
Open Reduction in Subtrochanteric Femur Fractures Is Not Accompanied by a Higher Rate of Complications

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Patient Inclusion
2.3. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Primary Outcome Parameter
3.3. Secondary Outcome Parameters
4. Discussion
4.1. Primary Outcome Parameter
4.2. Secondary Outcome Parameters
4.3. Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marks, R. Hip fracture epidemiological trends, outcomes, and risk factors, 1970-2009. Int. J. Gen. Med. 2009, 3, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Miedel, R.; Törnkvist, H.; Ponzer, S.; Söderqvist, A.; Tidermark, J. Musculoskeletal function and quality of life in elderly patients after a subtrochanteric femoral fracture treated with a cephalomedullary nail. J. Orthop. Trauma 2011, 25, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Buecking, B.; Ruchholtz, S. Trochanteric Fractures–Surgical Treatment and Short Term Outcome. OUP Orthopädische Unf. Prax. 2012, 1, 153–159. [Google Scholar]
- Carow, J.; Carow, J.B.; Coburn, M.; Kim, B.-S.; Bücking, B.; Bliemel, C.; Bollheimer, L.C.; Werner, C.J.; Bach, J.P.; Knobe, M. Mortality and cardiorespiratory complications in trochanteric femoral fractures: a ten year retrospective analysis. Int. Orthop. 2017, 41, 2371–2380. [Google Scholar] [CrossRef] [PubMed]
- Boyd, H.B.; Griffin, L.L. Classification and treatment of trochanteric fractures. Arch. Surg. 1949, 58, 853–866. [Google Scholar] [CrossRef] [PubMed]
- Parker, M.; Dutta, B.; Sivaji, C.; Pryor, G. Subtrochanteric fractures of the femur. Injury 1997, 28, 91–95. [Google Scholar] [CrossRef]
- AWMF. Leitlinie Pertrochantäre Oberschenkelfraktur. 2015. Accessed on: 7 July 2020.
- Shukla, S.; Johnston, P.; Ahmad, M.; Wynn-Jones, H.; Patel, A.; Walton, N. Outcome of traumatic subtrochanteric femoral fractures fixed using cephalo-medullary nails. Injury 2007, 38, 1286–1293. [Google Scholar] [CrossRef] [PubMed]
- Codesido-Vilar, P.; Mejía-Casado, A.; Riego-Fernández, J.; Rodriguez-Casas, N.; García-Cabanas, S.; Rivas-Felice, J.; García-Quevedo, L. Consequences of quality of reduction on osteosynthesis complications and quality of life in elderly patients with subtrochanteric fracture. Rev. Española Cirugía Ortopédica Traumatol. 2018, 62, 240–247. [Google Scholar] [CrossRef]
