
Stand-Alone Posterior Expandable Cage Technique for Adjacent Segment Degeneration with Lumbar Spinal Canal Stenosis: A Retrospective Case Series



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
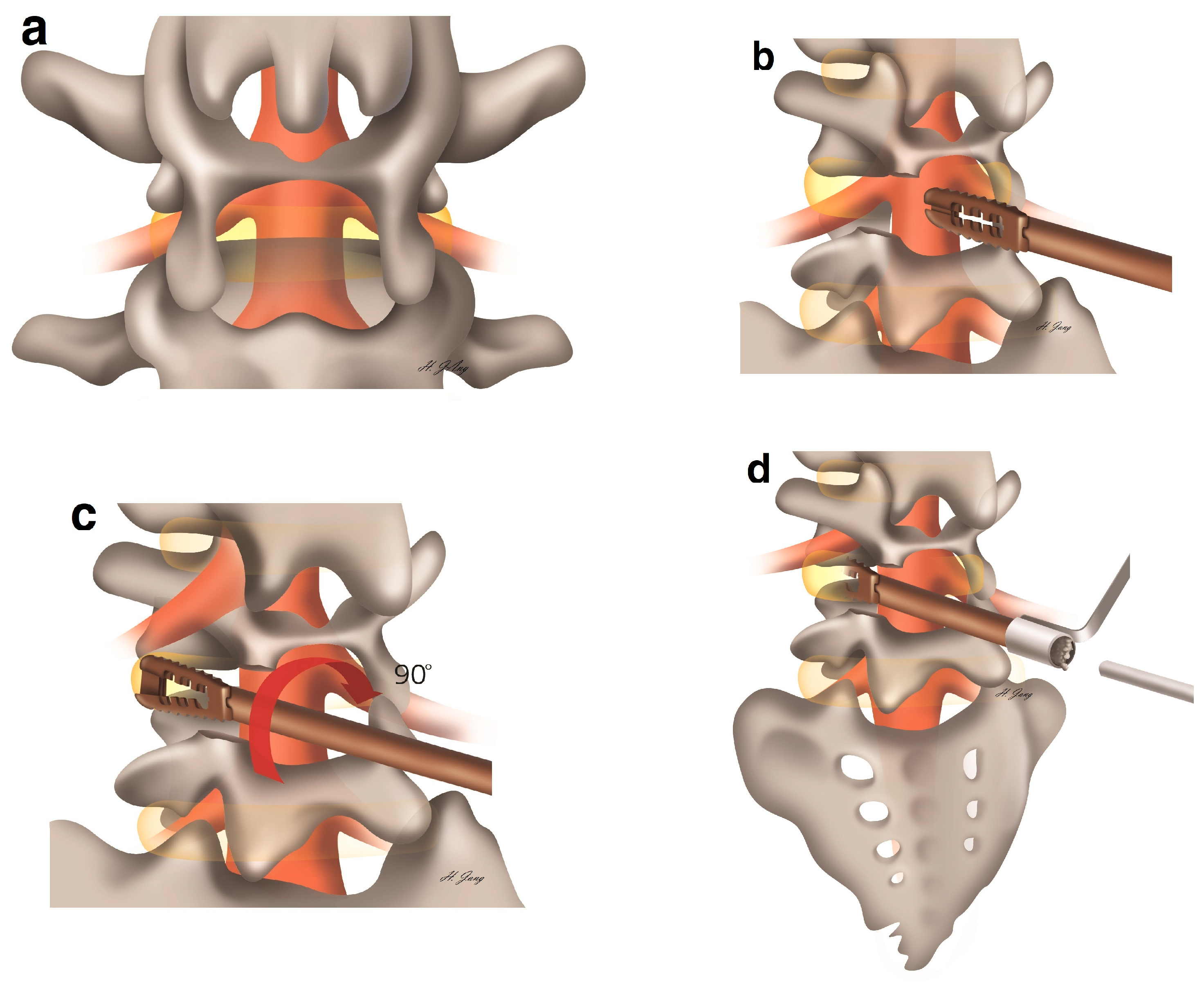
2.2. Surgical Protocol
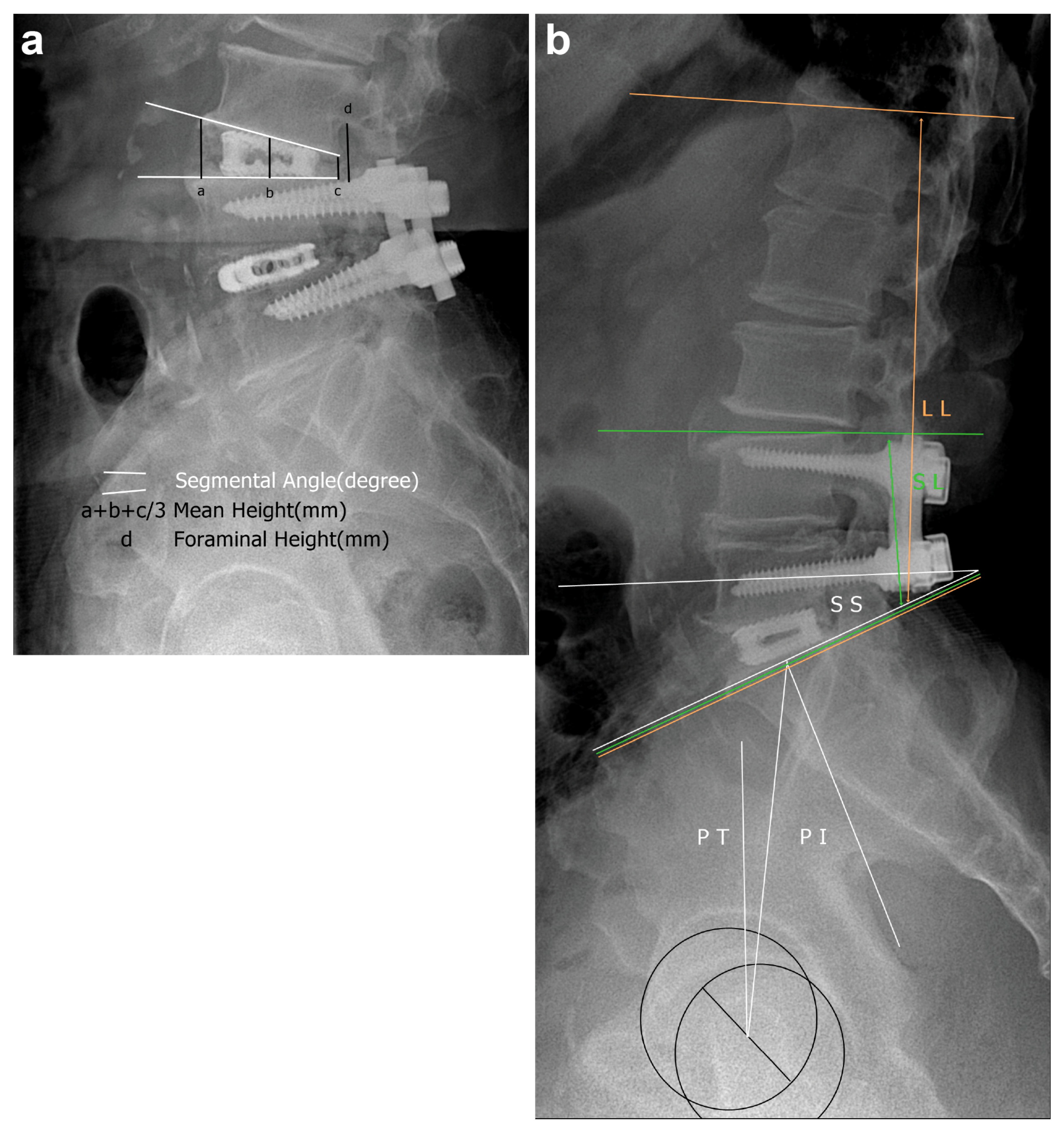
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, C.S.; Hwang, C.J.; Lee, S.W.; Ahn, Y.J.; Kim, Y.T.; Lee, D.H.; Lee, M.Y. Risk factors for adjacent segment disease after lumbar fusion. Eur. Spine J. 2009, 18, 1637–1643. [Google Scholar] [CrossRef]
- Senteler, M.; Weisse, B.; Snedeker, J.G.; Rothenfluh, D.A. Pelvic incidence-lumbar lordosis mismatch results in increased segmental joint loads in the unfused and fused lumbar spine. Eur. Spine J. 2014, 23, 1384–1393. [Google Scholar] [CrossRef]
- Park, P.; Garton, H.J.; Gala, V.C.; Hoff, J.T.; McGillicuddy, J.E. Adjacent segment disease after lumbar or lumbosacral fusion: Review of the literature. Spine 2004, 29, 1938–1944. [Google Scholar] [CrossRef]
- Louie, P.K.; Haws, B.E.; Khan, J.M.; Markowitz, J.; Movassaghi, K.; Ferguson, J.; Lopez, G.D.; An, H.S.; Phillips, F.M. Comparison of stand-alone lateral lumbar interbody fusion versus open laminectomy and posterolateral instrumented fusion in the treatment of adjacent segment disease following previous lumbar fusion surge. Spine 2009, 44, E1461–E1469. [Google Scholar] [CrossRef]
- Chen, W.J.; Lai, P.L.; Niu, C.C.; Chen, L.H.; Fu, T.S.; Wong, C.B. Surgical treatment of adjacent instability after lumbar spine fusion. Spine 2001, 26, E519–E524. [Google Scholar] [CrossRef]
- Djurasovic, M.O.; Carreon, L.Y.; Glassman, S.D.; Dimar, J.R.; Puno, R.M.; Johnson, J.R. Sagittal alignment as a risk factor for adjacent level degeneration: A case-control study. Orthopedics. 2008, 31, 546. [Google Scholar] [CrossRef]
