
Effects of Vitamin and Amino Acid-Enriched Hyaluronic Acid Gel on the Healing of Oral Mucosa: In Vivo and In Vitro Study

 ,
, 
 ,
, 

Abstract
1. Introduction
2. Materials and Methods
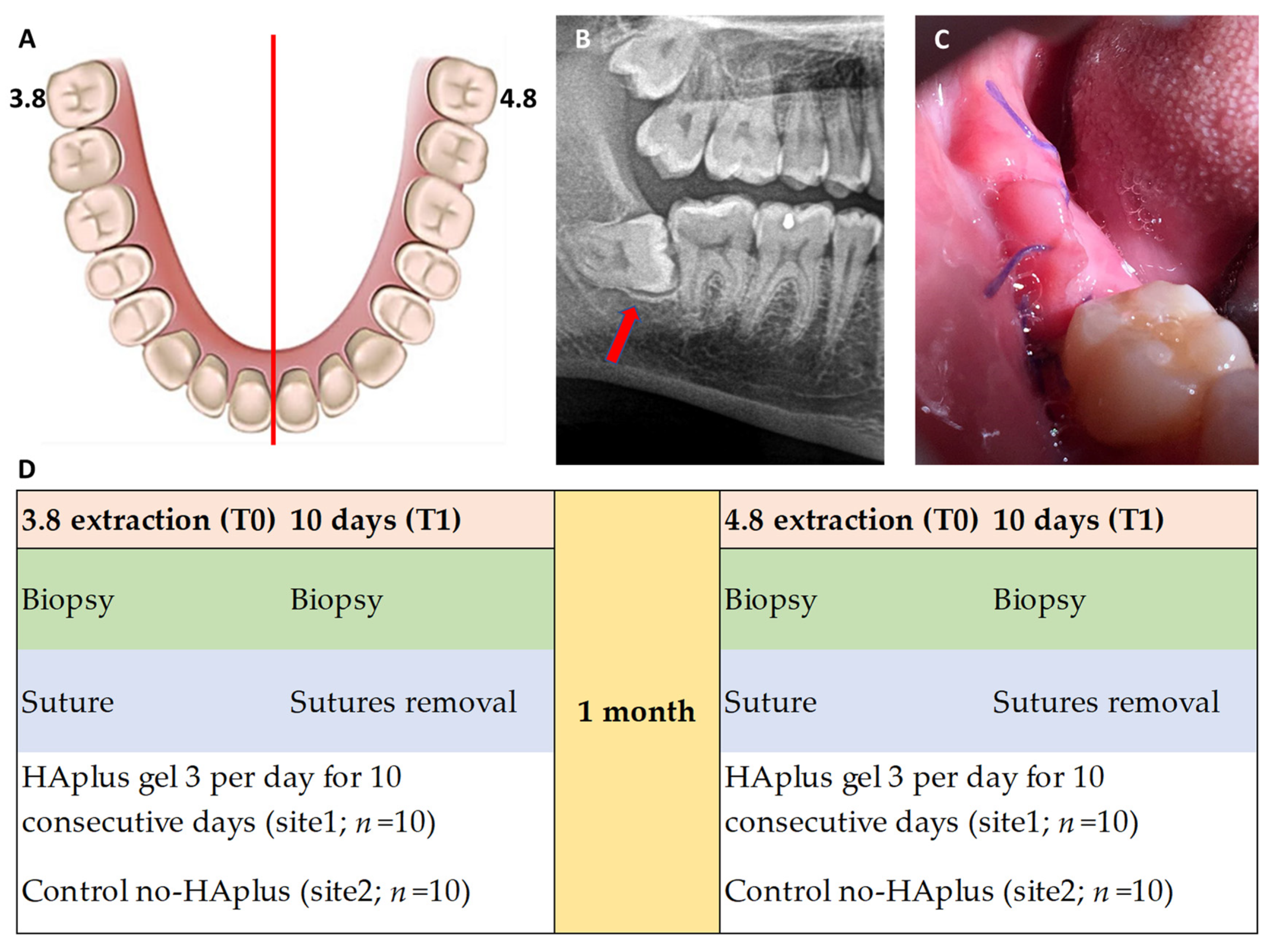
2.1. Phase I (In Vivo)
- Over 18 years old;
- Full-mouth plaque score (FMPS) and full-mouth bleeding score (FMBS) <15%.
