0) | 0.0 (0) | |
| Level 5 | 0.0 (0) | 0.0 (0) | |
| Level 6 | 0.0 (0) | 0.0 (0) | |
| Pain | |||
| Level 1 | 90.6 (29) | 81.3 (13) | 0.65 |
| Level 2 | 6.3 (2) | 12.5 (2) | |
| Level 3 | 3,1 (1) | 6.3 (1) | |
| Level 4 | 0.0 (0) | 0.0 (0) | |
| Level 5 | 0.0 (0) | 0.0 (0) | |
| Level 6 | 0.0 (0) | 0.0 (0) | |
| Ambulation | |||
| Level 1 | 75.0 (24) | 93.8 (15) | 0.12 |
| Level 2 | 25.0 (8) | 6.3 (1) | |
| Level 3 | 0.0 (0) | 0.0 (0) | |
| Level 4 | 0.0 (0) | 0.0 (0) | |
| Level 5 | 0.0 (0) | 0.0 (0) | |
| Level 6 | 0.0 (0) | 0.0 (0) | |
| Dexterity | |||
| Level 1 | 93.8 (30) | 100 (16) | 0.59 |
| Level 2 | 3.1 (1) | 0.0 (0) | |
| Level 3 | 3.1(1) | 0.0 (0) | |
| Level 4 | 0.0 (0) | 0.0 (0) | |
| Level 5 | 0.0 (0) | 0.0 (0) | |
| Level 6 | 0.0 (0) | 0.0 (0) | |
| Cognition | |||
| Level 1 | 68.8 (22) | 87.5 (14) | 0.36 |
| Level 2 | 25.0 (8) | 12.5 (2) | |
| Level 3 | 6.3 (2) | 0.0 (0) | |
| Level 4 | 0.0 (0) | 0.0 (0) | |
| Level 5 | 0.0 (0) | 0.0 (0) | |
| Level 6 | 0.0 (0) | 0.0 (0) |
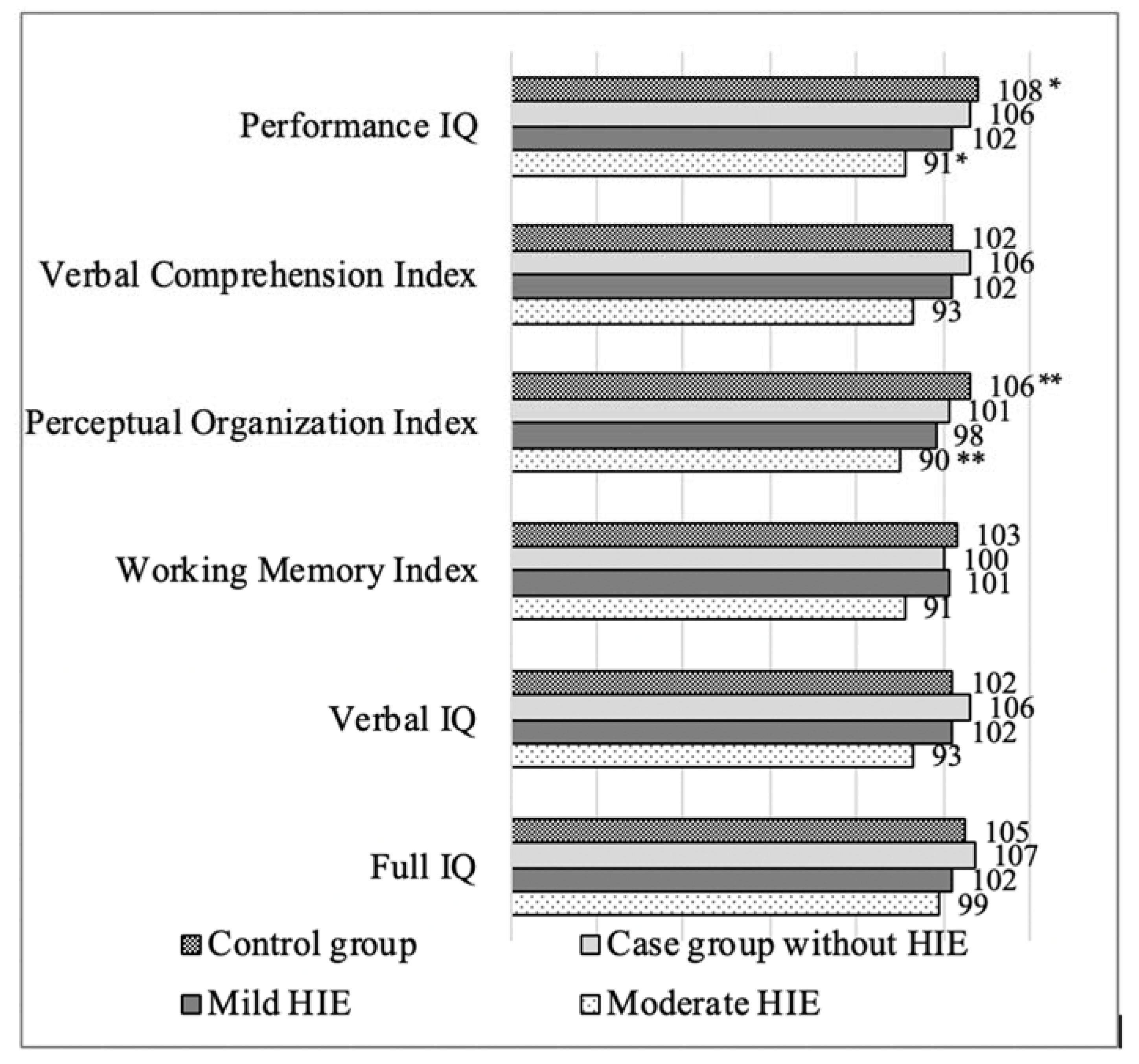
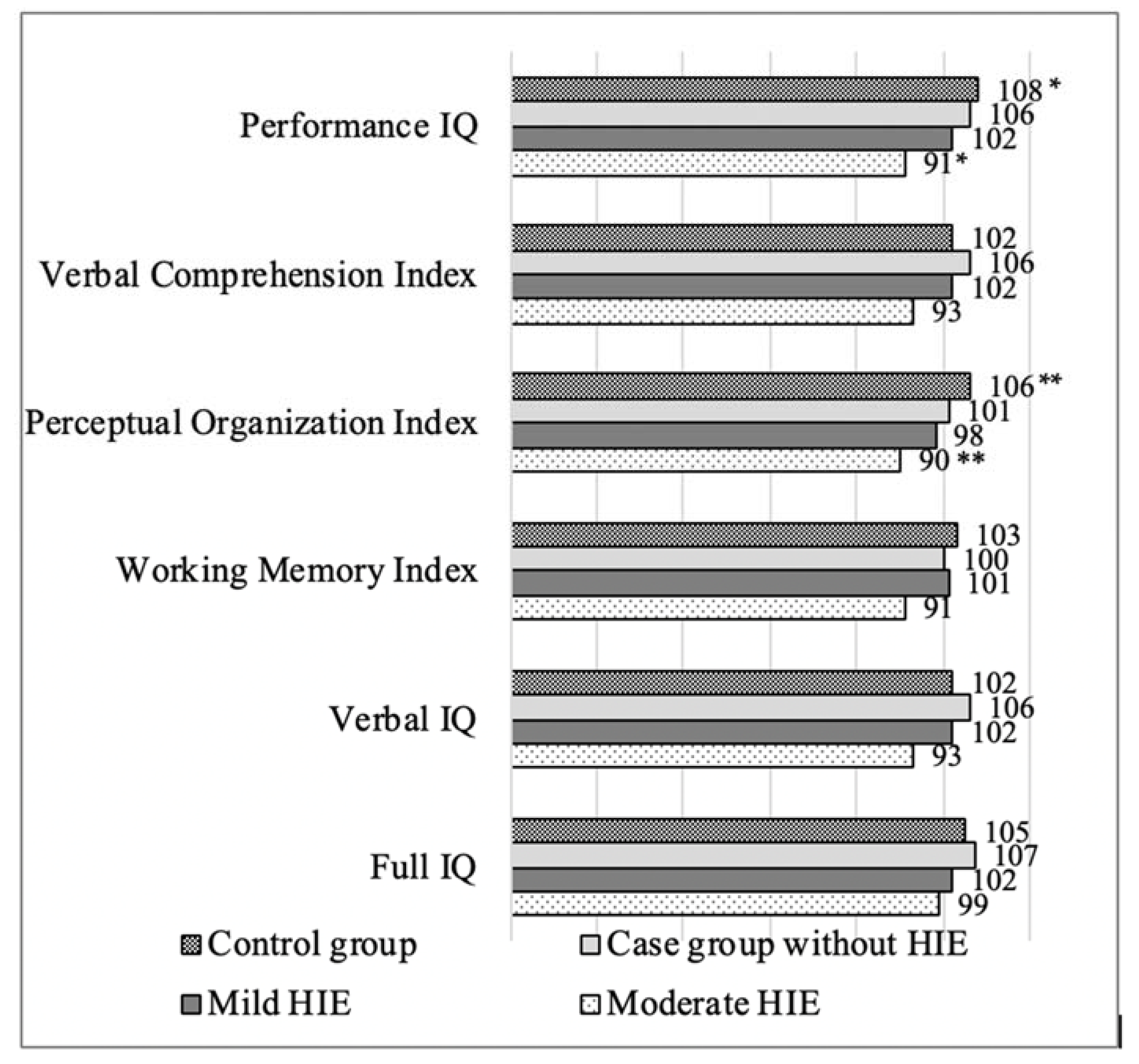
| Cognitive Assessments | Case Group (n = 32) Mean (SD) | Control group (n = 16) Mean (SD) | p |
|---|---|---|---|
| Full IQ | 87 (16.86) | 107 (12.15) | <0.001 |
| Verbal IQ | 89 (17.45) | 105 (11.55) | 0.002 |
