
Blood Cadmium Levels and Oxygen Desaturation during the 6-Minute Walk Test in Patients with Chronic Obstructive Pulmonary Disease

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
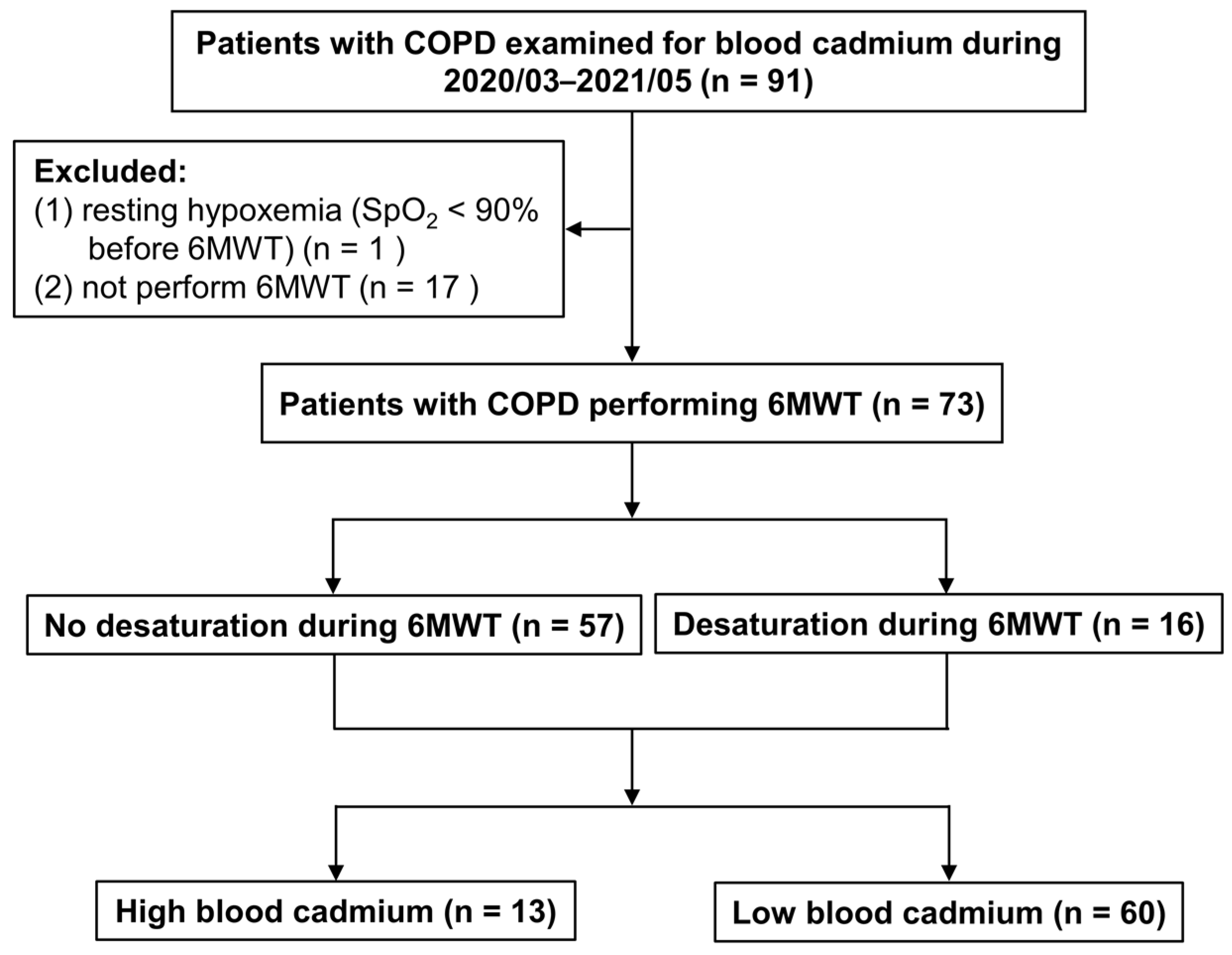
2.1. Study Design and Patients’ Inclusion
2.2. Definitions
2.3. Data Collection
2.4. Measurement of Blood Cadmium Levels
2.5. Statistical Analysis
3. Results
3.1. Study Patients
3.2. Comparisons of COPD Patients with or without Desaturation during the 6MWT
3.3. Comparing Patients with High- and Low-Blood Cadmium Levels
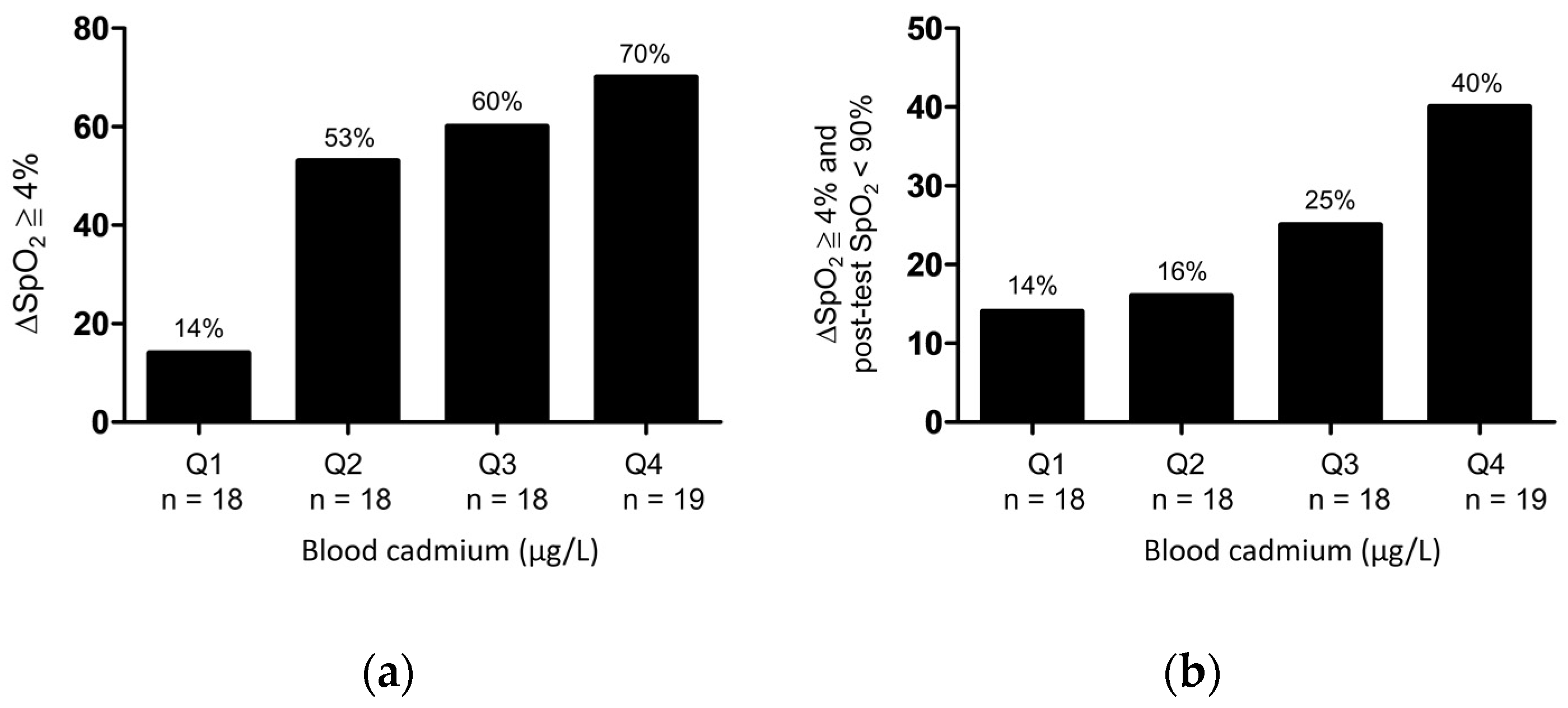
3.4. Correlation between Blood Cadmium Levels and Desaturation during the 6MWT
3.5. Factors Associated with Desaturation during the 6MWT in Patients with COPD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Halpin, D.M.G.; Criner, G.J.; Papi, A.; Singh, D.; Anzueto, A.; Martinez, F.J.; Agusti, A.A.; Vogelmeier, C.F. Global Initiative for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease. The 2020 GOLD Science Committee Report on COVID-19 and Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2021, 203, 24–36. [Google Scholar] [CrossRef]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2017, 195, 557–582. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Agusti, A.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Criner, G.J.; Frith, P.; Halpin, D.M.G.; Han, M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease: The GOLD science committee report 2019. Eur. Respir. J. 2019, 53, 1900164. [Google Scholar] [CrossRef]
- Ganguly, K.; Levänen, B.; Palmberg, L.; Åkesson, A.; Lindén, A. Cadmium in tobacco smokers: A neglected link to lung disease? Eur. Respir. Rev. 2018, 27, 170122. [Google Scholar] [CrossRef] [PubMed]
- Genchi, G.; Sinicropi, M.S.; Lauria, G.; Carocci, A.; Catalano, A. The Effects of Cadmium Toxicity. Int. J. Environ. Res. Public Health. 2020, 17, 3782. [Google Scholar] [CrossRef]
- Richter, P.; Faroon, O.; Pappas, R.S. Cadmium and Cadmium/Zinc Ratios and Tobacco-Related Morbidities. Int. J. Environ. Res. Public Health. 2017, 14, 1154. [Google Scholar] [CrossRef] [Green Version]