- Systemic disease (tumors, diabetes, HIV, Hepatitis B-C);
- Smoking;
- History of keloids and diseases affecting collagen turnover;
- Pregnant or lactating women;
- History of bisphosphonate therapy;
- Periodontal and periapical disease of adjacent teeth.
- —
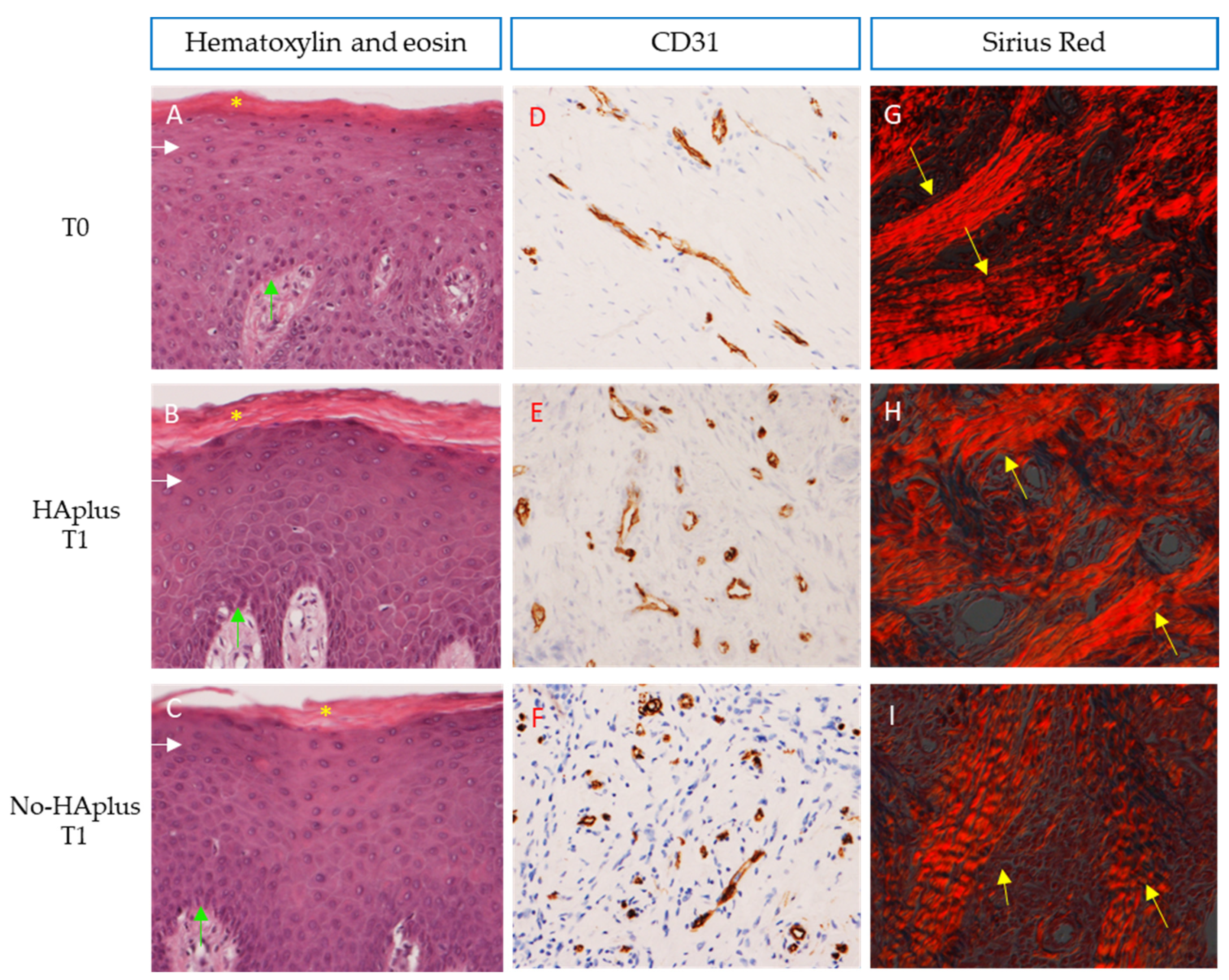
- “cell type/response”—evaluation of necrosis and inflammatory infiltrate.
