
The Prognostic Significance of MACC1 Expression in Breast Cancer and Its Relationship to Immune Cells in the Tumor Microenvironment and Patient Survival

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Subjects and Methods
2.1. Study Population and Design
2.2. Breast Tissue Specimen
2.3. Histopathological Evaluation
2.4. Detection of MACC1 Gene Expression by Quantitative Reverse Transcription PCR
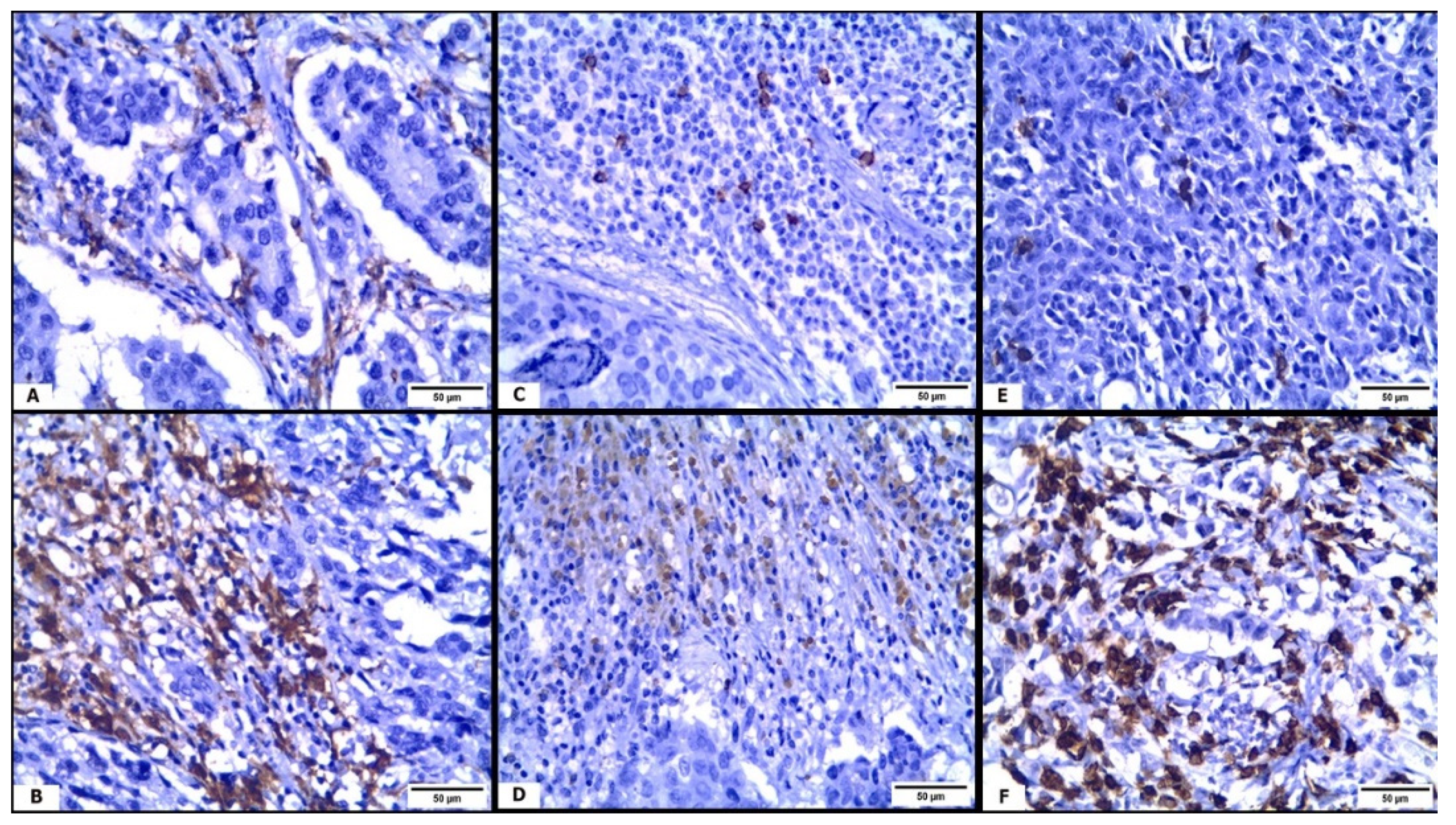
2.5. Immunohistochemical Staining
Quantification of Tumor-Infiltrating Immune Cells
2.6. Treatment and Follow-Up
2.7. Statistical Analysis
3. Results
3.1. The Clinicopathological Data
3.2. Evaluation of MACC1 mRNA Relative Expression by qRT-PCR
3.3. Relation between MACC1 mRNA Relative Expression and Clinicopathological Data
3.4. Immune Cells (CD163+ TAMs, CD8+ CTLs, and CD56+ NK Cells) in TME and Their Correlation with MACC1 mRNA Relative Expression
3.5. Relation between MACC1 mRNA Relative Expression and the Patients’ Survival
3.6. MACC1 mRNA Relative Expression as an Independent Prognostic Factors in BC Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BC | Breast cancer; |
| CTLs | Cytotoxic T lymphocytes; |
| DAB | diaminobenzidine; |
| ER | Estrogen receptor |
| HER2 | Human epidermal receptor 2; |
| HGF | Hepatocyte growth factor; |
| HRP | Horseradish peroxidase; |
| LHRH | Luteinizing-hormone-releasing hormone; |
| LVI | Lymphovascular invasion; |
| MACC1 | Metastasis-associated colon cancer-1; |
| NK cells | Natural killer cells; |
| OS | Overall survival; |
| PCR | Polymerase chain reaction; |
| PFS | Progression-free survival; |
| PR | Progesterone receptor; |
| TAMs | Tumor-associated macrophage; |
| TIIC | Tumor-infiltrating immune cells; |
| TME | Tumor microenvironment; |
| WHO | World Health Organization. |
References
- Gao, Z.-H.; Li, C.-X.; Liu, M.; Jiang, J.-Y. Predictive and prognostic role of tumour-infiltrating lymphocytes in breast cancer patients with different molecular subtypes: A meta-analysis. BMC Cancer 2020, 20, 1–14. [Google Scholar] [CrossRef]
- A Mina, L.; Lim, S.; Bahadur, S.W.; Firoz, A.T. Immunotherapy for the Treatment of Breast Cancer: Emerging New Data. Breast Cancer Targets Ther. 2019, 11, 321–328. [Google Scholar] [CrossRef]
- Stein, U.; Walther, W.; Arlt, F.; Schwabe, H.; Smith, J.; Fichtner, I.; Birchmeier, W.; Schlag, P.M. MACC1, a newly identified key regulator of HGF-MET sig-naling, predicts colon cancer metastasis. Nat. Med. 2009, 15, 59–67. [Google Scholar] [CrossRef]
