A Machine Learning-Based Investigation of Gender-Specific Prognosis of Lung Cancers

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Preprocessing of the SEER Database
2.3. Binary Classification Algorithms
2.4. Evaluation Metrics of Binary Classification Algorithms
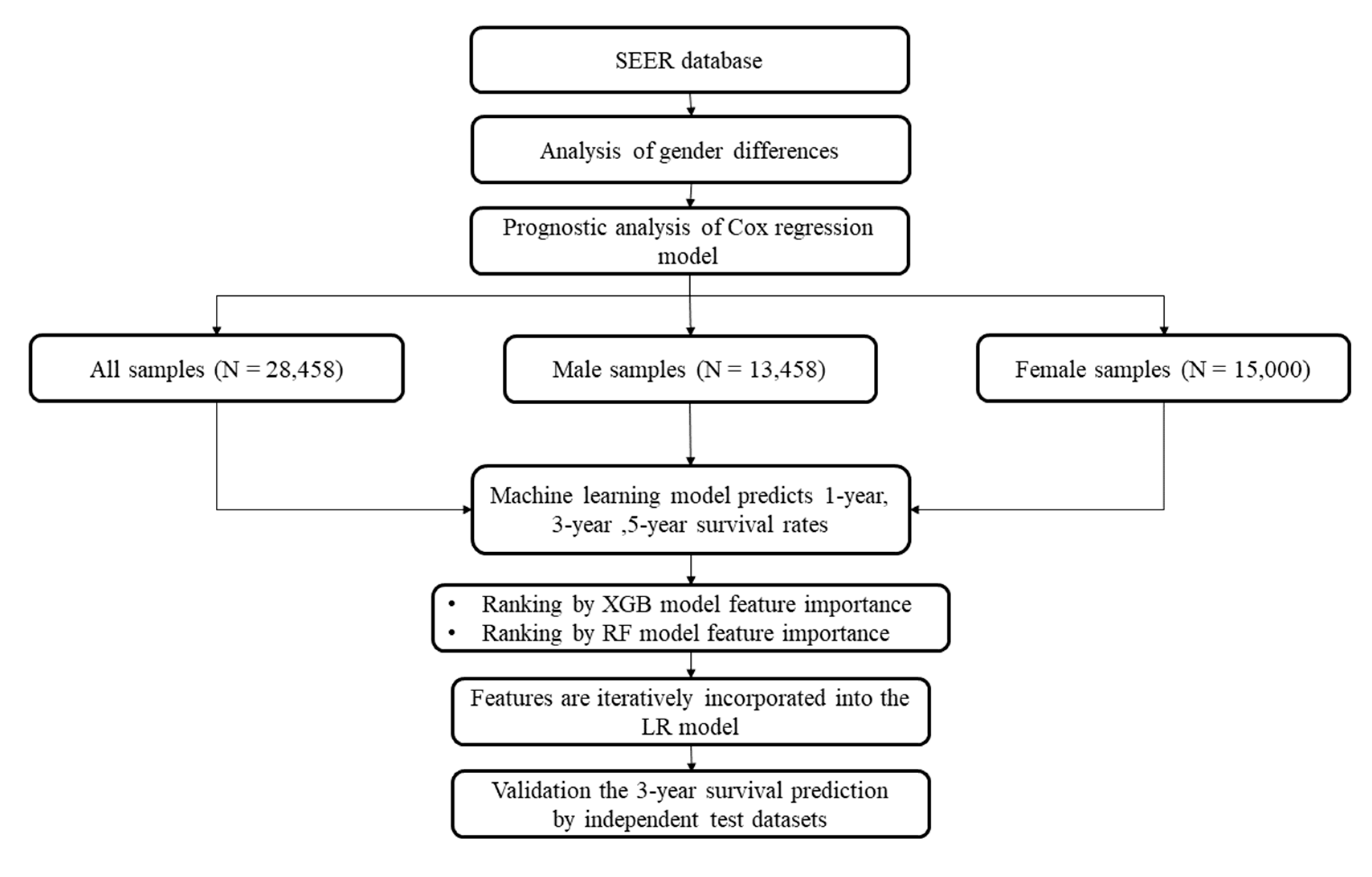
2.5. Data Analysis Procedure
3. Results
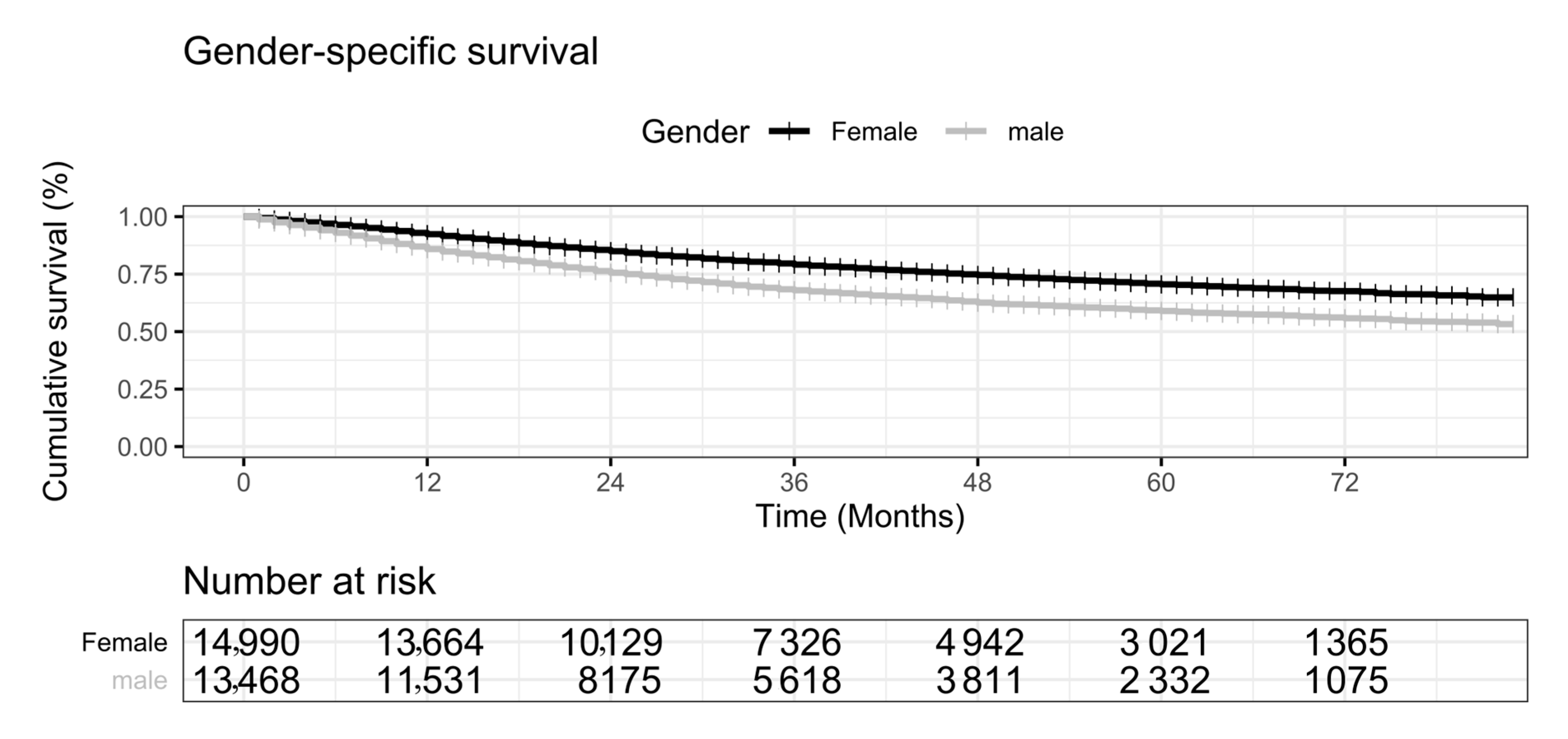
3.1. Gender Disparities in the Prognosis of Primary Lung Cancers
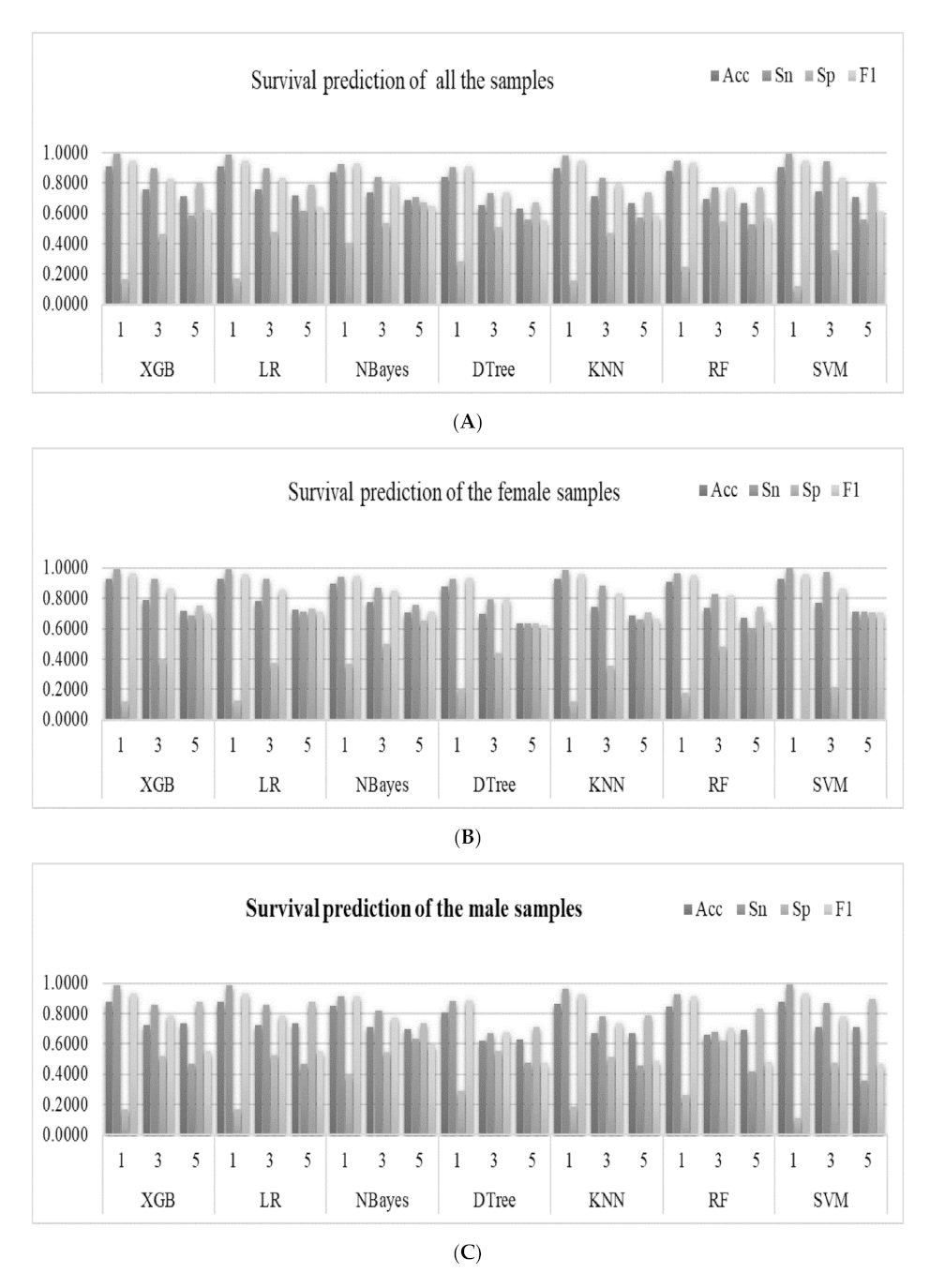
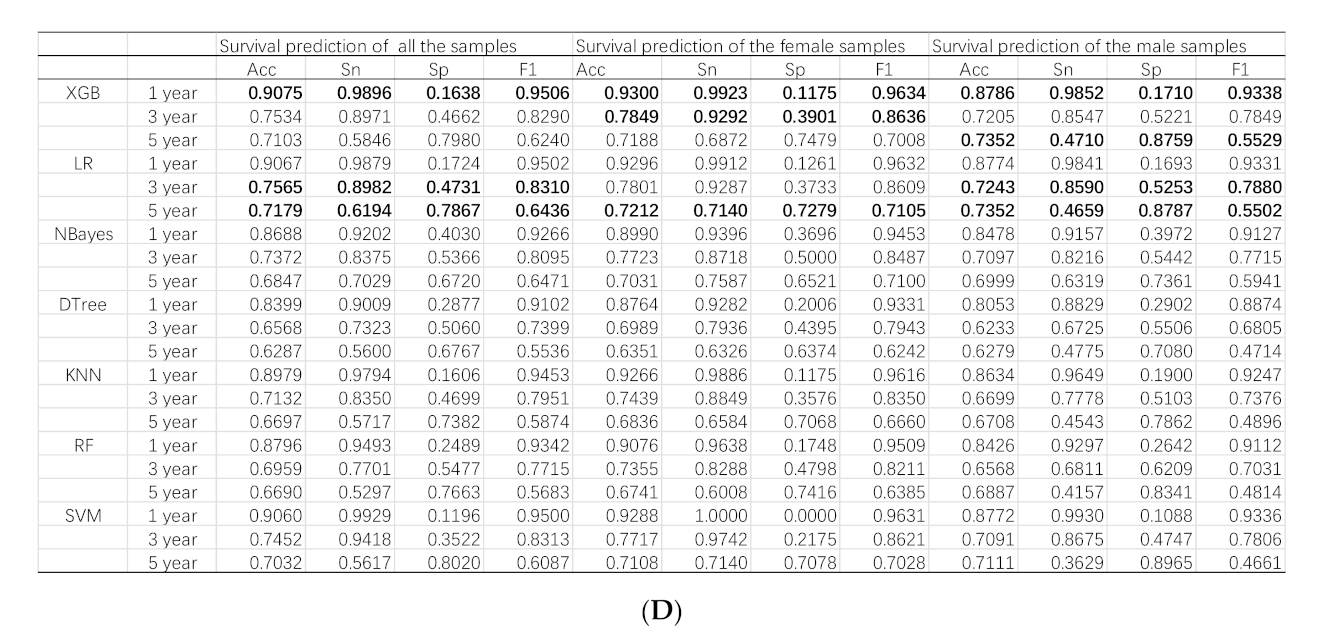
3.2. Machine Learning-Based Prediction of Survival Status
3.3. Feature Contributions of the XGB Models
3.4. Feature Contributions to the RF Models
3.5. Independent Validation of the Models Using Future Samples
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Jemal, A.; Miller, K.D.; Ma, J.; Siegel, R.L.; Fedewa, S.A.; Islami, F.; Devesa, S.S.; Thun, M.J. Higher Lung Cancer Incidence in Young Women Than Young Men in the United States. N. Engl. J. Med. 2018, 378, 1999–2009. [Google Scholar] [CrossRef] [PubMed]
- Sagerup, C.M.; Smastuen, M.; Johannesen, T.B.; Helland, A.; Brustugun, O.T. Sex-specific trends in lung cancer incidence and survival: A population study of 40,118 cases. Thorax 2011, 66, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, H.; Ando, K.; Shinmyo, T.; Morita, K.; Mochizuki, A.; Kurimoto, N.; Tatsunami, S. Female gender is an independent prognostic factor in non-small-cell lung cancer: A meta-analysis. Ann. Thorac. Cardiovasc. Surg. 2011, 17, 469–480. [Google Scholar] [CrossRef]
- Rivera, M.P. Lung cancer in women: Differences in epidemiology, biology, histology, and treatment outcomes. Semin. Respir. Crit. Care Med. 2013, 34, 792–801. [Google Scholar] [CrossRef]
- Liu, Y.; Shen, J.; Liu, L.; Shan, L.; He, J.; He, Q.; Jiang, L.; Guo, M.; Chen, X.; Pan, H.; et al. Impact of examined lymph node counts on survival of patients with stage IA non-small cell lung cancer undergoing sublobar resection. J. Thorac. Dis. 2018, 10, 6569–6577. [Google Scholar] [CrossRef]
- Wang, C.; Qiao, W.; Jiang, Y.; Zhu, M.; Shao, J.; Ren, P.; Liu, D.; Li, W. Effect of sex on the efficacy of patients receiving immune checkpoint inhibitors in advanced non-small cell lung cancer. Cancer Med. 2019, 8, 4023–4031. [Google Scholar] [CrossRef]
- Donington, J.S.; Colson, Y.L. Sex and gender differences in non-small cell lung cancer. Semin. Thorac. Cardiovasc. Surg. 2011, 23, 137–145. [Google Scholar] [CrossRef]
- Moore, R.; Doherty, D.; Chamberlain, R.; Khuri, F. Sex differences in survival in non-small cell lung cancer patients 1974–1998. Acta Oncol. 2004, 43, 57–64. [Google Scholar] [CrossRef]
- Zang, E.A.; Wynder, E.L. Differences in lung cancer risk between men and women: Examination of the evidence. J. Natl. Cancer Inst. 1996, 88, 183–192. [Google Scholar] [CrossRef]
- Stabile, L.P.; Siegfried, J.M. Sex and gender differences in lung cancer. J. Gend. Specif. Med. 2003, 6, 37–48. [Google Scholar] [PubMed]