- —
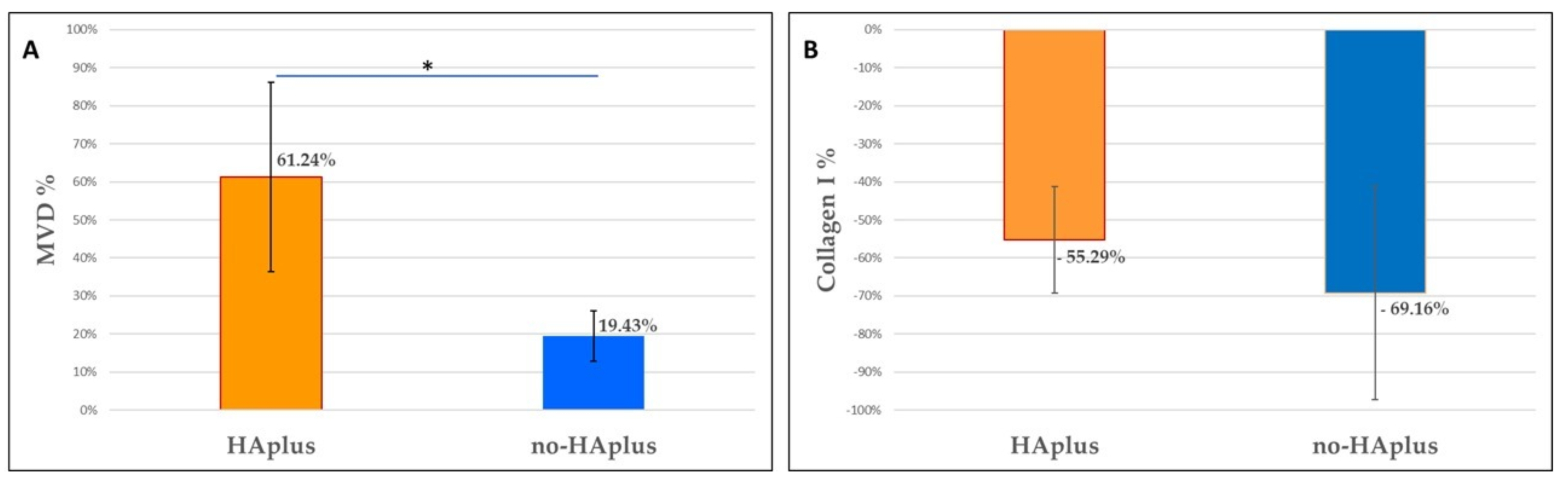
- “tissue response”—analysis of microvascular density (MVD), fibrosis and fatty infiltrate in the healing area.
