
Dynamics of Antibody Response to BNT162b2 mRNA COVID-19 Vaccine: A 7-Month Follow-Up Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Serologic Tests
2.3. PCR Test
2.4. Statistical Analysis
3. Results
3.1. Study Participants
3.1.1. SARS-CoV-2 Previously Infected Participants
3.1.2. Uninfected Participants
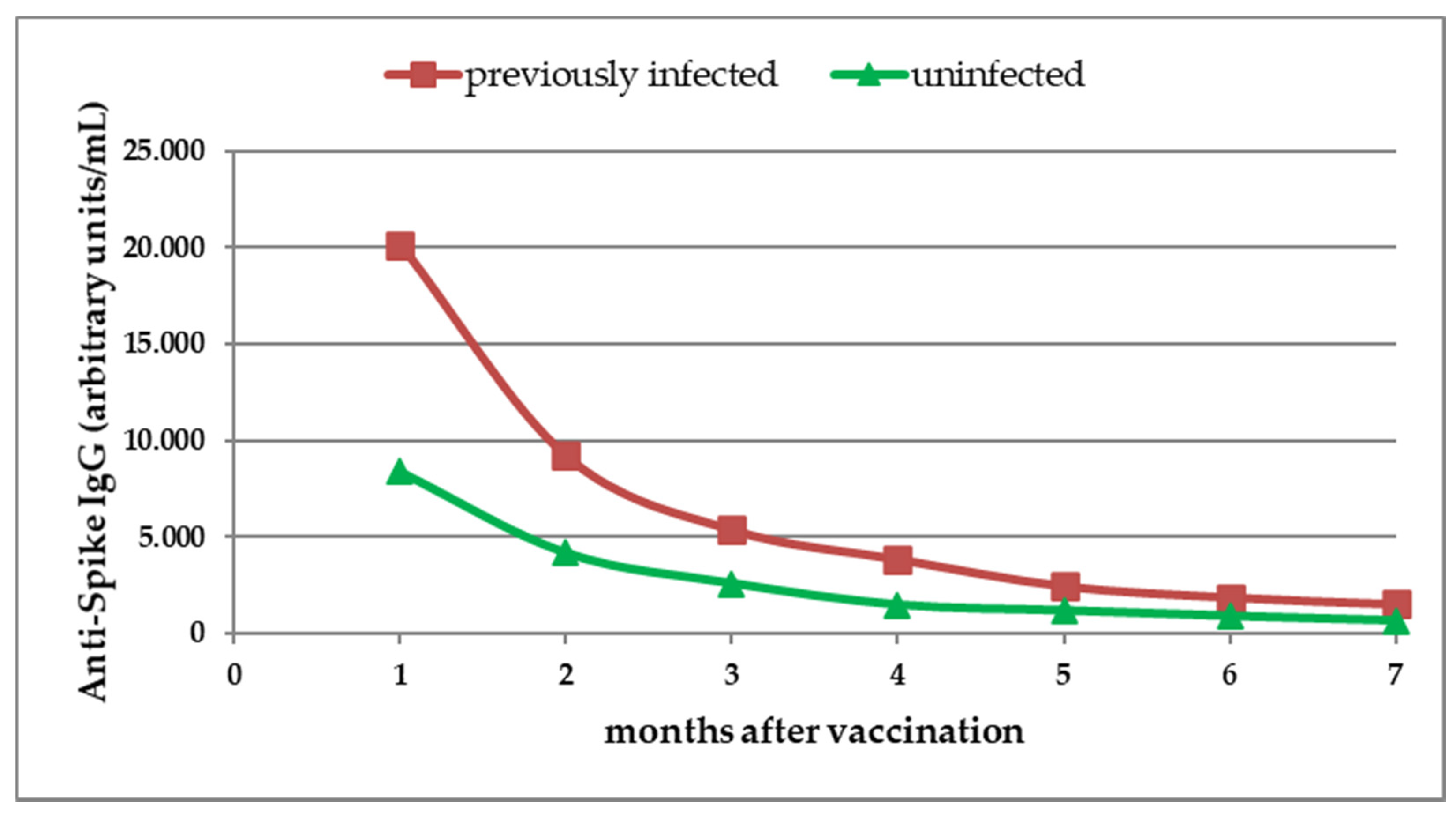
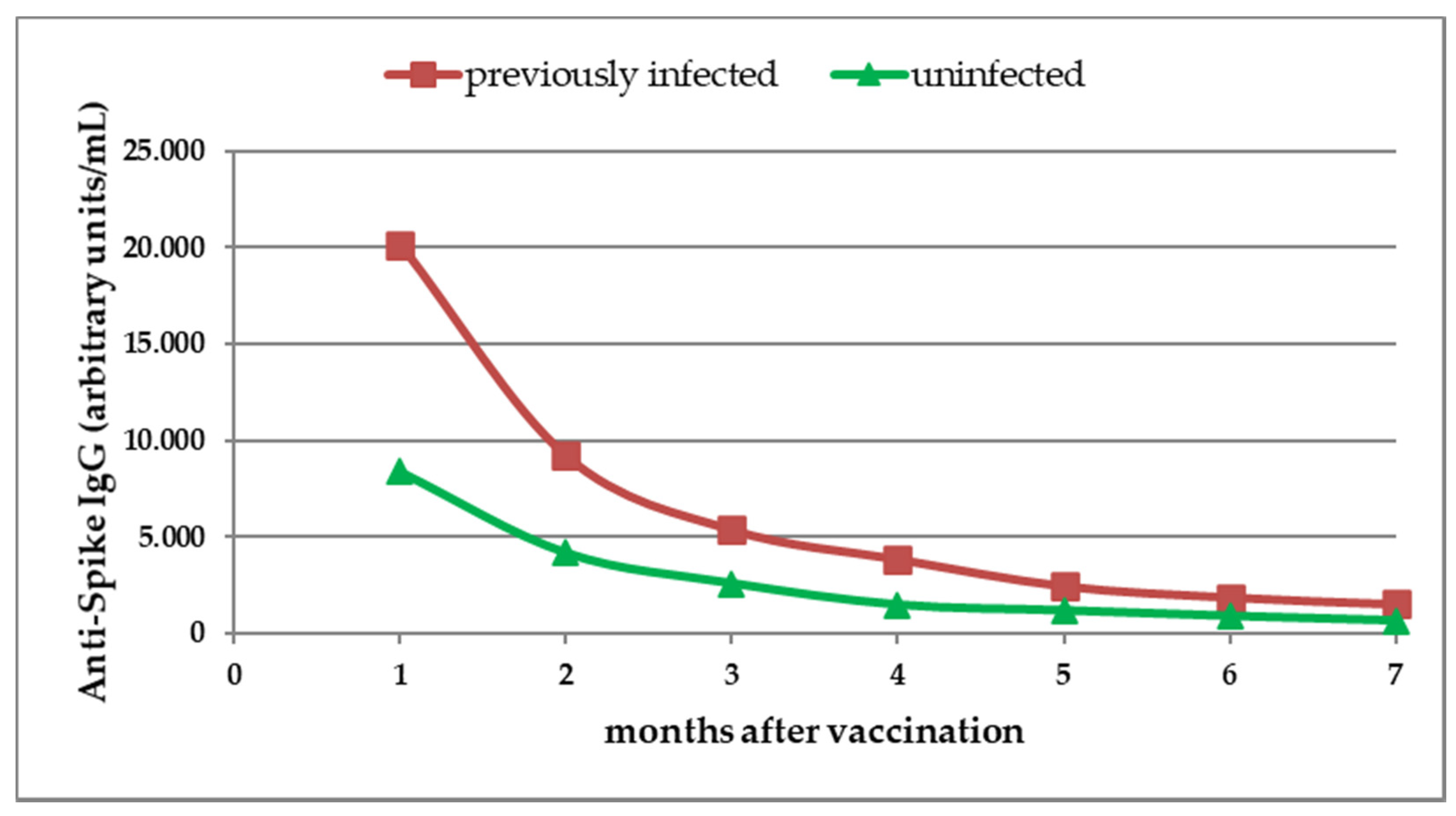
3.2. Antibody Response to BNT162b2 mRNA COVID-19 Vaccine
3.3. Antibody Response to Vaccine in Previously Infected Participants
