
Bipolar Radiofrequency Ablation of Painful Spinal Bone Metastases Performed under Local Anesthesia: Feasibility Regarding Patient’s Experience and Pain Outcome

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedure and Anesthesia
- Needle pathway local anesthetic injection (a mixture of fast- and slow-acting anesthetic (lidocaine hydrochloride 1% (1/3) and ropivacaine hydrochloride 0.25% (2/3): from skin entry point to tumor, associated to an intratumoral block with the same mixture. Quantities of injectant depended on both tumor size and patient’s tolerance, without exceeding dose limits [10].
- Inhalation of nitrous oxide throughout the procedure.
- IV administration of paracetamol (1 g) started 5 min prior to procedure. IV injection of nalbuphin (20 mg) could be added on demand in case of persisting pain.
2.2. RFA Technique
2.3. Pain Assessment
3. Statistical Analysis
4. Results
4.1. Procedure
4.2. Pain
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sciubba, D.M.; Petteys, R.J.; Dekutoski, M.B.; Fisher, C.G.; Fehlings, M.G.; Ondra, S.L.; Rhines, L.D.; Gokaslan, Z.L. Diagnosis and management of metastatic spine disease. A review. J. Neurosurg. Spine 2010, 13, 94–108. [Google Scholar] [CrossRef]
- Coleman, R.E. Skeletal complications of malignancy. Cancer 1997, 80, 1588–1594. [Google Scholar] [CrossRef]
- Coleman, R.E. Metastatic bone disease: Clinical features, pathophysiology and treatment strategies. Cancer Treat. Rev. 2001, 27, 165–176. [Google Scholar] [CrossRef]
- Coleman, R.E. Clinical features of metastatic bone disease and risk of skeletal morbidity. Clin. Cancer Res. 2006, 12, 6243s–6249s. [Google Scholar] [CrossRef] [Green Version]
- Bach, F.; Larsen, B.H.; Rohde, K.; Borgesen, S.E.; Gjerris, F.; Boge-Rasmussen, T.; Agerlin, N.; Rasmusson, B.; Stjernholm, P.; Sorensen, P.S. Metastatic spinal cord compression. Occurrence, symptoms, clinical presentations and prognosis in 398 patients with spinal cord compression. Acta Neurochir. 1990, 107, 37–43. [Google Scholar] [CrossRef]
- Helweg-Larsen, S.; Sorensen, P.S. Symptoms and signs in metastatic spinal cord compression: A study of progression from first symptom until diagnosis in 153 patients. Eur. J. Cancer 1994, 30, 396–398. [Google Scholar] [CrossRef]
- Spiegel, D.; Sands, S.; Koopman, C. Pain and depression in patients with cancer. Cancer 1994, 74, 2570–2578. [Google Scholar] [CrossRef]
