Trends in Mortality Rates of Corpus Uteri and Ovarian Cancer in Lithuania, 1987–2016

Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Analytic Methods
3. Results
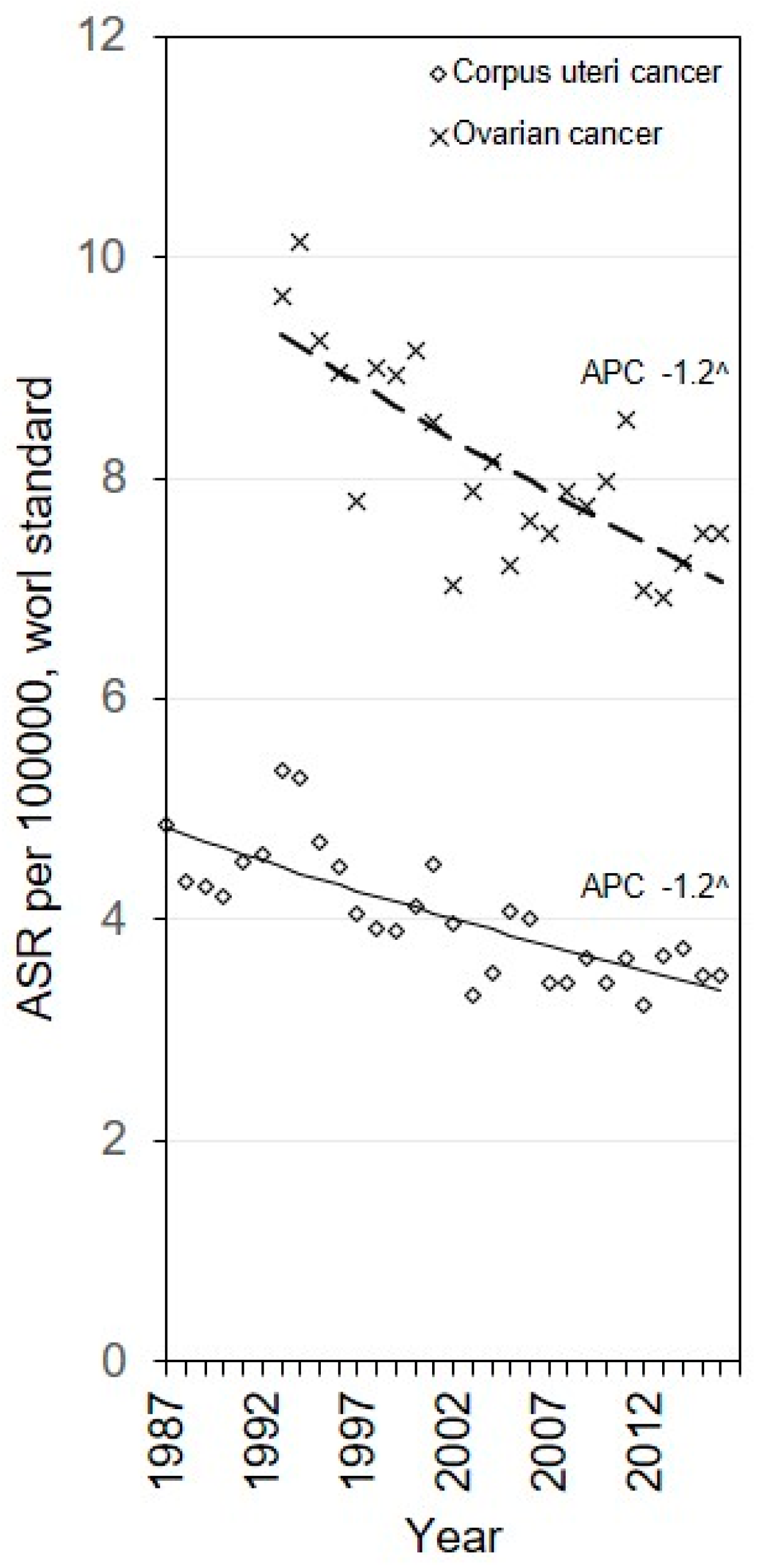
3.1. Age Standardized Mortality
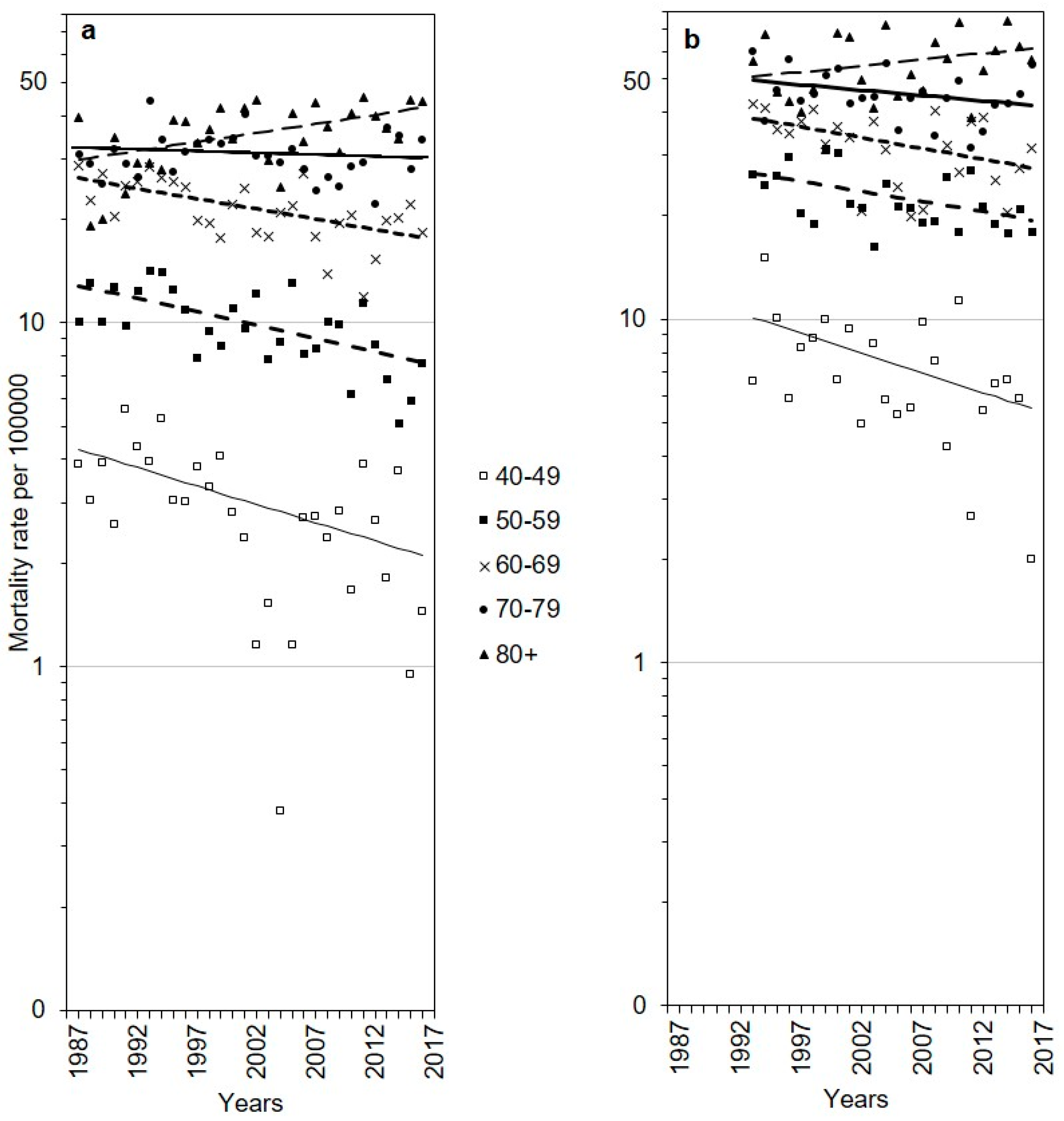
3.2. Age-Specific Trends
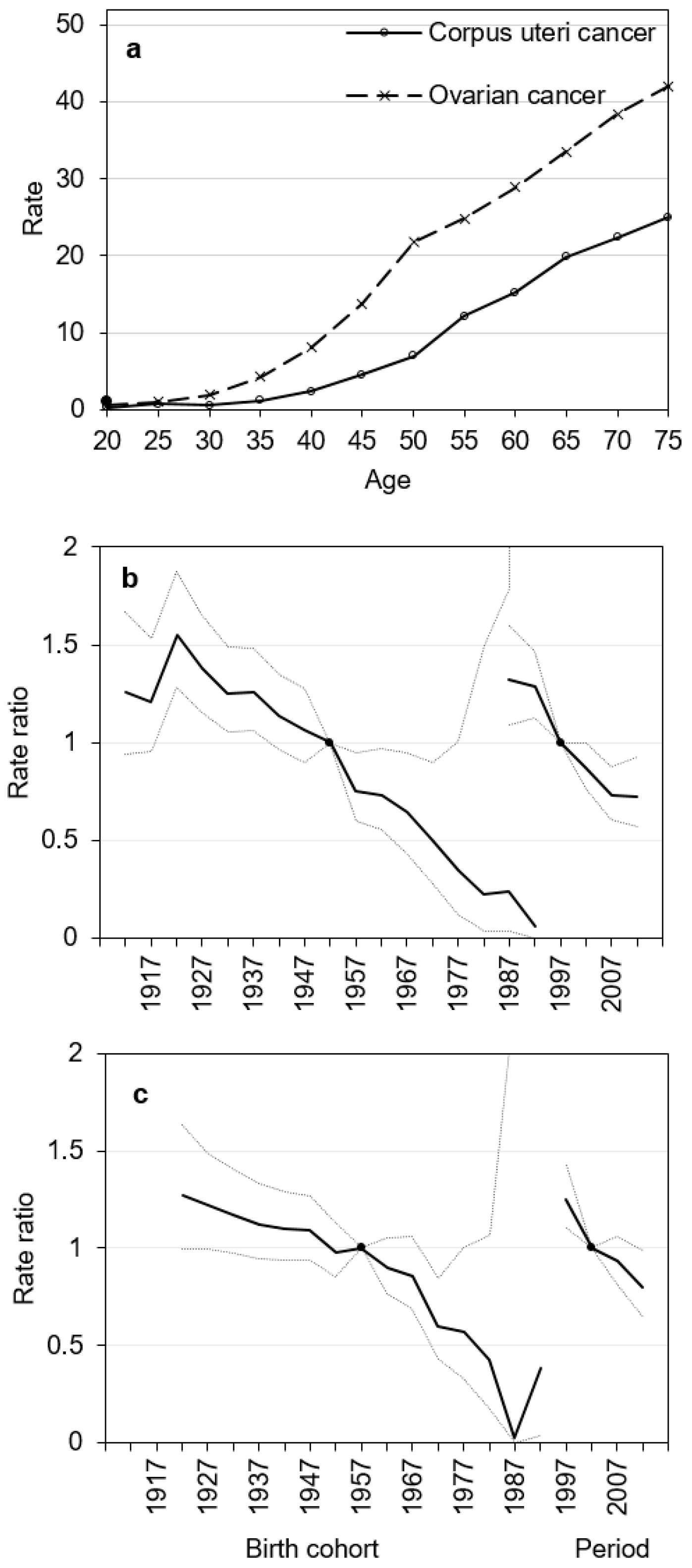
3.3. Age–Period–Cohort Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, N.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2014, 136. [Google Scholar] [CrossRef] [PubMed]
- Reid, B.M.; Permuth, J.B.; Sellers, T.A. Epidemiology of ovarian cancer: A review. Cancer Biol. Med. 2017, 14, 9–32. [Google Scholar] [CrossRef] [PubMed]
- Weiderpass, E.; Antoine, J.; Bray, F.; Oh, J.-K.; Arbyn, M. Trends in corpus uteri cancer mortality in member states of the European Union. Eur. J. Cancer 2014, 50, 1675–1684. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Statistical Information System WHO Mortality Database. Available online: http://www.who.int/healthinfo/mortality_data/en/ (accessed on 2 June 2020).
- Doll, R.; Payne, P.; Waterhouse, J. Cancer Incidence in Five Continents: A Technical Report; Springer-Verlag: Berlin, Germany, 1966. [Google Scholar]
- National Cancer Institute. Joinpoint Regression Program Version 4.5.0.1. Bethesda (MD): National Cancer Institute; 2017 June. Available online: https://surveillance.cancer.gov/joinpoint/ (accessed on 7 November 2019).