- Zhang, Q.; Xu, P.; Lu, Y.; Dou, H. Correlation of MACC1/c-Myc Expression in Endometrial Carcinoma with Clini-cal/Pathological Features or Prognosis. Med. Sci. Monit. 2018, 24, 4738–4744. [Google Scholar] [CrossRef] [PubMed]
- Link, T.; Kuhlmann, J.D.; Kobelt, D.; Herrmann, P.; Vassileva, Y.D.; Kramer, M.; Frank, K.; Göckenjan, M.; Wimberger, P.; Stein, U. Clinical relevance of circulating MACC1 and S100A4 transcripts for ovarian cancer. Mol. Oncol. 2019, 13, 1268–1279. [Google Scholar] [CrossRef] [PubMed]
- Zheng, G.; You, C.; Qiu, Z.; Zheng, X. Expression of MACC1 protein in gastric cancer and its effect on proliferation and invasion of gastric cancer cells. Cell. Mol. Biol. 2020, 66, 111–117. [Google Scholar] [CrossRef]
- Radhakrishnan, H.; Walther, W.; Zincke, F.; Kobelt, D.; Imbastari, F.; Erdem, M.; Kortüm, B.; Dahlmann, M.; Stein, U. MACC1—the first decade of a key metastasis molecule from gene discovery to clinical translation. Cancer Metastasis Rev. 2018, 37, 805–820. [Google Scholar] [CrossRef]
- Soysal, S.; Tzankov, A.; Muenst, S.E. Role of the Tumor Microenvironment in Breast Cancer. Pathobiology 2015, 82, 142–152. [Google Scholar] [CrossRef]
- de Visser, K.E.; Eichten, A.; Coussens, L.M. Paradoxical roles of the immune system during cancer development. Nat. Rev. Cancer 2006, 6, 24–37. [Google Scholar] [CrossRef]
- Ge, Z.; Ding, S. The Crosstalk Between Tumor-Associated Macrophages (TAMs) and Tumor Cells and the Corresponding Tar-geted. Therapy. Front. Oncol. 2020, 10, 590941. [Google Scholar] [CrossRef] [PubMed]
- Mwafy, S.E.; El-Guindy, D.M. Pathologic assessment of tumor-associated macrophages and their histologic localization in in-vasive breast carcinoma. J. Egypt. Natl. Cancer Inst. 2020, 32, 6. [Google Scholar] [CrossRef]
- Vivier, E.; Raulet, D.H.; Moretta, A.; Caligiuri, M.A.; Zitvogel, L.; Lanier, L.L.; Yokoyama, W.M.; Ugolini, S. Innate or Adaptive Immunity? The Example of Natural Killer Cells. Science 2011, 331, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Ames, E.; Murphy, W.J. Advantages and clinical applications of natural killer cells in cancer immunotherapy. Cancer Immunol. Immunother. 2013, 63, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, M.L.; O Idowu, M.; Zhao, Y.; Khalak, H.; Payne, K.K.; Wang, X.-Y.; I Dumur, C.; Bedognetti, D.; Tomei, S.; A Ascierto, P.; et al. Molecular signatures mostly associated with NK cells are predictive of relapse free survival in breast cancer patients. J. Transl. Med. 2013, 11, 145. [Google Scholar] [CrossRef] [PubMed]