- Gasperino, J. Gender is a risk factor for lung cancer. Med. Hypotheses 2011, 76, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Wisnivesky, J.P.; Halm, E.A. Sex differences in lung cancer survival: Do tumors behave differently in elderly women? J. Clin. Oncol. 2007, 25, 1705–1712. [Google Scholar] [CrossRef] [PubMed]
- Viswambaram, P.; Hayne, D. Gender discrepancies in bladder cancer: Potential explanations. Expert Rev. Anticancer. Ther. 2020, 20, 841–849. [Google Scholar] [CrossRef]
- Dittberner, A.; Friedl, B.; Wittig, A.; Buentzel, J.; Kaftan, H.; Boeger, D.; Mueller, A.H.; Schultze-Mosgau, S.; Schlattmann, P.; Ernst, T.; et al. Gender Disparities in Epidemiology, Treatment, and Outcome for Head and Neck Cancer in Germany: A Population-Based Long-Term Analysis from 1996 to 2016 of the Thuringian Cancer Registry. Cancers 2020, 12, 3418. [Google Scholar] [CrossRef]
- Li, J.; Zheng, Q.; Zhao, X.; Zhao, J.; An, T.; Wu, M.; Wang, Y.; Zhuo, M.; Zhong, J.; Yang, X.; et al. Nomogram model for predicting cause-specific mortality in patients with stage I small-cell lung cancer: A competing risk analysis. BMC Cancer 2020, 20, 793. [Google Scholar] [CrossRef]
- Xu, Y.; Liang, F.; Chen, Y.; Wang, Z.; Zhong, H.; Tang, W. Novel Model to Predict the Prognosis of Patients with Stage II-III Colon Cancer. BioMed Res. Int. 2020, 2020, 8812974. [Google Scholar] [CrossRef]
- Karakiewicz, P.I.; Shariat, S.F.; Palapattu, G.S.; Perrotte, P.; Lotan, Y.; Rogers, C.G.; Amiel, G.E.; Vazina, A.; Gupta, A.; Bastian, P.J.; et al. Precystectomy nomogram for prediction of advanced bladder cancer stage. Eur. Urol. 2006, 50, 1254–1260; discussion 1261–1262. [Google Scholar] [CrossRef]
- Iasonos, A.; Schrag, D.; Raj, G.V.; Panageas, K.S. How to build and interpret a nomogram for cancer prognosis. J. Clin. Oncol. 2008, 26, 1364–1370. [Google Scholar] [CrossRef]
- Deng, J.; Ren, Z.; Wen, J.; Wang, B.; Hou, X.; Xue, Z.; Chu, X. Construction of a nomogram predicting the overall survival of patients with distantly metastatic non-small-cell lung cancer. Cancer Manag. Res. 2018, 10, 6143–6156. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Pang, Z.; Chen, X.; Bie, F.; Wang, Y.; Wang, G.; Liu, Q.; Du, J. Survival nomogram for patients with initially diagnosed metastatic non-small-cell lung cancer: A SEER-based study. Futur. Oncol. 2019, 15, 3395–3409. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Zhang, L.; Jiang, G.; Wang, Q.; Liu, L.; Liu, D.; Wang, Z.; Zhu, Z.; Deng, Q.; Xiong, X.; et al. Development and validation of a nomogram for predicting survival in patients with resected non-small-cell lung cancer. J. Clin. Oncol. 2015, 33, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Yap, W.K.; Shih, M.C.; Kuo, C.; Pai, P.C.; Chou, W.C.; Chang, K.P.; Tsai, M.H.; Tsang, N.M. Development and Validation of a Nomogram for Assessing Survival in Patients With Metastatic Lung Cancer Referred for Radiotherapy for Bone Metastases. JAMA Netw. Open 2018, 1, e183242. [Google Scholar] [CrossRef] [PubMed]
- Bandini, M.; Fossati, N.; Briganti, A. Nomograms in urologic oncology, advantages and disadvantages. Curr. Opin. Urol. 2019, 29, 42–51. [Google Scholar] [CrossRef]
