
Resolution of Disseminated Intravascular Coagulation in a Patient with COVID-19 and Associated Sepsis—Induced Neutropenia

 ,
, 
Abstract
1. Introduction
2. Case History
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tang, N.; Bai, H.; Xiong, D.; Sun, Z. Specific coagulation markers may provide more therapeutic targets in COVID-19 patients receiving prophylactic anticoagulant. J. Thromb. Haemost. 2020, 18, 2428–2430. [Google Scholar] [CrossRef] [PubMed]
- Seitz, R.; Schramm, W. DIC in COVID-19: Implications for prognosis and treatment? J. Thromb. Haemost. 2020, 18, 1798–1799. [Google Scholar] [CrossRef] [PubMed]
- Semeraro, N.; Ammollo, C.T.; Semeraro, F.; Colucci, M. Sepsis, thrombosis and organ dysfunction. Thromb. Res. 2012, 129, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Di Micco, B.; Metafora, S.; Colonna, G.; Cartenì, M.; Ragone, R.; Macalello, M.A.; Di Micco, P.; Baroni, A.; Catalanotti, P.; Tufano, M.A. Porins from Salmonella typhimurium accelerate human blood coagulation in vitro by selective stimulation of thrombin activity: Implications in septic shock DIC pathogenesis. J. Endotoxin Res. 2001, 7, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Di Micco, B.; Di Micco, P.; Lepretti, M.; Stiuso, P.; Donnarumma, G.; Iovene, M.R.; Capasso, R.; Tufano, M.A. Hyperproduction of fibrin and inefficacy of antithrombin III and alpha2 macroglobulin in the presence of bacterial porins. Int. J. Exp. Pathol. 2005, 86, 241–245. [Google Scholar] [CrossRef] [PubMed]
- White, L.; Ybarra, M. Neutropenic Fever. Hematol. Oncol. Clin. N. Am. 2017, 31, 981–993. [Google Scholar] [CrossRef] [PubMed]
- Toma, A.; Fenaux, P.; Dreyfus, F.; Cordonnier, C. Infections in myelodysplastic syndromes. Haematologica 2012, 97, 1459–1470. [Google Scholar] [CrossRef] [PubMed]
- Pagano, L.; Caira, M. Risks for infection in patients with myelodysplasia and acute leukemia. Curr. Opin. Infect. Dis. 2012, 25, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.M. COVID-19, ECMO, and lymphopenia: A word of caution. Lancet Respir. Med. 2020, 8, e24. [Google Scholar] [CrossRef]
