
Impact of Lactate Clearance on Early Outcomes in Pediatric ECMO Patients

 ,
,  , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jenks, C.L.; Raman, L.; Dalton, H.J. Pediatric Extracorporeal Membrane Oxygenation. Crit. Care Clin. 2017, 33, 825–841. [Google Scholar] [CrossRef]
- O’Halloran, C.P.; Andren, K.G.; Mecklosky, J.; Larsen, S.; Brediger, S.; Vitali, S.; Zalieckas, J.M.; Fynn-Thompson, F.; Thiagarajan, R.R.; Alexander, P.M.A. Mortality and Factors Associated with Hemorrhage During Pediatric Extracorporeal Membrane Oxygenation. Pediatr. Crit. Care Med. 2020, 21, 75–81. [Google Scholar] [CrossRef]
- Slottosch, I.; Liakopoulos, O.; Kuhn, E.; Scherner, M.; Deppe, A.-C.; Sabashnikov, A.; Mader, N.; Choi, Y.-H.; Wippermann, J.; Wahlers, T. Lactate and lactate clearance as valuable tool to evaluate ECMO therapy in cardiogenic shock. J. Crit. Care 2017, 42, 35–41. [Google Scholar] [CrossRef]
- Khorsandi, M.; Dougherty, S.; Bouamra, O.; Pai, V.; Curry, P.; Tsui, S.; Clark, S.; Westaby, S.; Al-Attar, N.; Zamvar, V. Extra-corporeal membrane oxygenation for refractory cardiogenic shock after adult cardiac surgery: A systematic review and meta-analysis. J. Cardiothorac. Surg. 2017, 12, 1–13. [Google Scholar] [CrossRef]
- Lazzeri, C.; Bonizzoli, M.; Cianchi, G.; Batacchi, S.; Terenzi, P.; Cozzolino, M.; Bernardo, P.; Peris, A. Lactate and Echocardiography Before Veno-Venous Extracorporeal Membrane Oxygenation Support. Heart Lung Circ. 2018, 27, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Mungan, I.; Kazancı, D.; Bektaş, Ş.; Ademoglu, D.; Turan, S. Does lactate clearance prognosticates outcomes in ECMO therapy: A retrospective observational study. BMC Anesthesiol. 