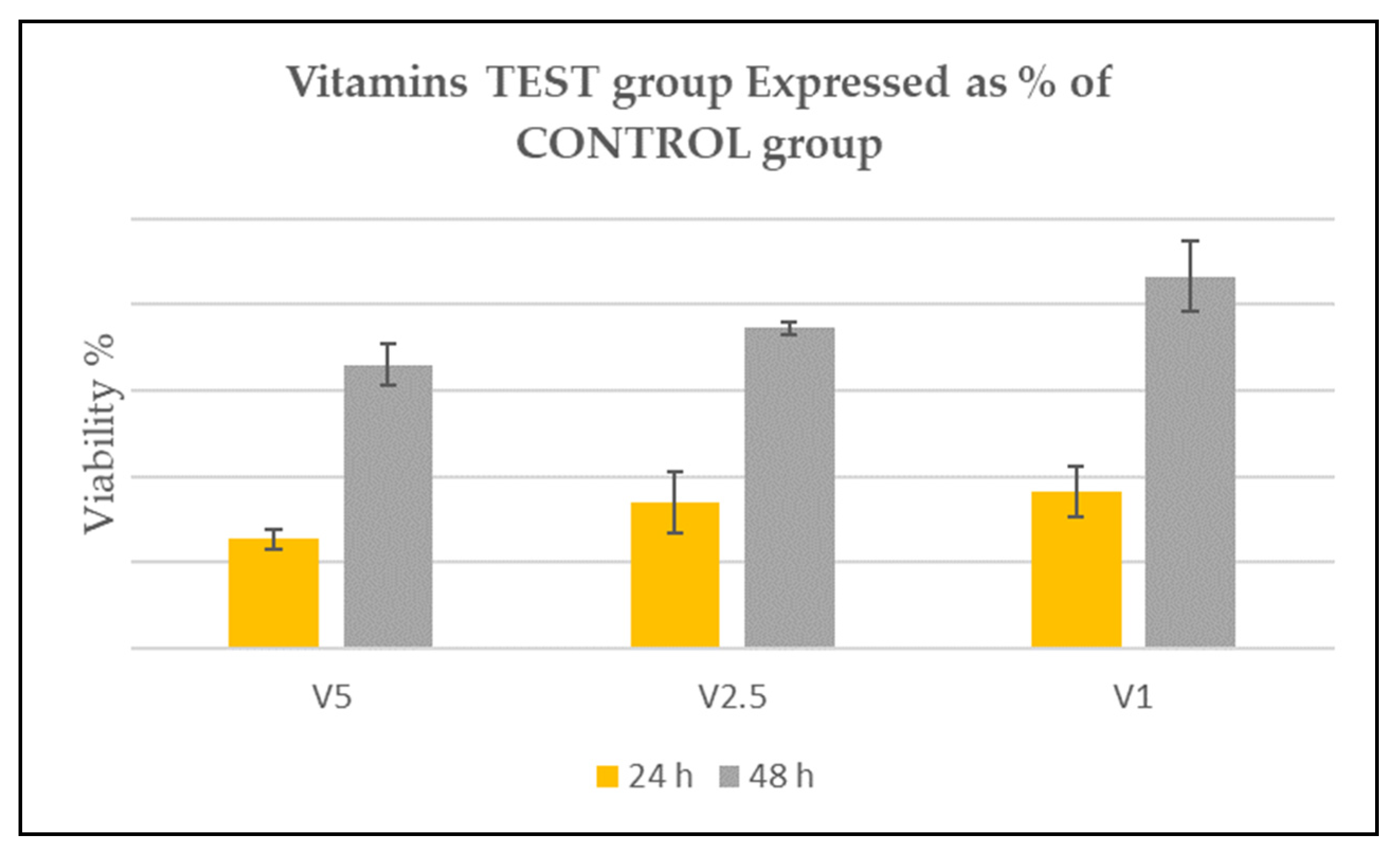
2.2. Phase II (In Vitro)
- —
- HA-VIT-1: HGF in HA medium with vitamin solution at 1%;
- —
- HA-VIT-2.5: HGF in HA medium with vitamin solution at 2.5%;
- —
- HA-VIT-5: HGF in HA medium with vitamin solution at 5%;
- —
- HA-Control: HGF in HA medium.
