
Post-Diverticulitis Colonoscopy Was Not Associated with Higher Colonic Adenoma and Carcinoma: A Multicenter Case–Control Study




Abstract
:1. Introduction
2. Materials and Methods
3. Study Endpoints
4. Statistical Analysis
5. Results
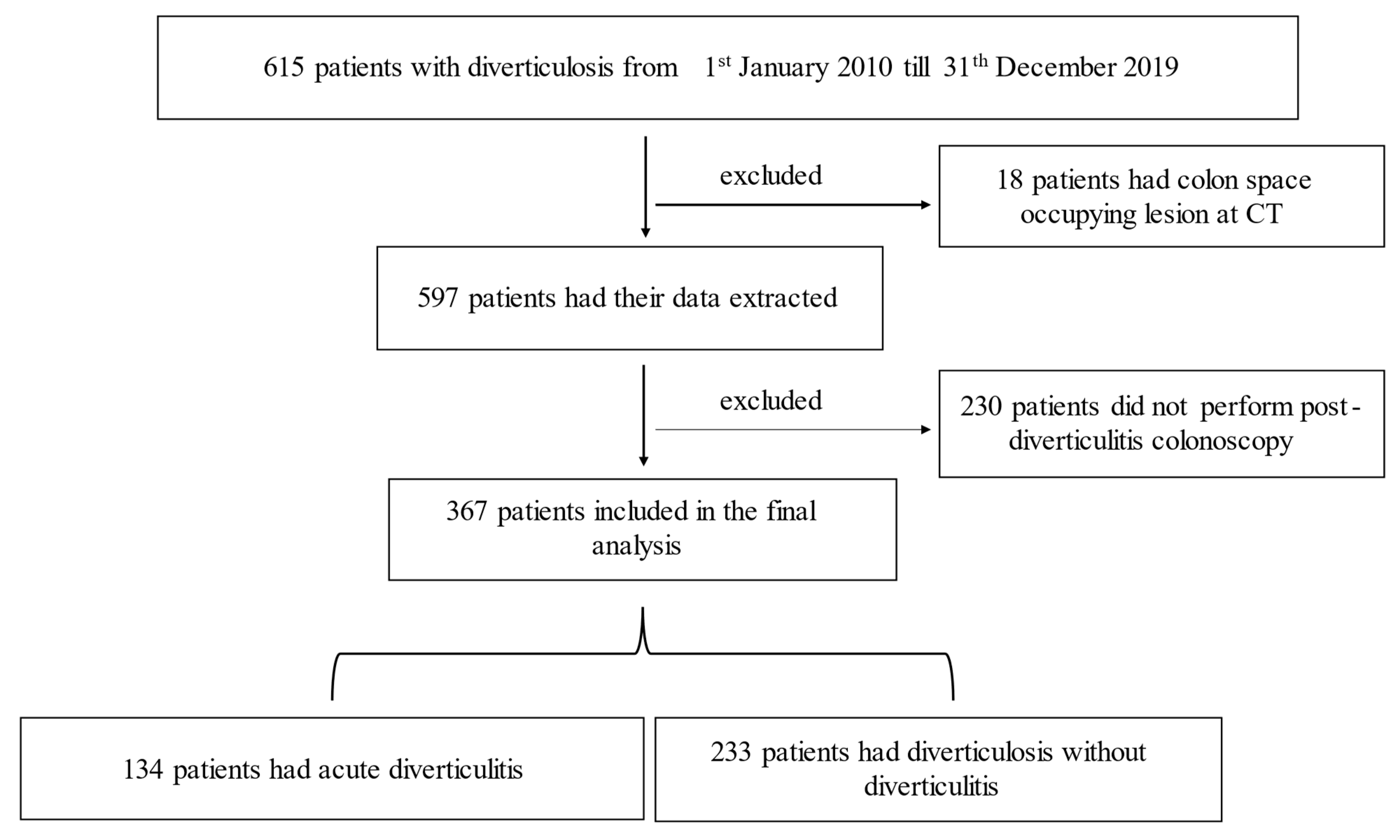
5.1. Demographics, Baseline Characteristics, and Colonoscopic Findings
5.2. Univariate Analysis of the Association between Colonoscopic Findings and Diverticulitis
5.3. Parameters Associated with the Diagnosis of Colonic Adenomas and CRC among Patients Who Had Diverticulitis
5.4. Association of Diverticulitis Severity with Colonoscopic Diagnosis of Colonic Adenoma and CRC
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peppas, G.; Bliziotis, I.A.; Oikonomaki, D.; Falagas, M.E. Outcomes after medical and surgical treatment of diverticulitis: A systematic review of the available evidence. J. Gastroenterol. Hepatol. 2007, 22, 1360–1368. [Google Scholar] [CrossRef]
- Stollman, N.; Raskin, J.B. Diverticular disease of the colon. Lancet 2004, 363, 631–639. [Google Scholar] [CrossRef] [Green Version]
- Brian West, A. The pathology of diverticulosis: Classical concepts and mucosal changes in diverticula. J. Clin. Gastroenterol. 2006, 40 (Suppl. 3), S126–S131. [Google Scholar] [CrossRef]
- Etzioni, D.A.; Mack, T.M.; Beart, R.W., Jr.; Kaiser, A.M. Diverticulitis in the United States: 1998–2005: Changing patterns of disease and treatment. Ann. Surg. 2009, 249, 210–217. [Google Scholar] [CrossRef]
- Stefansson, T.; Ekbom, A.; Sparen, P.; Pahlman, L. Increased risk of left sided colon cancer in patients with diverticular disease. Gut 1993, 34, 499–502. [Google Scholar] [CrossRef] [Green Version]
- Stefansson, T.; Ekbom, A.; Sparen, P.; Pahlman, L. Association between sigmoid diverticulitis and left-sided colon cancer: A nested, population-based, case control study. Scand. J. Gastroenterol. 2004, 39, 743–747. [Google Scholar] [CrossRef] [PubMed]
- Granlund, J.; Svensson, T.; Granath, F.; Hjern, F.; Ekbom, A.; Blomqvist, P.; Schmidt, P.T. Diverticular disease and the risk of colon cancer—A population-based case-control study. Aliment. Pharmacol. Ther. 2011, 34, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Ekbom, A. Is diverticular disease associated with colonic malignancy? Dig. Dis. 2012, 30, 46–50. [Google Scholar] [CrossRef]
- Stollman, N.; Smalley, W.; Hirano, I.; AGA Institute Clinical Guidelines Committee. American Gastroenterological Association Institute Guideline on the Management of Acute Diverticulitis. Gastroenterology 2015, 149, 1944–1949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westwood, D.A.; Eglinton, T.W.; Frizelle, F.A. Routine colonoscopy following acute uncomplicated diverticulitis. Br. J. Surg. 2011, 98, 1630–1634. [Google Scholar] [CrossRef] [PubMed]
- Khoury, T.; Mahamid, M.; Lubany, A.; Safadi, M.; Farah, A.; Sbeit, W.; Mari, A. Underlying Colorectal Cancer Was Rarely Detected After an Episode of Acute Diverticulitis: A Retrospective Analysis of 225 Patients. J. Gastrointest. Cancer 2020, 51, 48–52. [Google Scholar] [CrossRef]