- Alabi, R.O.; Mäkitie, A.A.; Pirinen, M.; Elmusrati, M.; Leivo, I.; Almangush, A. Comparison of nomogram with machine learning techniques for prediction of overall survival in patients with tongue cancer. Int. J. Med Inform. 2021, 145, 104313. [Google Scholar] [CrossRef]
- Marrogi, A.J.; Mechanic, L.E.; Welsh, J.A.; Bowman, E.D.; Khan, M.A.; Enewold, L.; Shields, P.G.; Harris, C.C. TP53 mutation spectrum in lung cancer is not different in women and men. Cancer Epidemiol. Biomark. Prev. 2005, 14, 1031–1033. [Google Scholar] [CrossRef]
- Delisle, M.; Singh, S.; Howard, J.; Panda, N.; Weppler, A.M.; Wang, Y. Refusal of colorectal cancer surgery in the United States: Predictors and associated cancer-specific mortality in a Surveillance, Epidemiology, and End Results (SEER) cohort. Surg. Open Sci. 2020, 2, 12–18. [Google Scholar] [CrossRef]
- Thompson, A.B.; Quinn, T.J.; Siddiqui, Z.A.; Almahariq, M.F.; Grills, I.S.; Stevens, C.W. Addition of radiotherapy to surgery and chemotherapy improves survival in localized malignant pleural mesothelioma: A Surveillance, Epidemiology, and End Results (SEER) study. Lung Cancer 2020, 146, 120–126. [Google Scholar] [CrossRef]
- Goldstraw, P.; Crowley, J.; Chansky, K.; Giroux, D.J.; Groome, P.A.; Rami-Porta, R.; Postmus, P.E.; Rusch, V.; Sobin, L. The IASLC Lung Cancer Staging Project: Proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumours. J. Thorac. Oncol. 2007, 2, 706–714. [Google Scholar] [CrossRef]
- Gao, Y.; Zhou, X. Analysis of clinical features and prognostic factors of lung cancer patients: A population-based cohort study. Clin. Respir. J. 2020. [Google Scholar] [CrossRef]
- Deng, W.; Xu, T.; Wang, Y.; Xu, Y.; Yang, P.; Gomez, D.; Liao, Z. Log odds of positive lymph nodes may predict survival benefit in patients with node-positive non-small cell lung cancer. Lung Cancer 2018, 122, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Zhang, Q.; Zhao, Y.; Liu, Y.; Chen, A.; Li, X.; Wu, T.; Li, J.; Guo, Y.; Liu, A. Radiomics Analysis of Iodine-Based Material Decomposition Images With Dual-Energy Computed Tomography Imaging for Preoperatively Predicting Microsatellite Instability Status in Colorectal Cancer. Front. Oncol. 2019, 9, 1250. [Google Scholar] [CrossRef] [PubMed]
- Cui, S.; Zhao, L.; Wang, Y.; Dong, Q.; Ma, J.; Wang, Y.; Zhao, W.; Ma, X. Using Naive Bayes Classifier to predict osteonecrosis of the femoral head with cannulated screw fixation. Injury 2018, 49, 1865–1870. [Google Scholar] [CrossRef] [PubMed]
- Wood, A.; Shpilrain, V.; Najarian, K.; Kahrobaei, D. Private naive bayes classification of personal biomedical data: Application in cancer data analysis. Comput. Biol. Med. 2019, 105, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Ferraz, P.F.P.; Julio, Y.H.F.; Ferraz, G.; Moura, R.S.; Rossi, G.; Saraz, J.A.O.; Barbari, M. Decision Trees for Predicting the Physiological Responses of Rabbits. Animals 2019, 9, 994. [Google Scholar] [CrossRef]
- Sarica, A.; Cerasa, A.; Quattrone, A. Random Forest Algorithm for the Classification of Neuroimaging Data in Alzheimer's Disease: A Systematic Review. Front. Aging Neurosci. 2017, 9, 329. [Google Scholar] [CrossRef]
