
Cor Triatriatum Sinistrum Combined with Changes in Atrial Septum and Right Atrium in a 60-Year-Old Woman


 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Macroscopical Analysis
3.2. Measurements of Atrial and Ventricular Wall Thickness
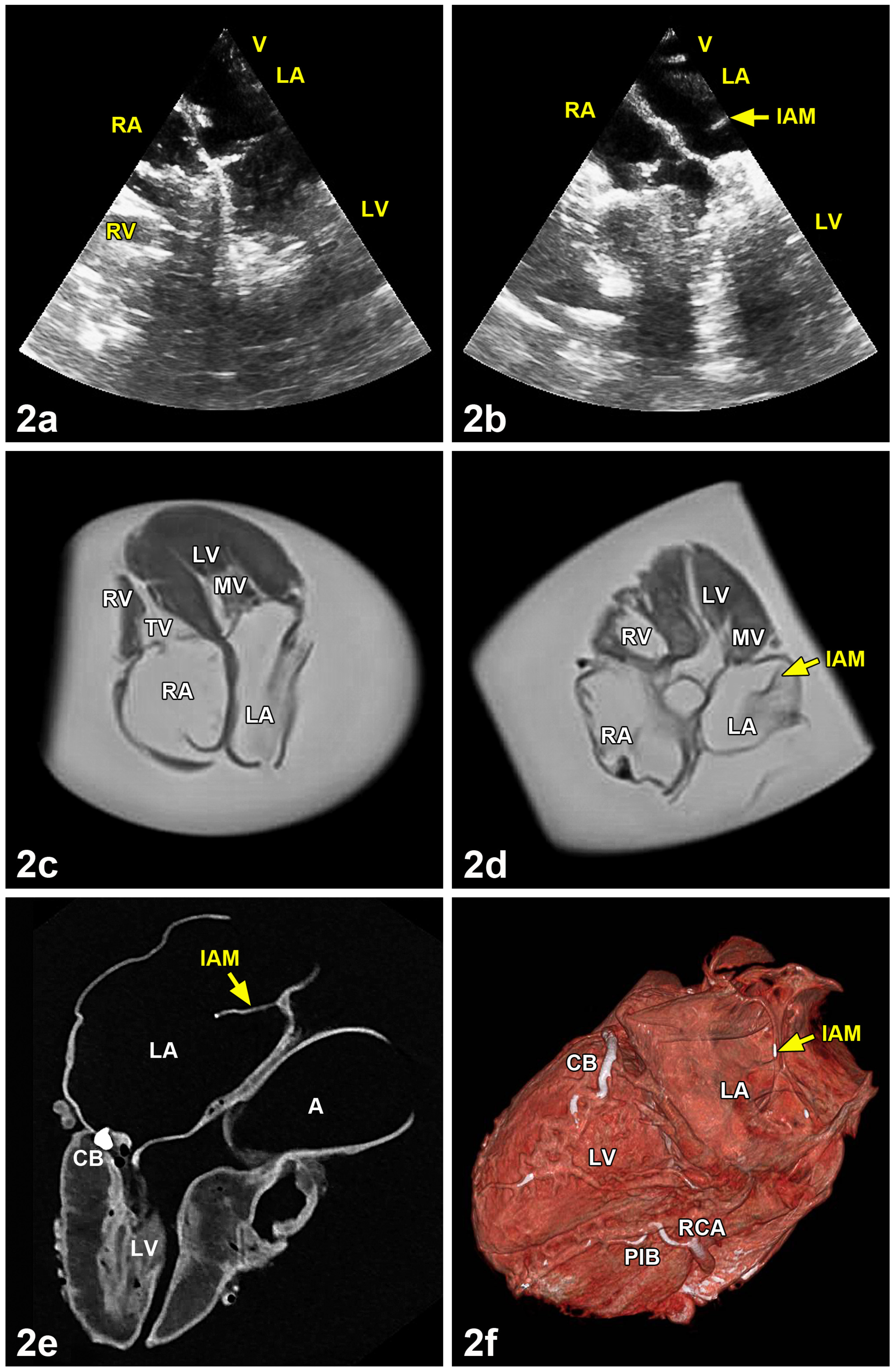
3.3. Analysis by Ultrasound, Magnetic Resonance Imaging, Computed Tomography and Cinematic Rendering
3.4. Comparison with Left and Right Atria of Regularly Formed Hearts
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zepeda, I.A.; Morcos, P.; Castellanos, L.R. Cor triatriatum sinister identified after new onset atrial fibrillation in an elderly man. Case. Rep. Med. 2014, 2014, 1–5. [Google Scholar] [CrossRef]
- Nassar, P.N.; Hamdan, R.H. Cor triatriatum sinistrum: Classification and imaging modalities. Eur. J. Cardiovasc. Med. 2011, 1, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Pfennig, E. Anomale Septumbildung im linken Vorhof des menschlichen Herzens. Virchows Arch. 1941, 307, 579–595. [Google Scholar] [CrossRef]
- Sadler, T.W. Medizinische Embryologie; Thieme: Stuttgart, Germany; New York, NY, USA, 2008; pp. 218–263. [Google Scholar]
- Moore, K.L.; Persaud, T.V.N.; Torchia, M.G. Embryologie; Elsevier—Urban & Fischer: München, Germany, 2013; pp. 361–414. [Google Scholar]
- Anderson, R.H.; Becker, A.E. Anatomie des Herzens; Thieme: Stuttgart, Germany; New York, NY, USA, 1982. [Google Scholar]
- Ertl, G. Krankheiten des Herzens und des Kreislaufs. In Innere Medizin; Classen, M., Diehl, V., Kochsiek, K., Eds.; Urban & Schwarzenberg: München, Germany; Wien, Austria; Baltimore, MD, USA, 1998; pp. 1099–1230. [Google Scholar]
- Slight, R.D.; Nzewi, O.C.; Buell, R.; Mankad, P.S. Cor-triatriatum sinister presenting in the adult mitral stenosis: An analysis of factors which may be relevant in late presentation. Heart Lung Circ. 2004, 14, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Capdeville, M.; Brozzi, N.; Petterson, G.; Gillinov, A.M.; Niezgoda, J. Case 3—2014: Cor triatriatum sinister presenting in adulthood. J. Cardiothorac. Vasc. Anesth. 2014, 28, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Comaniciu, D.; Engel, K.; Georgescu, B.; Mansi, T. Shaping the future through innovations: From medical imaging to precision medicine. Med. Image Anal. 2016, 33, 19–26. [Google Scholar] [CrossRef]
- Glemser, P.A.; Engel, K.; Simons, D.; Steffens, J.; Schlemmer, H.P.; Orakcioglu, B. A new approach for photorealistic visualization of rendered computed tomography images. World Neurosurg. 2018, 114, e283–e292. [Google Scholar] [CrossRef]