- Hinchey, E.J.; Schaal, P.G.; Richards, G.K. Treatment of perforated diverticular disease of the colon. Adv. Surg. 1978, 12, 85–109. [Google Scholar] [PubMed]
- Lau, K.C.; Spilsbury, K.; Farooque, Y.; Kariyawasam, S.B.; Owen, R.G.; Wallace, M.H.; Makin, G.B. Is colonoscopy still mandatory after a CT diagnosis of left-sided diverticulitis: Can colorectal cancer be confidently excluded? Dis. Colon Rectum 2011, 54, 1265–1270. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.O. Clinical practice. Diverticulitis. N. Engl. J. Med. 2007, 357, 2057–2066. [Google Scholar] [CrossRef] [PubMed]
- Daniels, L.; Unlu, C.; de Wijkerslooth, T.R.; Dekker, E.; Boermeester, M.A. Routine colonoscopy after left-sided acute uncomplicated diverticulitis: A systematic review. Gastrointest. Endosc. 2014, 79, 378–389. [Google Scholar] [CrossRef]
- Sharma, P.V.; Eglinton, T.; Hider, P.; Frizelle, F. Systematic review and meta-analysis of the role of routine colonic evaluation after radiologically confirmed acute diverticulitis. Ann. Surg. 2014, 259, 263–272. [Google Scholar] [CrossRef]
- Lee, D.; Jung, K.U.; Kim, H.O.; Kim, H.; Chun, H.K. Association between oral health and colorectal adenoma in a screening population. Medicine 2018, 97, e12244. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.S.; Kim, N.H.; Yang, H.J.; Park, S.K.; Park, J.H.; Park, D.I.; Sohn, C.I. The impact of passive smoking on the risk of colorectal neoplasia in never, former, and current smokers. J. Gastroenterol. Hepatol. 2018, 33, 1023–1030. [Google Scholar] [CrossRef]
- Chan, D.K.H.; Tan, K.K. There Is No Role for Colonoscopy after Diverticulitis among Asian Patients Less than 50 Years of Age. Gastrointest. Tumors 2017, 3, 136–140. [Google Scholar] [CrossRef] [Green Version]
- Zulli, C.; Maurano, A.; Tammaro, S. Endoscopic closure of a rectal diverticulum perforation during a diagnostic colonoscopy. Acta Gastroenterol. Belg. 2015, 78, 344–345. [Google Scholar]
- Lahat, A.; Yanai, H.; Menachem, Y.; Avidan, B.; Bar-Meir, S. The feasibility and risk of early colonoscopy in acute diverticulitis: A prospective controlled study. Endoscopy 2007, 39, 521–524. [Google Scholar] [CrossRef]
- Anderson, J.C.; Messina, C.R.; Cohn, W.; Gottfried, E.; Ingber, S.; Bernstein, G.; Coman, E.; Polito, J. Factors predictive of difficult colonoscopy. Gastrointest. Endosc. 2001, 54, 558–562. [Google Scholar] [CrossRef] [PubMed]
- Diamond, S.J.; Enestvedt, B.K.; Jiang, Z.; Holub, J.L.; Gupta, M.; Lieberman, D.A.; Eisen, G.M. Adenoma detection rate increases with each decade of life after 50 years of age. Gastrointest. Endosc. 2011, 74, 135–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, J.; Kalady, M.F.; Church, J. Young age of onset colorectal cancers. Int. J. Colorectal Dis. 2015, 30, 1653–1657. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Parameter | Group A (with Diverticulitis) | Group B (Diverticulosis) | p-Value |