- Waatevik, M.; Johannessen, A.; Gomez, R.F.; Aanerud, M.; Hardie, J.A.; Bakke, P.S.; Eagan, T.M.L. Oxygen desaturation in 6-min walk test is a risk factor for adverse outcomes in COPD. Eur. Respir. J. 2016, 48, 82–91. [Google Scholar] [CrossRef] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Liu, S.F.; Chin, C.H.; Tseng, C.W.; Chen, Y.C.; Kuo, H.C. Exertional Desaturation Has Higher Mortality Than Non-Desaturation in COPD. Medicina 2021, 57, 1110. [Google Scholar] [CrossRef] [PubMed]
- Gurbani, N.; Figueira Gonçalves, J.M.; García Bello, M.Á.; García-Talavera, I.; Afonso Díaz, A. Prognostic ability of the distance-saturation product in the 6-minute walk test in patients with chronic obstructive pulmonary disease. Clin. Respir. J. 2020, 14, 364–369. [Google Scholar] [CrossRef]
- Celli, B.; Tetzlaff, K.; Criner, G.; Polkey, M.I.; Sciurba, F.; Casaburi, R.; Tal-Singer, R.; Kawata, A.; Merrill, D.; Rennard, S.; et al. The 6-Minute-Walk Distance Test as a Chronic Obstructive Pulmonary Disease Stratification Tool. Insights from the COPD Biomarker Qualification Consortium. Am. J. Respir. Crit. Care Med. 2016, 194, 1483–1493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takigawa, N.; Tada, A.; Soda, R.; Date, H.; Yamashita, M.; Endo, S.; Takahashi, S.; Kawata, N.; Shibayama, T.; Hamada, N.; et al. Distance and oxygen desaturation in 6-min walk test predict prognosis in COPD patients. Respir. Med. 2007, 101, 561–567. [Google Scholar] [CrossRef] [Green Version]
- Casanova, C.; Cote, C.; Marin, J.M.; Pinto-Plata, V.; de Torres, J.P.; Aguirre-Jaíme, A.; Vassaux, C.; Celli, B.R. Distance and oxygen desaturation during the 6-min walk test as predictors of long-term mortality in patients with COPD. Chest 2008, 134, 746–752. [Google Scholar] [CrossRef]
- Lettieri, C.J.; Nathan, S.D.; Browning, R.F.; Barnett, S.D.; Ahmad, S.; Shorr, A.F. The distance-saturation product predicts mortality in idiopathic pulmonary fibrosis. Respir. Med. 2006, 100, 1734–1741. [Google Scholar] [CrossRef] [Green Version]
- Gupta, R.; Ruppel, G.L.; Espiritu, J.R.D. Exercise-Induced Oxygen Desaturation during the 6-Minute Walk Test. Med. Sci. 2020, 8, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrianopoulos, V.; Celli, B.R.; Franssen, F.M.; Pinto-Plata, V.M.; Calverley, P.M.; Vanfleteren, L.E.; Vogiatzis, I.; Vestbo, J.; Agusti, A.; Bakke, P.S.; et al. Determinants of exercise-induced oxygen