- Rosenberg, P.S.; Check, D.P.; Anderson, W.F. A Web Tool for Age-Period-Cohort Analysis of Cancer Incidence and Mortality Rates. Cancer Epidemiol. Biomark. Prev. 2014, 23, 2296–2302. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, A.Ø.; Schledermann, D.; Nyvang, G.-B.; Mogensen, O.; Herrstedt, J.; on behalf of the Academy of Geriatric Cancer Research (AgeCare). Trends in gynecologic cancer among elderly women in Denmark, 1980–2012. Acta Oncol. 2016, 55, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Czerw, A.; Banas, T.; Juszczyk, G.; Pitynski, K.; Nieweglowska, D.; Ludwin, A. Incidence and mortality rates in breast, corpus uteri, and ovarian cancers in Poland (1980–2013): An analysis of population-based data in relation to socio-economic changes. OncoTargets Ther. 2016, 9, 5521–5530. [Google Scholar] [CrossRef] [PubMed]
- Ojamaa, K.; Veerus, P.; Baburin, A.; Everaus, H.; Innos, K. Increasing incidence and survival of corpus uteri cancer in Estonia over the past two decades. Cancer Epidemiol. 2019, 62, 101566. [Google Scholar] [CrossRef] [PubMed]
- Henley, J.; Ward, E.M.; Scott, S.; Ma, J.; Anderson, R.N.; Bs, A.U.F.; Thomas, C.C.; Islami, F.; Weir, H.K.; Lewis, D.R.; et al. Annual report to the nation on the status of cancer, part I: National cancer statistics. Cancer 2020, 126, 2225–2249. [Google Scholar] [CrossRef] [PubMed]
- Purdie, D.M.; Green, A.C. Epidemiology of endometrial cancer. Best Pr. Res. Clin. Obstet. Gynaecol. 2001, 15, 341–354. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.; Peralta, M.; Naia, A.; Loureiro, N.; de Matos, M.G. Prevalence of adult overweight and obesity in 20 European countries, 2014. Eur. J. Public Health 2017, 28, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Kriaucioniene, V.; Petkevičienė, J.; Klumbiene, J.; Sakyte, E.; Raskiliene, A. The prevalence and trends of overweight and obesity among Lithuanian adults, 1994–2012. Public Health 2014, 128, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Morice, P.; Leary, A.; Creutzberg, C.; Abu-Rustum, N.; Darai, E. Endometrial cancer. Lancet 2016, 387, 1094–1108. [Google Scholar] [CrossRef]
- Kurtinaitis, J.; Aleknavičienė, B.; Tamošauskienė, J. The Main Results of Oncological Care in Lithuania in 2000; Lithuanian Oncological Center: Vilnius, Lithuania, 2001; 39p. (In Lithuanian) [Google Scholar]
- Cancer in Lithuania. National Cancer Institute: Vilnius, Lithuania. 2015. Available online: https://www.nvi.lt/uploads/pdf/Vezio%20registras/Vezys_lietuvoje_2012.pdf (accessed on 2 June 2020). (In Lithuanian).
- Krilaviciute, A.; Smailyte, G.; Brenner, H.; Gondos, A. Cancer survival in Lithuania after the restoration of independence: Rapid improvements, but persisting major gaps. Acta Oncol. 2014, 53, 1238–1244. [Google Scholar] [CrossRef] [PubMed]
- Sant, M.; Lopez, M.D.C.; Agresti, R.; Sánchez, M.-J.; Holleczek, B.; Bielska-Lasota, M.; Dimitrova, N.; Innos, K.; Katalinic, A.; Langseth, H.; et al. Survival of women with cancers of breast and genital organs in Europe 1999–2007: Results of the EUROCARE-5 study. Eur. J. Cancer 2015, 51, 2191–2205. [Google Scholar] [CrossRef] [PubMed]
- Keinan-Boker, L.; Silverman, B.G.; Walsh, P.M.; Gavin, A.T.; Hayes, C. Time Trends in the Incidence and Mortality of Ovarian Cancer in Ireland, Northern Ireland, and Israel, 1994–2013. Int. J. Gynecol. Cancer 2017, 27, 1628–1636. [Google Scholar] [CrossRef] [PubMed]