- Guang, P.; Huang, W.; Guo, L.; Yang, X.; Huang, F.; Yang, M.; Wen, W.; Li, L. Blood-based FTIR-ATR spectroscopy coupled with extreme gradient boosting for the diagnosis of type 2 diabetes: A STARD compliant diagnosis research. Medicine 2020, 99, e19657. [Google Scholar] [CrossRef]
- Fang, W.H.; Yang, J.R.; Lin, C.Y.; Hsiao, P.J.; Tu, M.Y.; Chen, C.F.; Tsai, D.J.; Su, W.; Huang, G.S.; Chang, H.; et al. Accuracy augmentation of body composition measurement by bioelectrical impedance analyzer in elderly population. Medicine 2020, 99, e19103. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Li, X.; Zong, M.; Zhu, X.; Wang, R. Efficient kNN Classification With Different Numbers of Nearest Neighbors. IEEE Trans. Neural Netw. Learn. Syst. 2018, 29, 1774–1785. [Google Scholar] [CrossRef]
- Jang, S.K.; Chang, J.Y.; Lee, J.S.; Lee, E.J.; Kim, Y.H.; Han, J.H.; Chang, D.I.; Cho, H.J.; Cha, J.K.; Yu, K.H.; et al. Reliability and Clinical Utility of Machine Learning to Predict Stroke Prognosis: Comparison with Logistic Regression. J. Stroke 2020, 22, 403–406. [Google Scholar] [CrossRef]
- Doubilet, P.M.; Phillips, C.H.; Durfee, S.M.; Benson, C.B. First-Trimester Prognosis When an Early Gestational Sac is Seen on Ultrasound Imaging: Logistic Regression Prediction Model. J. Ultrasound Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Quitadamo, L.R.; Cavrini, F.; Sbernini, L.; Riillo, F.; Bianchi, L.; Seri, S.; Saggio, G. Support vector machines to detect physiological patterns for EEG and EMG-based human-computer interaction: A review. J. Neural Eng. 2017, 14, 011001. [Google Scholar] [CrossRef] [PubMed]
- Claesson, L.; Blomstrand, J.; Eklund, K.; Eriksson, K.; Dahlin-Ivanoff, S. Comparison of visual acuity charts identifying visual impairment among older people outside the eye clinic. Disabil. Rehabil. 2013, 35, 1394–1400. [Google Scholar] [CrossRef] [PubMed]
- Dixit, A.; Yohannan, J.; Boland, M.V. Assessing Glaucoma Progression Using Machine Learning Trained on Longitudinal Visual Field and Clinical Data. Ophthalmology 2020. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Xu, C.; Yang, W.; Shu, Y.; Zheng, W.; Zhou, F. Multiple similarly effective solutions exist for biomedical feature selection and classification problems. Sci. Rep. 2017, 7, 12830. [Google Scholar] [CrossRef]
- Radkiewicz, C.; Dickman, P.W.; Johansson, A.L.V.; Wagenius, G.; Edgren, G.; Lambe, M. Sex and survival in non-small cell lung cancer: A nationwide cohort study. PLoS ONE 2019, 14, e0219206. [Google Scholar] [CrossRef]
- Berardi, R.; Verdecchia, L.; Paolo, M.D.; Giampieri, R.; Scartozzi, M.; Pierantoni, C.; Bianconi, M.; Mazzanti, P.; Cascinu, S. Women and lung cancer: Clinical and molecular profiling as a determinate for treatment decisions: A literature review. Crit. Rev. Oncol. 2009, 69, 223–236. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, F.L.; Ito, Y.; Morishima, T.; Miyashiro, I.; Nakayama, T. Sex differences in lung cancer survival: Long-term trends using population-based cancer registry data in Osaka, Japan. Jpn. J. Clin. Oncol. 2017, 47, 863–869. [Google Scholar] [CrossRef]
- Graham, P.D.; Thigpen, S.C.; Geraci, S.A. Lung cancer in women. South. Med. J. 2013, 106, 582–587. [Google Scholar] [CrossRef]