desaturation including pulmonary emphysema in COPD: Results from the ECLIPSE study. Respir. Med. 2016, 119, 87–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutchinson, D.; Müller, J.; McCarthy, J.E.; Gun’ko, Y.K.; Verma, N.K.; Bi, X.; Di Cristo, L.; Kickham, L.; Movia, D.; Prina-Mello, A.; et al. Cadmium nanoparticles citrullinate cytokeratins within lung epithelial cells: Cadmium as a potential cause of citrullination in chronic obstructive pulmonary disease. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 441–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutchinson, D. Cadmium lung adsorption, citrullination and an enhanced risk of COPD. Eur. Respir. Rev. 2018, 27, 180054. [Google Scholar] [CrossRef] [Green Version]
- Caramori, G.; Ruggeri, P.; Di Stefano, A.; Mumby, S.; Girbino, G.; Adcock, I.M.; Kirkham, P. Autoimmunity and COPD: Clinical Implications. Chest 2018, 153, 1424–1431. [Google Scholar] [CrossRef] [PubMed]
- Gergianaki, I.; Tsiligianni, I. Chronic obstructive pulmonary disease and rheumatic diseases: A systematic review on a neglected comorbidity. J. Comorb. 2019, 9, 2235042X18820209. [Google Scholar] [CrossRef]
- Joshua, V.; Hensvold, A.H.; Reynisdottir, G.; Hansson, M.; Cornillet, M.; Nogueira, L.; Serre, G.; Nyren, S.; Karimi, R.; Eklund, A.; et al. Association between number and type of different ACPA fine specificities with lung abnormalities in early, untreated rheumatoid arthritis. RMD Open 2020, 6, e001278. [Google Scholar] [CrossRef]
- Byrne, R.; Todd, I.; Tighe, P.J.; Fairclough, L.C. Autoantibodies in chronic obstructive pulmonary disease: A systematic review. Immunol. Lett. 2019, 214, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Wen, L.; Krauss-Etschmann, S.; Petersen, F.; Yu, X. Autoantibodies in Chronic Obstructive Pulmonary Disease. Front. Immunol. 2018, 9, 66. [Google Scholar] [CrossRef]
- Lytras, T.; Beckmeyer-Borowko, A.; Kogevinas, M.; Kromhout, H.; Carsin, A.E.; Antó, J.M.; Bentouhami, H.; Weyler, J.; Heinrich, J.; Nowak, D.; et al. Cumulative Occupational Exposures and Lung-Function Decline in Two Large General-Population Cohorts. Ann. Am. Thorac. Soc. 2021, 18, 238–246. [Google Scholar] [CrossRef]
- Pollard, K.M. Perspective: The Lung, Particles, Fibers, Nanomaterials, and Autoimmunity. Front. Immunol. 2020, 11, 587136. [Google Scholar] [CrossRef]