- Binder, J.; Krautz, C.; Engel, K.; Grützmann, R.; Fellner, F.A.; Burger, P.H.M.; Scholz, M. Leveraging medical imaging for medical education—A cinematic rendering-featured lecture. Ann. Anat. 2019, 222, 159–165. [Google Scholar] [CrossRef]
- Kir, M.; Ugurlu, B.; Saylam, G.S.; Karadas, U. Surgical treatment of cor triatriatum, ventricular septal defect in an infant with a giant omphalocele. J. Pediatr. Surg. 2011, 46, E23–E25. [Google Scholar] [CrossRef]
- Jorgensen, C.R.; Ferlic, R.M.; Varco, R.L.; Lillehei, C.W.; Eliot, R.S. Cor triatriatum. Review of the surgical aspects with a follow-up report on the first patient successfully treated with surgery. Circulation 1967, 36, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Guhathakurta, S.; Vadalapali, G.; Nalladaru, Z.; Easthope, R.N.; Sharma, A.K. Cor triatriatum in adults. Texas Heart Inst. J. 1999, 26, 206–210. [Google Scholar]
- Modi, K.A.; Senthilkumar, A.; Kiel, E.; Reddy, P.C. Diagnosis and surgical correction of cor triatriatum in an adult: Combined use of transesophageal and contrast echocardiography, and a review of literature. Echocardiography 2006, 23, 506–509. [Google Scholar] [CrossRef] [PubMed]
- Lima, R.P.; Fonseca, C.; Sampaio, F.; Ribeiro, J.; Ribeiro, V.G. Cor triatriatum sinistrum—Descricao e revisao de quatro casos clinicos. Rev. Port. Cardiol. 2010, 29, 827–836. [Google Scholar]
- Eichholz, J.L.; Hodroge, S.S.; Crook, J.J., II; Mack, J.W.; Wortham, D.C. Cor triatriatum sinister in a 43-year-old man with syncope. Texas Heart Inst. J. 2013, 40, 602–605. [Google Scholar]
- Goel, A.K.; Saxena, A.; Kothari, S.S. Atrioventricular septal defect with cor triatriatum: Case Report and review of the literature. Pediatr. Cardiol. 1998, 19, 243–245. [Google Scholar] [CrossRef]
- Strickland, P.T.; Pernetz, M.A.; Jokhadar, M.; Hartlage, G.; Clements, S. Cor triatriatum sinister: A patient, a review, and some unique findings. Echodardiography 2014, 31, 790–794. [Google Scholar] [CrossRef]
- Bojanic, K.; Bursac, D.; Zmijanac, J.; Duic, Z.; Scavonetto, F.; Weingarten, T.N.; Sprung, J. Isolated cor triatriatum sinistrum and pregnancy: Case report and review of the literature. Can. J. Anesth. 2013, 60, 577–583. [Google Scholar] [CrossRef][Green Version]
- Östman-Smith, I.; Silverman, N.H.; Oldershaw, P.; Lincoln, C.; Shinebourne, E.A. Cor triatriatum sinistrum. Diagnostic features on cross sectional echocardiography. Br. Heart J. 1984, 51, 211–219. [Google Scholar] [CrossRef]
- Baweja, G.; Nanda, N.C.; Kirklin, J.K. Definitive diagnosis of cor triatriatum with common atrium by three-dimensional transesophageal echocardiography in and adult. Echocardiography 2004, 21, 303–306. [Google Scholar] [CrossRef]
