
Aspirin Is Related to Worse Clinical Outcomes of COVID-19

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
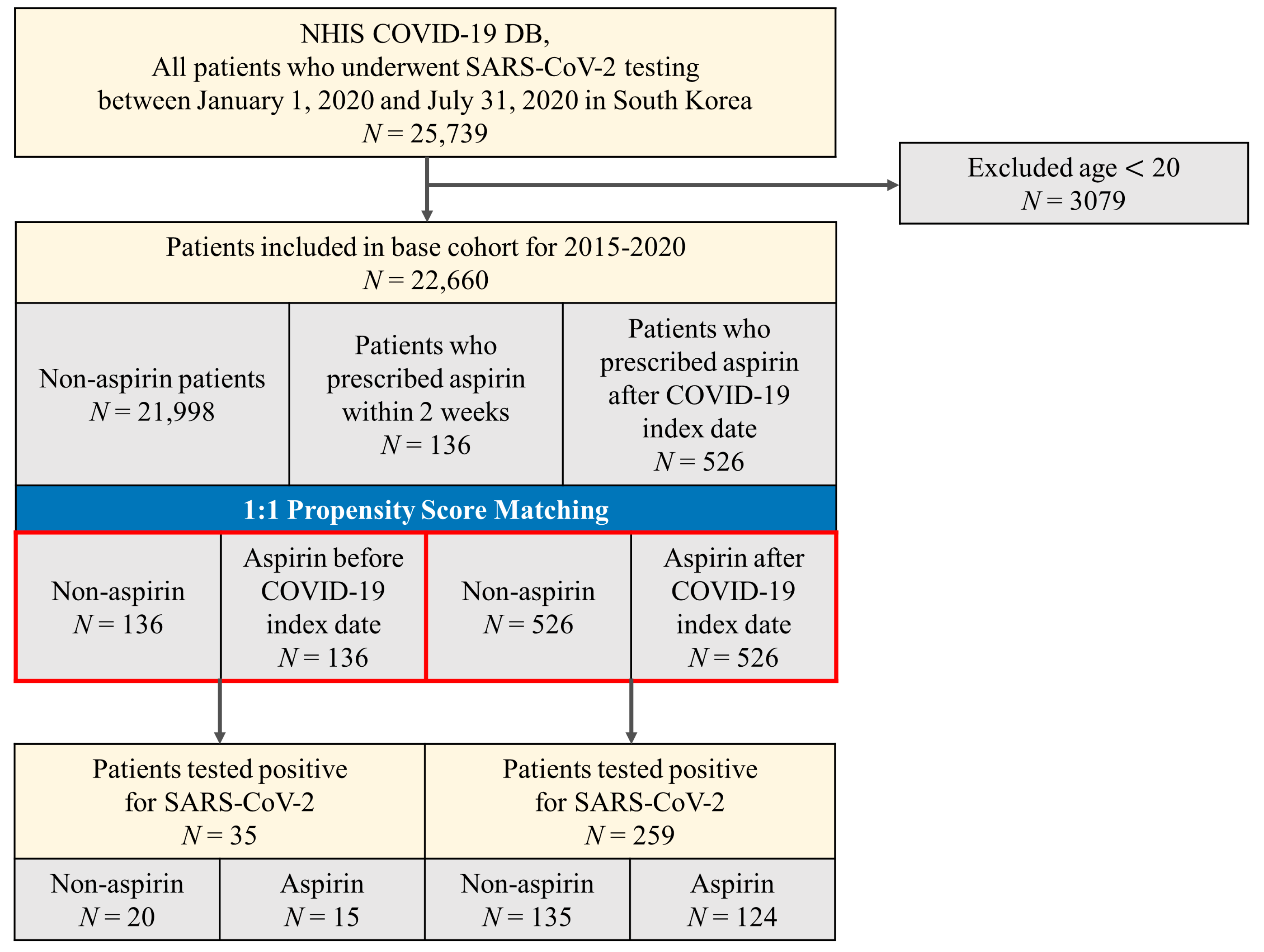
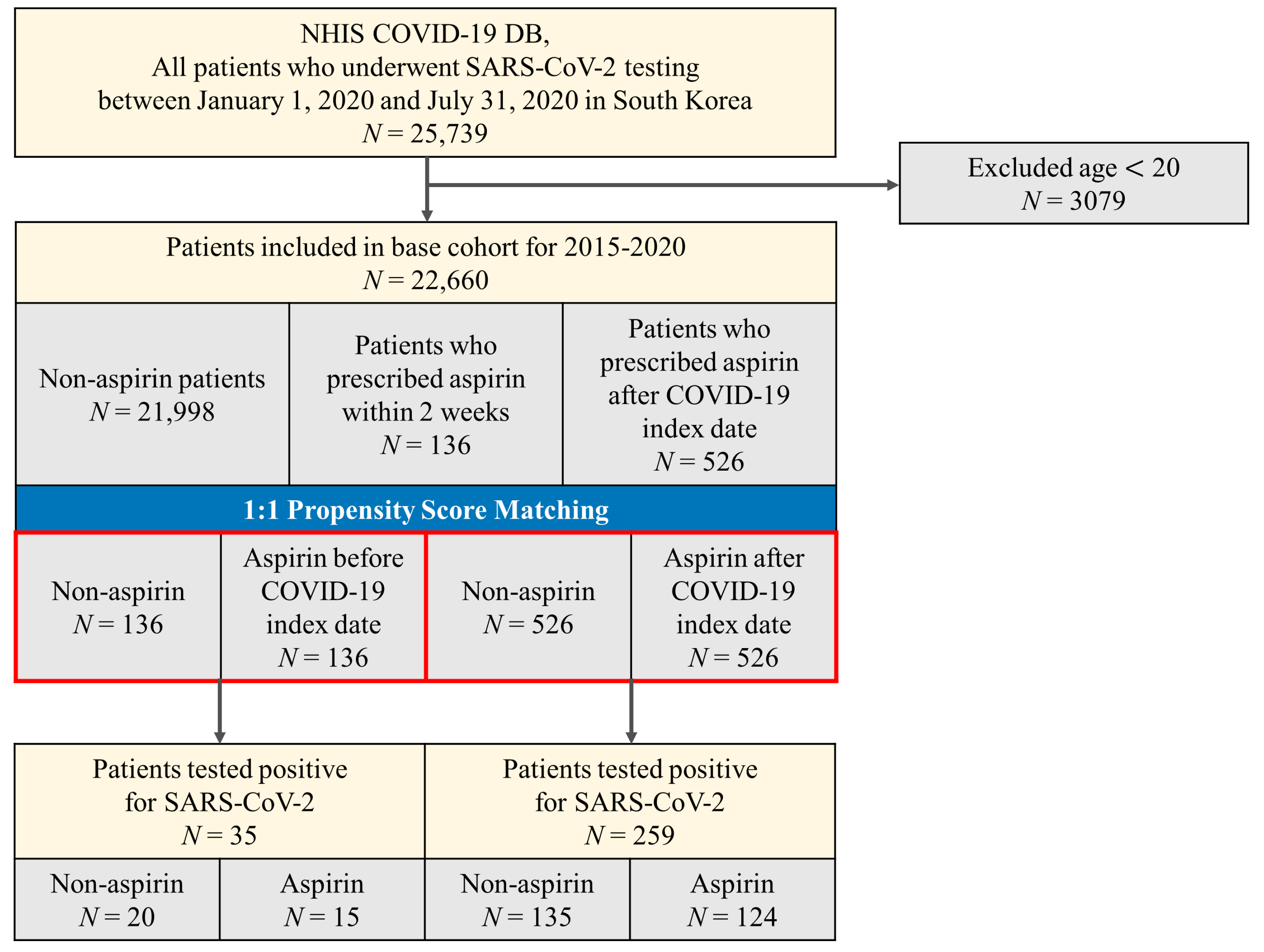
2.2. Study Population
2.3. Exposure
2.4. Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, J.; Shin, D.; Kim, H. Analysis of Major COVID-19 Issues Using Unstructured Big Data. Knowl. Manag. Res. 2021, 22, 145–165. [Google Scholar]
- World Health Organization. Coronavirus Disease (COVID-19); Weekly Epidemiological. 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19 (accessed on 15 June 2021).