3.4. Antibody Response to Vaccine in Uninfected Participants
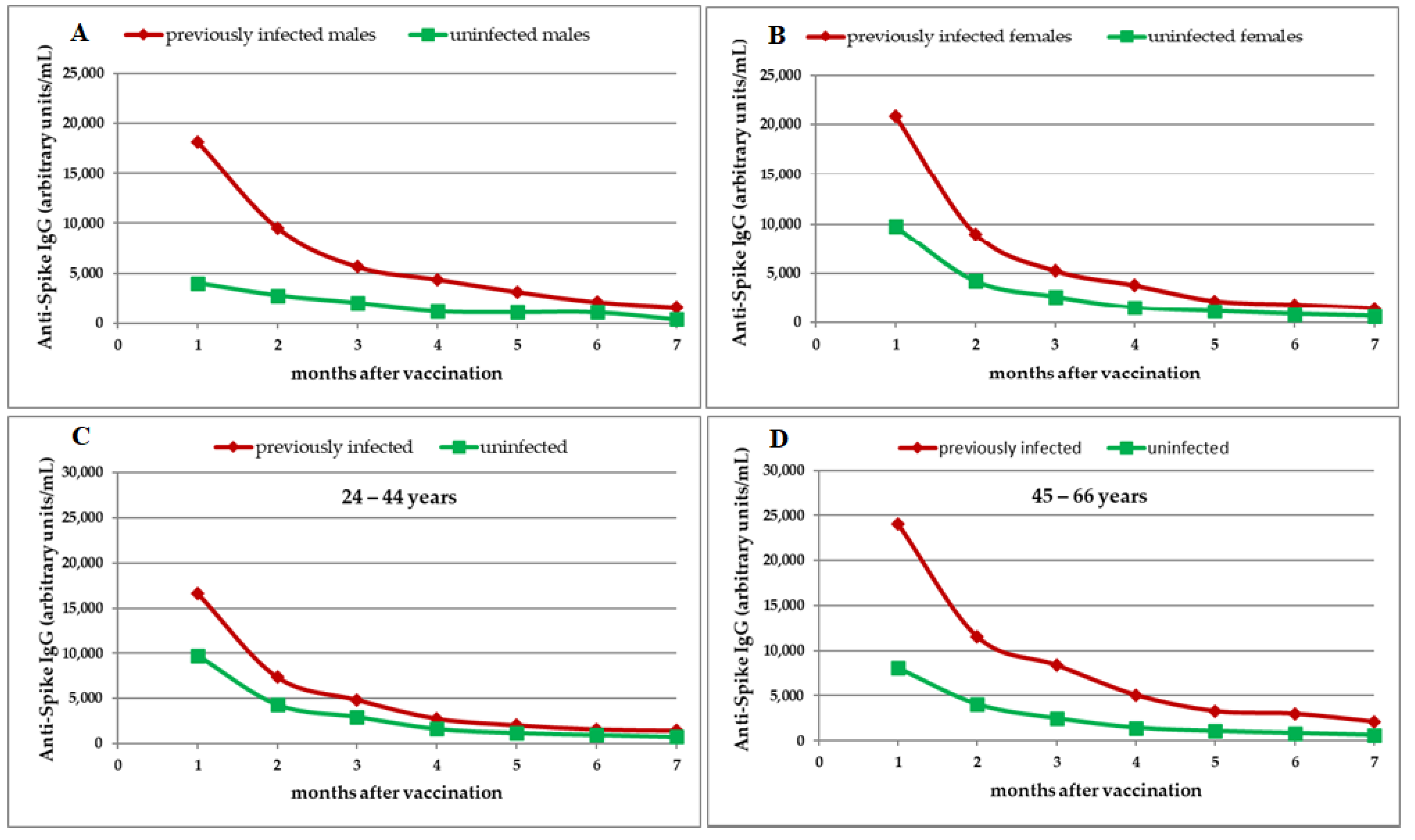
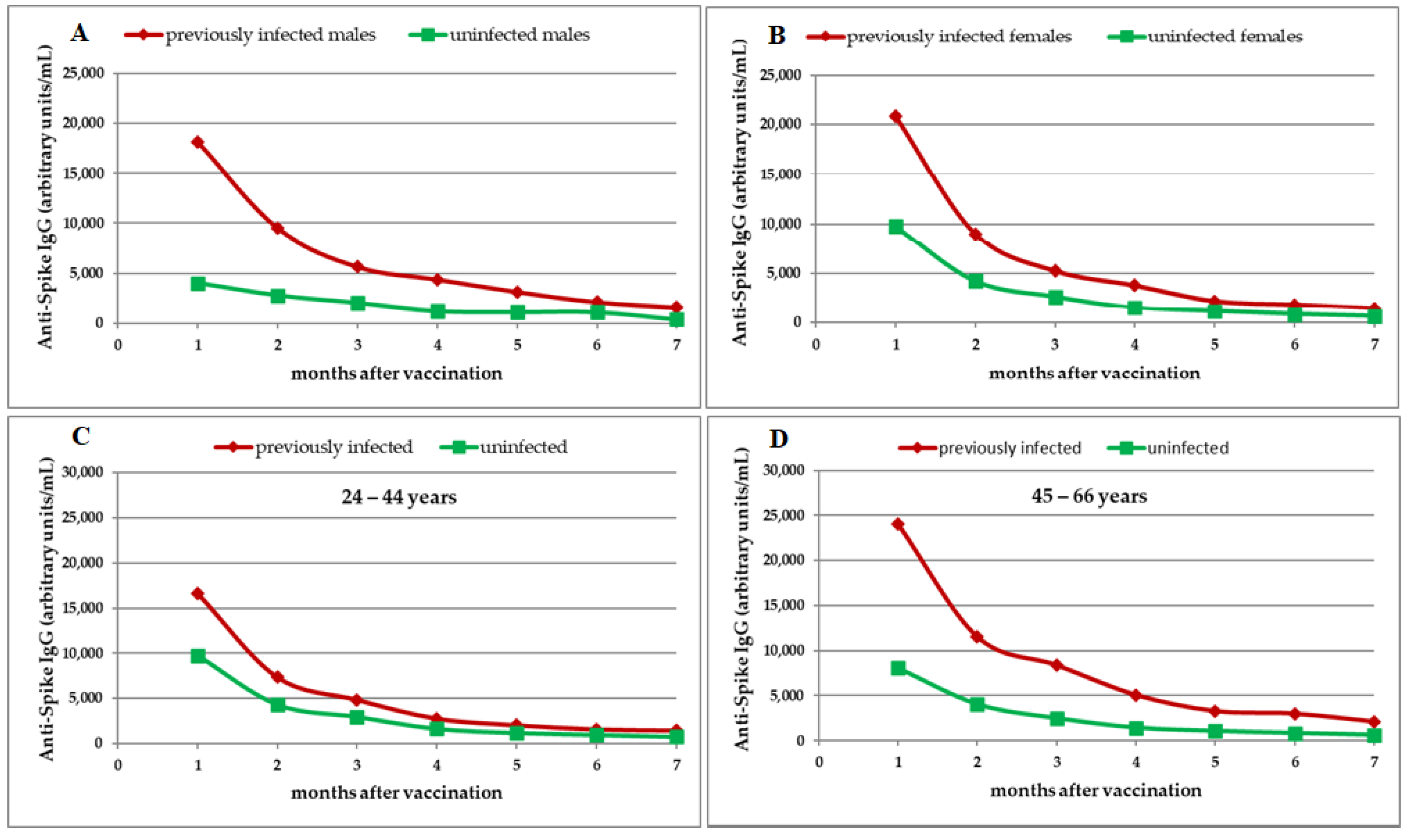
3.5. Comparison of IgGS Antibody Response to Vaccine between Previously Infected and Uninfected Participants According to Gender and Age Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Pfizer. Pfizer-BioNTech COVID-19 Vaccine (BNT162, PF-07302048). Vaccines and Related Biological Products Advisory Committee Briefing Document. Available online: https://www.fda.gov/media/144246/download (accessed on 9 October 2021).