- Krappinger, D.; Wolf, B.; Dammerer, D.; Thaler, M.; Schwendinger, P.; Lindtner, R.A. Risk factors for nonunion after intramedullary nailing of subtrochanteric femoral fractures. Arch. Orthop. Trauma Surg. 2019, 139, 769–777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasha, S.; Yalamanchili, R.K. Management of subtrochanteric fractures by nail osteosynthesis: A review of tips and tricks. Int. Orthop. 2019, 44, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Trikha, V.; Das, S.; Agrawal, P.; Arkesh, M.; Dhaka, S.K. Role of percutaneous cerclage wire in the management of subtrochanteric fractures treated with intramedullary nails. Chin. J. Traumatol. 2018, 21, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.-C.; Jha, A.; Oh, C.-W.; Durai, S.K.; Kim, Y.-W.; Kim, J.-H.; Oh, J.-K. The pointed clamp reduction technique for spiral subtrochanteric fractures: A technical note. Injury 2014, 45, 1000–1005. [Google Scholar] [CrossRef] [PubMed]
- Malik, M.H.A.; Harwood, P.; Diggle, P.; Khan, S.A. Factors affecting rates of infection and nonunion in intramedullary nailing. J. Bone Jt. Surgery Br. Vol. 2004, 86, 556–560. [Google Scholar] [CrossRef] [Green Version]
- Codesido, P.; Mejía, A.; Riego, J.; Ojeda-Thies, C. Subtrochanteric fractures in elderly people treated with intramedullary fixation: quality of life and complications following open reduction and cerclage wiring versus closed reduction. Arch. Orthop. Trauma Surg. 2017, 137, 1077–1085. [Google Scholar] [CrossRef] [PubMed]
- Boldin, C.; Seibert, F.J.; Fankhauser, F.; Peicha, G.; Grechenig, W.; Szyszkowitz, R. The proximal femoral nail (PFN)-A minimal invasive treatment of unstable proximal femoral fractures: A prospective study of 55 patients with a follow-up of 15 months. Acta Orthop. Scand. 2003, 74, 53–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AUC–Akademie der Unfallchirurgie; Arbeitskreis AltersTraumaRegister DGU. The geriatric trauma register of the DGU—current status, methods and publication guidelines. Unfallchirurg 2019, 122, 820–822. [Google Scholar] [CrossRef] [Green Version]
- Kani, K.K.; Porrino, J.A.; Mulcahy, H.; Chew, F.S. Fragility fractures of the proximal femur: review and update for radiologists. Skelet. Radiol. 2019, 48, 29–45. [Google Scholar] [CrossRef] [PubMed]
- Tevanov, I.; Liciu, E.; Chirila, M.O.; Dusca, A.; Ulici, A. The use of 3D printing in improving patient-doctor relationship and malpractice prevention. Rom. J. Leg. Med. 2017, 25, 279–282. [Google Scholar] [CrossRef]
- Hoskins, W.; Bingham, R.; Joseph, S.; Liew, D.; Love, D.; Bucknill, A.; Oppy, A.; Griffin, X. Griffin, Subtrochanteric fracture: The effect of cerclage wire on fracture reduction and outcome. Injury 2015, 46, 1992–1995. [Google Scholar] [CrossRef] [PubMed]