3. Results
3.1. Phase I (In Vivo)
3.2. Phase II (In Vitro)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, T.; Park, H.C.; Son, K.M.; Yang, H.C. Effects of dimethyloxalylglycine on wound healing of palatal mucosa in a rat model. BMC Oral Health 2015, 15, 60. [Google Scholar] [CrossRef] [PubMed]
- Okonkwo, U.A.; DiPietro, L.A. Diabetes and Wound Angiogenesis. Int. J. Mol. Sci. 2017, 18, 1419. [Google Scholar] [CrossRef] [PubMed]
- Kadota, Y.; Nishida, K.; Hashizume, K.; Nasu, Y.; Nakahara, R.; Kanazawa, T.; Ozawa, M.; Harada, R.; Machida, T.; Ozaki, T. Risk factors for surgical site infection and delayed wound healing after orthopedic surgery in rheumatoid arthritis patients. Mod. Rheumatol. 2016, 26, 68–74. [Google Scholar] [CrossRef]
- Müller, A.M.; Toepfer, A.; Harrasser, N.; Haller, B.; Walther, M.; von Eisenhart-Rothe, R.; Gemperlein, K.; Bergmann, K.; Bradaric, C.; Laugwitz, K.L.; et al. Significant prevalence of peripheral artery disease in patients with disturbed wound healing following elective foot and ankle surgery: Results from the ABI-PRIORY (ABI as a PRedictor of Impaired wound healing after ORthopedic surgerY) trial. Vasc. Med. 2020, 25, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Nazeer, J.; Singh, R.; Suri, P.; Mouneshkumar, C.D.; Bhardwaj, S.; Iqubal, M.A.; Dinesh. Evaluation of marginal bone loss around dental implants in cigarette smokers and nonsmokers. A comparative study. J. Family Med. Prim. Care 2020, 9, 729–734. [Google Scholar] [PubMed]
- Felmeden, D.C.; Blann, A.D.; Lip, G.Y. Angiogenesis: Basic pathophysiology and implications for disease. Eur. Heart J. 2003, 24, 586–603. [Google Scholar] [CrossRef]
- Della Valle, F.; Romeo, A. Esters of Hyaluronic Acid. US Pat. 1989, 4, 851. [Google Scholar]
- Kong, J.H.; Oh, E.J.; Chae, S.Y.; Lee, K.C.; Hahn, S.K. Long acting hyaluronate—Exendin 4 conjugate for the treatment of type 2 diabetes. Biomaterials 2010, 31, 4121–4128. [Google Scholar] [CrossRef] [PubMed]
- Fallacara, A.; Baldini, E.; Manfredini, S.; Vertuani, S. Hyaluronic Acid in the Third Millennium. Polymers 2018, 10, 701. [Google Scholar] [CrossRef]
- Nicole, S. Personalised Medicine: The Right Treatment for the Right Person at the Right Time. Briefing October 2015 European Parliamentary Research Service. Available online: https://www.europarl.europa.eu/RegData/etudes/BRIE/2015/569009/EPRS_BRI(2015)569009_EN.pdf (accessed on 1 September 2020).