- Oliver, S.E.; Gargano, J.W.; Marin, M.; Wallace, M.; Curran, K.G.; Chamberland, M.; McClung, N.; Campos-Outcalt, D.; Morgan, R.L.; Mbaeyi, S.; et al. The Advisory Committee on Immunization Practices’ Interim Recommendation for Use of Pfizer-BioNTech COVID-19 Vaccine—United States, December 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1922–1924. [Google Scholar] [CrossRef] [PubMed]
- Perkmann, T.; Perkmann-Nagele, N.; Koller, T.; Mucher, P.; Radakovics, A.; Marculescu, R.; Wolzt, M.; Wagner, O.F.; Binder, C.J.; Haslacher, H. Anti-Spike Protein Assays to Determine SARS-CoV-2 Antibody Levels: A Head-to-Head Comparison of Five Quantitative Assays. Microbiol. Spectr. 2021, 9, e0024721. [Google Scholar] [CrossRef] [PubMed]
- Poland, G.A.; Ovsyannikova, I.G.; Kennedy, R.B. SARS-CoV-2 immunity: Review and applications to phase 3 vaccine candidates. Lancet 2020, 396, 1595–1606. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. Vaccines and Related Biological Products Advisory Committee Briefing Document. BNT162b2 [COMIRNATY (COVID-19 Vaccine, mRNA)]. Evaluation of a Booster Dose (Third Dose). Available online: https://www.fda.gov/media/152161/download (accessed on 9 October 2021).
- Favresse, J.; Bayart, J.L.; Mullier, F.; Elsen, M.; Eucher, C.; Van Eeckhoudt, S.; Roy, T.; Wieers, G.; Laurent, C.; Dogné, J.M.; et al. Antibody titres decline 3-month post-vaccination with BNT162b2. Emerg. Microbes Infect. 2021, 10, 1495–1498. [Google Scholar] [CrossRef] [PubMed]
- Favresse, J.; Bayart, J.L.; Mullier, F.; Dogné, J.M.; Closset, M.; Douxfils, J. Early antibody response in health-care professionals after two doses of SARS-CoV-2 mRNA vaccine (BNT162b2). Clin. Microbiol. Infect. 2021, 27, 1351.e5–1351.e7. [Google Scholar] [CrossRef] [PubMed]
- Ebinger, J.E.; Fert-Bober, J.; Printsev, I.; Wu, M.; Sun, N.; Prostko, J.C.; Frias, E.C.; Stewart, J.L.; Van Eyk, J.E.; Braun, J.G.; et al. Antibody responses to the BNT162b2 mRNA vaccine in individuals previously infected with SARS-CoV-2. Nat. Med. 2021, 27, 981–984. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration. EUA Authorized Serology Test Performance. Available online: https://www.fda.gov/medical-devices/coronavirus-disease-2019-covid-19-emergency-use-authorizations-medical-devices/eua-authorized-serology-test-performance (accessed on 9 October 2021).
- U.S. Food and Drug Administration. FTD™ SARS-CoV-2. Available online: https://www.fda.gov/media/137690/download (accessed on 9 October 2021).
