A Randomized Controlled Trial Investigating the Effects of Equine Simulator Riding on Low Back Pain, Morphological Changes, and Trunk Musculature in Elderly Women



Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Experimental Design
2.3. Back Pain Measurement
2.4. Isokinetic Moments’ Measurements
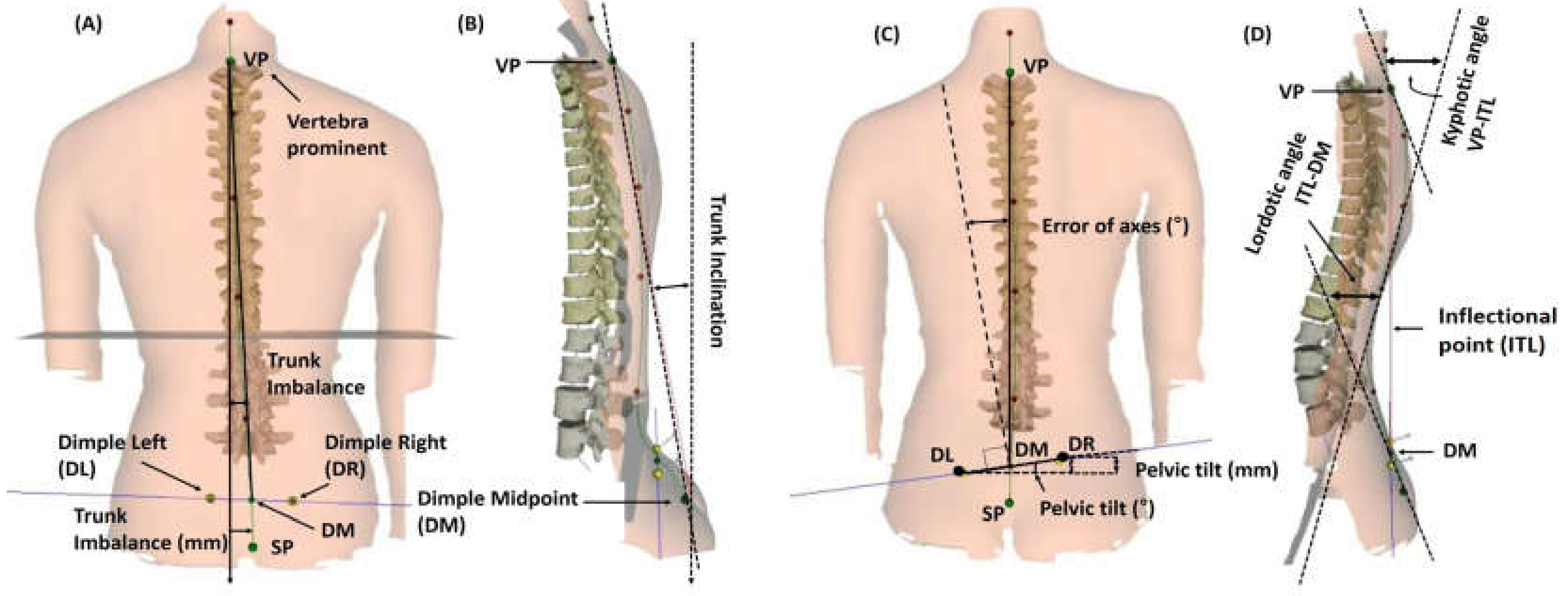
2.5. Morphological Measurements
2.6. Statistical Analyses
3. Results
3.1. Effect of ERS Exercise on Back Pain
3.2. Effect of ERS Exercise on Trunk Extensor and Flexor
3.3. Effect of ERS Exercise on Body Composition
3.4. Effect of ERS Exercise on Spinal Alignment
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Griffith, L.E.; Hogg-Johnson, S.; Cole, D.C.; Krause, N.; Hayden, J.; Burdorf, A.; Leclerc, A.; Coggon, D.; Bongers, P.; Walter, S.D.; et al. Low-back pain definitions in occupational studies were categorized for a meta-analysis using Delphi consensus methods. J. Clin. Epidemiol. 2007, 60, 625.e1–625.e23. [Google Scholar] [CrossRef] [PubMed]
- Thomas, E.; Peat, G.; Harris, L.; Wilkie, R.; Croft, P. The prevalence of pain and pain interference in a general population of older adults: Cross-sectional findings from the North Staffordshire Osteoarthritis Project (NorStOP). Pain 2004, 110, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Jee, Y.-S. Effects of 3D moving platform exercise on physiological parameters and pain in patients with chronic low back pain. Medicina 2020, 56, 351. [Google Scholar] [CrossRef] [PubMed]
- D’Astolfo, C.J.; Humphreys, B.K. A record review of reported musculoskeletal pain in an Ontario long term care facility. BMC Geriatr. 2006, 6, 5. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Koumantakis, G.A.; Watson, P.J.; Oldham, J.A. Trunk muscle stabilization training plus general exercise versus general exercise only: Randomized controlled trial of patients with recurrent low back pain. Phys. Ther. 2005, 85, 209–225. [Google Scholar] [CrossRef]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of exercise is a major cause of chronic diseases. Compr. Physiol. 2012, 2, 1143–1211. [Google Scholar] [CrossRef]
- Meakin, J.R.; Smith, F.W.; Gilbert, F.J.; Aspden, R.M. The effect of axial load on the sagittal plane curvature of the upright human spine in vivo. J. Biomech. 2008, 41, 2850–2854. [Google Scholar] [CrossRef]
- Donelson, R. Is your client’s back pain “rapidly reversible”? Improving low back care at its foundation. Prof. Case Manag. 2008, 13, 87–96. [Google Scholar] [CrossRef]
- Ferreira, M.L.; Ferreira, P.H.; Latimer, J.; Herbert, R.D.; Hodges, P.W.; Jennings, M.D.; Maher, C.G.; Refshauge, K.M. Comparison of general exercise, motor control exercise and spinal manipulative therapy for chronic low back pain: A randomized trial. Pain 2007, 131, 31–37. [Google Scholar] [CrossRef]