- Di Sanzo, M.; Cipolloni, L.; Borro, M.; La Russa, R.; Santurro, A.; Scopetti, M.; Simmaco, M.; Frati, P. Clinical Applications of Personalized Medicine: A New Paradigm and Challenge. Curr. Pharm. Biotechnol. 2017, 18, 194–203. [Google Scholar] [CrossRef]
- Favia, G.; Mariggio, M.A.; Maiorano, F.; Cassano, A.; Capodiferro, S.; Ribatti, D. Accelerated wound healing of oral soft tissues and angiogenic effect induced by a pool of aminoacids combined to sodium hyaluronate (AMINOGAM). J. Biol. Regul. Homeost. Agents 2008, 22, 109–116. [Google Scholar]
- Mariggiò, M.A.; Cassano, A.; Vinella, A.; Vincenti, A.; Fumarulo, R.; Lo Muzio, L.; Maiorano, E.; Ribatti, D.; Favia, G. Enhancement of fibroblast proliferation, collagen biosynthesis and production of growth factors as a result of combining sodium hyaluronate and aminoacids. Int. J. Immunopathol. Pharmacol. 2009, 22, 485–492. [Google Scholar] [CrossRef]
- Tammi, M.I.; Day, A.J.; Turley, E.A. Hyaluronan and homeostasis: A balancing act. J. Biol. Chem. 2002, 277, 4581–4584. [Google Scholar] [CrossRef]
- Mesa, F.L.; Aneiros, J.; Cabrera, A.; Bravo, M.; Caballero, T.; Revelles, F.; del Moral, R.G.; O’Valle, F. Antiproliferative effect of topic hyaluronic acid gel. Study in gingival biopsies of patients with periodontal disease. Histol. Histopathol. 2002, 17, 747–753. [Google Scholar]
- Litwiniuk, M.; Krejner, A.; Speyrer, M.S.; Gauto, A.R.; Grzela, T. Hyaluronic Acid in Inflammation and Tissue Regeneration. Wounds 2016, 28, 78–88. [Google Scholar] [PubMed]
- Romeo, U.; Libotte, F.; Palaia, G.; Galanakis, A.; Gaimari, G.; Tenore, G.; Del Vecchio, A.; Polimeni, A. Oral soft tissue wound healing after laser surgery with or without a pool of amino acids and sodium hyaluronate: A randomized clinical study. Photomed. Laser Surg. 2014, 32, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Muripiti, V.; Brijesh, L.; Rachamalla, H.K.; Marepally, S.K.; Banerjee, R.; Patri, S.V. α-Tocopherol-ascorbic acid hybrid antioxidant based cationic amphiphile for gene delivery: Design, synthesis and transfection. Bioorg. Chem. 2019, 82, 178–191. [Google Scholar] [CrossRef]
- Buranasin, P.; Mizutani, K.; Iwasaki, K.; Pawaputanon Na Mahasarakham, C.; Kido, D.; Takeda, K.; Izumi, Y. High glucose-induced oxidative stress impairs proliferation and migration of human gingival fibroblasts. PLoS ONE 2018, 13, e0201855. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Pellegrini, G.; Allievi, C.; Trombelli, L.; Annibali, S.; Dellavia, C. Soft tissues around long-term platform switching implant restorations: A histological human evaluation. Preliminary results. J. Clin. Periodontol. 2011, 38, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Trimbos, J.B.; Mouw, R.; Ranke, G.; Trimbos, K.B.; Zwinderman, K. The Donati stitch revisited: Favorable cosmetic results in a randomized clinical trial. J. Surg. Res. 2002, 107, 131–134. [Google Scholar] [CrossRef]
- Pellegrini, G.; Rasperini, G.; Obot, G.; Farronato, D.; Dellavia, C. Soft tissue healing in alveolar socket preservation technique: Histologic evaluations. Int. J. Periodontics Restor. Dent. 2014, 34, 531–539. [Google Scholar] [CrossRef]
