
Development and Application of Computerized Risk Registry and Management Tool Based on FMEA and FRACAS for Total Testing Process


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
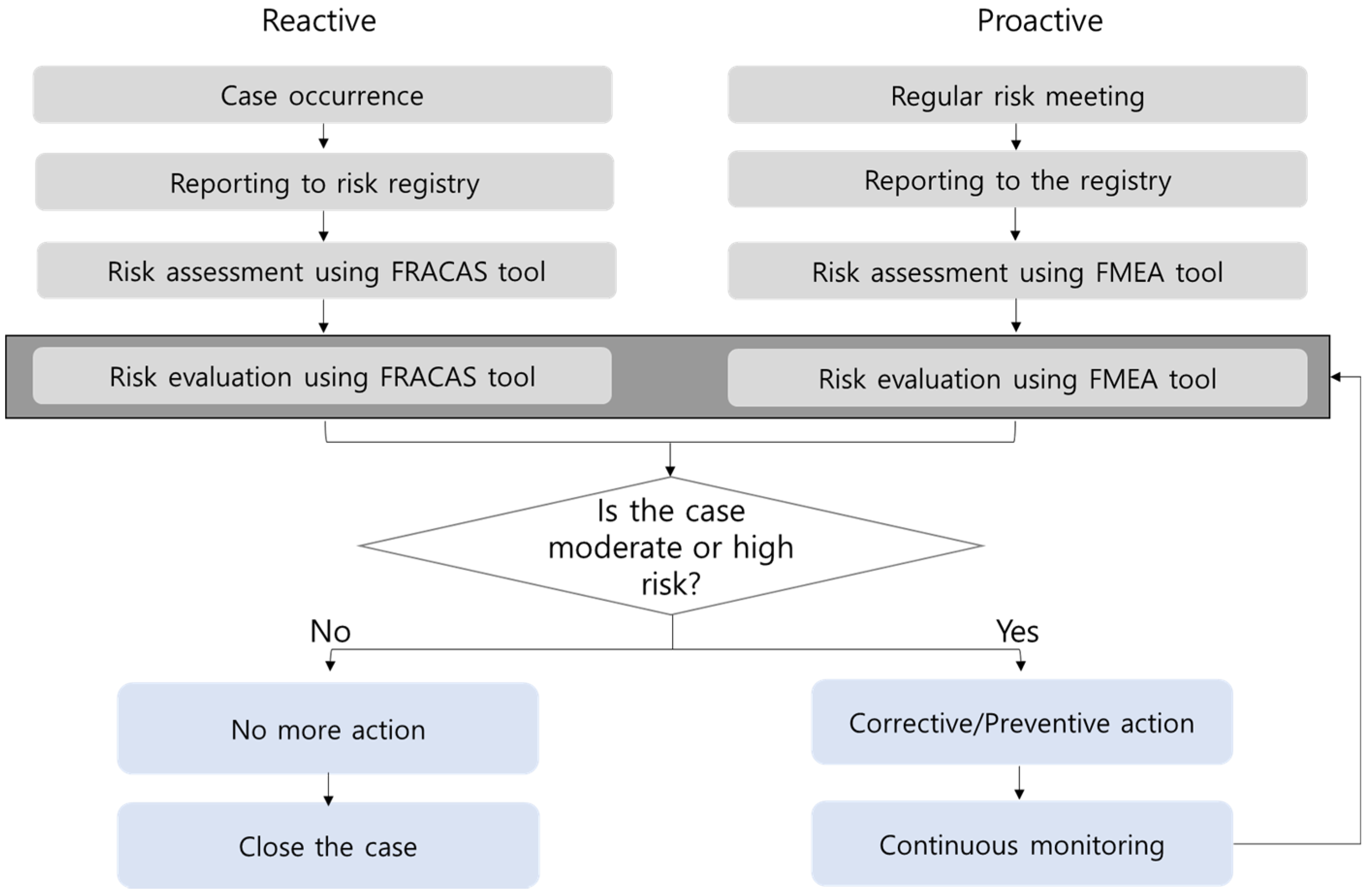
2.2. Concept Flow Diagram for Continuous and Practical Risk Management
2.3. Development of Computerized Risk Registry and Management Tools (RRMT)
2.4. Application and Scoring of Risk Management
3. Results
3.1. Concept Flow Diagram for Continuous and Practical Risk Management System
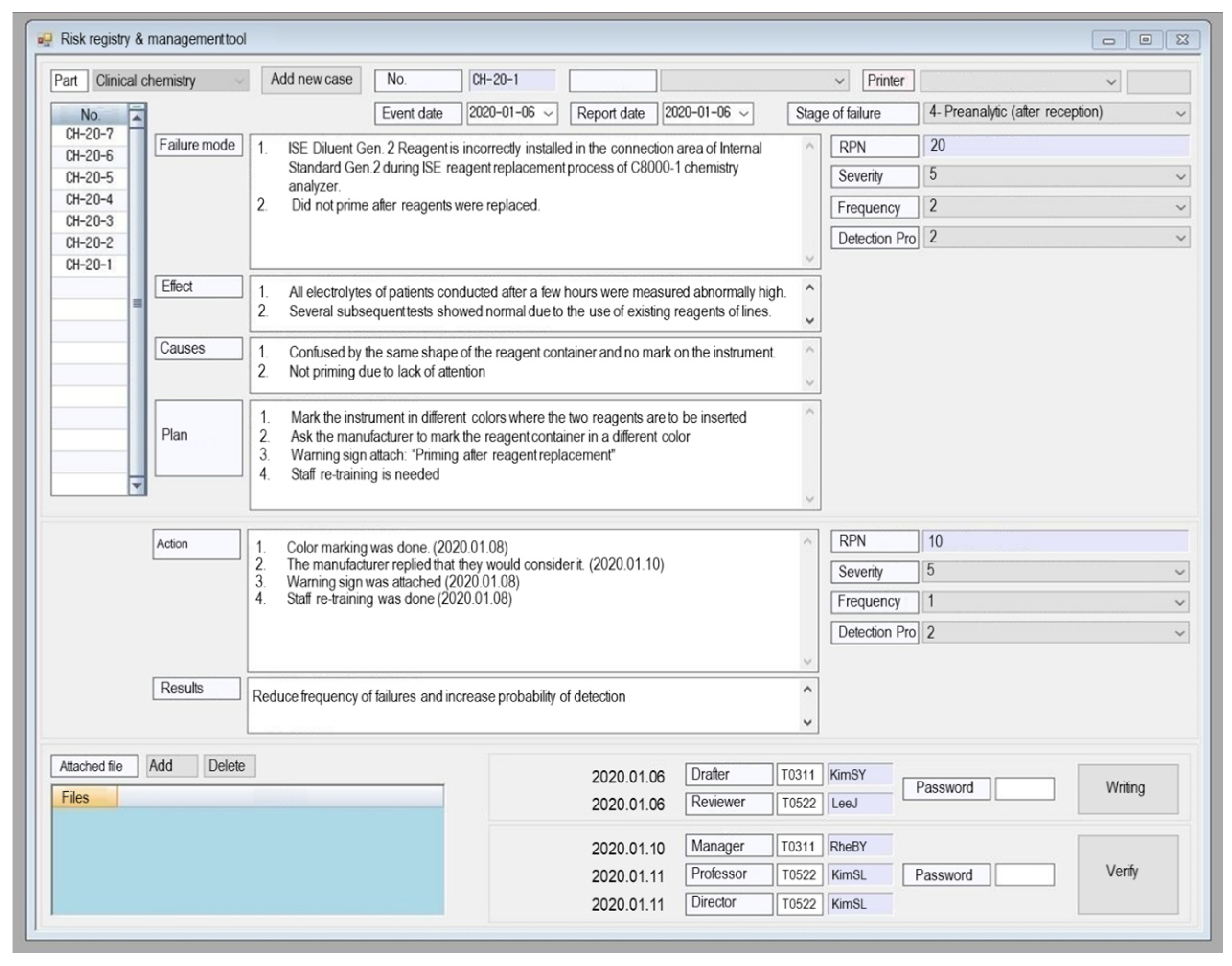
3.2. Developed RRMT
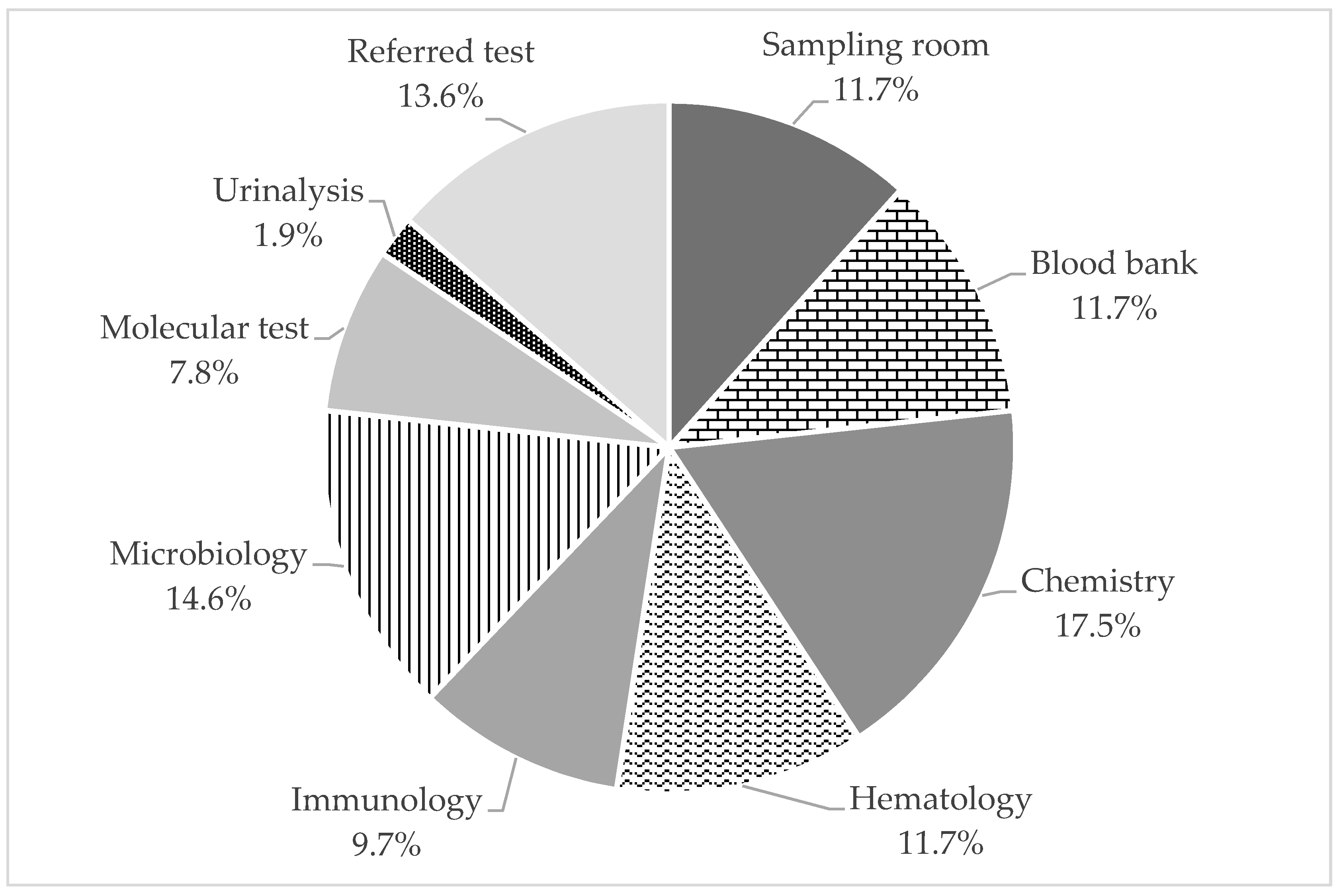
3.3. Application Results of RRMT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Standard Organization (ISO). ISO 31000:2018 Risk management—Guidelines; International Standard Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Youngberg, B.J. Principles of Risk Management and Patient Safety, 1st ed.; Jones & Bartlett Learning: Burlington, MA, USA, 2010; p. 504. [Google Scholar]
- Njoroge, S.W.; Nichols, J.H. Risk management in the clinical laboratory. Ann. Lab. Med. 2014, 34, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Aita, A.; Padoan, A.; Antonelli, G.; Sciacovelli, L.; Plebani, M. Patient safety and risk management in medical laboratories: Theory and practical application. J. Lab. Precis. Med. 2017, 2, 75. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute (CLSI). Laboratory Quality Control. Based on Risk Management; Approved Guideline, CLSI document EP23-A; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2011. [Google Scholar]
