
Outcome Reporting Bias in COVID-19 mRNA Vaccine Clinical Trials


Abstract
1. Introduction
“There may be much more complexity to the ‘95% effective’ announcement than meets the eye—or perhaps not. Only full transparency and rigorous scrutiny of the data will allow for informed decision making. The data must be made public.”
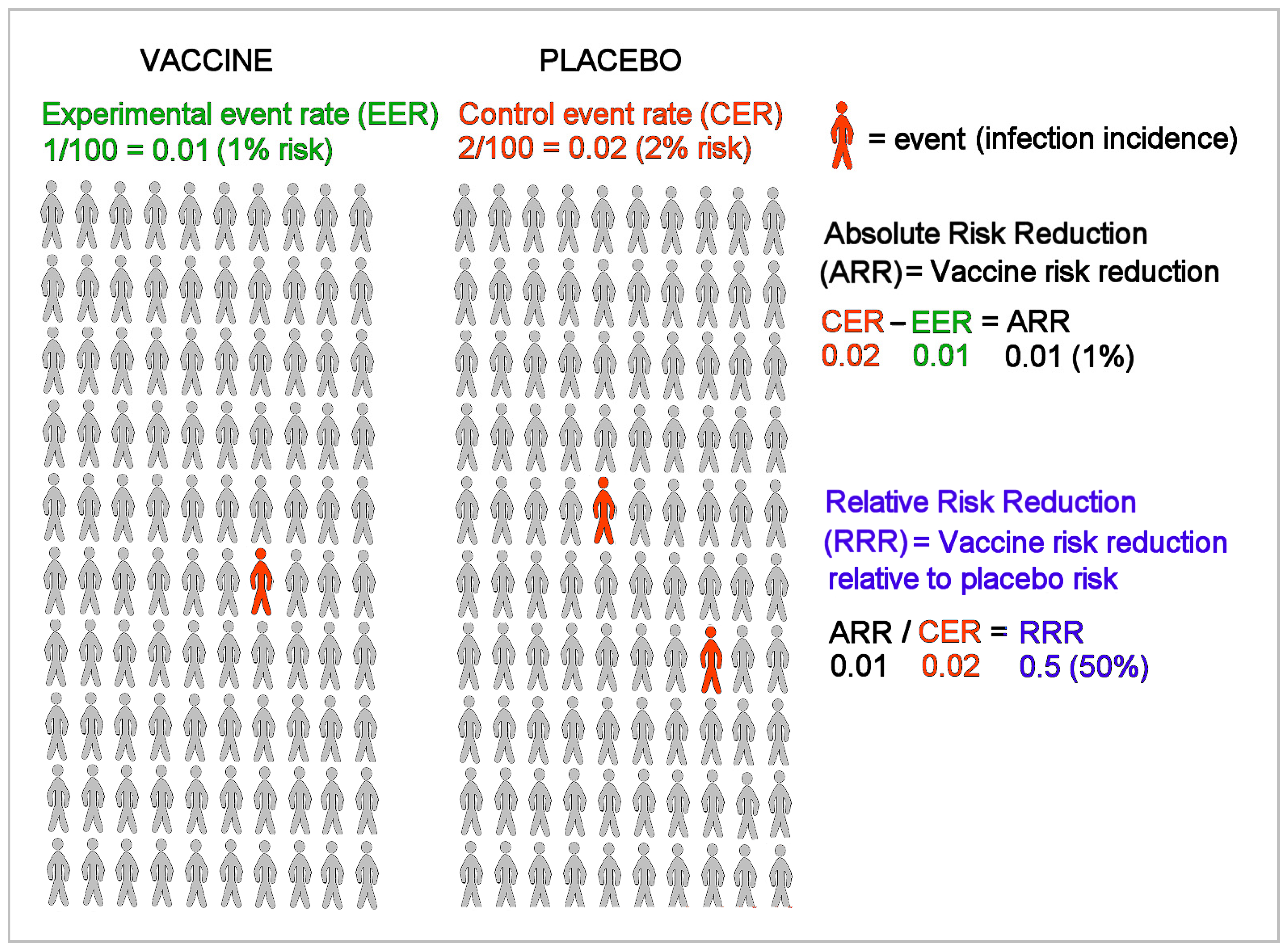
“Provide absolute risks, not just relative risks. Patients are unduly influenced when risk information is presented using a relative risk approach; this can result in suboptimal decisions. Thus, an absolute risk format should be used.”