- Rodriguez-Lara, V.; Ramirez-Tirado, L.A.; Barron, F.; Zatarain-Barron, Z.L.; Flores-Estrada, D.; Arrieta, O. Characteristics of non-small cell lung cancer: Differences by sex and hormonal status in a Mexican population. Salud Publica Mexico 2019, 61, 265–275. [Google Scholar] [CrossRef]
- Song, Y.; Gao, S.; Tan, W.; Qiu, Z.; Zhou, H.; Zhao, Y. Multiple Machine Learnings Revealed Similar Predictive Accuracy for Prognosis of PNETs from the Surveillance, Epidemiology, and End Result Database. J. Cancer 2018, 9, 3971–3978. [Google Scholar] [CrossRef] [PubMed]
- Conforti, F.; Pala, L.; Bagnardi, V.; Viale, G.; De Pas, T.; Pagan, E.; Pennacchioli, E.; Cocorocchio, E.; Ferrucci, P.F.; De Marinis, F.; et al. Sex-based heterogeneity in response to lung cancer immunotherapy: A systematic review and meta-analysis. J. Nat. Cancer Inst. 2019. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Cowley, L.A.; Liu, X.S. Sex Differences in Cancer Immunotherapy Efficacy, Biomarkers, and Therapeutic Strategy. Molecules 2019, 24, 3214. [Google Scholar] [CrossRef] [PubMed]
- Pino Peña, I.; Cheplygina, V.; Paschaloudi, S.; Vuust, M.; Carl, J.; Weinreich, U.M.; Østergaard, L.R.; de Bruijne, M. Automatic emphysema detection using weakly labeled HRCT lung images. PLoS ONE 2018, 13, e0205397. [Google Scholar] [CrossRef]
- Safta, W.; Frigui, H. Multiple Instance Learning for Benign vs. Malignant Classification of Lung Nodules in CT Scans. In Proceedings of the 2018 IEEE International Symposium on Signal Processing and Information Technology (ISSPIT), Louisville, KY, USA, 6–8 December 2018; pp. 490–494. [Google Scholar]
- Astorino, A.; Fuduli, A.; Veltri, P.; Vocaturo, E. Melanoma Detection by Means of Multiple Instance Learning. Interdiscip. Sci. Comput. Life Sci. 2020, 12, 24–31. [Google Scholar] [CrossRef]
- Fuduli, A.; Veltri, P.; Vocaturo, E.; Zumpano, E. Melanoma detection using color and texture features in computer vision systems. Adv. Sci. Technol. Eng. Syst. J. 2019, 4, 16–22. [Google Scholar] [CrossRef]
- Gaudioso, M.; Giallombardo, G.; Miglionico, G.; Vocaturo, E. Classification in the multiple instance learning framework via spherical separation. Soft Comput. 2020, 24, 5071–5077. [Google Scholar] [CrossRef]
- Vocaturo, E.; Zumpano, E.; Giallombardo, G.; Miglionico, G. DC-SMIL: A multiple instance learning solution via spherical separation for automated detection of displastyc nevi. In Proceedings of the 24th Symposium on International Database Engineering & Applications, Seoul, Korea, 12–18 August 2020. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Female | Male | t | p-value | |
| Age | 66.19 ± 10.52 | 66.45 ± 9.70 | 2.16 | 0.03 |
| LOODS | −2.24 ± 1.27 | −2.18 ± 1.32 | 3.77 | <0.001 |
| Female | Male | χ2 | p-value | |
| Race | 10.22 | 0.006 | ||
| White | 12,362 (82.50%) | 11,204 (83.20%) | ||
| Black | 1447 (9.70%) | 1157 (8.60%) | ||
| Other | 1181 (7.90%) | 1107 (8.20%) | ||
| Histological Type | 836.71 | <0.001 | ||
| Adenocarcinoma | 10,256 (68.40%) | 7330 (54.40%) | ||
| Squamous cell carcinoma | 2646 (17.70%) | 4319 (32.10%) | ||