|---|---|---|---|
| Number of patients | 134 | 233 | - |
| Age | 68.3 ± 10.5 | 70.5 ± 7.8 | 0.01 |
| Gender, N (%) | |||
| Male | 93 (69.4) | 149 (63.9) | 0.28 |
| Female | 41 (30.6) | 84 (36.1) | |
| Medical history | |||
| Hyperlipidemia | 80 (59.7) | 136 (58.4) | 0.80 |
| Hypertension | 97 (72.4) | 161 (69.5) | 0.51 |
| Chornic renal failure | 5 (3.7) | 16 (6.9) | 0.21 |
| Congestive heart failure | 5 (3.7) | 15 (6.4) | 0.27 |
| Diabetes mellitus | 106 (79.1) | 45 (19.3) | <0.0001 |
| Obesity | 106 (79.1) | 43 (18.5) | <0.0001 |
| Smoking, N (%) | 43 (31.8) | 50 (21.5) | 0.02 |
| Statin use, N (%) | 62 (46.3) | 97 (41.6) | 0.38 |
| NSAID use, N (%) | 13 (9.7) | 19 (8.2) | 0.61 |
| Aspirin use, N (%) | 81 (60) | 127 (54.5) | 0.27 |
| Colonoscopic findings, N (%) | |||
| Adenomas and CRC | 44 (32.8) | 57 (24.5) | 0.08 |
| CRC alone | 2 (1.5) | 4 (1.7) | 0.87 |
| Adenomas alone | 42 (31.3) | 53 (22.7) | 0.07 |
| Adenoma detection rate, N (%) | 42 (31.3) | 53 (22.7) | - |
| Pathological Findings | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|
| Adenomas and CRC | 1.51 | 0.94–2.41 | 0.085 |
| Adenomas alone | 1.60 | 0.96–2.50 | 0.07 |
| CRC alone | 0.87 | 0.16–4.80 | 0.87 |
| Parameter | Group C | Group D | p-Value |
|---|---|---|---|
| Number of patients | 44 | 90 | |
| Age | 69.02 ± 9.5 | 67.9 ± 10.9 | 0.27 |
| Gender, N (%) | |||
| Male | 38 (86.4) | 55 (61.1) | 0.001 for male |
| Female | 6 (13.6) | 35 (38.9) | |
| Medical history | |||
| Hyperlipidemia | 24 (54.5) | 56 (62.2) | 0.19 |
| Hypertension | 31 (70.5) | 66 (73.3) | 0.36 |
| Chornic renal failure | 2 (4.5) | 3 (3.3) | 0.36 |
| Congestive heart failure | 3 (6.8) | 2 (2.2) | 0.09 |
| Diabetes mellitus | 34 (77.3) | 72 (80) | 0.35 |
| Obesity | 34 (77.3) | 72 (80) | 0.35 |
| Smoking, N (%) | 40 (90.5) | 3 (3.4) | <0.0001 |
| Statin use, N (%) | 21 (47.7) | 41 (45.6) | 0.40 |
| NSAID use, N (%) | 6 (13.6) | 7 (7.8) | 0.14 |
| Aspirin use, N (%) | 28 (63.6) | 53 (58.9) | 0.30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mari, A.; Khoury, T.; Sbeit, W. Post-Diverticulitis Colonoscopy Was Not Associated with Higher Colonic Adenoma and Carcinoma: A Multicenter Case–Control Study. Medicina 2021, 57, 682. https://doi.org/10.3390/medicina57070682
Mari A, Khoury T, Sbeit W. Post-Diverticulitis Colonoscopy Was Not Associated with Higher Colonic Adenoma and Carcinoma: A Multicenter Case–Control Study. Medicina. 2021; 57(7):682. https://doi.org/10.3390/medicina57070682
Chicago/Turabian StyleMari, Amir, Tawfik Khoury, and Wisam Sbeit. 2021. "Post-Diverticulitis Colonoscopy Was Not Associated with Higher Colonic Adenoma and Carcinoma: A Multicenter Case–Control Study" Medicina 57, no. 7: 682. https://doi.org/10.3390/medicina57070682
APA StyleMari, A., Khoury, T., & Sbeit, W. (2021). Post-Diverticulitis Colonoscopy Was Not Associated with Higher Colonic Adenoma and Carcinoma: A Multicenter Case–Control Study. Medicina, 57(7), 682. https://doi.org/10.3390/medicina57070682