- Ostroumov, D.; Fekete-Drimusz, N.; Saborowski, M.; Kühnel, F.; Woller, N. CD4 and CD8 T lymphocyte interplay in controlling tumor growth. Cell. Mol. Life Sci. 2018, 75, 689–713. [Google Scholar] [CrossRef]
- Mao, Y.; Qu, Q.; Chen, X.; Huang, O.; Wu, J.; Shen, K. The Prognostic Value of Tumor-Infiltrating Lymphocytes in Breast Cancer: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0152500. [Google Scholar] [CrossRef]
- Hoon Tan, P.; Ellis, I.; Allison, K.; Brogi, E.; Fox, S.B.; Lakhani, S.; Lazar, A.J.; Morris, E.A.; Sahin, A.; Salgado, R.; et al. The 2019 World Health Organization classification of tumours of the breast. Histopathology 2020, 77, 181–185. [Google Scholar] [CrossRef]
- Elston, C.W.; Ellis, I.O. (Eds.) Assessment of histological grade. The Breast Edinburgh; Churchill Livingstone: New York, NY, USA, 1998; pp. 356–384. [Google Scholar]
- Giuliano, A.E.; Edge, S.B.; Hortobagyi, G.N. Eighth Edition of the AJCC Cancer Staging Manual: Breast Cancer. Ann. Surg. Oncol. 2018, 25, 1783–1785. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Ma, J.; Meng, Q.; Zhao, Z.-S.; Xu, W.-J. Prognostic Value and Clinical Pathology of MACC-1 and c-MET Expression in Gastric Carcinoma. Pathol. Oncol. Res. 2013, 19, 821–832. [Google Scholar] [CrossRef]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2 -ΔΔCT method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- Gwak, J.M.; Jang, M.H.; Kim, D.I.; Na Seo, A.; Park, S.Y. Prognostic Value of Tumor-Associated Macrophages According to Histologic Locations and Hormone Receptor Status in Breast Cancer. PLoS ONE 2015, 10, e0125728. [Google Scholar] [CrossRef]
- Al-Saleh, K.; El-Aziz, N.A.; Ali, A.; Abozeed, W.; El-Warith, A.A.; Ibraheem, A.; Ansari, J.; Al-Rikabi, A.; Husain, S.; Nabholtz, J.-M. Predictive and prognostic significance of CD8+ tumor-infiltrating lymphocytes in patients with luminal B/HER 2 negative breast cancer treated with neoadjuvant chemotherapy. Oncol. Lett. 2017, 14, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Stein, U.; Smith, J.; Walther, W.; Arlt, F. MACC1 controls Met: What a difference an Sp1 site makes. Cell Cycle 2009, 8, 2467–2469. [Google Scholar] [CrossRef]
- Wang, Z.; Li, Z.; Wu, C.; Wang, Y.; Xia, Y.; Chen, L.; Zhu, Q.; Chen, Y. MACC1 overexpression predicts a poor prognosis for non-small cell lung cancer. Med. Oncol. 2013, 31, 790. [Google Scholar] [CrossRef] [PubMed]