- Barrett-Tuck, R.; Del Monaco, D.; Block, J.E. One and two level posterior lumbar interbody fusion (PLIF) using an expandable, stand-alone, interbody fusion device: A VariLift® case series. J. Spine Surg. 2017, 3, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Park, H.C.; Yoon, S.H.; Oh, S.H.; Roh, S.W.; Rim, D.C.; Kim, T.S. A multi-center clinical study of posterior lumbar interbody fusion with the expandable stand-alone cage (Tyche® cage) for degenerative lumbar spinal disorders. J. Korean Neurosurg. Soc. 2007, 42, 251–257. [Google Scholar] [CrossRef]
- Neely, W.F.; Fichtel, F.; Del Monaco, D.C.; Block, J.E. Treatment of symptomatic lumbar disc degeneration with the VariLift-L interbody fusion system: Retrospective review of 470 cases. Int. J. Spine Surg. 2016, 10, 15. [Google Scholar] [CrossRef]
- Levin, D.A.; Hale, J.J.; Bendo, J.A. Adjacent segment degeneration following spinal fusion for degenerative disc disease. Bull. NYU Hosp. Jt. Dis. 2007, 65, 29–36. [Google Scholar]
- Le Huec, J.C.; Faundez, A.; Dominguez, D.; Hoffmeyer, P.; Aunoble, S. Evidence showing the relationship between sagittal balance and clinical outcomes in surgical treatment of degenerative spinal diseases: A literature review. Int. Orthop. 2015, 39, 87–95. [Google Scholar] [CrossRef]
- Cho, S.K.; Bridwell, K.H.; Lenke, L.G.; Yi, J.S.; Pahys, J.M.; Zebala, L.P.; Kang, M.M.; Cho, W.; Baldus, C.R. Major complications in revision adult deformity surgery: Risk factors and clinical outcomes with 2- to 7-year follow-up. Spine 2012, 37, 489–500. [Google Scholar] [CrossRef]
- Zhu, G.; Hao, Y.; Yu, L.; Cai, Y.; Yang, X. Comparing stand-alone oblique lumbar interbody fusion with posterior lumbar interbody fusion for revision of rostral adjacent segment disease: A STROBE-compliant study. Medicine 2018, 97, e12680. [Google Scholar] [CrossRef]
- Chiu, J.C.; Clifford, T.; Princenthal, R.; Shaw, S. Junctional disc herniation syndrome in post spinal fusion treated with endoscopic spine surgery. Surg. Technol. Int. 2005, 14, 305–315. [Google Scholar]