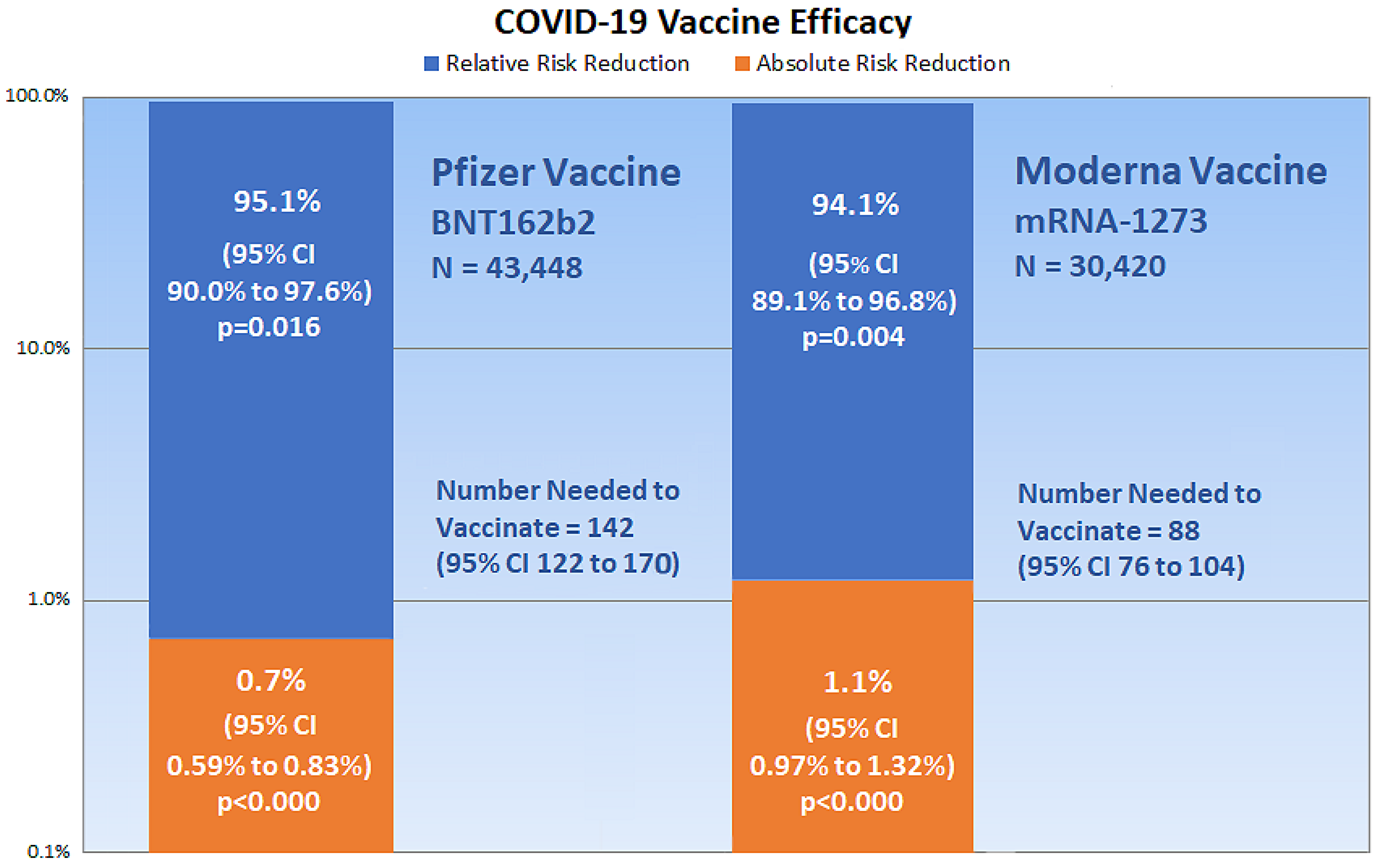
2. Critical Appraisal of Vaccine Efficacy
3. 2 × 2 Contingency Tables and Epidemiologic Equations
4. Discussion
“…critical appraisal knowledge and skills are limited among physicians,” and “use of relative effect measures was associated with greater perceptions of medication effectiveness and intent to prescribe, compared with the use of absolute effect measures.”[29]
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kwon, D. The Promise of mRNA Vaccines. Available online: https://www.the-scientist.com/news-opinion/the-promise-of-mrna-vaccines-68202 (accessed on 23 December 2020).