| Large cell carcinoma | 239 (1.60%) | 265 (2.00%) | ||
| Small cell carcinoma | 203 (1.40%) | 165 (1.20%) | ||
| Other | 1646 (11.00%) | 1389 (10.30%) | ||
| Grade | 432.92 | <0.001 | ||
| Grade I | 3296 (22.00%) | 1865 (13.80%) | ||
| Grade II | 6522 (43.50%) | 5701 (42.30%) | ||
| Grade III | 4843 (32.30%) | 5580 (41.40%) | ||
| Grade IV | 329 (2.20%) | 322 (2.40%) | ||
| surgery | 50.41 | <0.001 | ||
| YES | 14,241 (95.00%) | 12,521 (93.00%) | ||
| NO | 749 (5.00%) | 947 (7.00%) | ||
| Marital status | 1017.37 | <0.001 | ||
| Single | 7408 (49.40%) | 4151 (30.80%) | ||
| Married | 7582 (50.60%) | 9317 (69.20%) | ||
| Laterality | 1.84 | 0.175 | ||
| Right | 8826 (58.90%) | 77,823 (58.10%) | ||
| Left | 6164 (41.10%) | 5645 (41.90%) | ||
| T | 249.96 | <0.001 | ||
| T1 | 6796 (45.30%) | 4931 (36.60%) | ||
| T2 | 5526 (36.90%) | 5462 (40.60%) | ||
| T3 | 1877 (12.50%) | 2244 (16.70%) | ||
| T4 | 791 (5.30%) | 831 (6.20%) | ||
| N | 108.54 | <0.001 | ||
| N0 | 11,116 (74.20%) | 9278 (68.90%) | ||
| N1 | 1740 (11.60%) | 1987 (14.80%) | ||
| N2 | 1934 (12.90%) | 1944 (14.40%) | ||
| N3 | 200 (1.30%) | 259 (1.90%) | ||
| M | 20.22 | <0.001 | ||
| M0 | 14,266 (95.20%) | 12,655 (94.00%) | ||
| M1 | 724 (4.80%) | 813 (6.00%) | ||
| Year of diagnosis | 3.47 | 0.682 | ||
| 2010 | 2367 (15.80%) | 2176 (16.20%) | ||
| 2011 | 2381 (15.90%) | 2164 (16.10%) | ||
| 2012 | 2348 (15.70%) | 2169 (16.10%) | ||
| 2013 | 2541 (17.00%) | 2216 (16.50%) | ||
| 2014 | 2602 (17.40%) | 2332 (17.30%) | ||
| 2015 | 2751 (18.40%) | 2411 (17.90%) |
| Univariate | Multivariate | |||
| HR(95%CI) | p-value | HR(95%CI) | p-value | |
| Age | 1.017(1.014,1.019) | <0.001 | 1.024(1.021,1.026) | <0.001 |
| LOODS | 1.505(1.483,1.526) | <0.001 | 1.179(1.154,1.205) | <0.001 |
| Race | <0.001 | 0.001 | ||
| White | 1 | 1 | ||
| Black | 0.984(0.912,1.063) | 0.685 | 0.998(0.923,1.079) | 0.961 |
| Other | 0.828(0.759,0.904) | <0.001 | 0.841(0.77,0.918) | <0.001 |
| Sex | <0.001 | <0.001 | ||
| Male | 1 | 1 | ||
| Female | 0.628(0.601,0.657) | 0.698(0.666,0.731) | ||
| Histological Type | <0.001 | <0.001 | ||
| Adenocarcinoma | 1 | 1 | ||
| Squamous cell carcinoma | 1.501(1.427,1.578) | <0.001 | 1.171(1.111,1.235) | <0.001 |
| Large cell carcinoma | 2.049(1.792,2.342) | <0.001 | 1.603(1.389,1.851) | <0.001 |
| Small cell carcinoma | 3.381(2.95,3.876) | <0.001 | 1.481(1.272,1.724) | <0.001 |
| Other | 1.086(1.007,1.172) | 0.032 | 1.073(0.994,1.16) | 0.072 |
| Grade | <0.001 | <0.001 | ||
| Grade I | 1 | 1 | ||
| Grade II | 2.455(2.245,2.685) | <0.001 | 1.747(1.593,1.915) | <0.001 |
| Grade III | 4.273(3.914,4.665) | <0.001 | 2.305(2.102,2.526) | <0.001 |
| Grade IV | 5.424(4.713,6.242) | <0.001 | 2.306(1.97,2.701) | <0.001 |
| surgery | <0.001 | <0.001 | ||
| YES | 1 | 1 | ||
| NO | 5.354(5.036,5.692) | 1.631(1.502,1.77) | ||
| Marital status | 0.008 | <0.001 | ||
| Single | 1 | 1 | ||
| Married | 0.941(0.9,0.984) | 0.865(0.826,0.907) | ||
| Laterality | 0.322 | |||
| Right | 1 | |||
| Left | 1.023(0.978,1.069) | |||
| T | <0.001 | <0.001 | ||
| T1 | 1 | 1 | ||
| T2 | 2.068(1.954,2.188) | <0.001 | 1.529(1.443,1.62) | <0.001 |