- Bronson, C.; Brewerton, K.; Ong, J.; Palanca, C.; Sullivan, S.J. Does hippotherapy improve balance in persons with multiple sclerosis: A systematic review. Eur. J. Phys. Rehabil. Med. 2010, 46, 347–353. [Google Scholar]
- Meregillano, G. Hippotherapy. Phys. Med. Rehabil. Clin. N. Am. 2004, 15, 843–854. [Google Scholar] [CrossRef] [PubMed]
- Fuentes-García, J.P.; Lavín-Pérez, A.M.; Fuentes-García, J.P.; Garcia-Gordillo, M.Á.; Villafaina, S. Effects of equine-assisted therapies or horse-riding simulators on chronic pain: A systematic review and meta-analysis. Medicina 2020, 56, 444. [Google Scholar] [CrossRef]
- Hodges, P.W. Core stability exercise in chronic low back pain. Orthop. Clin. N. Am. 2003, 34, 245–254. [Google Scholar] [CrossRef]
- McGibbon, N.H.; Andrade, C.-K.; Widener, G.; Cintas, H.L. Effect of an equine-movement therapy program on gait, energy expenditure, and motor function in children with spastic cerebral palsy: A pilot study. Dev. Med. Child Neurol. 2008, 40, 754–762. [Google Scholar] [CrossRef]
- Yoo, J.-H.; Kim, S.-E.; Lee, M.-G.; Jin, J.-J.; Hong, J.; Choi, Y.-T.; Kim, M.-H.; Jee, Y.-S. The effect of horse simulator riding on visual analogue scale, body composition and trunk strength in the patients with chronic low back pain. Int. J. Clin. Pr. 2014, 68, 941–949. [Google Scholar] [CrossRef]
- Kubota, M.; Nagasaki, M.; Tokudome, M.; Shinomiya, Y.; Ozawa, T.; Sato, Y. Mechanical horseback riding improves insulin sensitivity in elder diabetic patients. Diabetes Res. Clin. Pr. 2006, 71, 124–130. [Google Scholar] [CrossRef]
- Hilliere, C.; Fuentes-García, J.P.; Villafaina, S.; Duque-Fonseca, P.; Parraça, J.A. Benefits of hippotherapy and horse riding simulation exercise on healthy older adults: A systematic review. PM R 2018, 10, 1062–1072. [Google Scholar] [CrossRef]
- Mannion, A.F.; Dvořák, J.; Taimela, S.; Müntener, M. Increase in strength after active therapy in chronic low back pain (CLBP) patients: Muscular adaptations and clinical relevance. Der Schmerz 2001, 15, 468–473. [Google Scholar] [CrossRef]
- Han, J.Y.; Kim, J.M.; Kim, S.K.; Chung, J.S.; Lee, H.-C.; Lim, J.K.; Lee, J.; Park, K.Y. Therapeutic effects of mechanical horseback riding on gait and balance ability in stroke patients. Ann. Rehabil. Med. 2012, 36, 762–769. [Google Scholar] [CrossRef]
- Minetto, M.A.; Gamerro, G.; Gays, G.; Vigo, S.; Caresio, C.; Gorji, N.; Massazza, G. Effectiveness of an innovative mattress overlay for improving rehabilitation in low back pain: A pilot randomized controlled study. J. Back Musculoskelet. Rehabil. 2018, 31, 1075–1083. [Google Scholar] [CrossRef]
- Ruiz, F.K.; Bohl, D.D.; Webb, M.L.; Russo, G.S.; Grauer, J.N. Oswestry Disability Index is a better indicator of lumbar motion than the Visual Analogue Scale. Spine J. 2014, 14, 1860–1865. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.-W.; Lee, M.-G.; Jang, J.-Y.; Jin, J.-J.; Cha, J.-Y.; Jin, Y.-Y.; Jee, Y.-S. Time-effects of horse simulator exercise on psychophysiological responses in men with chronic low back pain. Isokinet. Exerc. Sci. 2014, 22, 153–163. [Google Scholar] [CrossRef]