- Knobe, M.; Böttcher, B.; Coburn, M.; Friess, T.; Bollheimer, L.C.; Heppner, H.J.; Werner, C.J.; Bach, J.-P.; Wollgarten, M.; Poßelt, S.; et al. Geriatric Trauma Center DGU®: Evaluation of clinical and economic parameters: A pilot study in a german university hospital. Unfallchirurg 2019, 122, 134–146. [Google Scholar] [CrossRef] [PubMed]
- Dubljanin-Raspopović, E.; Marković-Denić, L.; Marinković, J.; Nedeljković, U.; Bumbaširević, M. Does early functional outcome predict 1-year mortality in elderly patients with hip fracture? Clin. Orthop. Relat. Res. 2013, 471, 2703–2710. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Patient Characteristics | All (n = 506) |
|---|---|
| Baseline Data—Initial Stay | |
| Age (n) | n = 506 |
| Median (Interquartile Range) (IQR) | 85 (81, 89) |
| Gender | n= 506 |
| Female | 74.1% (n = 375) |
| ASA Score | n= 480 |
| 1 | 0.417% (n = 2) |
| 2 | 23.1% (n = 111) |
| 3 | 67.9% (n = 326) |
| 4 | 8.12% (n = 39) |
| 5 | 0.417% (n = 2) |
| Type of Surgery (Subtrochanteric Fracture) | n = 506 |
| Intramedullary nail open reduction without wire cerclage | 73.3% (n = 371) |
| Intramedullary nail open reduction with wire cerclage | 5.5% (n = 28) |
| Intramedullary nail closed reduction | 21.1% (n = 107) |
| Length of Stay (Median/IQR) (n = 463) (Survivors) | 17.04 (11.06, 22.08) |
| Anticoagulation on Admission (n = 487) | |
| No anticoagulation | 50.3% (n = 245) |
| Vitamin K antagonist | 18.2% (n = 44) |
| Acetylsalicylic acid | 49.6% (n = 120) |
| Other thrombocyte aggregation inhibitors | 7.02% (n = 17) |
| Direct thrombin inhibitor (Dabigatran) | 3.72% (n = 9) |
| Direct factor Xa inhibitor (Rivaroxaban, Apixaban) | 22.3% (n = 54) |
| Heparin | 2.07% (n = 5) |
| Other | 2.07% (n = 5) |
| Surgical Complication (during initial stay) | 3.56% (n = 18) |
| Removal of implant or osteosynthesis | 11.1% (n = 2) |
| Revision of osteosynthesis | 22.2% (n = 4) |
| Soft tissue intervention | 66.7% (n = 12) |
| Others | 16.7% (n = 3) |
| Mortality | (n = 505) |
| During initial stay | 7.52% (n = 38) |
| Length of Stay (Median/IQR) (n=) (Survivors) | n = 463 17.04 (11.06, 22.08) |
| Discharge After Hospital (initial stay) | n = 461 |
| Home | 22.28% (n = 105) |
| Nursing home | 29.9% (n = 138) |
| Geriatric rehabilitation | 41.6% (n = 192) |
| Clinic for follow-up treatment | 3.90% (n = 18) |
| Other (different hospital, different department, other) | 1.74% (n = 8) |