2018, 18, 152. [Google Scholar] [CrossRef] [PubMed]
- Sabashnikov, A.; Djordjevic, I.; Deppe, A.-C.; Kuhn, E.W.; Merkle, J.; Weber, C.; Sindhu, D.; Eghbalzadeh, K.; Zeriouh, M.; Liakopoulos, O.J.; et al. Managing Traps and Pitfalls During Initial Steps of an ECMO Retrieval Program Using a Miniaturized Portable System: What Have We Learned From the First Two Years? Artif. Organs 2018, 42, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Merkle, J.; Azizov, F.; Fatullayev, J.; Weber, C.; Maier, J.; Eghbalzadeh, K.; Sabashnikov, A.; Pfister, R.; Wahlers, T.; Michels, G. Monitoring of adult patient on venoarterial extracorporeal membrane oxygenation in intensive care medicine. J. Thorac. Dis. 2019, 11 (Suppl. 6), S946–S956. [Google Scholar] [CrossRef]
- Azizov, F.; Merkle, J.; Fatullayev, J.; Eghbalzadeh, K.; Djordjevic, I.; Weber, C.; Saenko, S.; Kroener, A.; Zeriouh, M.; Sabashnikov, A.; et al. Outcomes and factors associated with early mortality in pediatric and neonatal patients requiring ex-tracorporeal membrane oxygenation for heart and lung failure. J. Thorac. Dis. 2019, 11 (Suppl. 6), S871–S888. [Google Scholar] [CrossRef]