- Cohen, I.; Rainville, J.; Rainville, J. Aggressive exercise as treatment for chronic low back pain. Sports Med. 2002, 32, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.G. Effective physical treatment for chronic low back pain. Orthop. Clin. N. Am. 2004, 35, 57–64. [Google Scholar] [CrossRef]
- Kim, T.; Lee, J.; Oh, S.; Kim, S.; Yoon, B. Effectiveness of simulated horseback riding for patients with chronic low back pain: A randomized controlled trial. J. Sport Rehabil. 2020, 29, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Deyo, R.A.; Battie, M.; Beurskens, A.J.H.M.; Bombardier, C.; Croft, P.; Koes, B.; Malmivaara, A.; Roland, M.; Von Korff, M.; Waddell, G. Outcome measures for low back pain research. Spine 1998, 23, 2003–2013. [Google Scholar] [CrossRef]
- Fairbank, J.C.T.; Pynsent, P.B. The Oswestry Disability Index. Spine 2000, 25, 2940–2953. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-Y.; Lee, S.-H.; Lee, H.-Y.; Lee, H.-J.; Chang, S.-B.; Chung, S.-K.; Kim, H.-J. Validation of the Korean version of the Oswestry disability index. Spine 2005, 30, E123–E127. [Google Scholar] [CrossRef]
- Jee, Y.-S. The efficacy and safety of whole-body electromyostimulation in applying to human body: Based from graded exercise test. J. Exerc. Rehabil. 2018, 14, 49–57. [Google Scholar] [CrossRef]
- Zouita, A.B.M.; Ben Salah, F.Z.; Dziri, C.; Beardsley, C. Comparison of isokinetic trunk flexion and extension torques and powers between athletes and nonathletes. J. Exerc. Rehabil. 2018, 14, 72–77. [Google Scholar] [CrossRef]
- Lippold, C.; Danesh, G.; Schilgen, M.; Drerup, B.; Hackenberg, L. Sagittal jaw position in relation to body posture in adult humans-A rasterstereographic study. BMC Musculoskelet. Disord. 2006, 7, 8. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Drerup, B.; Hierholzer, E. Back shape measurement using video rasterstereography and three-dimensional reconstruction of spinal shape. Clin. Biomech. 1994, 9, 28–36. [Google Scholar] [CrossRef]
- Manniche, C.; Lundberg, E.; Christensen, I.; Bentzen, L.; Hesselsøe, G. Intensive dynamic back exercises for chronic low back pain: A clinical trial. Pain 1991, 47, 53–63. [Google Scholar] [CrossRef]
- Risch, S.V.; Norvell, N.K.; Pollock, M.L.; Risch, E.D.; Langer, H.; Fulton, M.; Graves, J.E.; Leggett, S.H. Lumbar strengthening in chronic low back pain patients. Physiologic and psychological benefits. Spine 1993, 18, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Akuthota, V.; Ferreiro, A.; Moore, T.; Fredericson, M. Core stability exercise principles. Curr. Sports Med. Rep. 2008, 7, 39–44. [Google Scholar] [CrossRef]