- Wang, Z.; Sun, Y.; Yao, W.; Ba, Q.; Wang, H. Effects of Cadmium Exposure on the Immune System and Immunoregulation. Front. Immunol. 2021, 12, 695484. [Google Scholar] [CrossRef]
- Kim, J.; Song, H.; Heo, H.R.; Kim, J.W.; Kim, H.R.; Hong, Y.; Yang, S.R.; Han, S.S.; Lee, S.J.; Kim, W.J.; et al. Cadmium-induced ER stress and inflammation are mediated through C/EBP-DDIT3 signaling in human bronchial epithelial cells. Exp. Mol. Med. 2017, 49, e372. [Google Scholar] [CrossRef]
- Torén, K.; Olin, A.C.; Johnsson, Å.; Vikgren, J.; Forsgard, N.; Bergström, G.; Sallsten, G.; Barregård, L. The association between cadmium exposure and chronic airflow limitation and emphysema: The Swedish CArdioPulmonary BioImage Study (SCAPIS pilot). Eur. Respir. J. 2019, 54, 1900960. [Google Scholar] [CrossRef] [PubMed]
- Rokadia, H.K.; Agarwal, S. Serum heavy metals and obstructive lung disease: Results from the National Health and Nutrition Examination Survey. Chest 2013, 143, 388–397. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, D.E.; Ciavaglia, C.E.; Neder, J.A. When obesity and chronic obstructive pulmonary disease collide. Physiological and clinical consequences. Ann. Am. Thorac. Soc. 2014, 11, 635–644. [Google Scholar] [CrossRef] [PubMed]
- Lambert, A.A.; Putcha, N.; Drummond, M.B.; Boriek, A.M.; Hanania, N.A.; Kim, V.; Kinney, G.L.; McDonald, M.N.; Brigham, E.P.; Wise, R.A.; et al. COPDGene Investigators. Obesity Is Associated With Increased Morbidity in Moderate to Severe COPD. Chest 2017, 151, 68–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bautista, J.; Ehsan, M.; Normandin, E.; Zuwallack, R.; Lahiri, B. Physiologic responses during the six minute walk test in obese and non-obese COPD patients. Respir. Med. 2011, 105, 1189–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Variables | Controls (n = 50) | COPD | p | ||
|---|---|---|---|---|---|
| All (n = 73) | No-Desaturation (n = 57) | Desaturation (n = 16) | |||
| Age (years) | 53.6 ± 16.3 | 70.6 ± 9.1 | 71.0 ± 9.4 | 69.3 ± 8.1 | 0.491 |
| Male (gender) | 70 (95.9%) | 55 (96.5%) | 15 (93.8%) | 0.530 | |
| Body weight (kg) | 64.3 ± 12.7 | 61.8 ± 10.4 | 73.3 ± 16.4 | 0.030 | |