- Merkle, J.; Azizov, F.; Sabashnikov, A.; Weixler, V.; Weber, C.; Djordjevic, I.; Eghbalzadeh, K.; Kröner, A.; Zeriouh, M.; Wahlers, T.; et al. Pediatric patients requiring extracorporeal membrane oxygenation in heart failure: 30-day outcomes; mid- and long-term survival. A single center experience. Artif. Organs 2019, 43, 966–975. [Google Scholar] [CrossRef] [PubMed]
- Sabashnikov, A.; Merkle, J.; Azizov, F.; Djordjevic, I.; Eghbalzadeh, K.; Tunggal, I.; Weber, C.; Weixler, V.; Rustenbach, C.; Zeriouh, M.; et al. Early and long-term outcomes comparing neonates, infants, and preadolescents requiring ex-tracorporeal membrane oxygenation for heart failure. Perfusion 2019, 35, 323–330. [Google Scholar] [CrossRef]
- Li, C.-L.; Wang, H.; Jia, M.; Ma, N.; Meng, X.; Hou, X.-T. The early dynamic behavior of lactate is linked to mortality in postcardiotomy patients with extracorporeal membrane oxygenation support: A retrospective observational study. J. Thorac. Cardiovasc. Surg. 2015, 149, 1445–1450. [Google Scholar] [CrossRef] [PubMed]
- Napp, L.C.; Kühn, C.; Bauersachs, J. ECMO in cardiac arrest and cardiogenic shock. Herz 2017, 42, 27–44. [Google Scholar] [CrossRef]
- Singh, S.P.; Chauhan, S.; Bisoi, A.K.; Sahoo, M. Lactate clearance for initiating and weaning off extracorporeal membrane oxygenation in a child with regressed left ventricle after arterial switch operation. Ann. Card. Anaesth. 2016, 19, 188–191. [Google Scholar] [CrossRef] [PubMed]