| Baseline data—follow-up | |
| Surgical Complication | |
| Yes | 1.38% (n = 7) |
| Removal of implant or osteosynthesis | 42.9% (n = 3) |
| Revision of osteosynthesis | 14.3% (n = 1) |
| Conversion in total hip arthroplasty | 14.3% (n = 1) |
| Girdlestone | 14.3% (n = 1) |
| Soft tissue intervention | 14.3% (n = 1) |
| Others | 28.6% (n = 2) |
| Mortality | |
| Yes | 2.57% (n = 13) |
| Current Location | n = 140 |
| Home | 72.9% (n = 102) |
| Nursing home | 25.7% (n = 36) |
| Hospital | 0.714% (n = 1) |
| Other | 0.714% (n = 1) |
| Open Reduction (n = 399) | Closed Reduction (n = 107) | p | |
|---|---|---|---|
| Baseline Data | |||
| Age n | 399 | 107 | 0.327 * |
| Median (Interquartile Range) (IQR) | 85 (81; 89) | 84 (80; 89) | |
| Gender | 0.233 + | ||
| Female | 301(75.4%) | 74 (69.2%) | |
| Male | 98 (24.6%) | 33 (30.8%) | |
| ASA Score | 0.198 + | ||
| 1 | 1 (0.3%) | 1 (1.0%) | |
| 2 | 92 (24.4%) | 19 (18.4%) | |
| 3 | 256 (67.9%) | 70 (68.0%) | |
| 4 | 26 (6.9%) | 13 (12.6%) | |
| 5 | 2 (0.5%) | ||
| Anticoagulation on Admission | 0.088 + | ||
| No Anticoagulation | 48.2% (n = 185) | 58.3 ((n = 60) | |
| Walking Ability Before Fracture | |||
| Without aids/forearm crutches | 168 (46.2%) | 52 (52%) | 0.538 + |
| Walker | 128 (35.2%) | 28 (28%) | |
| Only at home | 58 (15.9%) | 16 (16%) | |
| No walking possible | 10 (2.8%) | 4 (4%) | |
| Full Weight Bearing of the Fracture is Allowed | 0.073 | ||
| Yes | 66.0% (n = 262) | 75.7% (n = 81) | |
| Primary Outcome Parameter | |||
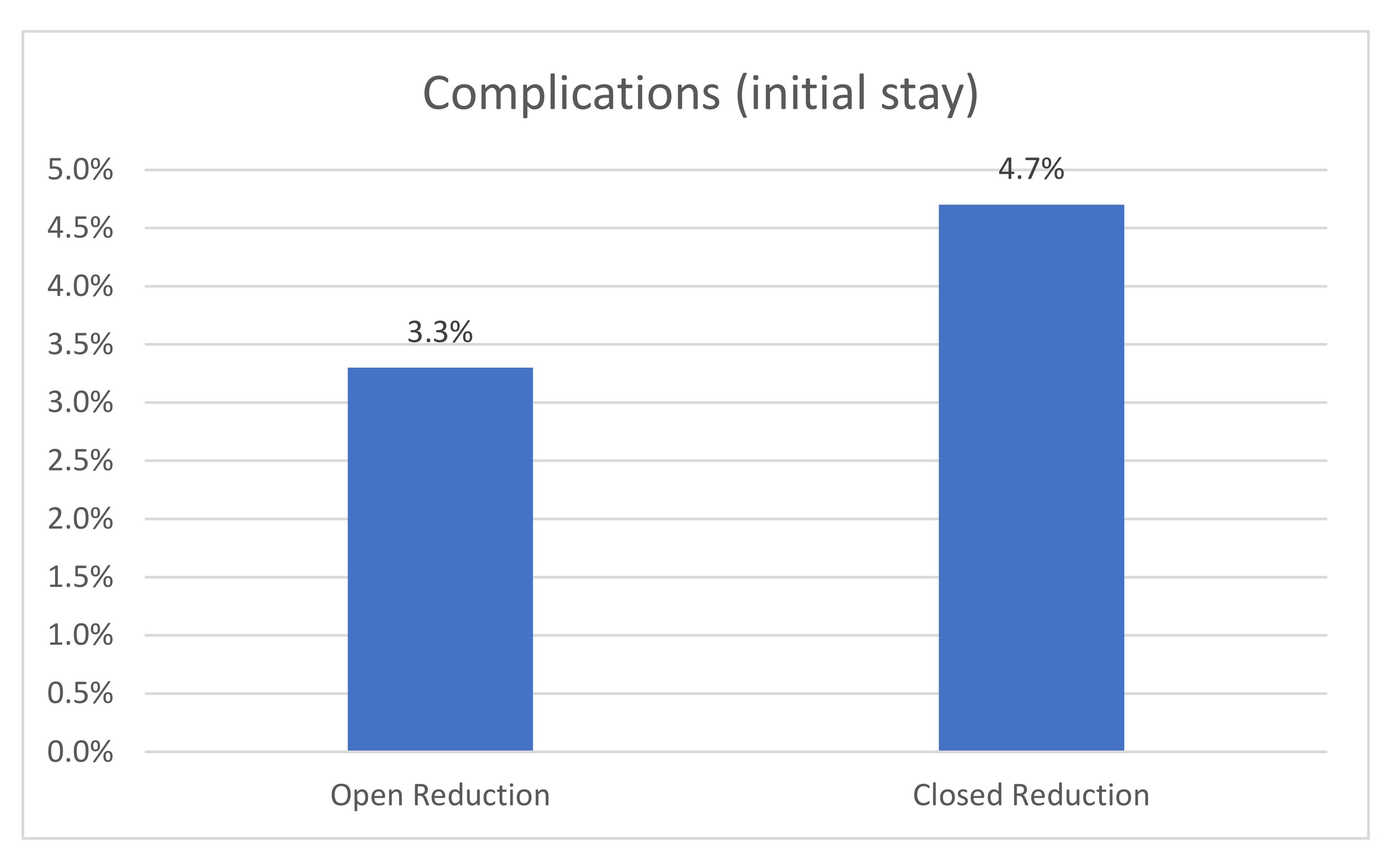
| Surgical Complication | 0.687 | ||
| Yes | 3.26% (n = 13) | 4.67% (n = 5) | |
| Soft tissue intervention | 2.5% (n = 10) | 1.8% (n = 2) | |
| Removal of Implant or osteosynthesis | 0.3% (n = 1) | 0.9% (n = 1) | |
| Revision of osteosynthesis | 0.5% (n = 2) | 1.8% (n = 2) | |
| Periosteosynthetic fracture | 0% (n = 0) | 0.9% (n = 1) | |
| Others | 0.8% (n = 3) | 0% (n = 0) | |
| Secondary Outcome Parameter | |||
| Discharge After Hospital (initial stay) (Survivors) | n = 366 | n = 95 | p = 0.846 |
| Home | 23.5% (n = 86) | 20% (n = 19) | |
| Nursing home | 30.3% (n = 111) | 28.4% (n = 27) | |
| Geriatric rehabilitation | 40.4% (n = 148) | 46.3% (n = 44) | |
| Clinic for follow-up treatment | 4.10% (n = 15) | 3.16% (n = 3) | |
| Other | 1.64% (n = 6) | 2.11% (n = 2) | |
| Mortality | 6.78% (n = 27) | 10.3% (n = 11) | 0.312 |
| Change in Walking Ability (pre-fracture to 7 days post-op) | 0.008 + | ||
| Worse | 61.8% (n = 218) | 77.1% (n = 74) | |