- Genome. Messenger RNA (mRNA). Available online: https://www.genome.gov/genetics-glossary/messenger-rna (accessed on 23 December 2020).
- Garde, D. The Story of mRNA: How a Once-Dismissed Idea Became a Leading Technology in the Covid Vaccine Race. Available online: https://www.statnews.com/2020/11/10/the-story-of-mrna-how-a-once-dismissed-idea-became-a-leading-technology-in-the-covid-vaccine-race/ (accessed on 5 January 2021).
- Centers for Disease Control and Prevention. Understanding mRNA COVID-19 Vaccines. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/mrna.html (accessed on 22 December 2020).
- Wadhwa, A.; Aljabbari, A.; Lokras, A.; Foged, C.; Thakur, A. Opportunities and Challenges in the Delivery of mRNA-based Vaccines. Pharmaceutics 2020, 12, 102. [Google Scholar] [CrossRef] [PubMed]
- Reichmuth, A.M.; Oberli, M.A.; Jaklenec, A.; Langer, R.; Blankschtein, D. mRNA vaccine delivery using lipid nanoparticles. Ther. Deliv. 2016, 7, 319–334. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. Pfizer-BioNTech COVID-19 Vaccine VRBPAC Briefing Document. Available online: https://www.fda.gov/media/144246/download (accessed on 23 December 2020).
- Food and Drug Administration. FDA Briefing Document: Moderna COVID-19 Vaccine. Available online: https://www.fda.gov/media/144434/download (accessed on 23 December 2020).
- Doshi, P. Peter Doshi: Pfizer and Moderna’s ”95% effective” Vaccines—Let’s Be Cautious and First See the Full Data. Available online: https://blogs.bmj.com/bmj/2020/11/26/peter-doshi-pfizer-and-modernas-95-effective-vaccines-lets-be-cautious-and-first-see-the-full-data/ (accessed on 23 December 2020).
- Food and Drug Administration. Roster of the Vaccines and Related Biological Products Advisory Committee. Available online: https://www.fda.gov/advisory-committees/vaccines-and-related-biological-products-advisory-committee/roster-vaccines-and-related-biological-products-advisory-committee (accessed on 23 December 2020).
- Fischhoff, B.; Brewer, N.; Downs, J. Communicating Risks and Benefits: An Evidence-Based User’s Guide; Food and Drug Administration (FDA), US Department of Health and Human Services: Silver Spring, MA, USA, 2011.
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C. Safety and efficacy of the BNT162b2 mRNA covid-19 vaccine. N. Engl. J. Med. 2020, 383. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2020, 384. [Google Scholar] [CrossRef]
- Sackett, D.L. Clinical epidemiology. Am. J. Epidemiol. 1969, 89, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Sackett, D.; Straus, S.; Scott Richardson, W.; Rosenberg, W.; Haynes, R. Evidence-Based Medicine: How to Practice and Teach EBM, 2nd ed.; Churchill Livingstone: Edinburgh, UK; London, UK, 2000. [Google Scholar]
- Cook, R.J.; Sackett, D.L. The number needed to treat: A clinically useful measure of treatment effect. BMJ 1995, 310, 452–454. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, S. A Review of Vaccine Efficacy Measures. Vaccin Res. Open J. 2019, 1, 61–64. [Google Scholar]
- Irwig, L.; Irwig, J.; Revena, L.; Sweet, M. Relative risk, relative and absolute risk reduction, number needed to treat and confidence intervals. In Smart Health Choices: Making Sense of Health Advice; Hammersmith Press: London, UK, 2008; Chapter 18. [Google Scholar]
- Kremer, L.; Moyer, V. Tips and tricks for understanding and using SR results—No 1: Relative risk, risk difference, and number needed to treat. Evidence-Based Child Health Cochrane Rev. J. 2009, 4, 1146–1148. [Google Scholar] [CrossRef]
- Sullivan, L. Confidence Intervals for the Risk Ratio (Relative Risk). Available online: https://sphweb.bumc.bu.edu/otlt/mph-modules/bs/bs704_confidence_intervals/bs704_confidence_intervals8.html#:~:text=Therefore%2C%20computing%20the%20confidence%20interval,confidence%20interval%20for%20the%20RR (accessed on 26 December 2020).