- Agarawal, J.P.; Swangsilpa, T.; van der Linden, Y.; Rades, D.; Jeremic, B.; Hoskin, P.J. The role of external beam radiotherapy in the management of bone metastases. Clin. Oncol. 2006, 18, 747–760. [Google Scholar] [CrossRef] [PubMed]
- Lutz, S.; Berk, L.; Chang, E.; Chow, E.; Hahn, C.; Hoskin, P.; Howell, D.; Konski, A.; Kachnic, L.; Lo, S.; et al. Palliative radiotherapy for bone metastases: An ASTRO evidence-based guideline. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 965–976. [Google Scholar] [CrossRef]
- Poulsen, H.S.; Nielsen, O.S.; Klee, M.; Rorth, M. Palliative irradiation of bone metastases. Cancer Treat. Rev. 1989, 16, 41–48. [Google Scholar] [CrossRef]
- Anselmetti, G.C.; Manca, A.; Ortega, C.; Grignani, G.; Debernardi, F.; Regge, D. Treatment of extraspinal painful bone metastases with percutaneous cementoplasty: A prospective study of 50 patients. Cardiovasc. Interv. Radiol. 2008, 31, 1165–1173. [Google Scholar] [CrossRef]
- Saliou, G.; Kocheida, E.M.; Lehmann, P.; Depriester, C.; Paradot, G.; Le Gars, D.; Balut, A.; Deramond, H. Percutaneous vertebroplasty for pain management in malignant fractures of the spine with epidural involvement. Radiology 2010, 254, 882–890. [Google Scholar] [CrossRef] [Green Version]
- Alemann, G.; Kastler, A.; Barbe, D.A.; Aubry, S.; Kastler, B. Treatment of painful extraspinal bone metastases with percutaneous bipolar radiofrequency under local anesthesia: Feasibility and efficacy in twenty-eight cases. J. Palliat. Med. 2014, 17, 947–952. [Google Scholar] [CrossRef] [PubMed]
- Kastler, A.; Alnassan, H.; Aubry, S.; Kastler, B. Microwave thermal ablation of spinal metastatic bone tumors. J. Vasc. Interv. Radiol. 2014, 25, 1470–1475. [Google Scholar] [CrossRef] [PubMed]
- Kastler, A.; Alnassan, H.; Pereira, P.L.; Alemann, G.; Barbe, D.A.; Aubry, S.; Tiberghien, F.; Kastler, B. Analgesic effects of microwave ablation of bone and soft tissue tumors under local anesthesia. Pain Med. 2013, 14, 1873–1881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, R.T.; Jakobs, T.F.; Trumm, C.; Weber, C.; Helmberger, T.K.; Reiser, M.F. Radiofrequency ablation in combination with osteoplasty in the treatment of painful metastatic bone disease. J. Vasc. Interv. Radiol. 2008, 19, 419–425. [Google Scholar] [CrossRef]