- Attanà, P.; Lazzeri, C.; Picariello, C.; Dini, C.S.; Gensini, G.F.; Valente, S. Lactate and lactate clearance in acute cardiac care patients. Eur. Heart J. Acute Cardiovasc. Care. 2012, 1, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Yanase, S.; Yasuda, K.; Ishii, N. Small-Scale Colorimetric Assays of Intracellular Lactate and Pyruvate in the Nematode Caenorhabditis elegans. J. Vis. Exp. 2018, 16, e57807. [Google Scholar] [CrossRef]
- Zang, Z.; Xu, H.; Dong, L.; Gao, F.; Yan, J. Prognostic significance of early lactate clearance rate for severe acute respiratory failure patients on extracorporeal membrane oxygenation. Chin. J. Tuberc. Respir. Dis. 2014, 37, 197–201. [Google Scholar]
- Schwartz, S.; Floh, A.A. Is glucose metabolism important for patients on extracorporeal membrane oxygenation? Pediatr. Crit. Care Med. 2015, 16, 296–297. [Google Scholar] [CrossRef] [PubMed]
- Jean-St-Michel, E.; Chetan, D.; Schwartz, S.M.; van Arsdell, G.S.; Floh, A.A.; Honjo, O.; Conway, J. Outcomes in Patients with Persistent Ventricular Dysfunction After Stage I Palliation for Hy-poplastic Left Heart Syndrome. Pediatr. Cardiol. 2016, 37, 239–247. [Google Scholar] [CrossRef]
- Luo, Y.; Fritz, C.; Hammache, N.; Grandmougin, D.; Kimmoun, A.; Orlowski, S.; Tran, N.; Albuisson, E.; Levy, B. Low versus standard-blood-flow reperfusion strategy in a pig model of refractory cardiac arrest resuscitated with Extra Corporeal Membrane Oxygenation. Resuscitation 2018, 133, 12–17. [Google Scholar] [CrossRef]
- Park, S.J.; Kim, S.-P.; Kim, J.B.; Jung, S.-H.; Choo, S.J.; Chung, C.H.; Lee, J.W. Blood lactate level during extracorporeal life support as a surrogate marker for survival. J. Thorac. Cardiovasc. Surg. 2014, 148, 714–720. [Google Scholar] [CrossRef] [PubMed]