- Tretyn, A.; Szczepanek, J.; Skorupa, M.; Jarkiewicz-Tretyn, J.; Sandomierz, D.; Dejewska, J.; Ciechanowska, K.; Jarkiewicz-Tretyn, A.; Koper, W.; Pałgan, K. Differences in the Concentration of Anti-SARS-CoV-2 IgG Antibodies Post-COVID-19 Recovery or Post-Vaccination. Cells 2021, 10, 1952. [Google Scholar] [CrossRef] [PubMed]
- Krammer, F.; Srivastava, K.; Alshammary, H.; Amoako, A.A.; Awawda, M.H.; Beach, K.F.; Bermúdez-González, M.C.; Bielak, D.A.; Carreño, J.M.; Chernet, R.L.; et al. Antibody Responses in Seropositive Persons after a Single Dose of SARS-CoV-2 mRNA Vaccine. N. Engl. J. Med. 2021, 384, 1372–1374. [Google Scholar] [CrossRef] [PubMed]
- Prendecki, M.; Clarke, C.; Brown, J.; Cox, A.; Gleeson, S.; Guckian, M.; Randell, P.; Pria, A.D.; Lightstone, L.; Xu, X.N.; et al. Effect of previous SARS-CoV-2 infection on humoral and T-cell responses to single-dose BNT162b2 vaccine. Lancet 2021, 397, 1178–1181. [Google Scholar] [CrossRef]
- Blain, H.; Tuaillon, E.; Gamon, L.; Pisoni, A.; Miot, S.; Picot, M.C.; Bousquet, J. Spike Antibody Levels of Nursing Home Residents With or Without Prior COVID-19 3 Weeks After a Single BNT162b2 Vaccine Dose. JAMA 2021, 325, 1898–1899. [Google Scholar] [CrossRef] [PubMed]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef] [PubMed]
- L’Huillier, A.G.; Meyer, B.; Andrey, D.O.; Arm-Vernez, I.; Baggio, S.; Didierlaurent, A.; Eberhardt, C.S.; Eckerle, I.; Grasset-Salomon, C.; Huttner, A.; et al. Antibody persistence in the first 6 months following SARS-CoV-2 infection among hospital workers: A prospective longitudinal study. Clin. Microbiol. Infect. 2021, 27, 784.e1–784.e8. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.; Liu, M.; Li, Q.; Zheng, X.; Ai, W.; Gong, F.; Fan, J.; Liu, S.; Wang, X.; Luo, J. Dynamic changes and prevalence of SARS-CoV-2 IgG/IgM antibodies: Analysis of multiple factors. Int. J. Infect. Dis. 2021, 108, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Lau, E.H.Y.; Tsang, O.T.Y.; Hui, D.S.C.; Kwan, M.Y.W.; Chan, W.; Chiu, S.S.; Ko, R.L.W.; Chan, K.H.; Cheng, S.M.S.; Perera, R.A.P.; et al. Neutralizing antibody titers in SARS-CoV-2 infections. Nat. Commun. 2021, 12, 63. [Google Scholar] [CrossRef] [PubMed]
- Conlon, A.; Ashur, C.; Washer, L.; Eagle, K.A.; Hofmann Bowman, M.A. Impact of the influenza vaccine on COVID-19 infection rates and severity. Am. J. Infect. Control. 2021, 49, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Connors, J.; Bell, M.R.; Marcy, J.; Kutzler, M.; Haddad, E.K. The impact of immuno-aging on SARS-CoV-2 vaccine development. Geroscience 2021, 43, 31–51. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Time after Second Vaccine Dose | Previously Infected Participants | Uninfected Participants | p-Value |
|---|---|---|---|
| 1 month | 20,160.0 (8572.4; 32,247.2) | 8386.2 (4015.3; 13,374.1) | <0.001 |
| 2 months | 9196.4 (4197.1; 21,490.9) | 4159.7 (2170.9; 6205.3) | <0.001 |
| 3 months | 5357.6 (2830.2; 9806.7) | 2582.2 (1285.3; 4692.4) | <0.001 |
| 4 months | 3837.8 (2100.1; 9051.9) | 1459 (785.9; 2789.9) | <0.001 |
| 5 months | 2442.5 (1678; 5282.0) | 1160.3 (591.5; 1990.9) | <0.001 |