- Laboratory Medicine Foundation (LMF). Accreditation Checklist for Good Laboratory Practice—Laboratory General; KSLM/LMF: Seoul, Korea, 2019. [Google Scholar]
- International Society for Quality in Health Care (ISQua). Guidelines and Principles for the Development of Health and Social Care Standards, 5th ed.; The International Society for Quality in Health Care: Dublin, Ireland, 2018. [Google Scholar]
- Xia, Y.; Wang, X.; Yan, C.; Wu, J.; Xue, H.; Li, M.; Lin, Y.; Li, J.; Ji, L. Risk assessment of the total testing process based on quality indicators with the Sigma metrics. Clin. Chem. Lab. Med. 2020, 58, 1223–1231. [Google Scholar] [CrossRef] [PubMed]
- Guinon, L.; Soler, A.; Gisell Diaz, M.; Fernandez, R.M.; Rico, N.; Bedini, J.L.; Mira, A.; Alvarez, L. Analytical performance assessment and improvement by means of the Failure mode and effect analysis (FMEA). Biochem. Med. (Zagreb) 2020, 30, 020703. [Google Scholar] [CrossRef] [PubMed]
- Keckler, M.S.; Anderson, K.; McAllister, S.; Rasheed, J.K.; Noble-Wang, J. Development and implementation of evidence-based laboratory safety management tools for a public health laboratory. Saf. Sci. 2019, 117, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Karadag, C.; Demirel, N.N. Continual improvement of the pre-analytical process in a public health laboratory with quality indicators-based risk management. Clin. Chem. Lab. Med. 2019, 57, 1530–1538. [Google Scholar] [CrossRef] [PubMed]
- Mackay, M.A.; Badrick, T.C. Steady state errors and risk of a QC strategy. Clin. Biochem. 2019, 64, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Bunting, R.F., Jr.; Siegal, D. Developing risk management dashboards using risk and quality measures: A visual best practices approach. J. Healthc. Risk Manag. 2017, 37, 8–28. [Google Scholar] [CrossRef] [PubMed]