- Yen, C.P.; Mosley, Y.I.; Uribe, J.S. Role of minimally invasive surgery for adult spinal deformity in preventing complications. Curr. Rev. Musculoskelet Med. 2016, 9, 309–315. [Google Scholar] [CrossRef]
- Radcliff, K.; Curry, P.; Hilibrand, A.; Kepler, C.; Lurie, J.; Zhao, W.; Albert, T.; Weinstein, J. Risk for adjacent segment and same segment reoperation after surgery for lumbar stenosis: A subgroup analysis of the Spine Patient Outcomes Research Trial (SPORT). Spine 2013, 38, 531–539. [Google Scholar] [CrossRef]
- Lu, K.; Liliang, P.C.; Wang, H.K.; Liang, C.L.; Chen, J.S.; Chen, T.B.; Wang, K.W.; Chen, H.J. Reduction in adjacent-segment degeneration after multilevel posterior lumbar interbody fusion with proximal DIAM implantation. J. Neurosurg. Spine 2015, 23, 190–196. [Google Scholar] [CrossRef]
- Lequin, M.B.; Verbaan, D.; Bouma, G.J. Posterior lumbar interbody fusion with stand-alone trabecular metal cages for repeatedly recurrent lumbar disc herniation and back pain. J. Neurosurg. Spine 2014, 20, 617–622. [Google Scholar] [CrossRef]
- Huang, K.F.; Chen, T.Y. Clinical results of a single central interbody fusion cage and transpedicle screws fixation for recurrent herniated lumbar disc and low-grade spondylolisthesis. Chang Gung Med. J. 2003, 26, 170–177. [Google Scholar]
- Tsai, T.T.; Lee, S.H.; Niu, C.C.; Lai, P.L.; Chen, L.H.; Chen, W.J. Unplanned revision spinal surgery within a week: A retrospective analysis of surgical causes. BMC Musculoskelet Disord. 2016, 17, 28. [Google Scholar] [CrossRef]
- Yao, Y.; Zhang, H.; Wu, J.; Liu, H.; Zhang, Z.; Tang, Y.; Zhou, Y. Comparison of three minimally invasive spine surgery methods for revision surgery for recurrent herniation after percutaneous endoscopic lumbar discectomy. World Neurosurg. 2017, 100, 641–647. [Google Scholar] [CrossRef]
- Barsa, P.; Suchomel, P. Factors affecting sagittal malalignment due to cage subsidence in standalone cage assisted anterior cervical fusion. Eur. Spine J. 2007, 16, 1395–1400. [Google Scholar] [CrossRef]