- Morris, J.A.; Gardner, M.J. Calculating Confidence Intervals For Relative Risks (Odds Ratios) And Standardised Ratios And Rates. BMJ 1988, 296, 1313–1316. [Google Scholar] [CrossRef] [PubMed]
- Schechtman, E. Odds ratio, relative risk, absolute risk reduction, and the number needed to treat—Which of these should we use? Value Health 2002, 5, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G.; Bland, J.M. How to obtain the P value from a confidence interval. BMJ 2011, 343, d2304. [Google Scholar] [CrossRef] [PubMed]
- Azzopardi, D. Group Comparison Calculator. Available online: https://www.neoweb.org.uk/Additions/compare.htm (accessed on 6 January 2021).
- Heidel, E. Epidemiology. Available online: https://www.scalestatistics.com/epidemiology.html (accessed on 6 January 2021).
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E. Safety and Efficacy of the ChAdOx1 nCoV-19 Vaccine (AZD1222) against SARS-CoV-2: An Interim Analysis of Four Randomised Controlled Trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Sadoff, J.; Le Gars, M.; Shukarev, G.; Heerwegh, D.; Truyers, C.; de Groot, A.M.; Stoop, J.; Tete, S.; Van Damme, W.; Leroux-Roels, I. Interim Results of a Phase 1–2a Trial of Ad26. COV2. S Covid-19 Vaccine. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Elliott, M.H.; Skydel, J.J.; Dhruva, S.S.; Ross, J.S.; Wallach, J.D. Characteristics and Reporting of Number Needed to Treat, Number Needed to Harm, and Absolute Risk Reduction in Controlled Clinical Trials, 2001–2019. JAMA Intern. Med. 2020, 181. [Google Scholar]
- Kahwati, L.; Carmody, D.; Berkman, N.; Sullivan, H.W.; Aikin, K.J.; DeFrank, J. Prescribers’ Knowledge and Skills for Interpreting Research Results: A Systematic Review. J. Contin. Educ. Health Prof. 2017, 37, 129–136. [Google Scholar] [CrossRef]
- Thomas, E.T.; Heneghan, C. Outcome Reporting Bias. Available online: https://catalogofbias.org/biases/outcome-reporting-bias/ (accessed on 23 November 2020).
- Shah, P.; Thornton, I.; Turrin, D.; Hipskind, J.E. Informed Consent. Available online: https://www.ncbi.nlm.nih.gov/books/NBK430827/#:~:text=Informed%20consent%20is%20the%20process,undergo%20the%20procedure%20or%20intervention (accessed on 8 February 2021).
- Demicheli, V.; Jefferson, T.; Ferroni, E.; Rivetti, A.; Di Pietrantonj, C. Vaccines for preventing influenza in healthy adults. In Cochrane Database Of Systematic Reviews; Cochrane Library: Hoboken, NJ, USA, 2018. Available online: https://pubmed.ncbi.nlm.nih.gov/29388196 (accessed on 7 January 2021).
- Centers for Disease Control and Prevention. Vaccine Effectiveness: How Well Do the Flu Vaccines Work? Available online: https://www.cdc.gov/flu/vaccines-work/vaccineeffect.htm (accessed on 26 November 2020).
- Remschmidt, C.; Wichmann, O.; Harder, T. Frequency and impact of confounding by indication and healthy vaccinee bias in observational studies assessing influenza vaccine effectiveness: A systematic review. BMC Infect. Dis. 2015, 15, 429. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Infection | No Infection | ||
|---|---|---|---|
| Vaccine | a | b | a + b |
| Placebo | c | d | c + d |
| Infection | No Infection | ||
|---|---|---|---|
| BNT162b2 | 8 | 21,712 | 21,720 |
| Placebo | 162 | 21,564 | 21,726 |
| Infection | No Infection | ||
|---|---|---|---|
| mRNA-1273 | 11 | 15,199 | 15,210 |
| Placebo | 185 | 15,025 | 15,210 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brown, R.B. Outcome Reporting Bias in COVID-19 mRNA Vaccine Clinical Trials. Medicina 2021, 57, 199. https://doi.org/10.3390/medicina57030199
Brown RB. Outcome Reporting Bias in COVID-19 mRNA Vaccine Clinical Trials. Medicina. 2021; 57(3):199. https://doi.org/10.3390/medicina57030199
Chicago/Turabian StyleBrown, Ronald B. 2021. "Outcome Reporting Bias in COVID-19 mRNA Vaccine Clinical Trials" Medicina 57, no. 3: 199. https://doi.org/10.3390/medicina57030199
APA StyleBrown, R. B. (2021). Outcome Reporting Bias in COVID-19 mRNA Vaccine Clinical Trials. Medicina, 57(3), 199. https://doi.org/10.3390/medicina57030199