| No change | 28.9% (n = 102) | 20.8% (n = 20) | |
| Better | 9.4% (n = 33) | 2.1% (n = 2) | |
| Lengths of stay (days) (Survivors) | n = 367 | n = 96 | 0.968 ^ |
| Median (IQR) | 17 (11, 22.1) | 16.6 (12, 21.6) |
| Open Reduction | Closed Reduction | ||
|---|---|---|---|
| Follow-Up Conducted | 38.8% (n = 155) | 36.4% (n = 39) | |
| Primary Outcome Parameter | |||
| Surgical Complication | n = 130 | n = 36 | p = 1 |
| Yes | 3.9% (n = 5) | 5.6% (n = 2) | |
| Soft tissue intervention | n = 0 | n = 1 | |
| Removal of implant or osteosynthesis | n = 2 | n = 1 | |
| Revision of osteosynthesis | n = 1 | n = 0 | |
| Conversion in HTEP | n = 1 | n = 0 | |
| Girdlestone | n = 1 | n = 0 | |
| Others | n = 1 | n = 1 | |
| Secondary Outcome Parameter | |||
| Mortality | 8.39% (n = 13 additional deaths in FU Period) | 0% (n = 0) | 0.075 |
| Change in Walking Ability (pre-fracture to 120-day follow-up) | 0.82 + | ||
| Worse | 65 (60.2%) | 19 (59.4%) | |
| No change | 39 (36.1%) | 11 (34.4%) | |
| Better | 4 (3.7%) | 2 (6.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knauf, T.; Eschbach, D.; Buecking, B.; Knobe, M.; Barthel, J.; Rascher, K.; Ruchholtz, S.; Aigner, R.; Schoeneberg, C.; on behalf of the Registry for German Trauma DGU. Open Reduction in Subtrochanteric Femur Fractures Is Not Accompanied by a Higher Rate of Complications. Medicina 2021, 57, 659. https://doi.org/10.3390/medicina57070659
Knauf T, Eschbach D, Buecking B, Knobe M, Barthel J, Rascher K, Ruchholtz S, Aigner R, Schoeneberg C, on behalf of the Registry for German Trauma DGU. Open Reduction in Subtrochanteric Femur Fractures Is Not Accompanied by a Higher Rate of Complications. Medicina. 2021; 57(7):659. https://doi.org/10.3390/medicina57070659
Chicago/Turabian StyleKnauf, Tom, Daphne Eschbach, Benjamin Buecking, Matthias Knobe, Juliane Barthel, Katherine Rascher, Steffen Ruchholtz, Rene Aigner, Carsten Schoeneberg, and on behalf of the Registry for German Trauma DGU. 2021. "Open Reduction in Subtrochanteric Femur Fractures Is Not Accompanied by a Higher Rate of Complications" Medicina 57, no. 7: 659. https://doi.org/10.3390/medicina57070659
APA StyleKnauf, T., Eschbach, D., Buecking, B., Knobe, M., Barthel, J., Rascher, K., Ruchholtz, S., Aigner, R., Schoeneberg, C., & on behalf of the Registry for German Trauma DGU. (2021). Open Reduction in Subtrochanteric Femur Fractures Is Not Accompanied by a Higher Rate of Complications. Medicina, 57(7), 659. https://doi.org/10.3390/medicina57070659