- Fu, J.; Kong, J.; Wang, W.; Wu, M.; Yao, L.; Wang, Z.; Jin, J.; Wu, D.; Yu, X. The clinical implication of dynamic neutrophil to lymphocyte ratio and D-dimer in COVID-19: A retrospective study in Suzhou China. Thromb. Res. 2020, 192, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Procopio, G.; Cancelliere, A.; Trecarichi, E.M.; Mazzitelli, M.; Arrighi, E.; Perri, G.; Serapide, F.; Pelaia, C.; Lio, E.; Busceti, M.T.; et al. Oxygen therapy via high flow nasal cannula in severe respiratory failure caused by Sars-Cov-2 infection: A real-life observational study. Ther. Adv. Respir. Dis. 2020, 14, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Levi, M.; Sivapalaratnam, S. Disseminated intravascular coagulation: An update on pathogenesis and diagnosis. Expert Rev. Hematol. 2018, 11, 663–672. [Google Scholar] [CrossRef] [PubMed]
- Soy, M.; Keser, G.; Atagündüz, P.; Tabak, F.; Atagündüz, I.; Kayhan, S. Cytokine storm in COVID-19: Pathogenesis and overview of anti-inflammatory agents used in treatment. Clin. Rheumatol. 2020, 39, 2085–2094. [Google Scholar] [CrossRef] [PubMed]
- Polycarpou, A.; Howard, M.; Farrar, C.A.; Greenlaw, R.; Fanelli, G.; Wallis, R.; Klavinskis, L.S.; Sacks, S. Rationale for targeting complement in COVID-19. EMBO Mol. Med. 2020, 12, e12642. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Li, S.; Niu, S. ACE2 and COVID-19 and the resulting ARDS. Postgrad. Med. J. 2020, 96, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Hoevenaar, M.; Goossens, D.; Roorda, J. Angiotensin-converting enzyme 2, the complement system, the kallikrein-kinin system, type-2 diabetes, interleukin-6, and their interactions regarding the complex COVID-19 pathophysiological crossroads. J. Renin Angiotensin Aldosterone Syst. 2020, 21, 1470320320979097. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
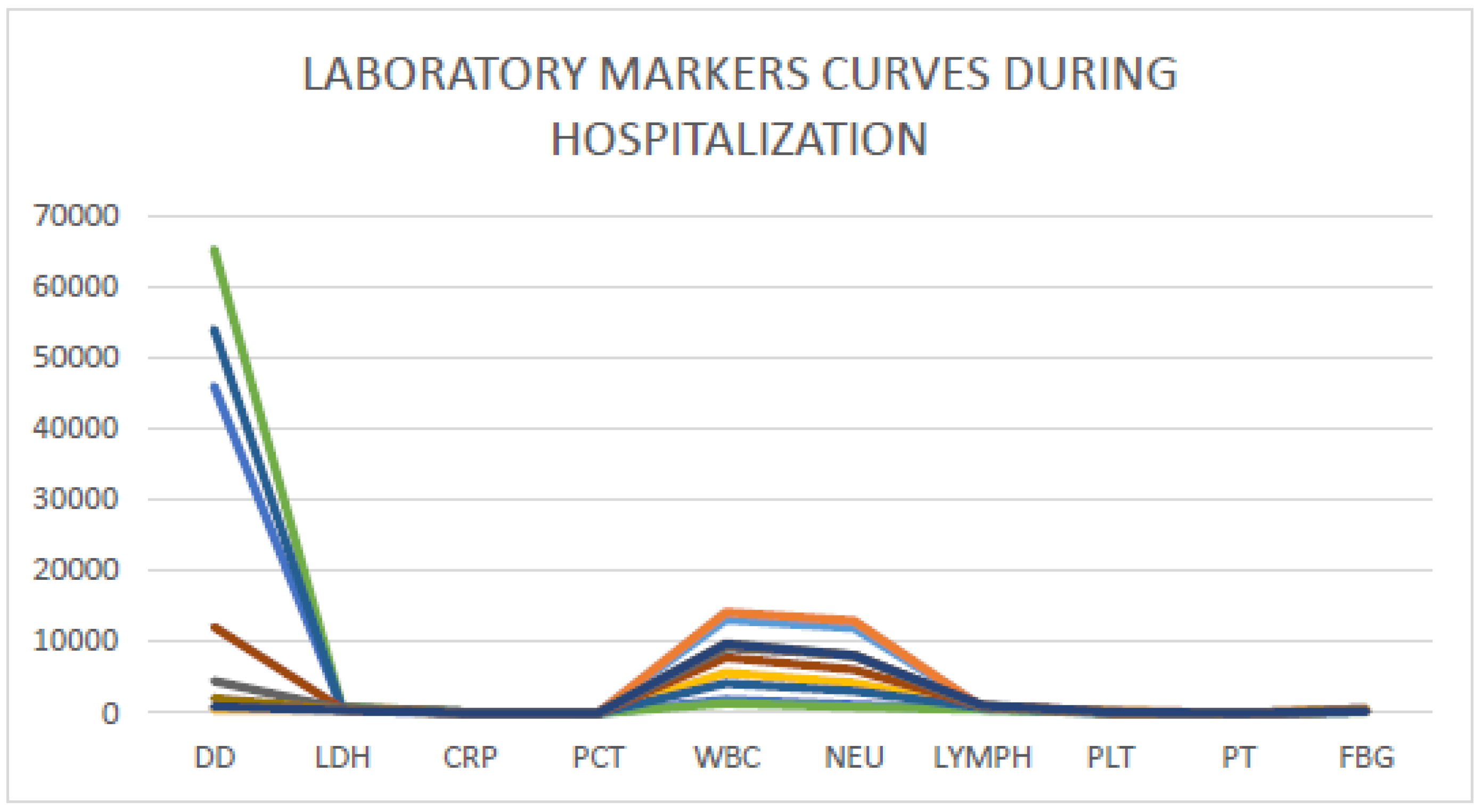
| Laboratory Test | Day 1 | Day 3 | Day 7 | Day 10 | Day 11 | Day 12 | Day 13 | Day 14 | Day 15 | Day 16 | Day 17 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| LDH (U/L) | 765 | 802 | 631 | 501 | 690 | 860 | 712 | 614 | 603 | 501 | 389 |
| CRP (mg/L) | 123 | 147 | 96 | 49 | 85 | 114 | 91 | 62 | 39 | 9 | 6 |