- Callstrom, M.R.; Atwell, T.D.; Charboneau, J.W.; Farrell, M.A.; Goetz, M.P.; Rubin, J.; Sloan, J.A.; Novotny, P.J.; Welch, T.J.; Maus, T.P.; et al. Painful metastases involving bone: Percutaneous image-guided cryoablation--prospective trial interim analysis. Radiology 2006, 241, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Clarencon, F.; Jean, B.; Pham, H.P.; Cormier, E.; Bensimon, G.; Rose, M.; Maksud, P.; Chiras, J. Value of percutaneous radiofrequency ablation with or without percutaneous vertebroplasty for pain relief and functional recovery in painful bone metastases. Skelet. Radiol. 2011, 42, 25–36. [Google Scholar] [CrossRef]
- Munk, P.L.; Rashid, F.; Heran, M.K.; Papirny, M.; Liu, D.M.; Malfair, D.; Badii, M.; Clarkson, P.W. Combined cementoplasty and radiofrequency ablation in the treatment of painful neoplastic lesions of bone. J. Vasc. Interv. Radiol. 2009, 20, 903–911. [Google Scholar] [CrossRef]
- Toyota, N.; Naito, A.; Kakizawa, H.; Hieda, M.; Hirai, N.; Tachikake, T.; Kimura, T.; Fukuda, H.; Ito, K. Radiofrequency ablation therapy combined with cementoplasty for painful bone metastases: Initial experience. Cardiovasc. Interv. Radiol. 2005, 28, 578–583. [Google Scholar] [CrossRef]
- Kostuik, J.P. Differential diagnosis and surgical treatment of metastatic spine tumors. In The Adult Spine; Raven Press: New York, NY, USA, 1991; pp. 861–888. [Google Scholar]
- Kastler, B. Interventional Radiology in Pain Treatment; Springer: Berlin, Germany, 2007. [Google Scholar]
- Thacker, P.G.; Callstrom, M.R.; Curry, T.B.; Mandrekar, J.N.; Atwell, T.D.; Goetz, M.P.; Rubin, J. Palliation of painful metastatic disease involving bone with imaging-guided treatment: Comparison of patients’ immediate response to radiofrequency ablation and cryoablation. Am. J. Roentgenol. 2011, 197, 510–515. [Google Scholar] [CrossRef]
- Kojima, H.; Tanigawa, N.; Kariya, S.; Komemushi, A.; Shomura, Y.; Sawada, S. Clinical assessment of percutaneous radiofrequency ablation for painful metastatic bone tumors. Cardiovasc. Interv. Radiol. 2006, 29, 1022–1026. [Google Scholar] [CrossRef] [PubMed]
- Nakada, S.Y.; Jerde, T.J.; Warner, T.F.; Wright, A.S.; Haemmerich, D.; Mahvi, D.M.; Lee, F.T., Jr. Bipolar radiofrequency ablation of the kidney: Comparison with monopolar radiofrequency ablation. J. Endourol. 2003, 17, 927–933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cazzato, R.L.; de Rubeis, G.; de Marini, P.; Dalili, D.; Koch, G.; Auloge, P.; Garnon, J.; Gangi, A. Percutaneous microwave ablation of bone tumors: A systematic review. Eur. Radiol. 2021, 31, 3530–3541. [Google Scholar] [CrossRef] [PubMed]