- Hirabayashi, Y.; Marugame, T. Comparison of Time Trends in Ovary Cancer Mortality (1990–2006) in the World, from the WHO Mortality Database. Jpn. J. Clin. Oncol. 2009, 39, 860–861. [Google Scholar] [CrossRef] [PubMed]
- Allemani, C.; Weir, H.K.; Carreira, H.; Harewood, R.; Spika, D.; Wang, X.-S.; Bannon, F.; Ahn, J.V.; Johnson, C.J.; Bonaventure, A.; et al. Global surveillance of cancer survival 1995–2009: Analysis of individual data for 2,676,887 patients from 279 population-based registries in 67 countries (CONCORD-2). Lancet 2015, 385, 977–1010. [Google Scholar] [CrossRef]
- Alkema, L.; Kantorová, V.; Menozzi, C.; Biddlecom, A.S. National, regional, and global rates and trends in contraceptive prevalence and unmet need for family planning between 1990 and 2015: A systematic and comprehensive analysis. Lancet 2013, 381, 1642–1652. [Google Scholar] [CrossRef]
- Grulich, A.E.; Swerdlow, A.J.; Dos-Santos-Silva, I.; Beral, V. Is the apparent rise in cancer mortality in the elderly real? Analysis of changes in certification and coding of cause of death in England and Wales, 1970–1990. Int. J. Cancer 1995, 63, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Fallah, M.; Kharazmi, E. Correction for under-ascertainment in cancer cases in the very elderly (aged 75+): External reference method. Cancer Causes Control 2008, 19, 739–749. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| ICD Definition | ICD-10 Detailed 1998–2016 | ICD-9 Basic 1993–1997 | ICD-9 Special 1987–1992 |
|---|---|---|---|
| Malignant neoplasm of cervix uteri | C53 | B120 | B120 |
| Malignant neoplasm of uterus, other and unspecified | C54, C55 | B122 | B122 |
| Malignant neoplasm of ovary and other uterine adnexa | C56 | B123 | B123 |
| Age at Death | Deaths | Rate | APC | |
|---|---|---|---|---|
| n | 1987 a | 2016 | From 1987 a to 2016 | |
| Corpus uteri cancer | ||||
| 40–49 | 203 | 3.9 | 1.4 | −2.4 (−4.0; −0.9) |
| 50–59 | 661 | 10.1 | 7.6 | −1.7 (−2.6; −0.9) |
| 60–69 | 1288 | 28.7 | 18.2 | −1.4 (−2.0; −0.7) |
| 70–79 | 1367 | 30.8 | 34.1 | −0.2 (−0.9; 0.4) |
| 80+ | 833 | 39.3 | 44.0 | 1.2 (0.5; 2.0) |
| Total (all ages) | 4405 | 4.9 | 3.5 | −1.2 (−1.8; −0.7) |
| Ovarian cancer | ||||
| 40–49 | 588 | 9.7 | 6.2 | −1.5 (−3.0; 0.0) |
| 50–59 | 1283 | 30.1 | 24.6 | −1.0 (−1.8; −0.2) |
| 60–69 | 1713 | 44.0 | 38.0 | −1.2 (−2.0; −0.5) |
| 70–79 | 1798 | 54.8 | 46.9 | −0.7 (−1.2; −0.1) |
| 80+ | 989 | 50.7 | 52.1 | 0.5 (−0.6; 1.6) |
| Total (all ages) | 6527 | 9.7 | 7.5 | −1.2 (−1.6; −0.8) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Everatt, R.; Intaitė, B. Trends in Mortality Rates of Corpus Uteri and Ovarian Cancer in Lithuania, 1987–2016. Medicina 2020, 56, 347. https://doi.org/10.3390/medicina56070347
Everatt R, Intaitė B. Trends in Mortality Rates of Corpus Uteri and Ovarian Cancer in Lithuania, 1987–2016. Medicina. 2020; 56(7):347. https://doi.org/10.3390/medicina56070347
Chicago/Turabian StyleEveratt, Rūta, and Birutė Intaitė. 2020. "Trends in Mortality Rates of Corpus Uteri and Ovarian Cancer in Lithuania, 1987–2016" Medicina 56, no. 7: 347. https://doi.org/10.3390/medicina56070347
APA StyleEveratt, R., & Intaitė, B. (2020). Trends in Mortality Rates of Corpus Uteri and Ovarian Cancer in Lithuania, 1987–2016. Medicina, 56(7), 347. https://doi.org/10.3390/medicina56070347