- Dirnagl, U.; Przesdzing, I.; Kurreck, C.; Major, S. A Laboratory Critical Incident and Error Reporting System for Experimental Biomedicine. PLoS Biol. 2016, 14, e2000705. [Google Scholar] [CrossRef] [PubMed]
- International Standard Organization (ISO). IEC 31010:2019 Risk Management—Risk Assessment Techniques; International Standard Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Clinical and Laboratory Standards Institute (CLSI). Risk Management Techniques to Identify and Control Laboratory Error Sources; Approved Guideline, 2nd ed.; CLSI document EP18-A2; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2009. [Google Scholar]
- Chang, J.; Kim, S.; Yoo, S.J.; Park, E.J.; Um, T.H.; Cho, C.R. Preanalytical Errors in the Central Laboratory of a University Hospital Based on the Analysis of Year-Round Data. Clin. Lab. 2020, 66. [Google Scholar] [CrossRef] [PubMed]
- Chiozza, M.L.; Ponzetti, C. FMEA: A model for reducing medical errors. Clin. Chim. Acta 2009, 404, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.; Kim, S.; Um, T.H.; Cho, C.R.; Shin, D.W.; Yoo, S.J. Real-time display of laboratory testing status improves satisfaction levels in an emergency department: A pilot study. J. Clin. Lab. Anal. 2020, 34, e23290. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Severity of Failure | Frequency of Occurrence | Detection Capability | |||
|---|---|---|---|---|---|
| Description | Score | Description | Score | Description | Score |