- Angileri, S.A.; Granata, G.; Savoldi, A.P.; Roda, G.M.; Di Meglio, L.; Grillo, P.; Tortora, S.; Arrichiello, A.; Papa, M.; Liguori, A.; et al. Cooled radiofrequency ablation technology for painful bone tumors. Acta Biomed. 2020, 91, e2020007. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.; Hopkins, T.; Morris, J.; Tran, N.D.; David, E.; Massari, F.; Farid, H.; Vogel, A.; O’Connell, W.G.; Sunenshine, P.; et al. Radiofrequency Ablation for the Palliative Treatment of Bone Metastases: Outcomes from the Multicenter OsteoCool Tumor Ablation Post-Market Study (OPuS One Study) in 100 Patients. J. Vasc. Interv. Radiol. 2020, 31, 1745–1752. [Google Scholar] [CrossRef] [PubMed]
- Tomasian, A.; Gangi, A.; Wallace, A.N.; Jennings, J.W. Percutaneous Thermal Ablation of Spinal Metastases: Recent Advances and Review. Am. J. Roentgenol. 2018, 210, 142–152. [Google Scholar] [CrossRef]
- Tsoumakidou, G.; Garnon, J.; Ramamurthy, N.; Buy, X.; Gangi, A. Interest of electrostimulation of peripheral motor nerves during percutaneous thermal ablation. Cardiovasc. Interv. Radiol. 2013, 36, 1624–1628. [Google Scholar] [CrossRef]
- Buy, X.; Tok, C.H.; Szwarc, D.; Bierry, G.; Gangi, A. Thermal protection during percutaneous thermal ablation procedures: Interest of carbon dioxide dissection and temperature monitoring. Cardiovasc. Interv. Radiol. 2009, 32, 529–534. [Google Scholar] [CrossRef]
- Ing, E.B.; Philteos, J.; Sholohov, G.; Kim, D.T.; Nijhawan, N.; Mark, P.W.; Gilbert, J. Local anesthesia and anxiolytic techniques for oculoplastic surgery. Clin. Ophthalmol. 2019, 13, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Pan, Q.; Xu, L.; Lin, R.; Dai, J.; Chen, X.; Jiang, M.; Chen, Z. Comparison of analgesic and anxiolytic effects of nitrous oxide in burn wound treatment: A single-blind prospective randomized controlled trial. Medicine 2019, 98, e18188. [Google Scholar] [CrossRef] [PubMed]
- Dennis, K.; Wong, K.; Zhang, L.; Culleton, S.; Nguyen, J.; Holden, L.; Jon, F.; Tsao, M.; Danjoux, C.; Barnes, E.; et al. Palliative radiotherapy for bone metastases in the last 3 months of life: Worthwhile or futile? Clin. Oncol. 2011, 23, 709–715. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Sex/Age | Primary | Lesion Level | Size (mm) | Type | Soft-Tissue Involvement | Posterior Wall Involvement | Cementoplasty |
|---|---|---|---|---|---|---|---|