- Buijs, E.A.; Houmes, R.J.; Rizopoulos, D.; Wildschut, E.D.; Reiss, I.K.; Ince, C.; Tibboel, D. Arterial lactate for predicting mortality in children requiring extracorporeal membrane oxygenation. Minerva Anestesiol. 2014, 80, 1282–1293. [Google Scholar] [PubMed]
- Scolari, F.L.; Schneider, D.; Fogazzi, D.V.; Gus, M.; Rover, M.M.; Bonatto, M.G.; De Araújo, G.N.; Zimerman, A.; Sganzerla, D.; Goldraich, L.A.; et al. Association between serum lactate levels and mortality in patients with cardiogenic shock receiving mechanical circulatory support: A multicenter retrospective cohort study. BMC Cardiovasc. Disord. 2020, 20, 496. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall | Survivors | Non-Survivors | p-Value | |
|---|---|---|---|---|
| Age (days) | 98(12;653) | 128(16;188) | 84(9;5722) | 0.77 |
| Gender (m/f) | 24/17 | 18/9 | 6/8 | 0.19 |
| Weight (gram) | 5040(3247;11,000) | 5200(3230;9000) | 4600(3050;68,000) | 0.44 |
| Length (cm) | 58(51;84) | 58(51;70) | 90(51;180) | 0.38 |
| MAP (mmHg) | 37(26;43) | 35(23;50) | 40(27;43) | 0.74 |
| Heart rate (min−1) | 147(131;177) | 145(135;180) | 160(65;177) | 0.95 |
| Blood sugar (mg/dL) | 200 ± 86 | 196 ± 75 | 209 ± 108 | 0.97 |
| HCO3−1 (mEq/L) | 20.2 ± 6.1 | 22.4 ± 5.3 | 16.8 ± 6.1 | 0.03 |
| Body temperature (°C) | 35.6(34.1;36) | 35.8(35.4;36.3) | 34(32;36) | 0.13 |
| Lactate (mmol/L) | 11 ± 5.8 | 9.8 ± 5.3 | 13.5 ± 6.1 | 0.07 |