- Whiteside, T.L. The tumor microenvironment and its role in promoting tumor growth. Oncogene 2008, 27, 5904–5912. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, R.D.; Old, L.J.; Smyth, M.J. Cancer Immunoediting: Integrating Immunity’s Roles in Cancer Suppression and Promotion. Science 2011, 331, 1565. [Google Scholar] [CrossRef]
- Han, Z.; Gong, X.; Zhu, B.; Wu, S.; Yu, L.; Song, W.; Wang, D. Expression of ALDH 1, MACC 1, and KAI 1 in the triple-negative breast cancer and their clinical significance. Int. J. Clin. Exp. Pathol. 2017, 10, 5655–5664. [Google Scholar]
- Tan, W.; Xie, X.; Li, L.; Tang, H.; Ye, X.; Chen, L.; Tang, W.; Gao, J.; Pan, L.; Zhang, X.; et al. Diagnostic and prognostic value of serum MACC1 in breast cancer patients. Oncotarget 2016, 7, 84408–84415. [Google Scholar] [CrossRef]
- Ahmed, M.; Aslam, M. Serum MACC-1: A new biomarker for breast cancer. Oncotarget 2020, 11, 4521–4526. [Google Scholar] [CrossRef]
- Huang, Y.; Zhang, H.; Cai, J.; Fang, L.; Wu, J.; Ye, C.; Zhu, X.; Li, M. Overexpression of MACC1 and Its significance in human Breast Cancer Progression. Cell Biosci. 2013, 3, 16. [Google Scholar] [CrossRef] [PubMed]
- Dai, Z.J.; Liu, X.H.; Kang, H.F.; Wang, X.J.; Jin, T.B.; Zhang, S.Q.; Feng, T.; Ma, X.-B.; Wang, M.; Feng, Y.-J.; et al. Genetic Variation in Metastasis-Associated in Colon Cancer-1 and the Risk of Breast Cancer Among the Chinese Han Population: A STROBE-Compliant Observational Study. Medicine 2016, 95, e2801. [Google Scholar] [CrossRef]
- Muendlein, A.; Hubalek, M.; Geller-Rhomberg, S.; Gasser, K.; Winder, T.; Drexel, H.; Decker, T.; Mueller-Holzner, E.; Chamson, M.; Marth, C.; et al. Significant survival impact of MACC1 polymorphisms in HER2 positive breast cancer patients. Eur. J. Cancer 2014, 50, 2134–2141. [Google Scholar] [CrossRef]
- Birchmeier, C.; Birchmeier, W.; Gherardi, E.; Woude, G.F.V. Met, metastasis, motility and more. Nat. Rev. Mol. Cell Biol. 2003, 4, 915–925. [Google Scholar] [CrossRef]
- Ponzo, M.G.; Lesurf, R.; Petkiewicz, S.; O’Malley, F.P.; Pinnaduwage, D.; Andrulis, I.L.; Bull, S.B.; Chughtai, N.; Zuo, D.; Souleimanova, M.; et al. Met induces mammary tumors with diverse histologies and is associated with poor outcome and human basal breast cancer. Proc. Natl. Acad. Sci. USA 2009, 106, 12903–12908. [Google Scholar] [CrossRef]