- Niu, C.C.; Liao, J.C.; Chen, W.J.; Chen, L.H. Outcomes of interbody fusion cages used in 1 and 2-levels anterior cervical discectomy and fusion: Titanium cages versus polyetheretherketone (PEEK) cages. J. Spinal Disord. Technol. 2010, 23, 310–316. [Google Scholar] [CrossRef]
- Böker, D.K.; Schultheiss, R.; van Roost, D.; Osborn, J.F.; Kaden, B. Anterior cervical discectomy and vertebral interbody fusion with hydroxy-apatite ceramic. Preliminary results. Acta Neurochir. 1993, 121, 191–195. [Google Scholar] [CrossRef]
- McGilvray, K.C.; Easley, J.; Seim, H.B.; Regan, D.; Berven, S.H.; Hsu, W.K.; Mroz, T.E.; Puttlitz, C.M. Bony ingrowth potential of 3D-printed porous titanium alloy: A direct comparison of interbody cage materials in an in vivo ovine lumbar fusion model. Spine J. 2018, 18, 1250–1260. [Google Scholar] [CrossRef]
- Kerezoudis, P.; Rinaldo, L.; Drazin, D.; Kallmes, D.; Krauss, W.; Hassoon, A.; Bydon, M. Association between vitamin D deficiency and outcomes following spinal fusion surgery: A systematic review. World Neurosurg. 2016, 95, 71–76. [Google Scholar] [CrossRef]
- Cho, P.G.; Ji, G.Y.; Shin, D.A.; Ha, Y.; Yoon, D.H.; Kim, K.N. An effect comparison of teriparatide and bisphosphonate on posterior lumbar interbody fusion in patients with osteoporosis: A prospective cohort study and preliminary data. Eur. Spine J. 2017, 26, 691–697. [Google Scholar] [CrossRef]
- Ide, M.; Yamada, K.; Kaneko, K.; Sekiya, T.; Kanai, K.; Higashi, T.; Saito, T. Combined teriparatide and denosumab therapy accelerates spinal fusion following posterior lumbar interbody fusion. Orthop. Traumatol. Surg. Res. 2018, 104, 1043–1048. [Google Scholar] [CrossRef]
- Suchomel, P.; Barsa, P.; Buchvald, P.; Svobodnik, A.; Vanickova, E. Autologous versus allogenic bone grafts in instrumented anterior cervical discectomy and fusion: A prospective study with respect to bone union pattern. Eur. Spine J. 2004, 13, 510–515. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Value |