| Body mass index (kg/m2) | 23.9 ± 4.2 | 23.1 ± 3.6 | 26.5 ± 4.9 | 0.009 | |
| Hypertension | 28 (38.4%) | 24 (42.1%) | 4 (25%) | 0.257 | |
| Diabetes mellitus | 18 (24.7%) | 13 (22.8%) | 5 (31.3%) | 0.489 | |
| Coronary artery disease | 5 (6.8%) | 4 (7%) | 1 (6.3%) | 1.000 | |
| Congestion heart failure | 5 (6.8%) | 4 (7%) | 1 (6.3%) | 1.000 | |
| Chronic liver disease | 4 (5.5%) | 2 (3.5%) | 2 (12.5%) | 0.207 | |
| Chronic kidney disease | 6 (8.2%) | 6 (10.5%) | 0 | 0.328 | |
| Malignancies | 10 (13.7%) | 8 (14%) | 2 (12.5%) | 1.000 | |
| Osteoporosis | 4 (5.5%) | 3 (5.3%) | 1 (6.3%) | 1.000 | |
| Hemoglobin (g/dL) | 14.0 ± 1.9 | 13.7 ± 2.0 | 15.3 ± 1.3 | 0.003 | |
| Serum creatinine (mg/dL) | 1.0 ± 0.4 | 1.0 ± 0.3 | 1.0 ± 0.5 | 0.696 | |
| Blood cadmium (μg/L) | 1.03 ± 0.56 | 1.29 ± 0.67 | 1.14 ± 0.46 | 1.81 ± 0.99 | 0.017 |
| Smoking status | |||||
| Never | 6 (8.2%) | 4 (7.1%) | 2 (12.5%) | 0.606 | |
| Former | 43 (58.9%) | 34 (59.6%) | 9 (56.3%) | 0.807 | |
| Current | 24 (32.9%) | 19 (33.3%) | 5 (31.2%) | 0.875 | |
| FVC (L) | 2.4 ± 0.7 | 2.5 ± 0.7 | 2.1 ± 0.6 | 0.057 | |
| FVC (%) | 73.7 ± 18.9 | 76.3 ± 19.2 | 64.4 ± 14.6 | 0.026 | |
| FEV1 (L) | 1.4 ± 0.5 | 1.4 ± 0.5 | 1.1 ± 0.3 | 0.003 | |
| FEV1 (%) | 54.5 ± 17.7 | 57.7 ± 18.1 | 42.9 ± 9.5 | <0.001 | |
| FEV1/FVC (%) | 56.6 ± 9.8 | 57.5 ± 9.7 | 53.2 ± 9.8 | 0.121 | |
| GOLD classification | |||||
| Stage I | 7 (9.6%) | 7 (12.3%) | 0 | 0.335 | |
| Stage II | 32 (43.8%) | 29 (50.9%) | 3 (18.8%) | 0.025 | |
| Stage III | 32 (43.8%) | 20 (35.1%) | 12 (75%) | 0.009 | |
| Stage IV | 2 (2.8%) | 1 (1.7%) | 1 (6.2%) | 0.393 | |
| Number of COPD exacerbations in the previous year | |||||
| 0–1 | 7 (9.6%) | 7 (12.3%) | 0 | 0.335 | |
| ≥2 | 4 (5.5%) | 3 (5.3%) | 1 (6.3%) | 1.000 | |
| Six-minute walk test | |||||
| Pre-test saturation (%) | 94.9 ± 2.7 | 95.6 ± 1.9 | 92.6 ± 3.8 | <0.001 | |
| Post-test saturation (%) | 90.9 ± 4.3 | 92.6 ± 2.3 | 84.8 ± 4.3 | <0.001 | |
| Desaturation (%) | 4.0 ± 3.1 | 2.9 ± 2.2 | 7.9 ± 3.1 | <0.001 | |
| Pre-test heart rate (bpm) | 86.4 ± 18.6 | 86.3 ± 19.4 | 86.6 ± 16.2 | 0.956 | |
| Post-test heart rate (bpm) | 104.3 ± 13.6 | 103.7 ± 13.7 | 106.5 ± 13.6 | 0.466 | |
| Distance (m) | 412.6 ± 99.1 | 416.2 ± 103.8 | 399.6 ± 82.2 | 0.558 | |
| Distance <350 m | 14 (19.2%) | 9 (15.8%) | 5 (31.3%) | 0.278 | |