| 6 months | 1855.7 (1234.3; 3462.6) | 870.7 (480.8; 1566.1) | <0.001 |
| 7 months | 1501.4 (916.4; 2743.0) | 632.4 (385; 1151.8) | <0.001 |
| Time after 2nd Vaccine Dose | SARS-CoV-2 Anti-Spike IgG Antibody Test Results (AU/mL): Median (Interquartile Range) | |||||||
|---|---|---|---|---|---|---|---|---|
| Gender | Age Groups | |||||||
| Male | Female | 24–44 Years | 45–66 Years | |||||
| Previously Infected Participants | Uninfected Participants | Previously Infected Participants | Uninfected Participants | Previously Infected Participants | Uninfected Participants | Previously Infected Participants | Uninfected Participants | |
| 1 month | 18,110.0 (7823.8; 29,370.7) | 4015.3 (2967.4; 16,862.6) | 20,812.6 (8572.4; 34,575.2) | 9750.9 (6087.4; 13,231.3) | 16,629.7 (5365.5; 20,812.6) | 9760.3 (5587.7; 15,278.1) | 24,014.4 (9492.35; 40,000) | 8069.0 (3663.55; 13,169.9) |
| 2 months | 9506.6 (4043.95; 21,714.6) | 2781.7 (1563.9; 7177.8) | 9005.5 (4473.1; 20,102.3) | 4221.1 (2782.9; 6169.2) | 7377.0 (3248.2; 9701.9) | 4314.5 (2660.7; 7585.7) | 11,520.4 (5113.8; 27,542.9) | 4053.4 (2151.5; 6205.3) |
| 3 months | 5667.1 (2776.45; 12,044.0) | 2031.4 (661.5; 4974.0) | 5239.1 (3503.2; 9763.8) | 2645.0 (1747.2; 4262.6) | 4865.8 (1812; 5976.7) | 2953.7 (1500.3; 4899.0) | 8388.1 (3402.5; 21,722.95) | 2485.0 (1171.4; 4410.2) |
| 4 months | 4398.2 (2100.1; 9182.6) | 1240.8 (535.9; 4168.4) | 3772.0 (2089.7; 8541.7) | 1518.7 (897.25; 2648.1) | 2794.5 (1085.9; 3816.2) | 1625.6 (802.6; 3196.2) | 5083.1 (2414.4; 15,228.4) | 1439.8 (720.4; 2714.7) |
| 5 months | 3144.2 (1225.35; 7221.5) | 1154.4 (429.1; 3114.7) | 2212.1 (1826.1; 5282.0) | 1162.1 (594.9; 1798.3) | 2063.8 (1084.2; 2488.1) | 1171.4 (592.2; 1924.1) | 3291.7 (1796.9; 14,634.9) | 1062.0 (590.8; 2110.3) |
| 6 months | 2122.3 (1131.6; 3277.4) | 1140.9 (376.25; 2520.55) | 1855.7 (1521.2; 5517.7) | 856.5 (588.4; 1256.4) | 1614.5 (533.8; 2535.2) | 955.9 (477.95; 1481.5) | 3005.2 (1615.3; 12,451.0) | 836.3 (480.8; 1566.1) |
| 7 months | 1590.2 (916.4; 2875.5) | 418.0 (189.3; 1160.6) | 1501.4 (1131.8; 2668.1) | 651.3 (440.2; 1151.8) | 1468.2 (724.2; 2119.1) | 737.3 (397.7; 1971.1) | 2126.3 (1071.1; 5328.0) | 618.2 (311.3; 1044.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olariu, T.R.; Ursoniu, S.; Marincu, I.; Lupu, M.A. Dynamics of Antibody Response to BNT162b2 mRNA COVID-19 Vaccine: A 7-Month Follow-Up Study. Medicina 2021, 57, 1330. https://doi.org/10.3390/medicina57121330
Olariu TR, Ursoniu S, Marincu I, Lupu MA. Dynamics of Antibody Response to BNT162b2 mRNA COVID-19 Vaccine: A 7-Month Follow-Up Study. Medicina. 2021; 57(12):1330. https://doi.org/10.3390/medicina57121330
Chicago/Turabian StyleOlariu, Tudor Rares, Sorin Ursoniu, Iosif Marincu, and Maria Alina Lupu. 2021. "Dynamics of Antibody Response to BNT162b2 mRNA COVID-19 Vaccine: A 7-Month Follow-Up Study" Medicina 57, no. 12: 1330. https://doi.org/10.3390/medicina57121330
APA StyleOlariu, T. R., Ursoniu, S., Marincu, I., & Lupu, M. A. (2021). Dynamics of Antibody Response to BNT162b2 mRNA COVID-19 Vaccine: A 7-Month Follow-Up Study. Medicina, 57(12), 1330. https://doi.org/10.3390/medicina57121330