|---|---|
| Female sex, n (%) | 12 (63.16) |
| Age (years), mean ± SD | 67.13 ± 9.31 |
| Symptoms, n (%) | |
| Sensory | 4 (21.05) |
| Sensorimotor | 11 (57.89) |
| Bladder and bowel | 4 (21.05) |
| ASA-PS grade, n (%) | |
| I | 3 (15.79) |
| II | 15 (78.95) |
| III | 1 (5.26) |
| Initial operation, n (%) | |
| PLF | 4 (21.05) |
| PLIF | 9 (47.37) |
| Stand-alone cages | 5 (26.32) |
| PVP | 1 (5.26) |
| Involved levels, n (%) | |
| 1 | 13 (68.42) |
| 2 | 5 (26.31) |
| 3 | 1 (5.26) |
| Duration of ASD (years), mean ± SD | 8.26 ± 4.04 |
| Follow-up duration (years), mean ± SD | 7.61 ± 2.03 |
| Inclusion of sacrum level, n (%) | 1 (5.26) |
| Pfirrmann disc degeneration grade at the ASD level, n (%) | |
| 4 | 6 (31.58) |
| 5 | 13 (68.42) |
| Variables | Preoperative | After 1-Year Follow-Up | p-Value | Final Follow-Up | p-Value | |
|---|---|---|---|---|---|---|
| Local factors | Anterior disc height at the ASD level (mm), mean | 7.38 | 14.51 | <0.01 †* | 13.36 | <0.01 †* |
| Middle disc height at the ASD level (mm), mean | 6.01 | 11.93 | <0.01 †* | 11.22 | <0.01 †* | |
| Posterior disc height at the ASD level (mm), mean | 5.01 | 9.45 | <0.01 †* | 8.87 | <0.01 †* | |
| Foraminal height at the ASD level (mm), mean | 14.22 | 18.57 | <0.01 †* | 17.99 | 0.01 †* | |
| Segmental angle at the ASD level (°), mean | 2.40 | 7.86 | 0.03 †* | 6.53 | 0.10 † | |
| Lumbar factors | Short lumbar lordosis (°), mean | 11.64 | 18.36 | 0.08 † | 17.34 | 0.14 † |
| Whole lumbar lordosis (°), mean | 27.12 | 30.36 | 0.55 † | 29.80 | 0.62 † | |
| Sacropelvic profiles | Pelvic incidence (°), mean | 47.40 | 49.78 | 0.47 † | 49.75 | 0.48 † |
| Pelvic tilt (°), mean | 23.23 | 26.38 | 0.33 † | 25.71 | 0.45 ‡ | |
| Sacral slope (°), mean | 24.13 | 23.97 | 0.94 † | 23.56 | 0.79 † | |
| C7 plumb line (cm), mean | 4.94 | 4.00 | 0.97 † | 4.21 | 0.80 † | |
| Variables | Preoperative | 1-Year Follow-Up | p-Value | Final Follow-Up | p-Value |