| T3 | 3.5(3.283,3.732) | <0.001 | 2.23(2.086,2.385) | <0.001 |
| T4 | 4.633(4.272,5.023) | <0.001 | 1.992(1.825,2.174) | <0.001 |
| N | <0.001 | <0.001 | ||
| N0 | 1 | 1 | ||
| N1 | 2.453(2.312,2.602) | <0.001 | 1.554(1.452,1.664) | <0.001 |
| N2 | 3.75(3.557,3.954) | <0.001 | 1.731(1.606,1.865) | <0.001 |
| N3 | 8.143(7.307,9.075) | <0.001 | 1.661(1.443,1.912) | <0.001 |
| M | <0.001 | <0.001 | ||
| M0 | 1 | 1 | ||
| M1 | 4.581(4.294,4.887) | 2.137(1.984,2.302) | ||
| One-year | |||||
| All | Male | Female | |||
| Characteristic | Relative Importance | Characteristic | Relative Importance | Characteristic | Relative Importance |
| Surgery | 0.3279 | Surgery | 0.4734 | Surgery | 0.2771 |
| T | 0.1334 | T | 0.1284 | N | 0.1652 |
| M | 0.1261 | M | 0.0972 | M | 0.1560 |
| N | 0.1208 | N | 0.0801 | T | 0.1123 |
| Grade | 0.0917 | Grade | 0.0662 | Grade | 0.0926 |
| Histologic Type | 0.0450 | Histologic Type | 0.0406 | LOODS | 0.0495 |
| Gender | 0.0446 | LOODS | 0.0375 | Histologic Type | 0.0471 |
| LOODS | 0.0396 | Age | 0.0289 | Age | 0.0385 |
| Age | 0.0303 | Race | 0.0217 | Marital | 0.0294 |
| Marital | 0.0174 | Marital | 0.0155 | Race | 0.0208 |
| Race | 0.0122 | Laterality | 0.0107 | Laterality | 0.0115 |
| Laterality | 0.0112 | ||||
| Three-year | |||||
| All | Male | Female | |||
| Characteristic | Relative Importance | Characteristic | Relative Importance | Characteristic | Relative Importance |
| N | 0.4364 | N | 0.3591 | N | 0.4251 |
| Surgery | 0.1538 | Surgery | 0.2031 | Surgery | 0.1588 |
| T | 0.1059 | T | 0.1508 | Grade | 0.1152 |
| Grade | 0.0883 | M | 0.0902 | T | 0.0935 |
| M | 0.0695 | Grade | 0.0633 | M | 0.0815 |
| Gender | 0.0491 | LOODS | 0.0373 | LOODS | 0.0308 |
| LOODS | 0.0240 | Age | 0.0290 | Histologic Type | 0.0278 |
| Histologic Type | 0.0235 | Histologic Type | 0.0256 | Age | 0.0259 |
| Age | 0.0209 | Marital | 0.0235 | Race | 0.0169 |
| Race | 0.0120 | Race | 0.0103 | Marital | 0.0166 |
| Marital | 0.0107 | Laterality | 0.0077 | Laterality | 0.0080 |
| Laterality | 0.0058 | ||||
| Five-year | |||||
| All | Male | Female | |||
| Characteristic | Relative Importance | Characteristic | Relative Importance | Characteristic | Relative Importance |
| N | 0.4279 | N | 0.4389 | N | 0.4728 |
| Surgery | 0.1357 | T | 0.1282 | Grade | 0.1299 |
| T | 0.1321 | Surgery | 0.1275 | Surgery | 0.1144 |
| Grade | 0.0858 | M | 0.0959 | T | 0.0949 |
| M | 0.0523 | Grade | 0.0611 | M | 0.0570 |
| Gender | 0.0471 | LOODS | 0.0391 | LOODS | 0.0316 |
| LOODS | 0.0325 | Age | 0.0341 | Age | 0.0288 |
| Age | 0.0283 | Marital | 0.0267 | Histologic Type | 0.0206 |
| Histologic Type | 0.0248 | Histologic Type | 0.0231 | Marital | 0.0205 |
| Marital | 0.0185 | Race | 0.0150 | Laterality | 0.0159 |
| Race | 0.0079 | Laterality | 0.0105 | Race | 0.0135 |
| Laterality | 0.0070 |
| One-Year | |||||
| All | Male | Female | |||
| Characteristic | Relative Importance | Characteristic | Relative Importance | Characteristic | Relative Importance |
| LOODS | 0.2869 | LOODS | 0.3040 | LOODS | 0.2898 |
| Age | 0.2820 | Age | 0.2880 | Age | 0.2813 |
| T | 0.0751 | T | 0.0814 | Grade | 0.0802 |