| 1-M/46 | melanoma | body T6 | 16 × 25 × 12 | lytic | no | yes | yes |
| 2-M/54 | lung | body L1 | 29 × 35 × 13 | lytic | no | no | yes |
| 3-M/58 | lung | body L2 | 30 × 30 × 26 | lytic | no | no | yes |
| 4-M/56 | lung | body T7 | 15 × 26 × 13 | lytic | no | no | yes |
| body T8 | 17 × 28 × 12 | lytic | no | no | yes | ||
| 5-F/75 | lung | body L1 | 61 × 58 × 20 | lytic | yes | yes | yes |
| 6-F/55 | lung | body L5 | 25 × 12 × 33 | lytic | yes | no | yes |
| 7-M/60 | lung | pedicle L T12 | 54 × 32 × 20 | lytic | yes | no | no |
| 8-M/72 | lung | R Transverse process T5 | 16 × 19 × 13 | lytic | yes | no | no |
| 9-M/59 | lung | body T10 | 32 × 35 × 20 | lytic | yes | no | yes |
| 10-M/76 | prostate | body L3 | 32 × 27 × 19 | osteoblastic | no | yes | yes |
| 11-M/56 | urothelial | body L3 | 13 × 13 × 12 | lytic | yes | no | no |
| 12-M/74 | prostate | body T9 | 16 × 19 × 12 | osteoblastic | no | yes | no |
| 13-M/59 | kidney | body L2 | 14 × 15 × 14 | lytic | yes | no | yes |
| 14-M/44 | head and neck | body T12 | 15 × 13 × 8 | osteoblastic | no | no | no |
| 15-M/61 | hepatocellular carcinoma | pedicle L L5 | 38 × 47 × 22 | lytic | yes | yes | no |
| pedicle L L4 et L5 | 54 × 30 × 33 | lytic | yes | yes | no | ||
| 16-F/57 | breast | body T12 | 40 × 57 × 11 | mixt | no | no | yes |
| 17-M/75 | pancreas | R pedicle C7/T1 | 55 × 44 × 40 | lytic | yes | yes | no |
| 18-M/63 | lung | pedicle R L2 | 15 × 20 × 16 | lytic | no | yes | no |
| 19-F/69 | neuroendocrine | sacrum L S1 | 28 × 31 × 20 | lytic | no | no | no |
| 20-M/61 | pancreas | body L2 | 45 × 40 × 22 | lytic | no | no | yes |
| 21-F/35 | breast | body L3 | 25 × 29 × 21 | lytic | no | no | yes |
| 22-F/46 | colorectal | body L4 | 22 × 38 × 24 | lytic | yes | no | yes |
| SI right | 19 × 30 × 18 | lytic | no | no | yes | ||
| 23-M/76 | colorectal | body L1 | 21 × 18 × 13 | lytic | no | no | yes |
| 24-M/63 | colorectal | L Transverse process T6 | 10 × 10 × 10 | lytic | yes | no | no |
| 25-F/66 | colorectal | sacrococcygeal | 56 × 55 × 71 | lytic | yes | yes | no |
| colorectal | sacrococcygeal | 50 × 56 × 45 | lytic | yes | yes | no |
| Patient | VAS Scores | Tolerance | |||||
|---|---|---|---|---|---|---|---|
| Before Procedure | 24 h | 1 Month | 3 Month | 6 Month | 12 Month | ||
| 1 | 10 | 5 | 0 | 1 | 2 | _ | 1 |
| 2 | 10 | 1 | 2 | 0 | 0 | _ | 0 |
| 3 | 9 | 2 | 1 | 3 | 4 | 0 | 0 |
| 4 | 9 | 2 | 2 | 0 | 0 | 0 | 1 |