- Francetti, L.; Dellavia, C.; Corbella, S.; Cavalli, N.; Moscheni, C.; Canciani, E.; Gagliano, N. Morphological and Molecular Characterization of Human Gingival Tissue Overlying Multiple Oral Exostoses. Case Rep. Dent. 2019, 2019, 31263605. [Google Scholar] [CrossRef]
- Colella, G.; Vicidomini, A.; Soro, V.; Lanza, A.; Cirillo, N. Molecular insights into the effects of sodium hyaluronate preparations in keratinocytes. Clin. Exp. Dermatol. 2012, 37, 516–520. [Google Scholar] [CrossRef] [PubMed]
- Canciani, E.; Dellavia, C.; Ferreira, L.M.; Giannasi, C.; Carmagnola, D.; Carrassi, A.; Brini, A.T. Human Adipose-Derived Stem Cells on Rapid Prototyped Three-Dimensional Hydroxyapatite/Beta-Tricalcium Phosphate Scaffold. J. Craniofac. Surg. 2016, 27, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Rauff, A.; LaBelle, S.A.; Strobel, H.A.; Hoying, J.B.; Weiss, J.A. Imaging the Dynamic Interaction Between Sprouting Microvessels and the Extracellular Matrix. Front. Physiol. 2019, 10, 1011. [Google Scholar] [CrossRef] [PubMed]
- DesJardins-Park, H.E.; Mascharak, S.; Chinta, M.S.; Wan, D.C.; Longaker, M.T. The Spectrum of Scarring in Craniofacial Wound Repair. Front. Physiol. 2019, 10, 322. [Google Scholar] [CrossRef] [PubMed]
- West, D.C.; Kumar, S. Hyaluronan and angiogenesis. Biol. Hyaluronan 1989, 143, 187–201. [Google Scholar]
- Sattar, A.; Rooney, P.; Kumar, S.; Pye, D.; West, D.C.; Scott, I.; Ledger, P. Application of angiogenic oligosaccharides of hyaluronan increases blood vessel numbers in rat skin. J. Investig. Dermato. 1994, 103, 576–579. [Google Scholar] [CrossRef]
- Montesano, R.; Kumar, S.; Orci, L.; Pepper, M.S. Synergistic effect of hyaluronan oligosaccharides and vascular endothelial growth factor on angiogenesis in vitro. Lab. Investig. 1996, 75, 249–262. [Google Scholar]
- Çankaya, Z.T.; Gürbüz, S.; Bakirarar, B.; Kurtiş, B. Evaluation of the Effect of Hyaluronic Acid Application on the Vascularization of Free Gingival Graft for Both Donor and Recipient Sites with Laser Doppler Flowmetry: A Randomized, Examiner-Blinded, Controlled Clinical Trial. Int. J. Periodontics Restor. Dent. 2020, 40, 233–243. [Google Scholar] [CrossRef]
- Karna, E.; Miltyk, W.; Wołczyński, S.; Pałka, J.A. The potential mechanism for glutamine-induced collagen biosynthesis in cultured human skin fibroblasts. Comp. Biochem. Physiol. B Biochem. Mol. Biol. 2001, 130, 23–32. [Google Scholar] [CrossRef]
- Murakami, H.; Shimbo, K.; Inoue, Y.; Takino, Y.; Kobayashi, H. Importance of amino acid composition to improve skin collagen protein synthesis rates in UV-irradiated mice. Amino Acids 2012, 42, 2481–2489. [Google Scholar] [CrossRef]
- Zhang, X.J.; Chinkes, D.L.; Wolfe, R.R. Leucine supplementation has an anabolic effect on proteins in rabbit skin wound and muscle. J. Nutr. 2004, 134, 3313–3318. [Google Scholar] [CrossRef] [PubMed]