- Park, K.J.; Park, I.K.; Sir, J.J.; Kim, H.T.; Park, Y.I.; Tsung, P.C.; Chung, J.M.; Park, K.I.; Cho, W.H.; Choi, S.K. Adult cor triatriatum presenting as cardioembolic stroke. Intern Med. 2009, 48, 1149–1152. [Google Scholar] [CrossRef]
- Bassareo, P.P.; Tumbarello, R.; Mercuro, G. Cor triatriatum and lipomatous hypertrophy of the interatrial septum in the elderly: A case report. Cardiovasc. Ultrasound 2010, 8, 1–5. [Google Scholar] [CrossRef]
- Li, W.W.; Koolbergen, D.R.; Bouma, B.J.; Hazekamp, M.G.; de Mol, B.A.; de Winter, R.J. Cathether-based interventional strategies for cor triatriatum in the adult—Feasibility study through a hybrid approach. BMC Cardiovasc. Disord. 2015, 15, 1–6. [Google Scholar] [CrossRef]
- Balli, O.; Aytemir, K.; Karcaaltincaba, M. Multidetector CT of left atrium. Eur. J. Radiol. 2012, 81, e37–e46. [Google Scholar] [CrossRef] [PubMed]
- Sehra, R.; Ensing, G.; Hurwitz, R. Persistent Eustachian valves in infants: Course and management in symptomatic patients. Pediatr. Cardiol. 1998, 19, 221–224. [Google Scholar] [CrossRef]
- Wyss, E.; Ammann, P.; Rickli, H.; Jenni, R. Cor triatriatum dexter bei einem erwachsenen Patienten. Z. Kardiol. 1998, 87, 891–893. [Google Scholar] [CrossRef]
- Malik, S.B.; Kwan, D.; Shah, A.B.; Hsu, J.Y. The right atrium: Gateway to the heart—Anatomic and pathologic imaging findings. RadioGraphics 2015, 35, 14–31. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, A.; Angulo, P.; Martinez, P.; Romero, C.; Pastor, E.; Galdeano, J.M. Cor triatrial con comunicacion interventricular: Diagnostico por eco-Doppler color y resonancia magnetica. Correccion en los primeros meses. Rev. Esp. Cardiol. 1997, 50, 290–292. [Google Scholar] [CrossRef]
- Jha, A.K.; Makhija, N. Cor triatriatum: A review. Semin. Cardiothorac. Vasc. Anesth. 2017, 21, 178–185. [Google Scholar] [CrossRef]
- Alphonso, N.; Norgaard, M.A.; Newcomb, A.; d’Udekem, Y.; Brizard, C.P.; Cochrane, A. Cor triatriatum: Presentation, diagnosis and long-term surgical results. Ann. Thorac. Surg. 2005, 80, 1666–1671. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Gender | Age | Right Atrium | Left Atrium | Right Ventricle | Left Ventricle |
|---|---|---|---|---|---|
| M | 77 | 2 | 2 | 6 | 15 |
| M | 85 | 4 | 3 | 5 | 14 |
| M | 84 | 3 | 1 | 9 | 11 |
| M | 78 | 1 | 1 | 7 | 15 |
| M | 90 | 1 | 1 | 6 | 15 |
| M | 80 | 4 | 2 | 5 | 14 |
| M | 78 | 2 | 2 | 4 | 18 |
| Mean = 2.43 | Mean = 1.71 | Mean = 6.00 | Mean = 14,57 | ||