|---|---|---|---|---|---|
| Pain (VAS, mean) | 6.78 | 2.26 | <0.01 †* | 2.12 | <0.01 †* |
| Disability (ODI, mean) | 28.89 | 11.96 | <0.01 †* | 11.26 | <0.01 †* |
| Bone fusion grade | Grade 1, 2 (achieved fusion, n (%)) | 16 (84.21) | |||
| Grade 3 (non-union, n (%)) | 2 (10.52) | ||||
| Grade 4 (pseudoarthrosis, n (%)) | 1 (5.26) | ||||
| Early complication rate | Total | 2 (10.52) | |||
| Incidental dura tear | 1 (5.26) | ||||
| Wound dehiscence | 1 (5.26) | ||||
| Implant problems | Total | 8 (42.10) | |||
| Retropulsion (n), (%) | 3 (15.79) | ||||
| Subsidence (n), (%) | 4 (21.05) | ||||
| Pseudoarthrosis (n), (%) | 1 (5.26) | ||||
| Cage breakage (n), (%) | 1 (5.26) | ||||
| Adjacent segment degeneration (n), (%) | 3 (15.79) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, W.-J.; Kim, S.-K.; Alaraj, M.; Kim, H.-S.; Lee, S.-C. Stand-Alone Posterior Expandable Cage Technique for Adjacent Segment Degeneration with Lumbar Spinal Canal Stenosis: A Retrospective Case Series. Medicina 2021, 57, 237. https://doi.org/10.3390/medicina57030237
Choi W-J, Kim S-K, Alaraj M, Kim H-S, Lee S-C. Stand-Alone Posterior Expandable Cage Technique for Adjacent Segment Degeneration with Lumbar Spinal Canal Stenosis: A Retrospective Case Series. Medicina. 2021; 57(3):237. https://doi.org/10.3390/medicina57030237
Chicago/Turabian StyleChoi, Woo-Jin, Seung-Kook Kim, Manhal Alaraj, Hyeun-Sung Kim, and Su-Chan Lee. 2021. "Stand-Alone Posterior Expandable Cage Technique for Adjacent Segment Degeneration with Lumbar Spinal Canal Stenosis: A Retrospective Case Series" Medicina 57, no. 3: 237. https://doi.org/10.3390/medicina57030237
APA StyleChoi, W.-J., Kim, S.-K., Alaraj, M., Kim, H.-S., & Lee, S.-C. (2021). Stand-Alone Posterior Expandable Cage Technique for Adjacent Segment Degeneration with Lumbar Spinal Canal Stenosis: A Retrospective Case Series. Medicina, 57(3), 237. https://doi.org/10.3390/medicina57030237