- Noormohammadpour, P.; Kordi, M.; Mansournia, M.A.; Akbari-Fakhrabadi, M.; Kordi, R. The role of a multi-step core stability exercise program in the treatment of nurses with chronic low back pain: A single-blinded randomized controlled trial. Asian Spine J. 2018, 12, 490–502. [Google Scholar] [CrossRef]
- Brumitt, J.; Matheson, J.W.; Meira, E.P. Core stabilization exercise prescription, Part I. Sports Health Multidiscip. Approach 2013, 5, 504–509. [Google Scholar] [CrossRef]
- Holmes, B.; Leggett, S.; Mooney, V.; Nichols, J.; Negri, S.; Hoeyberghs, A. Comparison of female geriatric lumbar-extension strength: Asymptotic versus chronic low back pain patients and their response to active rehabilitation. J. Spinal Disord. 1996, 9, 17–22. [Google Scholar] [CrossRef]
- Kim, J.-D.; Oh, H.-W.; Lee, J.-H.; Cha, J.-Y.; Ko, I.-G.; Jee, Y.-S. The effect of inversion traction on pain sensation, lumbar flexibility and trunk muscles strength in patients with chronic low back pain. Isokinet. Exerc. Sci. 2013, 21, 237–246. [Google Scholar] [CrossRef]
- Rainville, J.; Hartigan, C.; Martinez, E.; Limke, J.; Jouve, C.; Finno, M. Exercise as a treatment for chronic low back pain. Spine J. 2004, 4, 106–115. [Google Scholar] [CrossRef]
- Norris, C.; Matthews, M. The role of an integrated back stability program in patients with chronic low back pain. Complement. Ther. Clin. Pr. 2008, 14, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.J.; Noh, M.Y. The role of core stabilization in lumbosacral radiculopathy. Phys. Med. Rehabil. Clin. N. Am. 2011, 22, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Rissanen, A.; Kalimo, H.; Alaranta, H. Effect of intensive training on the isokinetic strength and structure of lumbar muscles in patients with chronic low back pain. Spine 1995, 20, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Ogden, L.G.; Stroebele, N.; Wyatt, H.R.; Catenacci, V.A.; Peters, J.C.; Stuht, J.; Wing, R.R.; Hill, J.O. Cluster analysis of the national weight control registry to identify distinct subgroups maintaining successful weight loss. Obesity 2012, 20, 2039–2047. [Google Scholar] [CrossRef] [PubMed]
- Roffey, D.M.; Budiansky, A.; Coyle, M.J.; Wai, E.K. Obesity and low back pain: Is there a weight of evidence to support a positive relationship? Curr. Obes. Rep. 2013, 2, 241–250. [Google Scholar] [CrossRef]
- Thompson, D.; Karpe, F.; Lafontan, M.; Frayn, K. Physical activity and exercise in the regulation of human adipose tissue physiology. Physiol. Rev. 2012, 92, 157–191. [Google Scholar] [CrossRef]
- Kim, W.; Jin, Y.S.; Lee, C.S.; Hwang, C.J.; Lee, S.Y.; Chung, S.G.; Choi, K.H. Relationship between the type and amount of physical activity and low back pain in Koreans aged 50 years and older. PM R 2014, 6, 893–899. [Google Scholar] [CrossRef]
- Van Der Velde, G.; Mierau, D. The effect of exercise on percentile rank aerobic capacity, pain, and self-rated disability in patients with chronic low-back pain: A retrospective chart review. Arch. Phys. Med. Rehabil. 2000, 81, 1457–1463. [Google Scholar] [CrossRef]