| Negligible (minor effect on patients) | 1 | Improbable (once in a lifetime) | 1 | Definitely detected (10 out of 10) | 1 |
| Remote (once every few years) | 2 | Probably detected (7 out of 10) | 2 | ||
| Serious (impairment requiring professional medical intervention) | 3 | Occasional (once per year) | 3 | Moderate (5 out of 10) | 3 |
| Probable (once per month) | 4 | Difficult to detect (2 out of 10) | 4 | ||
| Catastrophic (life-threatening to patients) | 5 | Frequent (once per week) | 5 | Undetectable (0 out of 10) | 5 |
| Failure Phase | Risk Management Type | Sampling Unit | Blood Bank | Chemistry | Hematology | Immunology | Microbiology | Molecular Test | Urinalysis | Referred Test | Total (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Test requesting | Proactive (FMEA) | 2 | 2 | 1 | 1 | 1 | 1 | 8 (7.8) | 9 (8.8) | |||
| Reactive (FRACAS) | 1 | 1 (1.0) | ||||||||||
| Pre-analytic phase: Pre-reception | Proactive (FMEA) | 5 | 1 | 2 | 2 | 1 | 8 | 19 (18.4) | 26 (25.2) | |||
| Reactive (FRACAS) | 3 | 1 | 1 | 2 | 7 (6.8) | |||||||
| Pre-analytic phase: Post-reception | Proactive (FMEA) | 1 | 1 | 4 | 2 | 2 | 2 | 12 (11.7) | 18 (17.5) | |||
| Reactive (FRACAS) | 1 | 3 | 1 | 1 | 6 (5.8) | |||||||
| Analytic | Proactive (FMEA) | 2 | 1 | 8 | 3 | 3 | 3 | 20 (19.4) | 28 (27.2) | |||
| Reactive (FRACAS) | 1 | 1 | 2 | 2 | 2 | 8 (7.8) | ||||||
| Post-analytic | Proactive (FMEA) | 1 | 5 | 2 | 1 | 2 | 1 | 12 (11.7) | 22 (21.4) | |||
| Reactive (FRACAS) | 1 | 2 | 1 | 1 | 4 | 1 | 10 (9.7) | |||||
| Total | 12 | 12 | 18 | 12 | 10 | 15 | 8 | 2 | 14 | 103 (100) | ||