| Arterial blood pH | 7.220(7.075;7.304) | 7.273(7.108;7.355) | 7.105(6.815;7.265) | 0.08 |
| Base excess (mEq/L) | −5.6(−14.7;3.1) | −3.1(−5.6;4.0) | −15(−17;−9) | 0.01 |
| paO2 (mmHg) | 41(32;58) | 43(37;57) | 41(26;70) | 0.50 |
| paCO2 (mmHg) | 46(35;64) | 45(36;61) | 50(31;94) | 0.55 |
| Overall | Survivors | Non-Survivors | p-Value | |
|---|---|---|---|---|
| Peak lactate level in the first 24 h of ECMO support (mmol/L) | 11.8 ± 6.8 | 10.4 ± 6.0 | 14.7 ± 7.1 | 0.07 |
| Lactate (mmol/L) | ||||
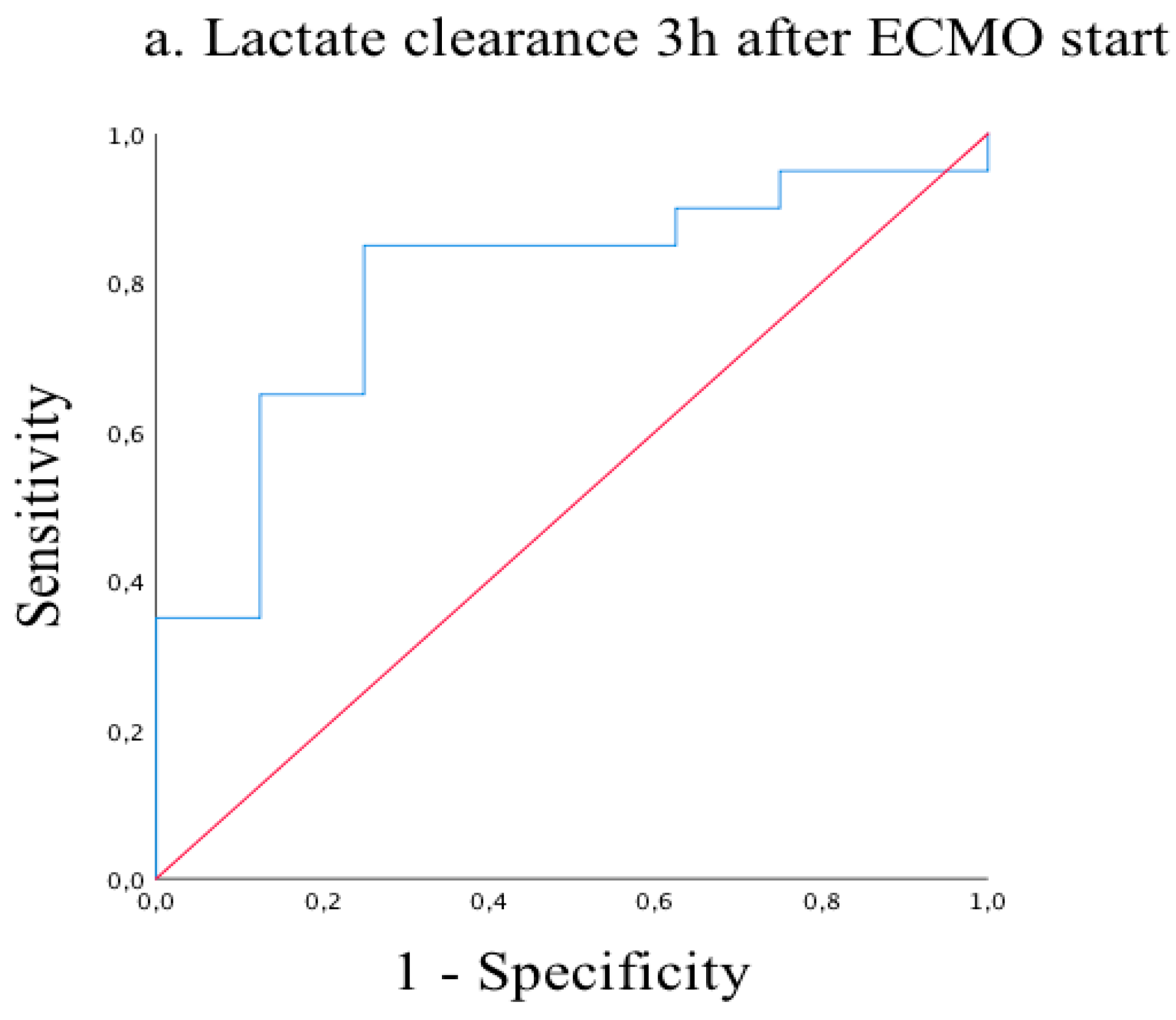
| 3 h after ECMO start | 8.5 ± 5.5 | 6.9 ± 5.0 | 10.1 ± 7.3 | 0.059 |
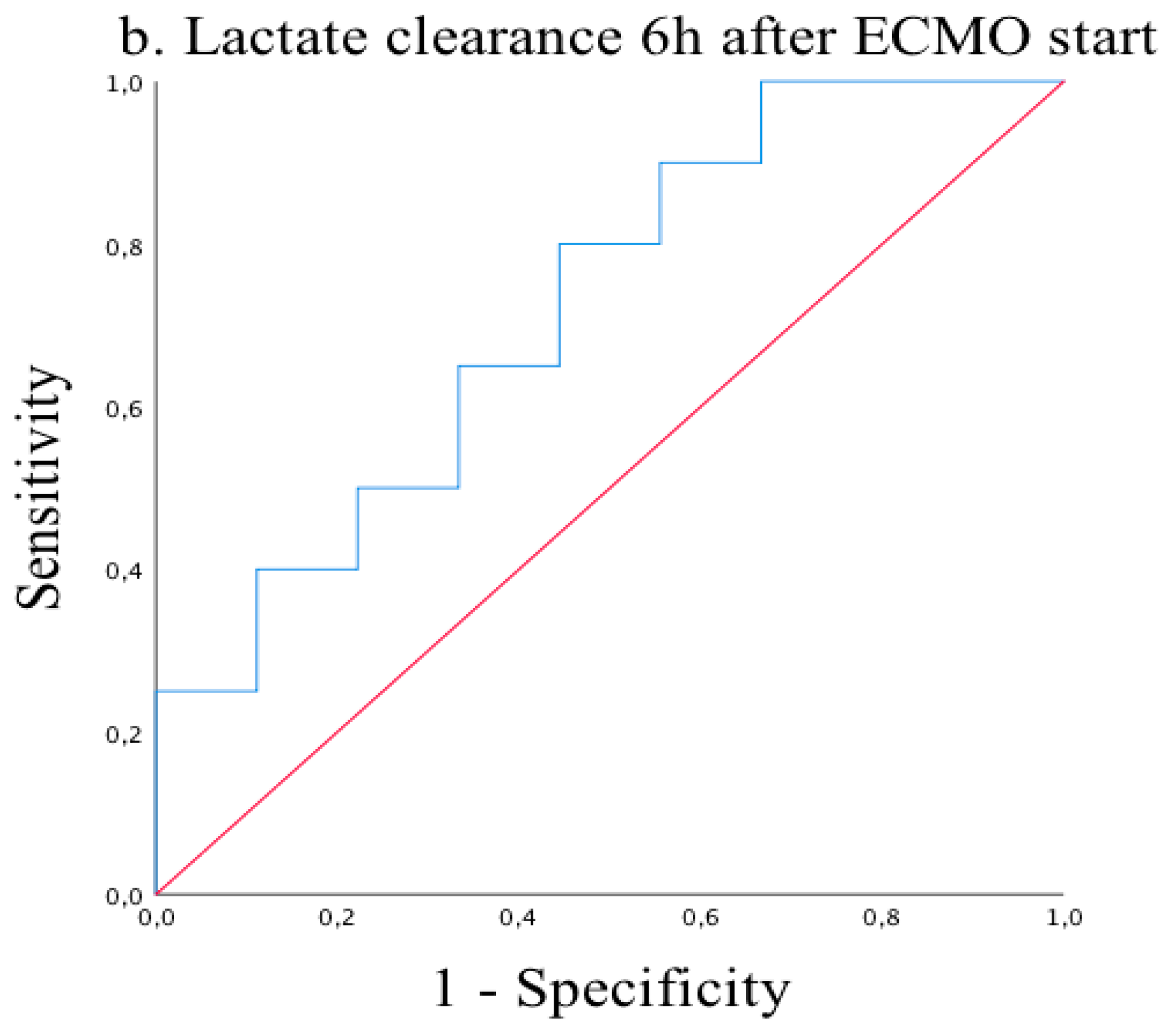
| 6 h after ECMO start | 5.3 ± 4.9 | 3.8 ± 2.7 | 6.7 ± 6.0 | 0.015 |
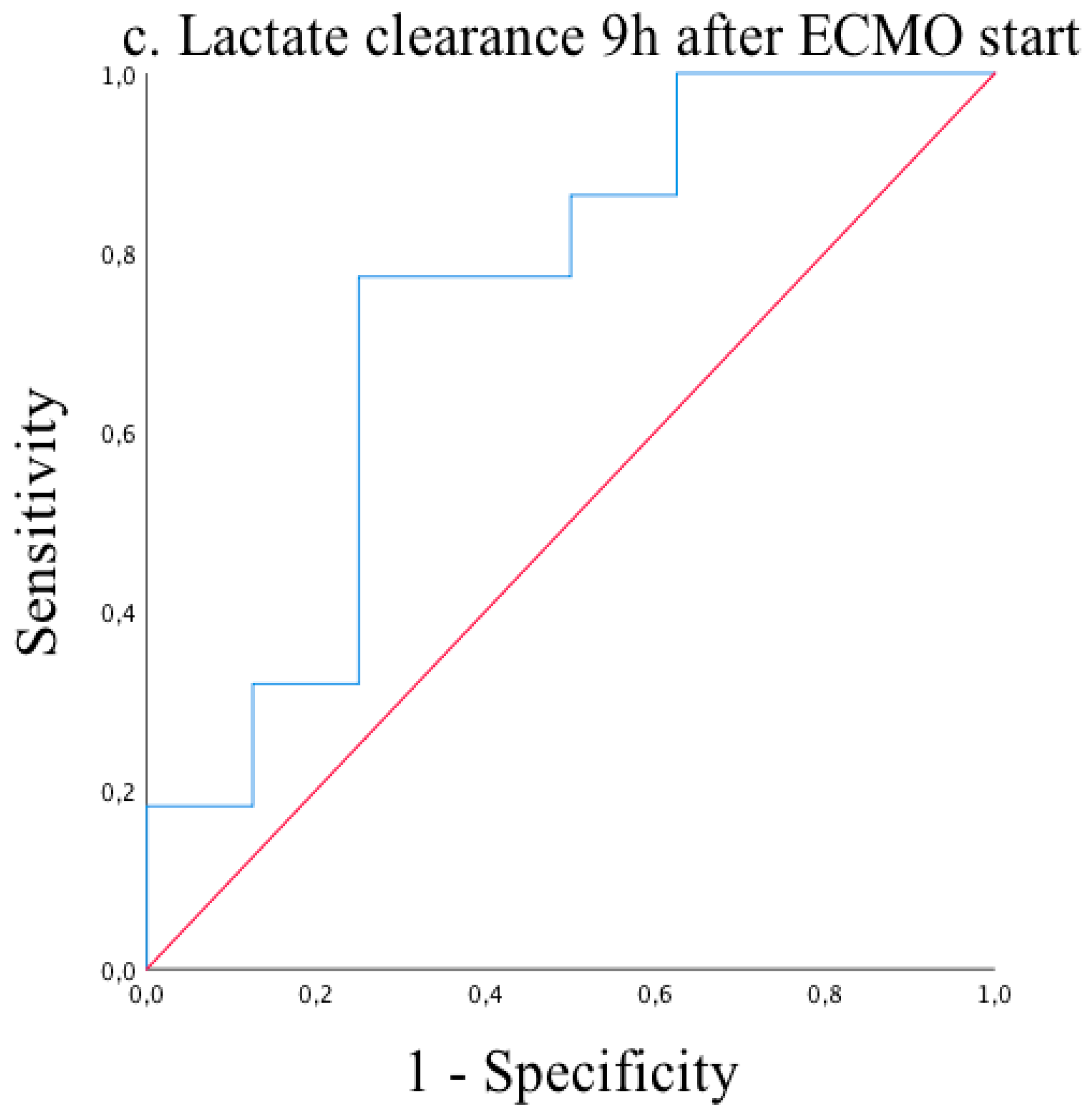
| 9 h after ECMO start | 4.2 ± 3.0 | 3.3 ± 2.0 | 4.4 ± 2.4 | 0.075 |
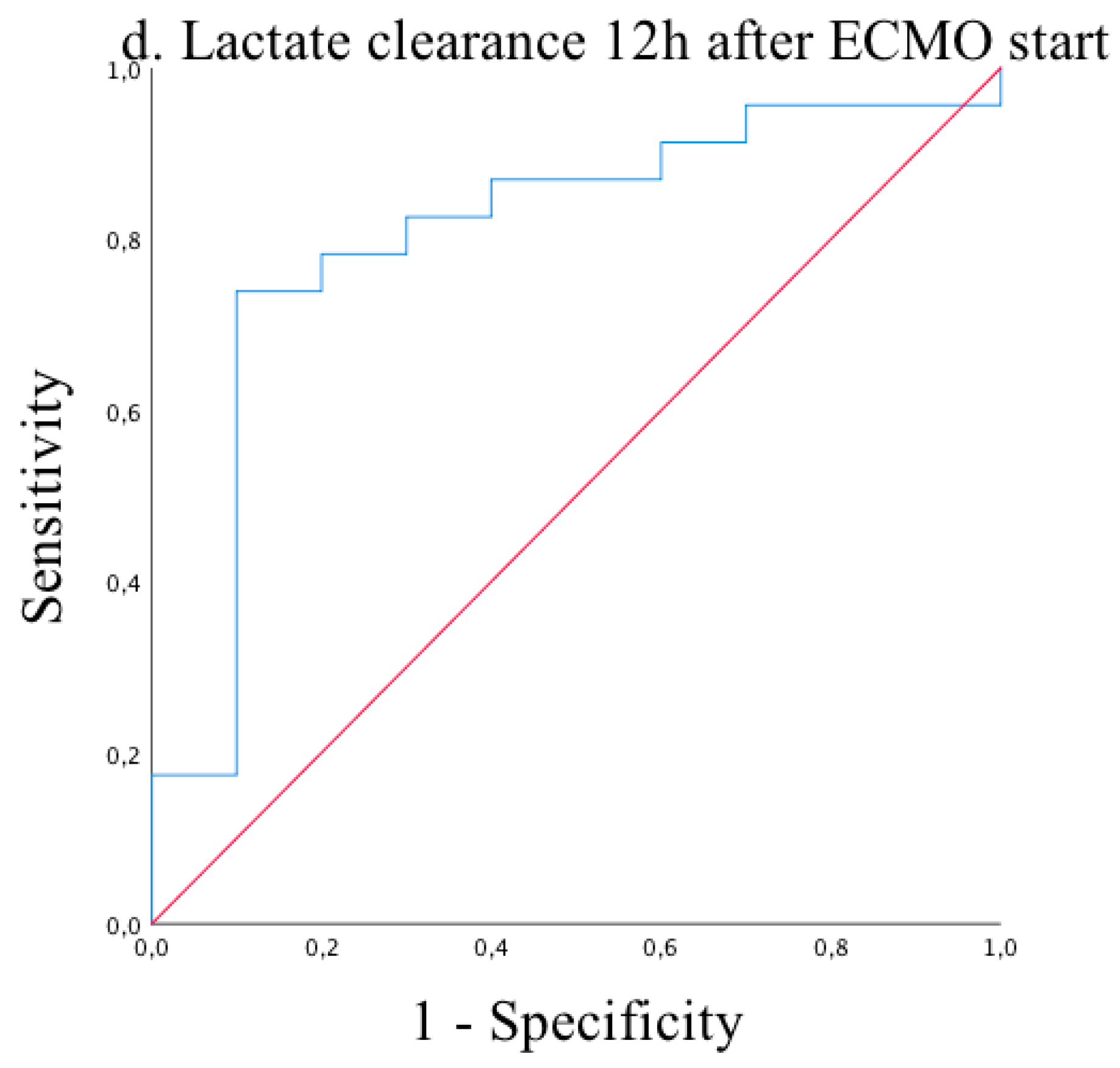
| 12 h after ECMO start | 4.1 ± 3.1 | 2.9 ± 1.5 | 4.3 ± 2.2 | 0.022 |
| ECMO duration (d) | 4(2;6) | 4(3;7) | 1.5(1;3.7) | 0.01 |
| Duration of mechanical ventilation (h) | 205(78;545) | 354(195;665) | 55(32;123) | <0.001 |
| eCPR | 16(39%) | 8(29.6%) | 8(57.1%) | 0.10 |
| pre-ECMO | 1st Day | 2nd Day | 3rd Day | |
|---|---|---|---|---|
| Creatine kinase | 0.72 | 0.25 | 0.004 | 0.001 |
| Creatine kinase MB | 0.71 | 0.01 | 0.001 | <0.001 |
| hsTnT | 0.61 | 0.007 | 0.001 | 0.002 |
| INR | 0.80 | 0.63 | 0.48 | 0.98 |
| AST (GOT) | 0.35 | 0.17 | 0.004 | 0.002 |
| ALT (GPT) | 0.49 | 0.46 | 0.057 | 0.068 |