- The RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar]
- Warner, T.D.; Nylander, S.; Whatling, C. Anti-platelet therapy: Cyclo-oxygenase inhibition and the use of aspirin with particular regard to dual anti-platelet therapy. Br. J. Clin. Pharmacol. 2011, 72, 619–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Li, H.; Gu, X.; Wang, Z.; Liu, S.; Chen, L. Effect of antiplatelet therapy on acute respiratory distress syndrome and mortality in critically ill patients: A meta-analysis. PLoS ONE 2016, 11, e0154754. [Google Scholar] [CrossRef] [Green Version]
- Du, F.; Jiang, P.; He, S.; Song, D.; Xu, F. Antiplatelet therapy for critically ill patients: A pairwise and Bayesian network meta-analysis. Shock. Inj. Inflamm. Sepsis Lab. Clin. Approach. 2018, 49, 616–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, J.H.; Khanna, A.K.; Kethireddy, S.; Yamane, D.; Levine, A.; Jackson, A.M.; McCurdy, M.T.; Tabatabai, A.; Kumar, G.; Park, P.; et al. Aspirin Use Is Associated With Decreased Mechanical Ventilation, Intensive Care Unit Admission, and In-Hospital Mortality in Hospitalized Patients With Coronavirus Disease 2019. Anesth. Analg. 2021, 132, 930–941. [Google Scholar] [CrossRef]
- Yuan, S.; Chen, P.; Li, H.; Chen, C.; Wang, F.; Wang, D.W. Mortality and pre-hospitalization use of low-dose aspirin in COVID-19 patients with coronary artery disease. J. Cell. Mol. Med. 2021, 25, 1263–1273. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.Y.; Choi, J.C.; You, S.H.; Kim, W.Y. Association of Renin-angiotensin-aldosterone System Inhibitors With Coronavirus Disease 2019 (COVID-19)- Related Outcomes in Korea: A Nationwide Population-based Cohort Study. Clin. Infect. Dis. 2020, 71, 2121–2128. [Google Scholar] [CrossRef]
- Zhang, Z.; Kim, H.J.; Lonjon, G.; Zhu, Y. Balance diagnostics after propensity score matching. Ann. Transl. Med. 2019, 7, 16. [Google Scholar] [CrossRef]
- Paranjpe, I.; Fuster, V.; Lala, A.; Russak, A.J.; Glicksberg, B.S.; Levin, M.A.; Charney, A.W.; Narula, J.; Fayad, Z.A.; Bagiella, E.; et al. Association of treatment dose anticoagulation with in-hospital survival among hospitalized patients with COVID-19. J. Am. Coll. Cardiol. 2020, 76, 122–124. [Google Scholar] [CrossRef]