- Jamiyan, T.; Kuroda, H.; Yamaguchi, R.; Abe, A.; Hayashi, M. CD68- and CD163-positive tumor-associated macrophages in triple negative cancer of the breast. Virchows Archiv. 2020, 477, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Liu, W.; Hu, B.; Wang, P.; Lv, X.; Chen, S.; Shao, Z. Prognostic Significance of Tumor-Infiltrating Natural Killer Cells in Sol-id Tumors: A Systematic Review and Meta-Analysis. Front. Immunol. 2020, 11, 1242. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Chagollan, M.; Carranza-Torres, I.E.; Carranza-Rosales, P.; Guzmán-Delgado, N.E.; Ramírez-Montoya, H.; Martínez-Silva, M.G.; Mariscal-Ramirez, I.; Barrón-Gallardo, C.A.; Pereira-Suárez, A.L.; Aguilar-Lemarroy, A.; et al. Expression of NK Cell Surface Receptors in Breast Cancer Tissue as Predictors of Resistance to Antineoplastic Treatment. Technol. Cancer Res. Treat. 2018, 17. [Google Scholar] [CrossRef] [PubMed]
- Oshi, M.; Asaoka, M.; Tokumaru, Y.; Yan, L.; Matsuyama, R.; Ishikawa, T.; Endo, I.; Takabe, K. CD8 T Cell Score as a Prognostic Biomarker for Triple Negative Breast Cancer. Int. J. Mol. Sci. 2020, 21, 6968. [Google Scholar] [CrossRef]
- Zhao, C.; Liu, Y.; Liang, Z.; Feng, H.; Xu, S. MACC1 facilitates the escape of nasopharyngeal carcinoma cells from killing by natu-ral killer cells. Biotechnol. Biotechnol. Equip. 2019, 33, 579–588. [Google Scholar] [CrossRef]
- Erreni, M.; Mantovani, A.; Allavena, P. Tumor-associated Macrophages (TAM) and Inflammation in Colorectal Cancer. Cancer Microenviron. 2011, 4, 141–154. [Google Scholar] [CrossRef]
- de Aquino, M.T.; Malhotra, A.; Mishra, M.K.; Shanker, A. Challenges and future perspectives of T cell immunotherapy in cancer. Immunol. Lett. 2015, 166, 117–133. [Google Scholar] [CrossRef] [PubMed]
- Tong, G.; Cheng, B.; Li, J.; Wu, X.; Nong, Q.; He, L.; Li, X.; Li, L.; Wang, S. MACC1 regulates PDL1 expression and tumor immunity through the c-Met/AKT/mTOR pathway in gastric cancer cells. Cancer Med. 2019, 8, 7044–7054. [Google Scholar] [CrossRef] [PubMed]
- Nomi, T.; Sho, M.; Akahori, T.; Hamada, K.; Kubo, A.; Kanehiro, H.; Nakamura, S.; Enomoto, K.; Yagita, H.; Azuma, M.; et al. Clinical Significance and Therapeutic Potential of the Programmed Death-1 Ligand/Programmed Death-1 Pathway in Human Pancreatic Cancer. Clin. Cancer Res. 2007, 13, 2151–2157. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No. = 120 (%) | |
|---|---|
| Age (Years) | |
| Mean ± SD. | 47.3 ± 5 |
| Median (Min.–Max.) | 48 (36–56) |
| Menopausal status | |
| Premenopausal | 52 (43.3%) |
| Postmenopausal | 68 (56.7%) |