| Verbal Comprehension Index | 89 (17.36) | 105 (10.74) | 0.002 |
| Working Memory Index | 89 (15.68) | 104 (11.84) | 0.002 |
| Performance IQ | 87 (16.51) | 108 (15.48) | <0.001 |
| Perceptual Organization Index | 85 (15.71) | 105 (15.93) | <0.001 |
| Cognitive Assessments | Case Group % (n) | Control Group % (n) | p |
|---|---|---|---|
| Full IQ | 18.8 (6) | 12.5 (2) | 0.58 |
| Verbal IQ | 18.8 (6) | 6.3 (1) | 0.25 |
| Verbal Comprehension Index | 18.8 (6) | 12.5 (2) | 0.58 |
| Working Memory Index | 25.0 (8) | 18.8 (3) | 0.63 |
| Performance IQ | 28.1 (9) | 12.5 (2) | 0.23 |
| Perceptual Organization Index | 37.5 (12) | 12.5 (2) | 0.075 |
| IQ Coefficient Scores at an Early School Age | Slight Mental Retardation at the Age of 1 Year (n = 4) Mean (SD) | Normal Mental Development at the Age of 1 Year (n = 27/8 *) Mean (SD) | p |
|---|---|---|---|
| Full IQ | 75.8 (21.1) | 101.8 (15.1)/111.5 (21.1) * | 0.027/0.017 * |
| Verbal IQ | 78.0 (15.8) | 102.3 (15.4)/110.1 (9.76) * | 0.01/0.006 * |
| Verbal Comprehension Index | 79.0 (13.3) | 101.9 (15.5)/110.1 (9.70) * | 0.018/0.006 * |
| Working Memory Index | 76.5 (20.0) | 100.3 (12.8)/107.4 (6.30) * | 0.014/0.008 * |
| Performance IQ | 77.3 (25.3) | 100.7 (16.6)/110.9 (16.50) * | 0.072/0.061 * |