- Ikonomidis, I.; Andreotti, F.; Economou, E.; Stefanadis, C.; Toutouzas, P.; Nihoyannopoulos, P. Increased proinflammatory cytokines in patients with chronic stable angina and their reduction by aspirin. Circulation 1999, 100, 793–798. [Google Scholar] [CrossRef] [Green Version]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Klok, F.A.; Kruip, M.J.H.A.; van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.; Kant, K.M.; Kaptein, F.H.J.; van Paassen, J.; Stals, M.A.M.; Huisman, M.V.; et al. Confirmation of the high cumulative incidence of thrombotic complications in critically ill ICU patients with COVID-19: An updated analysis. Thromb. Res. 2020, 191, 148–150. [Google Scholar] [CrossRef]
- Rapkiewicz, A.V.; Mai, X.; Carsons, S.E.; Pittaluga, S.; Kleiner, D.E.; Berger, J.S.; Thomas, S.; Adler, N.M.; Charytan, D.M.; Gasmi, B.; et al. Megakaryocytes and platelet-fibrin thrombi characterize multi-organ thrombosis at autopsy in COVID-19: A case series. EClinicalMedicine 2020, 24, 100434. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Panka, B.A.; de Grooth, H.J.; Spoelstra-de Man, A.M.; Looney, M.R.; Tuinman, P.R. Prevention or Treatment of Ards With Aspirin: A Review of Preclinical Models and Meta-Analysis of Clinical Studies. Shock 2017, 47, 13–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, B.; Moss, C.; Rigg, A.; Van Hemelrijck, M. COVID-19 and treatment with NSAIDs and corticosteroids: Should we be limiting their use in the clinical setting? Ecancermedicalscience 2020, 14, 1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asghar, W.; Aghazadeh-Habashi, A.; Jamali, F. Cardiovascular effect of inflammation and nonsteroidal anti-inflammatory drugs on renin–angiotensin system in experimental arthritis. Inflammopharmacology 2017, 25, 543–553. [Google Scholar] [CrossRef]