| Distance saturation product (m%) | 378.4 ± 86.0 | 390.1 ± 86.3 | 339.1 ± 74.3 | 0.036 | |
| Variables | High (>1.75 μg/L) n = 13 | Low (≤1.75 μg/L) n = 60 | p |
|---|---|---|---|
| Age (years) | 68.3 ± 7.3 | 71.2 ± 9.4 | 0.310 |
| Male (gender) | 13 (100%) | 57 (95%) | 1.000 |
| Body weight (kg) | 66.3 ± 17.0 | 63.6 ± 11.8 | 0.629 |
| Body mass index (kg/m2) | 25.4 ± 6.8 | 23.6 ± 3.5 | 0.457 |
| Hypertension | 3 (23.1%) | 25 (41.7%) | 0.346 |
| Diabetes mellitus | 4 (30.8%) | 14 (23.3%) | 0.723 |
| Coronary artery disease | 0 | 5 (8.3%) | 0.578 |
| Congestive heart failure | 1 (7.7%) | 4 (6.7%) | 1.000 |
| Chronic liver disease | 1 (7.7%) | 3 (5%) | 0.552 |
| Chronic kidney disease | 1 (7.7%) | 5 (8.3%) | 1.000 |
| Malignancies | 4 (30.8%) | 6 (10%) | 0.070 |
| Osteoporosis | 0 | 4 (6.7%) | 1.000 |
| Hemoglobin (g/dL) | 14.7 ± 1.6 | 13.9 ± 2.0 | 0.182 |
| Serum creatinine (mg/dL) | 1.1 ± 0.5 | 1.0 ± 0.3 | 0.323 |
| Blood cadmium (μg/L) | 2.4 ± 0.6 | 1.0 ± 0.3 | <0.001 |
| Smoking status | |||
| Never | 0 | 6 (10%) | 0.583 |
| Former | 7 (53.8%) | 36 (60%) | 0.683 |
| Current | 6 (46.2%) | 18 (30%) | 0.261 |
| FVC (L) | 2.1 ± 0.5 | 2.5 ± 0.7 | 0.110 |
| FVC (%) | 62.8 ± 15.7 | 76.0 ± 18.8 | 0.021 |
| FEV1 (L) | 1.0 ± 0.2 | 1.4 ± 0.5 | <0.001 |
| FEV1 (%) | 44.5 ± 17.0 | 56.6 ± 17.2 | 0.023 |
| FEV1/FVC (%) | 51.1 ± 12.6 | 57.8 ± 8.8 | 0.025 |
| GOLD classification | |||
| Stage I | 1 (7.7%) | 6 (10%) | 1.000 |
| Stage II | 2 (15.4%) | 30 (50%) | 0.031 |
| Stage III | 8 (61.5%) | 23 (38.3%) | 0.215 |
| Stage IV | 2 (15.4%) | 1 (1.7%) | 0.080 |
| Number of COPD exacerbations in the previous year | |||
| 0–1 | 2 (15.4%) | 5 (8.3%) | 0.601 |
| ≥2 | 1 (7.7%) | 3 (5%) | 0.552 |
| Six-minute walk test | |||
| Pre-test saturation (%) | 93.4 ± 4.6 | 95.3 ± 2.0 | 0.170 |
| Post-test saturation (%) | 87.5 ± 6.0 | 91.7 ± 3.5 | 0.029 |
| Desaturation (%) | 5.9 ± 3.5 | 3.6 ± 3.0 | 0.019 |
| Desaturation ≥ 4% | 10 (76.9%) | 28 (46.7%) | 0.048 |
| Post-test saturation < 90% | 7 (53.8%) | 10 (16.7%) | 0.004 |
| Pre-test heart rate (bpm) | 92.0 ± 10.9 | 85.2 ± 19.8 | 0.234 |
| Post-test heart rate (bpm) | 109.9 ± 7.6 | 103.1 ± 14.4 | 0.020 |
| Distance (m) | 378.8 ± 70.8 | 435.6 ± 87.4 | 0.033 |