| Tumor size (cm) | |
| ≤2 | 38 (31.7%) |
| >2–≤5 | 60 (50%) |
| >5 | 22 (18.3%) |
| Histologic grade | |
| Grade II | 88 (73.3%) |
| Grade III | 32 (26.7%) |
| Nodal involvement | |
| Absent | 16 (13.3%) |
| Present | 104 (86.7%) |
| Lymphovascular invasion | |
| Absent | 103 (85.8%) |
| Present | 17 (14.2%) |
| Tumor stage | |
| I | 35 (29.2%) |
| II | 21 (17.5%) |
| III | 64 (53.3%) |
| ER | |
| Negative | 48 (40%) |
| Positive | 72 (60%) |
| PR | |
| Negative | 56 (46.7%) |
| Positive | 64 (53.3%) |
| HER2 receptor | |
| Negative | 78 (65%) |
| Positive | 42 (35%) |
| Ki-67 | |
| <15 | 50 (41.7%) |
| ≥15 | 70 (58.3%) |
| Molecular subtypes | |
| Luminal A | 36 (30%) |
| Luminal B | 65 (54.2%) |
| HER2 enriched | 8 (6.7%) |
| TNBC | 11 (9.1%) |
| CD163+ TAMs count | |
| Mean ± SD. | 31.6 ± 14.8 |
| Median (Min.–Max.) | 34.5 (0–53) |
| CD56+ NK cells count | |
| Mean ± SD. | 30.8 ± 18.1 |
| Median (Min.–Max.) | 29 (0–60) |
| CD8+ CTLs count | |
| Mean ± SD. | 52.2 ± 23.4 |
| Median (Min.–Max.) | 47.5 (13–95) |
| Survival (3 years) | |
| Dead | 16 (13.3%) |
| Alive | 104 (86.7%) |
| Recurrence | |
| No | 84 (70%) |
| Yes | 36 (30%) |
| MACC1 Expression | ||||
|---|---|---|---|---|
| n = 120 | Median | Range | p-Value | |
| Menopausal status | ||||
| Premenopausal | 52 | 1.8 | 0.5–3.2 | 0.567 |
| Postmenopausal | 68 | 1.8 | 0.4–3.1 | |
| Tumor size (cm) | ||||
| ≤2 | 38 | 1.3 | 0.5–3.0 | <0.001 * |
| >2–≤5 | 60 | 1.8 | 0.4–3.1 | |
| >5 | 22 | 2.5 | 1.3–3.2 | |
| Histologic grade | ||||
| Grade II | 88 | 1.4 | 0.4–3.0 | <0.001 * |
| Grade III | 32 | 2.3 | 1.2–3.2 | |
| Nodal involvement | ||||
| Absent | 16 | 0.7 | 0.5–2.1 | 0.001 * |
| Present | 104 | 2.0 | 0.4–3.2 | |
| Lymphovascular invasion | ||||
| Absent | 103 | 1.5 | 0.4–3.2 | <0.001 * |
| Present | 17 | 2.5 | 1.6–3.2 | |
| Tumor stage | ||||
| I | 35 | 0.9 | 0.5–3.0 | <0.001 * |
| II | 21 | 1.2 | 0.4–2.4 | |
| III | 64 | 2.3 | 0.5–3.2 | |
| ER | ||||
| Negative | 48 | 2.10 | 0.50–3.20 | 0.106 |
| Positive | 72 | 1.50 | 0.40–3.10 | |
| PR | ||||
| Negative | 56 | 1.95 | 0.50–3.20 | 0.091 |
| Positive | 64 | 1.65 | 0.4–3.00 | |
| HER2 receptor | ||||
| Negative | 78 | 1.75 | 0.40–3.00 | 0.061 |
| Positive | 42 | 1.90 | 0.50–3.20 | |
| Ki-67 | ||||
| <15 | 50 | 0.7 | 0.4–3.0 | <0.001 * |
| ≥15 | 70 | 2.3 | 0.5–3.2 | |
| Molecular subtypes | ||||
| Luminal A | 36 | 1.14 | 0.4–3.0 | |
| Luminal B | 65 | 2.06 | 0.5–3.2 | <0.001 * |
| HER2 enriched | 8 | 1.74 | 0.5–3.2 | |