- Alamdari, N.M.; Afaghi, S.; Rahimi, F.S.; Tarki, F.E.; Tavana, S.; Zali, A.; Fathi, M.; Besharat, S.; Bagheri, L.; Pourmotahari, F.; et al. Mortality risk factors among hospitalized COVID-19 patients in a major referral center in Iran. Tohoku J. Exp. Med. 2020, 252, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Salah, H.M.; Mehta, J.L. Meta-Analysis of the Effect of Aspirin on Mortality in COVID-19. Am. J. Cardiol. 2021, 142, 158–159. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [Green Version]
- de Moraes, V.L.G.; Vargaftig, B.B.; Lefort, J.; Meager, A.; Chignard, M. Effect of cyclo-oxygenase inhibitors and modulators of cyclic AMP formation on lipopolysaccharide-induced neutrophil infiltration in mouse lung. Br. J. Pharmacol. 1996, 117, 1792–1796. [Google Scholar] [CrossRef] [Green Version]
- Kor, D.; Carter, R.; Park, P.; Festic, E.; Banner-Goodspeed, V.; Hinds, R.; Talmor, D.; Gajic, O.; Ware, L.; Gong, M. Effect of aspirin on development of ARDS in at-risk patients presenting to the emergency department: The LIPS-A randomized clinical trial. JAMA 2016, 315, 2406–2414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osborne, T.F.; Veigulis, Z.P.; Arreola, D.M.; Mahajan, S.M.; Roosli, E.; Curtin, C.M. Association of mortality and aspirin prescription for COVID-19 patients at the Veterans Health Administration. PLoS ONE 2021, 16, e0246825. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-j.; Ni, Z.-y.; Hu, Y.; Liang, W.-h.; Ou, C.-q.; He, J.-x.; Liu, L.; Shan, H.; Lei, C.-l.; David, S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Hsia, J.; Sarin, N.; Oliver, J.H.; Goldstein, A.L. Aspirin and thymosin increase interleukin-2 and interferon-γ production by human peripheral blood lymphocytes. Immunopharmacology 1989, 17, 167–173. [Google Scholar] [CrossRef]
- Abers, M.S.; Delmonte, O.M.; Ricotta, E.E.; Fintzi, J.; Fink, D.L.; de Jesus, A.A.A.; Zarember, K.A.; Alehashemi, S.; Oikonomou, V.; Desai, J.V.; et al. An immune-based biomarker signature is associated with mortality in COVID-19 patients. JCI Insight 2021, 6, e144455. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristic | Entire Cohort N = 22,660 | Non-Aspirin N = 21,998 | Aspirin Before COVID-19 Index Date N = 136 | Aspirin After COVID-19 Index Date N = 526 |
|---|---|---|---|---|
| Sex, n (%) | ||||
| Male | 9992 (44.1) | 9601 (43.6) | 86 (63.2) | 305 (58.0) |