- Wong, A.; Parent, E.; Kawchuk, G.N. Reliability of 2 ultrasonic imaging analysis methods in quantifying lumbar multifidus thickness. J. Orthop. Sports Phys. Ther. 2013, 43, 251–262. [Google Scholar] [CrossRef]
- Frerich, J.M.; Hertzler, K.; Knott, P.; Mardjetko, S. Comparison of radiographic and surface topography measurements in adolescents with idiopathic scoliosis. Open Orthop. J. 2012, 6, 261–265. [Google Scholar] [CrossRef]
- Fakurnejad, S.; Scheer, J.K.; Lafage, V.; Smith, J.S.; Deviren, V.; Hostin, R.; Mundis, G.M.; Burton, D.C.; Klineberg, E.O.; Gupta, M.C.; et al. The likelihood of reaching minimum clinically important difference and substantial clinical benefit at 2 years following a 3-column osteotomy: Analysis of 140 patients. J. Neurosurg. Spine 2015, 23, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Champain, S.; Benchikh, K.; Nogier, A.; Mazel, C.; Guise, J.D.; Skalli, W. Validation of new clinical quantitative analysis software applicable in spine orthopaedic studies. Eur. Spine J. 2005, 15, 982–991. [Google Scholar] [CrossRef] [PubMed]
- Lafage, V.; Schwab, F.; Patel, A.; Hawkinson, N.; Farcy, J.-P. Pelvic tilt and truncal inclination. Spine 2009, 34, E599–E606. [Google Scholar] [CrossRef] [PubMed]
- Roussouly, P.; Pinheiro-Franco, J.L. Biomechanical analysis of the spino-pelvic organization and adaptation in pathology. Eur. Spine J. 2011, 20, 609–618. [Google Scholar] [CrossRef]
- Ekedahl, H.; Jönsson, B.; Frobell, R.B. Fingertip-to-floor test and straight leg raising test: Validity, responsiveness, and predictive value in patients with acute/subacute low back pain. Arch. Phys. Med. Rehabil. 2012, 93, 2210–2215. [Google Scholar] [CrossRef]
- Moghadam, N.; Ghaffari, M.S.; Noormohammadpour, P.; Rostami, M.; Zarei, M.; Moosavi, M.; Kordi, R. Comparison of the recruitment of transverse abdominis through drawing-in and bracing in different core stability training positions. J. Exerc. Rehabil. 2019, 15, 819–825. [Google Scholar] [CrossRef]
- Augeard, N.; Carroll, S.P. Core stability and low-back pain: A causal fallacy. J. Exerc. Rehabil. 2019, 15, 493–495. [Google Scholar] [CrossRef]
- Kim, D.-H.; Kim, T.-H. Comparison of the effects of stability exercise and balance exercise on muscle activity in female patients with chronic low back pain. J. Exerc. Rehabil. 2018, 14, 1053–1058. [Google Scholar] [CrossRef]
- Rainville, J.; Ahern, D.K.; Phalen, L.; Childs, L.A.; Sutherland, R. The association of pain with physical activities in chronic low back pain. Spine 1992, 17, 1060–1064. [Google Scholar] [CrossRef]
- Paungmali, A.; Henry, L.J.; Sitilertpisan, P.; Pirunsan, U.; Uthaikhup, S. Improvements in tissue blood flow and lumbopelvic stability after lumbopelvic core stabilization training in patients with chronic non-specific low back pain. J. Phys. Ther. Sci. 2016, 28, 635–640. [Google Scholar] [CrossRef][Green Version]