| 8 | 0 | 0 | 0 | _ | _ | 1 | |
| 5 | 10 | 1 | 0 | 2 | 1 | 0 | 0 |
| 6 | 9 | 4 | 0 | 4 | 5 | lost | 0 |
| 7 | 9 | 7 | 0 | 6 | 3 | 4 | 0 |
| 8 | 10 | 0 | 9 | 7 | _ | _ | 1 |
| 9 | 10 | 7 | 3 | _ | _ | _ | 1 |
| 10 | 9 | 2 | 0 | 0 | 4 | 4 | 1 |
| 11 | 8 | 0 | 0 | 4 | 2 | 3 | 1 |
| 12 | 8 | 0 | 0 | 0 | 0 | 0 | 0 |
| 13 | 9 | 0 | 3 | 0 | 0 | 5 | 0 |
| 14 | 6 | 0 | 0 | 0 | 0 | 0 | 0 |
| 15 | 8 | 3 | 4 | 4 | 0 | 0 | 1 |
| 4 | 4 | 4 | _ | _ | _ | 0 | |
| 16 | 8 | 0 | 0 | 0 | 2 | _ | 1 |
| 17 | 8 | 8 | 8 | _ | _ | _ | 2 |
| 18 | 7 | 4 | 3 | _ | _ | _ | 0 |
| 19 | 9 | 2 | 3 | 1 | 0 | 0 | 1 |
| 20 | 6 | 0 | 0 | _ | _ | _ | 0 |
| 21 | 9 | 0 | 2 | 4 | 5 | 5 | 0 |
| 22 | 9 | 1 | 2 | 1 | 3 | 1 | 0 |
| 9 | 2 | 1 | 2 | 2 | 2 | 1 | |
| 23 | 9 | 4 | 0 | 0 | 1 | _ | 1 |
| 24 | 8 | 4 | 3 | 3 | 3 | 3 | 0 |
| 25 | 9 | 1 | 2 | 0 | 0 | 0 | 0 |
| 8 | 0 | 0 | 0 | _ | _ | 0 | |
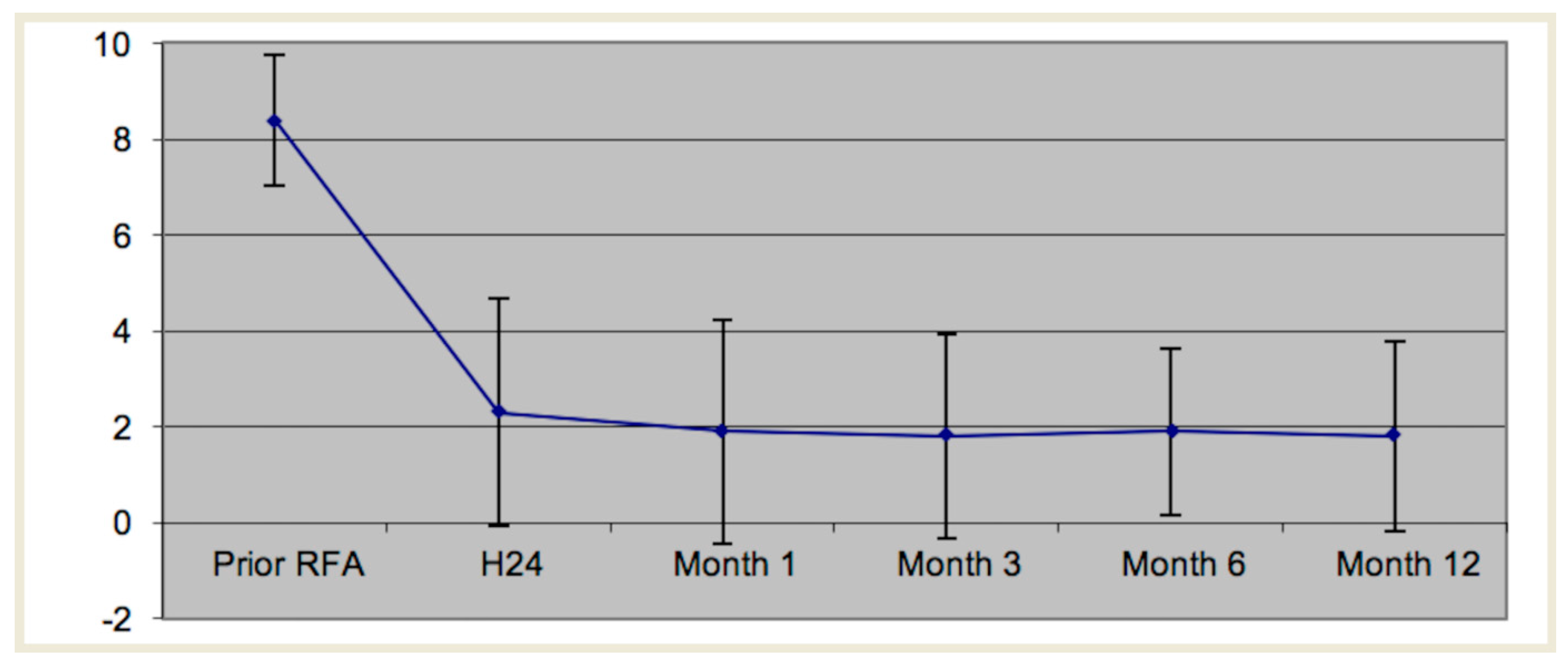
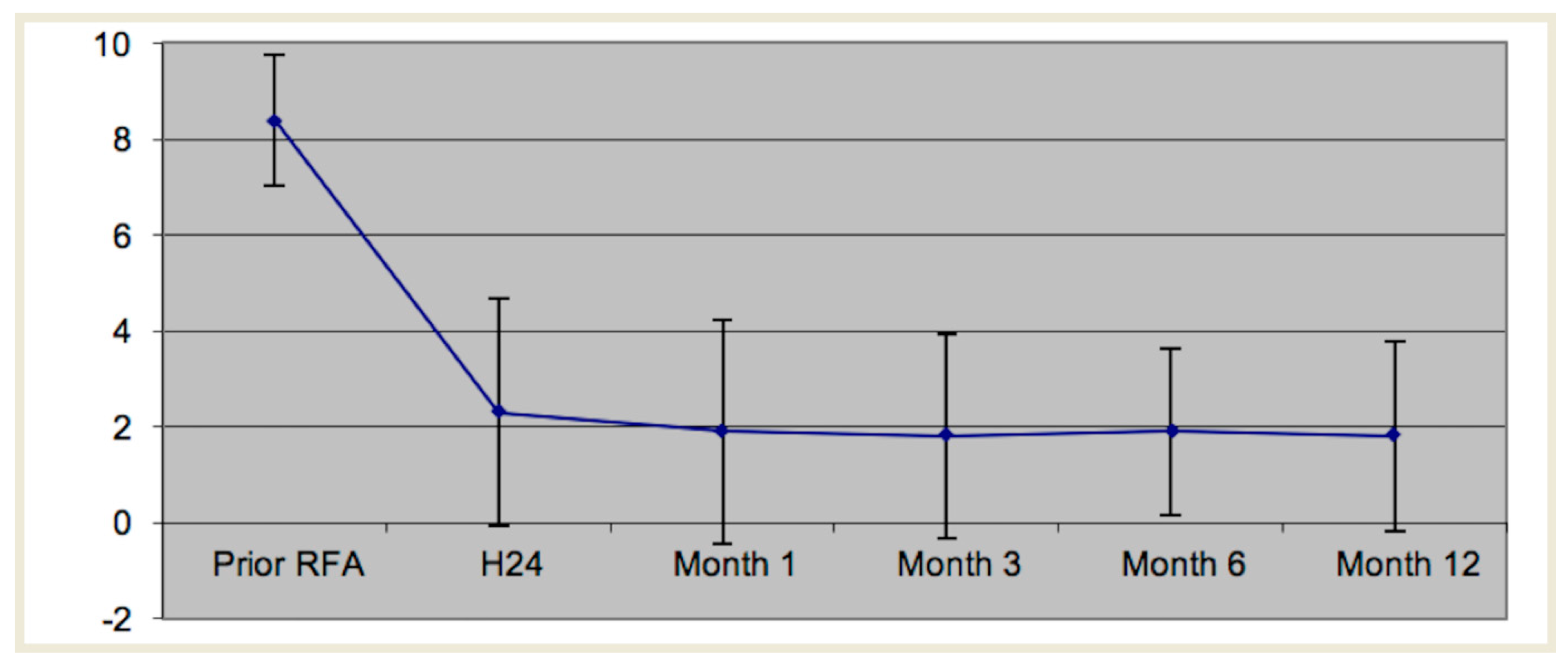
| Mean | 8.4 | 2.2 | 1.8 | 1.8 | 1.9 | 1.8 | |
| Standard Deviation | ±1.4 | ±2.4 | ±2.3 | ±2.2 | ±1.8 | ±2.1 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kastler, A.; Barbé, D.-A.; Alemann, G.; Hadjidekov, G.; Cornelis, F.H.; Kastler, B. Bipolar Radiofrequency Ablation of Painful Spinal Bone Metastases Performed under Local Anesthesia: Feasibility Regarding Patient’s Experience and Pain Outcome. Medicina 2021, 57, 966. https://doi.org/10.3390/medicina57090966
Kastler A, Barbé D-A, Alemann G, Hadjidekov G, Cornelis FH, Kastler B. Bipolar Radiofrequency Ablation of Painful Spinal Bone Metastases Performed under Local Anesthesia: Feasibility Regarding Patient’s Experience and Pain Outcome. Medicina. 2021; 57(9):966. https://doi.org/10.3390/medicina57090966
Chicago/Turabian StyleKastler, Adrian, Daniel-Ange Barbé, Guillaume Alemann, Georges Hadjidekov, Francois H. Cornelis, and Bruno Kastler. 2021. "Bipolar Radiofrequency Ablation of Painful Spinal Bone Metastases Performed under Local Anesthesia: Feasibility Regarding Patient’s Experience and Pain Outcome" Medicina 57, no. 9: 966. https://doi.org/10.3390/medicina57090966
APA StyleKastler, A., Barbé, D.-A., Alemann, G., Hadjidekov, G., Cornelis, F. H., & Kastler, B. (2021). Bipolar Radiofrequency Ablation of Painful Spinal Bone Metastases Performed under Local Anesthesia: Feasibility Regarding Patient’s Experience and Pain Outcome. Medicina, 57(9), 966. https://doi.org/10.3390/medicina57090966