| Female | 12,668 (55.9) | 12,397 (56.4) | 50 (36.8) | 221 (42.0) |
| Age, n (%) | ||||
| 20–29 | 4841 (21.4) | 4835 (22.0) | 0 (0.0) | 6 (1.1) |
| 30–39 | 3764 (16.6) | 3758 (17.1) | 1 (0.7) | 5 (1.0) |
| 40–49 | 3399 (15.0) | 3374 (15.3) | 7 (5.1) | 18 (3.4) |
| 50–59 | 3662 (16.2) | 3598 (16.4) | 17 (12.5) | 47 (8.9) |
| 60–69 | 3068 (13.5) | 2914 (13.2) | 36 (26.5) | 118 (22.4) |
| 70–79 | 2156 (9.5) | 1945 (8.8) | 47 (34.6) | 164 (31.2) |
| 80+ | 1770 (7.8) | 1574 (7.2) | 28 (20.6) | 168 (31.9) |
| Region, n (%) | ||||
| Seoul | 3902 (17.2) | 3794 (17.2) | 22 (16.2) | 86 (16.3) |
| Gyeonggi | 2726 (12.0) | 2637 (12.0) | 17 (12.5) | 72 (13.7) |
| Daegu | 8592 (37.9) | 8401 (38.2) | 36 (26.5) | 155 (29.5) |
| Gyeongbuk | 1831 (8.1) | 1759 (8.0) | 14 (10.3) | 58 (11.0) |
| Others | 5609 (24.8) | 5407 (24.6) | 47 (34.6) | 155 (29.5) |
| HTN, n (%) | 5675 (25.0) | 5170 (23.5) | 108 (79.4) | 397 (75.5) |
| COPD, n (%) | 767 (3.4) | 703 (3.2) | 13 (9.6) | 51 (9.7) |
| Asthma, n (%) | 2433 (10.7) | 2314 (10.5) | 23 (16.9) | 96 (18.3) |
| CKD, n (%) | 1071 (4.7) | 895 (4.1) | 62 (45.6) | 114 (21.7) |
| DM, n (%) | 3713 (16.4) | 3354 (15.2) | 92 (67.6) | 267 (50.8) |
| CVD, n (%) | 1888 (8.3) | 1631 (7.4) | 66 (48.5) | 191 (36.3) |
| Charlson Comorbidity Index, n (%) | ||||
| 0 | 11,775 (52.0) | 11,719 (53.3) | 12 (8.8) | 44 (8.4) |
| 1 | 3029 (13.4) | 2861 (13.0) | 35 (25.7) | 133 (25.3) |
| 2 or more | 7856 (34.7) | 7418 (33.7) | 89 (65.4) | 349 (66.3) |
| Current use of medication, n (%) | ||||
| Steroid | 1921 (8.5) | 1826 (8.3) | 36 (26.5) | 59 (11.2) |
| Characteristic | Non-Aspirin N = 136 | Aspirin before COVID-19 Index Date N = 136 | SMD | Non-Aspirin N = 526 | Aspirin after COVID-19 Index Date N = 526 | SMD |
|---|---|---|---|---|---|---|
| Sex, n (%) | 0.030 | 0.023 | ||||
| Male | 84 (61.8) | 86 (63.2) | 299 (56.8) | 305 (58.0) | ||
| Female | 52 (38.2) | 50 (36.8) | 227 (43.2) | 221 (42.0) | ||
| Age, n (%) | 0.128 | 0.052 | ||||
| 20–29 | 0 (0.0) | 0 (0.0) | 3 (0.6) | 6 (1.1) | ||
| 30–39 | 1 (0.7) | 1 (0.7) | 7 (1.3) | 5 (1.0) | ||
| 40–49 | 6 (4.4) | 7 (5.1) | 17 (3.2) | 18 (3.4) | ||