| Grade | 0.0664 | Grade | 0.0738 | N | 0.0789 |
| N | 0.0650 | Histologic Type | 0.0568 | T | 0.0768 |
| Histologic Type | 0.0537 | N | 0.0554 | Histologic Type | 0.0542 |
| Laterality | 0.0343 | Laterality | 0.0357 | Laterality | 0.0343 |
| Race | 0.0326 | Race | 0.0336 | Race | 0.0314 |
| Marital | 0.0308 | Marital | 0.0319 | Marital | 0.0291 |
| Surgery | 0.0290 | M | 0.0210 | Surgery | 0.0261 |
| Gender | 0.0285 | Surgery | 0.0184 | M | 0.0179 |
| M | 0.0155 | ||||
| Three-year | |||||
| All | Male | Female | |||
| Characteristic | Relative Importance | Characteristic | Relative Importance | Characteristic | Relative Importance |
| LOODS | 0.2867 | LOODS | 0.2993 | LOODS | 0.2920 |
| Age | 0.2594 | Age | 0.2810 | Age | 0.2857 |
| T | 0.0667 | T | 0.0732 | T | 0.0606 |
| Histologic Type | 0.0610 | Histologic Type | 0.0617 | Histologic Type | 0.0603 |
| N | 0.0517 | Grade | 0.0560 | Grade | 0.0576 |
| Surgery | 0.0515 | N | 0.0472 | N | 0.0520 |
| Grade | 0.0503 | M | 0.0409 | M | 0.0468 |
| Laterality | 0.0393 | Laterality | 0.0384 | Laterality | 0.0415 |
| Marital | 0.0376 | Surgery | 0.0356 | Marital | 0.0390 |
| M | 0.0341 | Race | 0.0334 | Race | 0.0325 |
| Race | 0.0318 | Marital | 0.0332 | Surgery | 0.0321 |
| Gender | 0.0297 | ||||
| Five-year | |||||
| All | Male | Female | |||
| Characteristic | Relative Importance | Characteristic | Relative Importance | Characteristic | Relative Importance |
| LOODS | 0.2869 | LOODS | 0.3040 | LOODS | 0.2898 |
| Age | 0.2820 | Age | 0.2880 | Age | 0.2813 |
| T | 0.0751 | T | 0.0814 | Grade | 0.0802 |
| Grade | 0.0664 | Grade | 0.0738 | N | 0.0789 |
| N | 0.0650 | Histologic Type | 0.0568 | T | 0.0768 |
| Histologic Type | 0.0537 | N | 0.0554 | Histologic Type | 0.0542 |
| Laterality | 0.0343 | Laterality | 0.0357 | Laterality | 0.0343 |
| Race | 0.0326 | Race | 0.0336 | Race | 0.0314 |
| Marital | 0.0308 | Marital | 0.0319 | Marital | 0.0291 |
| Surgery | 0.0290 | M | 0.0210 | Surgery | 0.0261 |
| Gender | 0.0285 | Surgery | 0.0184 | M | 0.0179 |
| M | 0.0155 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Liu, S.; Wang, Z.; Fan, Y.; Huang, J.; Huang, L.; Li, Z.; Li, X.; Jin, M.; Yu, Q.; et al. A Machine Learning-Based Investigation of Gender-Specific Prognosis of Lung Cancers. Medicina 2021, 57, 99. https://doi.org/10.3390/medicina57020099
Wang Y, Liu S, Wang Z, Fan Y, Huang J, Huang L, Li Z, Li X, Jin M, Yu Q, et al. A Machine Learning-Based Investigation of Gender-Specific Prognosis of Lung Cancers. Medicina. 2021; 57(2):99. https://doi.org/10.3390/medicina57020099
Chicago/Turabian StyleWang, Yueying, Shuai Liu, Zhao Wang, Yusi Fan, Jingxuan Huang, Lan Huang, Zhijun Li, Xinwei Li, Mengdi Jin, Qiong Yu, and et al. 2021. "A Machine Learning-Based Investigation of Gender-Specific Prognosis of Lung Cancers" Medicina 57, no. 2: 99. https://doi.org/10.3390/medicina57020099
APA StyleWang, Y., Liu, S., Wang, Z., Fan, Y., Huang, J., Huang, L., Li, Z., Li, X., Jin, M., Yu, Q., & Zhou, F. (2021). A Machine Learning-Based Investigation of Gender-Specific Prognosis of Lung Cancers. Medicina, 57(2), 99. https://doi.org/10.3390/medicina57020099