- De Paz-Lugo, P.; Lupiáñez, J.A.; Meléndez-Hevia, E. High glycine concentration increases collagen synthesis by articular chondrocytes in vitro: Acute glycine deficiency could be an important cause of osteoarthritis. Amino Acids 2018, 50, 1357–1365. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudi, S.; Mancini, E.; Xu, L.; Moore, A.; Jahanbani, F.; Hebestreit, K.; Srinivasan, R.; Li, X.; Devarajan, K.; Prélot, L.; et al. Heterogeneity in old fibroblasts is linked to variability in reprogramming and wound healing. Nature 2019, 574, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, E.; Faintuch, J.; Machado Moreira, E.A.; Gonçalves da Silva, V.R.; Lopes Pereima, M.J.; Martins Fagundes, R.L.; Filho, D.W. Supplementation of vitamin E, vitamin C, and zinc attenuates oxidative stress in burned children: A randomized, double-blind, placebo-controlled pilot study. J. Burn Care Res. 2009, 3, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Scholl, D.; Langkamp-Henken, B. Nutrient recommendations for wound healing. J. Intraven. Nurs. 2001, 24, 124–132. [Google Scholar]
- Torshabi, M.; Esfahrood, Z.R.; Jamshidi, M.; Torshizi, A.M.; Sotoudeh, S. Efficacy of vitamins E and C for reversing the cytotoxic effects of nicotine and cotinine. Eur. J. Oral. Sci. 2017, 125, 426–437. [Google Scholar] [CrossRef] [PubMed]
- Nishida, M.; Grossi, S.G.; Dunford, R.G.; Ho, A.W.; Trevisan, M.; Genco, R.J. Dietary vitamin C and the risk for periodontal disease. J. Periodontol. 2000, 71, 1215–1223. [Google Scholar] [CrossRef] [PubMed]
- Takamizawa, S.; Maehata, Y.; Imai, K.; Senoo, H.; Sato, S.; Hata, R. Effects of ascorbic acid and ascorbic acid 2-phosphate, a long-acting vitamin C derivative, on the proliferation and differentiation of human osteoblast-like cells. Cell Biol. Int. 2004, 28, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Galliera, E.; Ragone, V.; Marazzi, M.G.; Selmin, F.; Banci, L.; Corsi Romanelli, M.M. Vitamin E-stabilized UHMWPE: Biological response on human osteoblasts to wear debris. Clin. Chim. Acta 2018, 486, 18–25. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MVD | T0 | T1 | |
|---|---|---|---|
| HAplus | 7.00% ± 1% | 11.91% ± 3% | p < 0.001 |
| no-HAplus | 7.18% ± 1% | 8.62% ± 2% | p < 0.001 |
| ns | p = 0.013 |
| Collagen Content | T0 | T1 | |
|---|---|---|---|
| HAplus | 38.96% ± 5% | 18.92% ± 7% | p < 0.001 |
| no-HAplus | 40.98% ± 8% | 18.45% ± 5% | p < 0.001 |
| ns | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canciani, E.; Sirello, R.; Pellegrini, G.; Henin, D.; Perrotta, M.; Toma, M.; Khomchyna, N.; Dellavia, C. Effects of Vitamin and Amino Acid-Enriched Hyaluronic Acid Gel on the Healing of Oral Mucosa: In Vivo and In Vitro Study. Medicina 2021, 57, 285. https://doi.org/10.3390/medicina57030285
Canciani E, Sirello R, Pellegrini G, Henin D, Perrotta M, Toma M, Khomchyna N, Dellavia C. Effects of Vitamin and Amino Acid-Enriched Hyaluronic Acid Gel on the Healing of Oral Mucosa: In Vivo and In Vitro Study. Medicina. 2021; 57(3):285. https://doi.org/10.3390/medicina57030285
Chicago/Turabian StyleCanciani, Elena, Riccardo Sirello, Gaia Pellegrini, Dolaji Henin, Mariachiara Perrotta, Marilisa Toma, Nataliya Khomchyna, and Claudia Dellavia. 2021. "Effects of Vitamin and Amino Acid-Enriched Hyaluronic Acid Gel on the Healing of Oral Mucosa: In Vivo and In Vitro Study" Medicina 57, no. 3: 285. https://doi.org/10.3390/medicina57030285
APA StyleCanciani, E., Sirello, R., Pellegrini, G., Henin, D., Perrotta, M., Toma, M., Khomchyna, N., & Dellavia, C. (2021). Effects of Vitamin and Amino Acid-Enriched Hyaluronic Acid Gel on the Healing of Oral Mucosa: In Vivo and In Vitro Study. Medicina, 57(3), 285. https://doi.org/10.3390/medicina57030285