| 50–59 | 14 (10.3) | 17 (12.5) | 41 (7.8) | 47 (8.9) | ||
| 60–69 | 30 (22.1) | 36 (26.5) | 118 (22.4) | 118 (22.4) | ||
| 70–79 | 52 (38.2) | 47 (34.6) | 160 (30.4) | 164 (31.2) | ||
| 80+ | 33 (24.3) | 28 (20.6) | 180 (34.2) | 168 (31.9) | ||
| Region, n (%) | 0.027 | 0.006 | ||||
| Seoul | 17 (12.5) | 22 (16.2) | 93 (17.7) | 86 (16.3) | ||
| Gyeonggi | 41 (30.1) | 36 (26.5) | 158 (30.0) | 155 (29.5) | ||
| Daegu | 17 (12.5) | 17 (12.5) | 63 (12.0) | 72 (13.7) | ||
| Gyeongbuk | 13 (9.6) | 14 (10.3) | 54 (10.3) | 58 (11.0) | ||
| Others | 48 (35.3) | 47 (34.6) | 158 (30.0) | 155 (29.5) | ||
| HTN, n (%) | 112 (82.4) | 108 (79.4) | 0.072 | 401 (76.2) | 397 (75.5) | 0.018 |
| COPD, n (%) | 11 (8.1) | 13 (9.6) | 0.050 | 38 (7.2) | 51 (9.7) | 0.083 |
| Asthma, n (%) | 26 (19.1) | 23 (16.9) | 0.059 | 85 (16.2) | 96 (18.3) | 0.054 |
| CKD, n (%) | 54 (39.7) | 62 (45.6) | 0.118 | 93 (17.7) | 114 (21.7) | 0.097 |
| DM, n (%) | 98 (72.1) | 92 (67.6) | 0.094 | 262 (49.8) | 267 (50.8) | 0.019 |
| CVD, n (%) | 67 (49.3) | 66 (48.5) | 0.015 | 184 (35.0) | 191 (36.3) | 0.028 |
| Charlson Comorbidity Index, n (%) | 0.113 | 0.003 | ||||
| 0 | 11 (8.1) | 12 (8.8) | 42 (8.0) | 44 (8.4) | ||
| 1 | 27 (19.9) | 35 (25.7) | 136 (35.9) | 133 (25.3) | ||
| 2 or more | 98 (72.1) | 89 (65.4) | 348 (66.2) | 349 (66.3) | ||
| Current use of medication, n (%) | ||||||
| Steroid | 35 (25.7) | 36 (26.5) | 0.017 | 54 (10.3) | 59 (11.2) | 0.030 |
| COVID-19, n (%) | ||||||
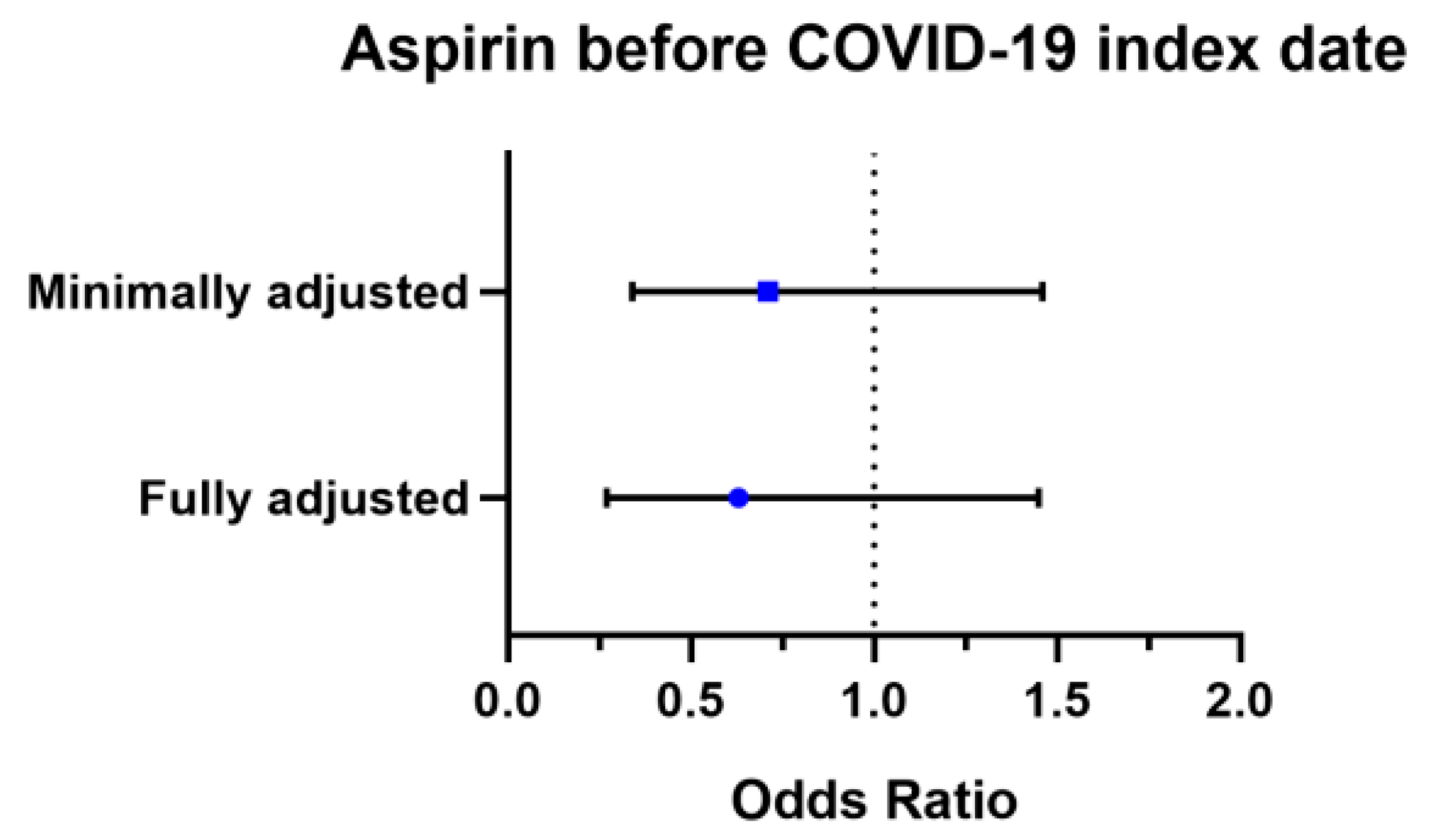
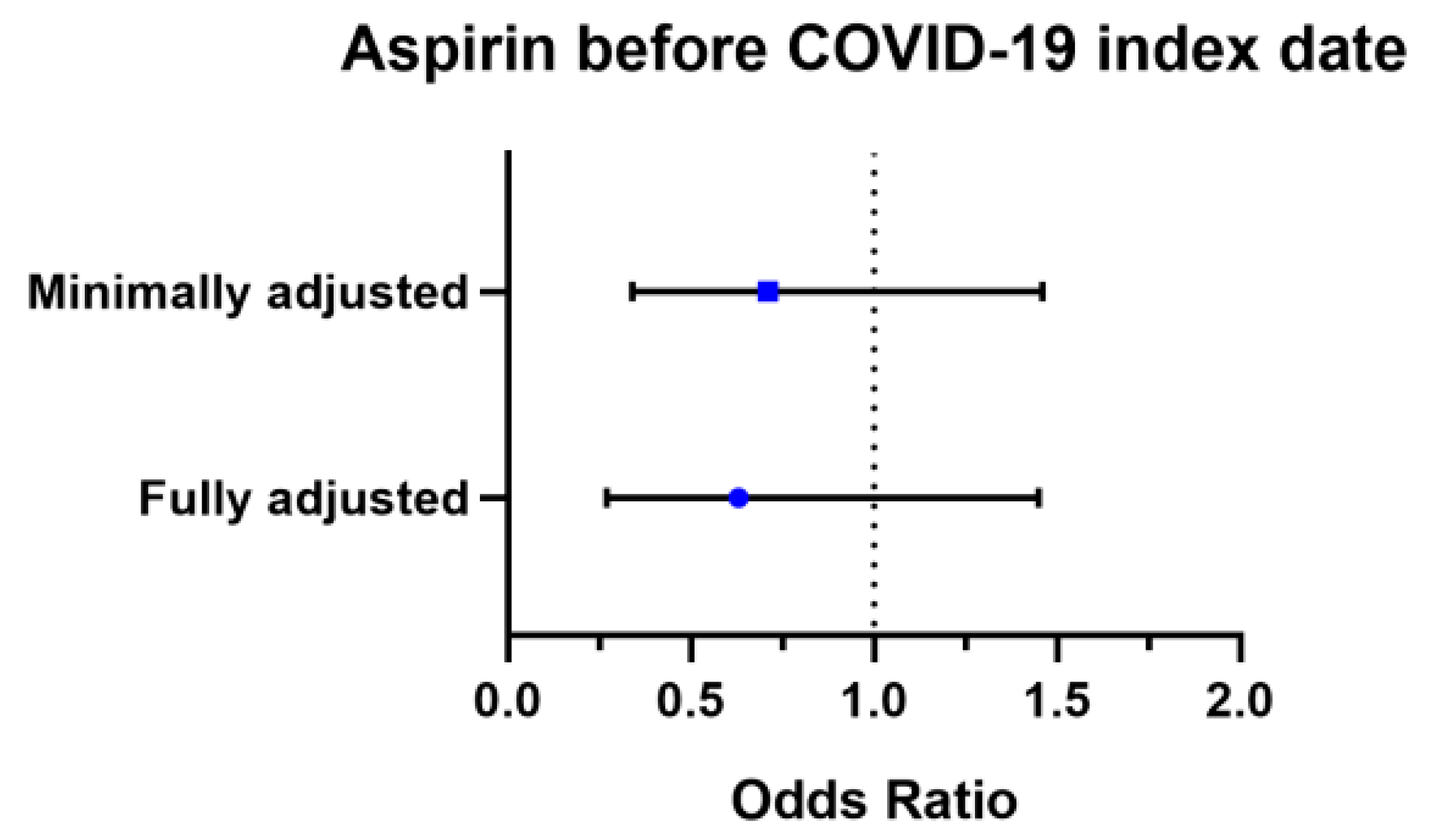
| Minimally adjusted OR * | 1.00 (reference) | 0.71 (0.34–1.46) | 1.00 (reference) | 0.89 (0.67–1.18) | ||
| Fully adjusted OR † | 1.00 (reference) | 0.63 (0.27–1.45) | 1.00 (reference) | 0.89 (0.64–1.24) | ||
| Variables | Non-Aspirin N = 136 | Aspirin before COVID-19 Index Date N = 136 | p-Value * |
|---|---|---|---|
| COVID-19, n (%) | 0.469 | ||
| No | 116 (85.3) | 121 (89.0) | |
| Yes | 20 (14.7) | 15 (11.0) |
| Variables | Non-Aspirin N = 20 | Aspirin before COVID-19 Index Date N = 15 | p-Value |
|---|---|---|---|
| Composite endpoint 1, n (%) | 0.043 * | ||
| No | 12 (60.0) | 3 (20.0) | |