| SEM = 0.48 | SEM = 0.29 | SEM = 0.62 | SEM = 0.78 | ||
| F | 87 | 2 | 2 | 7 | 11 |
| F | 87 | 1 | 2 | 5 | 15 |
| F | 83 | 2 | 1 | 4 | 10 |
| F | 89 | 2 | 2 | 4 | 14 |
| F | 81 | 2 | 1 | 6 | 12 |
| F | 92 | 1 | 1 | 7 | 16 |
| F | 91 | 2 | 1 | 6 | 15 |
| F | 92 | 2 | 1 | 4 | 10 |
| Mean = 1.75 | Mean = 1.38 | Mean = 5.37 | Mean = 12.88 | ||
| SEM = 0.16 | SEM = 0.18 | SEM = 0.46 | SEM = 0.85 | ||
| F | 60 | 1 | 2 | 3 | 17 |
| C.t.s. |
| Heart Compartment | Hearts | Variation | n | % |
|---|---|---|---|---|
| Left atrium | 59 | Atrial septum smooth | 26 | 44.0 |
| Atrial septum with sickle-like fold, directed dorsally | 20 | 33.9 | ||
| Atrial septum with sickle-like fold, directed cranially | 1 | 1.7 | ||
| Atrial septum with sickle-like fold, directed caudally | 1 | 1.7 | ||
| Atrial septum with various sieve-like depressions | 4 | 6.8 | ||
| Oval fossa bulged in direction of left atrium | 7 | 11.9 | ||
| Right atrium | 58 | Oval fossa barely expressed | 7 | 12.0 |
| Oval fossa flat | 28 | 48.3 | ||
| Oval fossa deepened | 23 | 39.7 | ||
| Right atrium | 59 | Eustacian valve not expressed | 15 | 25.4 |
| Eustacian valve normally expressed | 29 | 49.2 | ||
| Eustacian valve strongly expressed | 15 | 25.4 | ||
| Right atrium | 58 | Thebesian valve not expressed | 16 | 27.6 |
| Thebesian valve normally expressed | 32 | 55.2 | ||
| Thebesian valve strongly expressed | 10 | 17.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Claassen, H.; Busch, C.; May, M.S.; Schicht, M.; Scholz, M.; Schulze, M.; Paulsen, F.; Wree, A. Cor Triatriatum Sinistrum Combined with Changes in Atrial Septum and Right Atrium in a 60-Year-Old Woman. Medicina 2021, 57, 777. https://doi.org/10.3390/medicina57080777
Claassen H, Busch C, May MS, Schicht M, Scholz M, Schulze M, Paulsen F, Wree A. Cor Triatriatum Sinistrum Combined with Changes in Atrial Septum and Right Atrium in a 60-Year-Old Woman. Medicina. 2021; 57(8):777. https://doi.org/10.3390/medicina57080777
Chicago/Turabian StyleClaassen, Horst, Christian Busch, Matthias Stefan May, Martin Schicht, Michael Scholz, Marko Schulze, Friedrich Paulsen, and Andreas Wree. 2021. "Cor Triatriatum Sinistrum Combined with Changes in Atrial Septum and Right Atrium in a 60-Year-Old Woman" Medicina 57, no. 8: 777. https://doi.org/10.3390/medicina57080777
APA StyleClaassen, H., Busch, C., May, M. S., Schicht, M., Scholz, M., Schulze, M., Paulsen, F., & Wree, A. (2021). Cor Triatriatum Sinistrum Combined with Changes in Atrial Septum and Right Atrium in a 60-Year-Old Woman. Medicina, 57(8), 777. https://doi.org/10.3390/medicina57080777