| TNBC | 11 | 1.9 | 0.5–2.9 | |
| Univariate | Multivariate # | |||
|---|---|---|---|---|
| p-Value | HR (95% C.I) | p-Value | HR (95% C.I) | |
| Tumor size (>5 cm) | 0.456 | 1538 (0.496–4769) | ||
| Nodal involvement | 0.300 | 25.402 (0.056–11557.02) | ||
| Lymphovascular invasion | <0.001 * | 7122 (2665–19.031) | 0.042 * | 3138 (1040–9471) |
| Stage (III) | 0.042 * | 64.419 (1154–3597.441) | 0.943 | 54.893.102 (0.0–1004) |
| ER | 0.409 | 0.662 (0.248–1763) | ||
| PR | 0.027 * | 3574 (1.152–11.084) | 0.406 | 0.560 (0.142–1128) |
| HER2 receptor | 0.889 | 1.075 (0.391–2958) | ||
| Ki-67 | 0.178 | 2176 (0.70–6748) | ||
| CD163 | 0.001 * | 1106 (1042–1173) | 0.083 | 1058 (0.993–1128) |
| CD56 | 0.001 * | 0.942 (0.909–0.976) | 0.207 | 0.979 (0.947–1012) |
| CD8 | 0.267 | 0.988 (0.966–1010) | ||
| MACC1 expression | <0.001 * | 12.690 (3510–45.876) | 0.015 * | 5932 (1423–24.738) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, D.A.; El-Guindy, D.M.; Elrashidy, M.A.; Sabry, N.M.; Kabel, A.M.; Gaber, R.A.; Ibrahim, R.R.; Samy, S.M.; Shalaby, M.M.; Salama, S.A.; et al. The Prognostic Significance of MACC1 Expression in Breast Cancer and Its Relationship to Immune Cells in the Tumor Microenvironment and Patient Survival. Medicina 2021, 57, 934. https://doi.org/10.3390/medicina57090934
Ali DA, El-Guindy DM, Elrashidy MA, Sabry NM, Kabel AM, Gaber RA, Ibrahim RR, Samy SM, Shalaby MM, Salama SA, et al. The Prognostic Significance of MACC1 Expression in Breast Cancer and Its Relationship to Immune Cells in the Tumor Microenvironment and Patient Survival. Medicina. 2021; 57(9):934. https://doi.org/10.3390/medicina57090934
Chicago/Turabian StyleAli, Dina A., Dina M. El-Guindy, Mohamed A. Elrashidy, Nesreen M. Sabry, Ahmed M. Kabel, Rasha A. Gaber, Rowida R. Ibrahim, Sara M. Samy, Marwa M. Shalaby, Samir A. Salama, and et al. 2021. "The Prognostic Significance of MACC1 Expression in Breast Cancer and Its Relationship to Immune Cells in the Tumor Microenvironment and Patient Survival" Medicina 57, no. 9: 934. https://doi.org/10.3390/medicina57090934
APA StyleAli, D. A., El-Guindy, D. M., Elrashidy, M. A., Sabry, N. M., Kabel, A. M., Gaber, R. A., Ibrahim, R. R., Samy, S. M., Shalaby, M. M., Salama, S. A., & Abdelhai, D. (2021). The Prognostic Significance of MACC1 Expression in Breast Cancer and Its Relationship to Immune Cells in the Tumor Microenvironment and Patient Survival. Medicina, 57(9), 934. https://doi.org/10.3390/medicina57090934