| RPN Category | Risk Evaluation after Corrective/Preventive Action | Sampling Room | Blood Bank | Chemistry | Hematology | Immunology | Microbiology | Molecular Test | Urinalysis | Referred Test | Total (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| High-risk (20 ≤ RPN) | Risk reduced Risk not reduced | 1 | 1 | 6 | 5 | 1 | 2 | 1 | 5 | 22 (21.4) | 22 (21.4) | |
| Moderate-risk (10 ≤ RPN < 20) | Risk reduced | 8 | 1 | 3 | 2 | 2 | 1 | 2 | 7 | 25 (24.3) | 26 (25.3) | |
| Risk not reduced * | 1 | 1 (1.0) | ||||||||||
| Low-risk (RPN < 10) | Not applicable | 3 | 10 | 8 | 5 | 7 | 12 | 7 | 3 | 55 (53.4) | 55 (53.4) | |
| Total | 12 | 12 | 18 | 12 | 10 | 15 | 8 | 2 | 14 | 103 (100) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, J.; Yoo, S.J.; Kim, S. Development and Application of Computerized Risk Registry and Management Tool Based on FMEA and FRACAS for Total Testing Process. Medicina 2021, 57, 477. https://doi.org/10.3390/medicina57050477
Chang J, Yoo SJ, Kim S. Development and Application of Computerized Risk Registry and Management Tool Based on FMEA and FRACAS for Total Testing Process. Medicina. 2021; 57(5):477. https://doi.org/10.3390/medicina57050477
Chicago/Turabian StyleChang, Jeonghyun, Soo Jin Yoo, and Sollip Kim. 2021. "Development and Application of Computerized Risk Registry and Management Tool Based on FMEA and FRACAS for Total Testing Process" Medicina 57, no. 5: 477. https://doi.org/10.3390/medicina57050477
APA StyleChang, J., Yoo, S. J., & Kim, S. (2021). Development and Application of Computerized Risk Registry and Management Tool Based on FMEA and FRACAS for Total Testing Process. Medicina, 57(5), 477. https://doi.org/10.3390/medicina57050477