| Distance < 350 m | 4 (30.8%) | 10 (16.7%) | 0.258 |
| Distance saturation product (m%) | 332.0 ± 70.4 | 395.9 ± 79.4 | 0.010 |
| Factors | Odds Ratio (95% CI) | p |
|---|---|---|
| Univariate analysis | ||
| Body weight (kg) | 1.075 (1.018–1.135) | 0.009 |
| Body mass index (kg/m2) | 1.225 (1.040–1.443) | 0.015 |
| Chronic liver disease | 3.929 (0.508–30.392) | 0.190 |
| Hemoglobin (g/dL) | 1.857 (1.186–2.906) | 0.007 |
| Blood cadmium concentration (μg/L) | 4.188 (1.650–10.631) | 0.003 |
| FVC (%) | 0.960 (0.925–0.996) | 0.031 |
| FEV1 (%) | 0.934 (0.889–0.981) | 0.006 |
| FEV1/FVC (%) | 0.014 (0.002–3.396) | 0.127 |
| Pre-test SpO2 (%) | 0.588 (0.426–0.813) | 0.001 |
| Multivariate analysis | ||
| Body weight (kg) (with each kg increase) | 1.114 (1.002–1.239) | 0.046 |
| Blood cadmium concentration (μg/L) (with each μg/L increase) | 12.849 (1.168–141.329) | 0.037 |
| Pre-test SpO2 (%) (with each unit (%) increase) | 0.413 (0.192–0.890) | 0.024 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, L.-C.; Hsu, P.-C.; Yen, T.-H.; Kuo, S.C.-H.; Fang, Y.-F.; Lo, Y.-L.; Lin, S.-M.; Yang, C.-T.; Lee, C.-S. Blood Cadmium Levels and Oxygen Desaturation during the 6-Minute Walk Test in Patients with Chronic Obstructive Pulmonary Disease. Medicina 2021, 57, 1160. https://doi.org/10.3390/medicina57111160
Chiu L-C, Hsu P-C, Yen T-H, Kuo SC-H, Fang Y-F, Lo Y-L, Lin S-M, Yang C-T, Lee C-S. Blood Cadmium Levels and Oxygen Desaturation during the 6-Minute Walk Test in Patients with Chronic Obstructive Pulmonary Disease. Medicina. 2021; 57(11):1160. https://doi.org/10.3390/medicina57111160
Chicago/Turabian StyleChiu, Li-Chung, Ping-Chih Hsu, Tzung-Hai Yen, Scott Chih-Hsi Kuo, Yueh-Fu Fang, Yu-Lun Lo, Shu-Min Lin, Cheng-Ta Yang, and Chung-Shu Lee. 2021. "Blood Cadmium Levels and Oxygen Desaturation during the 6-Minute Walk Test in Patients with Chronic Obstructive Pulmonary Disease" Medicina 57, no. 11: 1160. https://doi.org/10.3390/medicina57111160
APA StyleChiu, L.-C., Hsu, P.-C., Yen, T.-H., Kuo, S. C.-H., Fang, Y.-F., Lo, Y.-L., Lin, S.-M., Yang, C.-T., & Lee, C.-S. (2021). Blood Cadmium Levels and Oxygen Desaturation during the 6-Minute Walk Test in Patients with Chronic Obstructive Pulmonary Disease. Medicina, 57(11), 1160. https://doi.org/10.3390/medicina57111160