| Perceptual Organization Index | 77.5 (23.5) | 97.4 (17.1)/105.0 (19.50) * | 0.067/0.05 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dzikienė, R.; Lukoševičius, S.; Laurynaitienė, J.; Marmienė, V.; Nedzelskienė, I.; Tamelienė, R.; Rimdeikienė, I.; Kudrevičienė, A. Long-Term Outcomes of Perinatal Hypoxia and Asphyxia at an Early School Age. Medicina 2021, 57, 988. https://doi.org/10.3390/medicina57090988
Dzikienė R, Lukoševičius S, Laurynaitienė J, Marmienė V, Nedzelskienė I, Tamelienė R, Rimdeikienė I, Kudrevičienė A. Long-Term Outcomes of Perinatal Hypoxia and Asphyxia at an Early School Age. Medicina. 2021; 57(9):988. https://doi.org/10.3390/medicina57090988
Chicago/Turabian StyleDzikienė, Renata, Saulius Lukoševičius, Jūratė Laurynaitienė, Vitalija Marmienė, Irena Nedzelskienė, Rasa Tamelienė, Inesa Rimdeikienė, and Aušrelė Kudrevičienė. 2021. "Long-Term Outcomes of Perinatal Hypoxia and Asphyxia at an Early School Age" Medicina 57, no. 9: 988. https://doi.org/10.3390/medicina57090988
APA StyleDzikienė, R., Lukoševičius, S., Laurynaitienė, J., Marmienė, V., Nedzelskienė, I., Tamelienė, R., Rimdeikienė, I., & Kudrevičienė, A. (2021). Long-Term Outcomes of Perinatal Hypoxia and Asphyxia at an Early School Age. Medicina, 57(9), 988. https://doi.org/10.3390/medicina57090988