| Bilirubine | 0.069 | 0.63 | 0.33 | 0.45 |
| Creatinine | 0.38 | 0.055 | 0.007 | 0.002 |
| Creatinine | 0.38 | 0.055 | 0.007 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merkle-Storms, J.; Djordjevic, I.; Weber, C.; Avgeridou, S.; Krasivskyi, I.; Gaisendrees, C.; Mader, N.; Kuhn-Régnier, F.; Kröner, A.; Bennink, G.; et al. Impact of Lactate Clearance on Early Outcomes in Pediatric ECMO Patients. Medicina 2021, 57, 284. https://doi.org/10.3390/medicina57030284
Merkle-Storms J, Djordjevic I, Weber C, Avgeridou S, Krasivskyi I, Gaisendrees C, Mader N, Kuhn-Régnier F, Kröner A, Bennink G, et al. Impact of Lactate Clearance on Early Outcomes in Pediatric ECMO Patients. Medicina. 2021; 57(3):284. https://doi.org/10.3390/medicina57030284
Chicago/Turabian StyleMerkle-Storms, Julia, Ilija Djordjevic, Carolyn Weber, Soi Avgeridou, Ihor Krasivskyi, Christopher Gaisendrees, Navid Mader, Ferdinand Kuhn-Régnier, Axel Kröner, Gerardus Bennink, and et al. 2021. "Impact of Lactate Clearance on Early Outcomes in Pediatric ECMO Patients" Medicina 57, no. 3: 284. https://doi.org/10.3390/medicina57030284
APA StyleMerkle-Storms, J., Djordjevic, I., Weber, C., Avgeridou, S., Krasivskyi, I., Gaisendrees, C., Mader, N., Kuhn-Régnier, F., Kröner, A., Bennink, G., Sabashnikov, A., Trieschmann, U., Wahlers, T., & Menzel, C. (2021). Impact of Lactate Clearance on Early Outcomes in Pediatric ECMO Patients. Medicina, 57(3), 284. https://doi.org/10.3390/medicina57030284