- Leonard, J.H.; Paungmali, A.; Sitilertpisan, P.; Pirunsan, U.; Uthaikhup, S. Changes in transversus abdominis muscle thickness after lumbo-pelvic core stabilization training among chronic low back pain individuals. La Clin. Ter. 2015, 166, 312. [Google Scholar]


{kind=link}
| Variables (Unit) | Groups | ||
|---|---|---|---|
| CON (n = 40) | ERSG (n = 40) | p-value | |
| Age (y) | 72.05 ± 6.82 | 71.50 ± 6.34 | 0.732 |
| Height (cm) | 159.96 ± 7.92 | 161.30 ± 8.74 | 0.410 |
| Weight (kg) | 64.03 ± 9.38 | 60.23 ± 6.88 | 0.363 |
| Muscle mass (kg) | 42.75 ± 6.91 | 42.98 ± 5.72 | 0.063 |
| Fat mass (kg) | 18.44 ± 4.20 | 17.41 ± 4.94 | 0.348 |
| Percent fat (%) | 27.23 ± 5.01 | 27.35 ± 6.16 | 0.840 |
| LBP history (month) | 22.10 ± 7.47 | 23.61 ± 8.47 | 0.550 |
| Items | Time (T) | Group (G) | ANOVA (p-Value) | |||
|---|---|---|---|---|---|---|
| CON (n = 40) | ERSG (n = 40) | G | T | G × T | ||
| VAS | Pre | 7.27 ± 1.52 | 7.35 ± 1.63 | 0.001 | 0.001 | 0.001 |
| Post | 7.64 ± 1.31 | 2.10 ± 2.54 | ||||
| ODI | Pre | 43.98 ± 6.58 | 44.31 ± 6.68 | 0.001 | 0.001 | 0.001 |
| Post | 45.71 ± 8.04 | 17.82 ± 4.66 | ||||
| Items (Units) | Time (T) | Group (G) | ANOVA (p-Value) | |||
|---|---|---|---|---|---|---|
| CON (n = 40) | ERSG (n = 40) | G | T | G × T | ||
| Trunk extensor at 30°/s (Nm) | Pre | 120.03 ± 48.36 | 128.20 ± 42.13 | 0.030 | 0.373 | 0.002 |
| Post | 103.63 ± 49.62 | 137.35 ± 44.23 | ||||
| Trunk flexor at 30°/s (Nm) | Pre | 140.03 ± 43.45 | 139.73 ± 28.08 | 0.486 | 0.441 | 0.061 |
| Post | 136.55 ± 45.63 | 147.98 ± 32.62 | ||||
| Trunk extensor at 60°/s (Nm) | Pre | 112.30 ± 38.27 | 117.25 ± 47.37 | 0.133 | 0.203 | 0.036 |
| Post | 97.80 ± 43.58 | 120.88 ± 51.46 | ||||
| Trunk flexor at 60°/s (Nm) | Pre | 128.90 ± 46.87 | 145.38 ± 35.82 | 0.052 | 0.782 | 0.842 |
| Post | 127.83 ± 43.02 | 145.20 ± 31.28 | ||||
| Trunk extensor at 120°/s (Nm) | Pre | 79.20 ± 39.17 | 83.00 ± 33.03 | 0.015 | 0.073 | 0.001 |
| Post | 68.50 ± 41.46 | 108.03 ± 54.56 | ||||
| Trunk flexor at 120°/s (Nm) | Pre | 102.35 ± 46.71 | 124.50 ± 39.67 | 0.001 | 0.011 | 0.001 |
| Post | 99.68 ± 48.26 | 142.90 ± 43.66 | ||||
| Items (Units) | Time (T) | Group (G) | ANOVA (p-Value) | |||
|---|---|---|---|---|---|---|
| CON (n = 40) | ERSG (n = 40) | G | T | G × T | ||
| Weight (kg) | Pre | 64.03 ± 9.38 | 61.42 ± 7.90 | 0.061 | 0.314 | 0.002 |
| Post | 64.64 ± 9.04 | 60.23 ± 6.88 | ||||
| Muscle mass (kg) | Pre | 42.75 ± 6.91 | 42.98 ± 5.72 | 0.667 | 0.002 | 0.123 |
| Post | 41.65 ± 6.64 | 42.60 ± 6.06 | ||||
| Fat mass (kg) | Pre | 18.44 ± 4.20 | 17.41 ± 4.94 | 0.009 | 0.305 | 0.001 |
| Post | 20.38 ± 4.80 | 16.31 ± 4.52 | ||||
| Percent fat (%) | Pre | 27.23 ± 5.01 | 27.35 ± 6.16 | 0.080 | 0.001 | 0.001 |