| Yes | 8 (40.0) | 12 (80.0) | |
| Composite endpoint 2, n (%) | 0.016 * | ||
| No | 17 (85.0) | 6 (40.0) | |
| Yes | 3 (15.0) | 9 (60.0) | |
| Conventional oxygen therapy | 0.727 * | ||
| No | 13 (65.0) | 8 (53.3) | |
| Yes | 7 (35.0) | 7 (46.7) | |
| Intensive care unit | 0.141 † | ||
| No | 19 (95.0) | 11 (73.3) | |
| Yes | 1 (5.0) | 4 (26.7) | |
| Mechanical ventilation | 0.141 † | ||
| No | 19 (95.0) | 11 (73.3) | |
| Yes | 1 (5.0) | 4 (26.7) | |
| Death | 0.027 † | ||
| No | 19 (95.0) | 9 (60.0) | |
| Yes | 1 (5.0) | 6 (40.0) |
| Variables | Non-Aspirin N = 135 | Aspirin after COVID-19 Index Date N = 124 | p-Value * |
|---|---|---|---|
| Composite endpoint 1, n (%) | 0.038 | ||
| No | 92 (68.1) | 68 (54.8) | |
| Yes | 43 (31.9) | 56 (45.2) | |
| Composite endpoint 2, n (%) | 0.549 | ||
| No | 106 (78.5) | 102 (82.3) | |
| Yes | 29 (21.5) | 22 (17.7) | |
| Conventional oxygen therapy | 0.000 | ||
| No | 108 (80.0) | 73 (58.9) | |
| Yes | 7 (35.0) | 7 (46.7) | |
| Intensive care unit | 0.447 | ||
| No | 131 (97.0) | 117 (94.4) | |
| Yes | 4 (3.0) | 7 (5.6) | |
| Mechanical ventilation | 0.173 | ||
| No | 128 (94.8) | 111 (89.5) | |
| Yes | 7 (5.2) | 13 (10.5) | |
| Death | 0.253 | ||
| No | 112 (83.0) | 110 (88.7) | |
| Yes | 23 (17.0) | 14 (11.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, I.; Yoon, S.; Kim, M.; Lee, H.; Park, S.; Kim, W.; Lee, S. Aspirin Is Related to Worse Clinical Outcomes of COVID-19. Medicina 2021, 57, 931. https://doi.org/10.3390/medicina57090931
Kim I, Yoon S, Kim M, Lee H, Park S, Kim W, Lee S. Aspirin Is Related to Worse Clinical Outcomes of COVID-19. Medicina. 2021; 57(9):931. https://doi.org/10.3390/medicina57090931
Chicago/Turabian StyleKim, Isaac, Siyeong Yoon, Minsup Kim, Hyunil Lee, Sinhyung Park, Wonsang Kim, and Soonchul Lee. 2021. "Aspirin Is Related to Worse Clinical Outcomes of COVID-19" Medicina 57, no. 9: 931. https://doi.org/10.3390/medicina57090931
APA StyleKim, I., Yoon, S., Kim, M., Lee, H., Park, S., Kim, W., & Lee, S. (2021). Aspirin Is Related to Worse Clinical Outcomes of COVID-19. Medicina, 57(9), 931. https://doi.org/10.3390/medicina57090931