| Procalcitonin (ng/mL) | 0.31 | 0.26 | 0.19 | 0.16 | 1.5 | 2.3 | 1.9 | 1.1 | 0.8 | 0.6 | 0.2 |
| WBC (mmcube) | 13,150 | 14,200 | 9180 | 5691 | 1900 | 1400 | 4203 | 7802 | 9201 | 9650 | 9730 |
| Neutrophils | 11,980 | 13,000 | 8120 | 4260 | 1215 | 890 | 3120 | 6123 | 8123 | 8003 | 8115 |
| Lymphocytes | 900 | 850 | 750 | 906 | 650 | 500 | 790 | 990 | 900 | 1100 | 1110 |
| Platelets | 206 | 401 | 352 | 263 | 63 | 46 | 79 | 112 | 115 | 126 | 169 |
| Prothrombin time (INR) | 1.08 | 1.02 | 1.03 | 1.06 | 1.42 | 1.75 | 1.53 | 1.3 | 1.1 | 1.06 | 1.09 |
| Fibrinogen (mg/dL) | 612 | 602 | 630 | 590 | 260 | 202 | 301 | 402 | 289 | 302 | 236 |
| D-dimer (ng/dL) | 650 | 712 | 502 | 509 | 46,000 | 65,023 | 54,000 | 12,361 | 4526 | 2103 | 960 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Micco, P.; Imparato, M.; Lubrano, G.; Iannuzzo, D.; Fontanella, L.; Improta, L.; Poggiano, M.R.; Salzano, C.; Rodolico, A.; Fontanella, A. Resolution of Disseminated Intravascular Coagulation in a Patient with COVID-19 and Associated Sepsis—Induced Neutropenia. Medicina 2021, 57, 106. https://doi.org/10.3390/medicina57020106
Di Micco P, Imparato M, Lubrano G, Iannuzzo D, Fontanella L, Improta L, Poggiano MR, Salzano C, Rodolico A, Fontanella A. Resolution of Disseminated Intravascular Coagulation in a Patient with COVID-19 and Associated Sepsis—Induced Neutropenia. Medicina. 2021; 57(2):106. https://doi.org/10.3390/medicina57020106
Chicago/Turabian StyleDi Micco, Pierpaolo, Michele Imparato, Giuseppe Lubrano, Donatella Iannuzzo, Luca Fontanella, Lucio Improta, Maria Rita Poggiano, Ciro Salzano, Alessio Rodolico, and Andrea Fontanella. 2021. "Resolution of Disseminated Intravascular Coagulation in a Patient with COVID-19 and Associated Sepsis—Induced Neutropenia" Medicina 57, no. 2: 106. https://doi.org/10.3390/medicina57020106
APA StyleDi Micco, P., Imparato, M., Lubrano, G., Iannuzzo, D., Fontanella, L., Improta, L., Poggiano, M. R., Salzano, C., Rodolico, A., & Fontanella, A. (2021). Resolution of Disseminated Intravascular Coagulation in a Patient with COVID-19 and Associated Sepsis—Induced Neutropenia. Medicina, 57(2), 106. https://doi.org/10.3390/medicina57020106