| Post | 31.62 ± 6.16 | 27.33 ± 6.43 | ||||
| BMR (kcal/day) | Pre | 1261.30 ± 149.25 | 1238.09 ± 127.86 | 0.962 | 0.048 | 0.001 |
| Post | 1248.47 ± 145.06 | 1274.58 ± 129.66 | ||||
| Items (Units) | Time (T) | Group (G) | ANOVA (p-Value) | |||
|---|---|---|---|---|---|---|
| CON (n = 40) | ERSG (n = 40) | G | T | G × T | ||
| Trunk inclination (°) | Pre | 2.27 ± 1.25 | 2.41 ± 1.37 | 0.126 | 0.016 | 0.001 |
| Post | 2.40 ± 1.22 | 1.54 ± 1.14 | ||||
| Trunk imbalance (°) | Pre | 5.84 ± 2.21 | 5.87 ± 2.32 | 0.167 | 0.030 | 0.005 |
| Post | 5.99 ± 1.79 | 4.74 ± 2.36 | ||||
| Pelvic tilt (°) | Pre | 4.63 ± 1.41 | 4.68 ± 1.62 | 0.075 | 0.117 | 0.001 |
| Post | 4.95 ± 1.61 | 3.79 ± 1.67 | ||||
| Pelvic torsion (°) | Pre | 2.21 ± 0.91 | 2.26 ± 0.97 | 0.323 | 0.532 | 0.076 |
| Post | 2.35 ± 0.81 | 1.97 ± 0.96 | ||||
| Kyphotic angle (°) | Pre | 45.58 ± 8.15 | 44.26 ± 7.79 | 0.001 | 0.006 | 0.001 |
| Post | 46.88 ± 7.87 | 36.57 ± 7.26 | ||||
| Lordotic angle (°) | Pre | 39.61 ± 8.45 | 38.63 ± 8.73 | 0.017 | 0.045 | 0.004 |
| Post | 40.63 ± 9.80 | 33.03 ± 10.32 | ||||
| Surface rotation to the right side (°) | Pre | 4.17 ± 2.13 | 4.13 ± 1.95 | 0.103 | 0.504 | 0.005 |
| Post | 4.61 ± 1.56 | 3.43 ± 1.78 | ||||
| Surface rotation to the left side (°) | Pre | −4.07 ± 2.56 | −4.17 ± 2.52 | 0.481 | 0.253 | 0.169 |
| Post | −4.14 ± 2.35 | −3.41 ± 2.28 | ||||
| Lateral deviation to the right side (mm) | Pre | 5.80 ± 2.00 | 6.02 ± 2.20 | 0.766 | 0.523 | 0.202 |
| Post | 5.97 ± 2.05 | 5.51 ± 2.28 | ||||
| Lateral deviation to the left side (mm) | Pre | −5.42 ± 2.03 | −5.63 ± 1.97 | 0.210 | 0.375 | 0.028 |
| Post | −5.86 ± 2.58 | −4.60 ± 2.81 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Park, S.; Min, S.; Kim, C.-J.; Jee, Y.-S. A Randomized Controlled Trial Investigating the Effects of Equine Simulator Riding on Low Back Pain, Morphological Changes, and Trunk Musculature in Elderly Women. Medicina 2020, 56, 610. https://doi.org/10.3390/medicina56110610
Park S, Park S, Min S, Kim C-J, Jee Y-S. A Randomized Controlled Trial Investigating the Effects of Equine Simulator Riding on Low Back Pain, Morphological Changes, and Trunk Musculature in Elderly Women. Medicina. 2020; 56(11):610. https://doi.org/10.3390/medicina56110610
Chicago/Turabian StylePark, Sihwa, Sunhee Park, Sukyung Min, Chang-Ju Kim, and Yong-Seok Jee. 2020. "A Randomized Controlled Trial Investigating the Effects of Equine Simulator Riding on Low Back Pain, Morphological Changes, and Trunk Musculature in Elderly Women" Medicina 56, no. 11: 610. https://doi.org/10.3390/medicina56110610
APA StylePark, S., Park, S., Min, S., Kim, C.-J., & Jee, Y.-S. (2020). A Randomized Controlled Trial Investigating the Effects of Equine Simulator Riding on Low Back Pain, Morphological Changes, and Trunk Musculature in Elderly Women. Medicina, 56(11), 610. https://doi.org/10.3390/medicina56110610