Effect of Decompression on Jaw Cystic Lesions Based on Three-Dimensional Volumetric Analysis

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients’ Criteria
2.2. Surgical Procedures for Decompression
2.3. Computed Tomography Data Acquisition
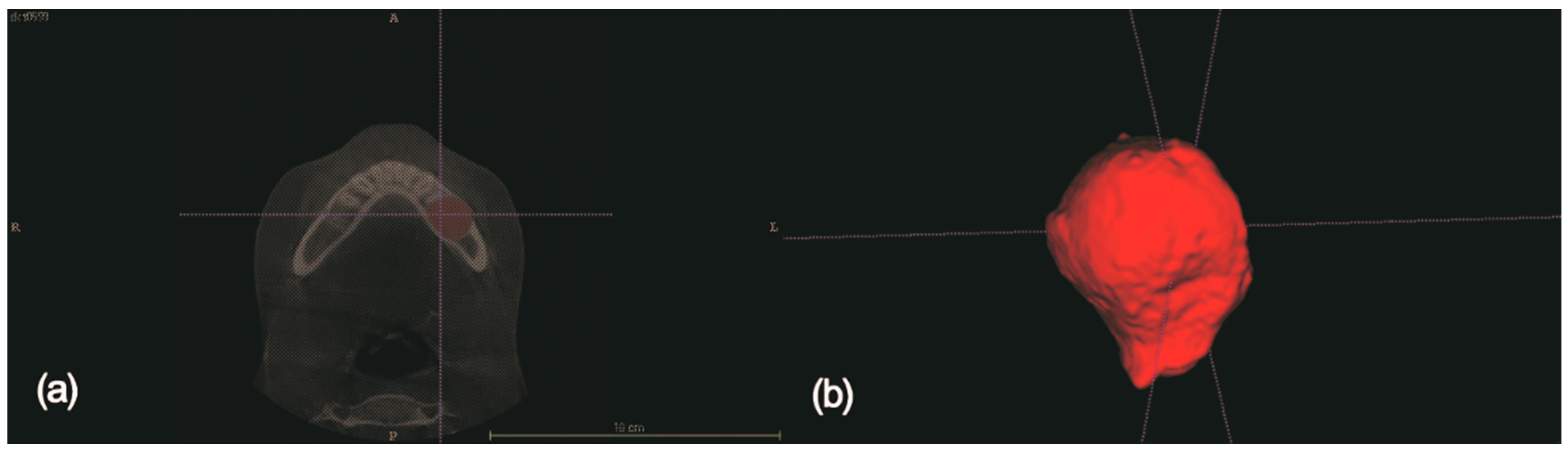
2.4. 3D Volume Measurements
2.5. Determination of Effective Parameters
2.6. Statistical Analyses
3. Results
3.1. Patient Distribution
3.2. Effective Factors in the Two Statistical Analyses
4. Discussion
5. Conclusions
- In the patient group to which the decompression procedure was applied, an average of 54.68% reduction in cyst size was observed during an average observation period of 9.41 months.
- Decompression is an effective procedure for reducing the size of cysts in all patients, as determined by 3D volumetric analysis.
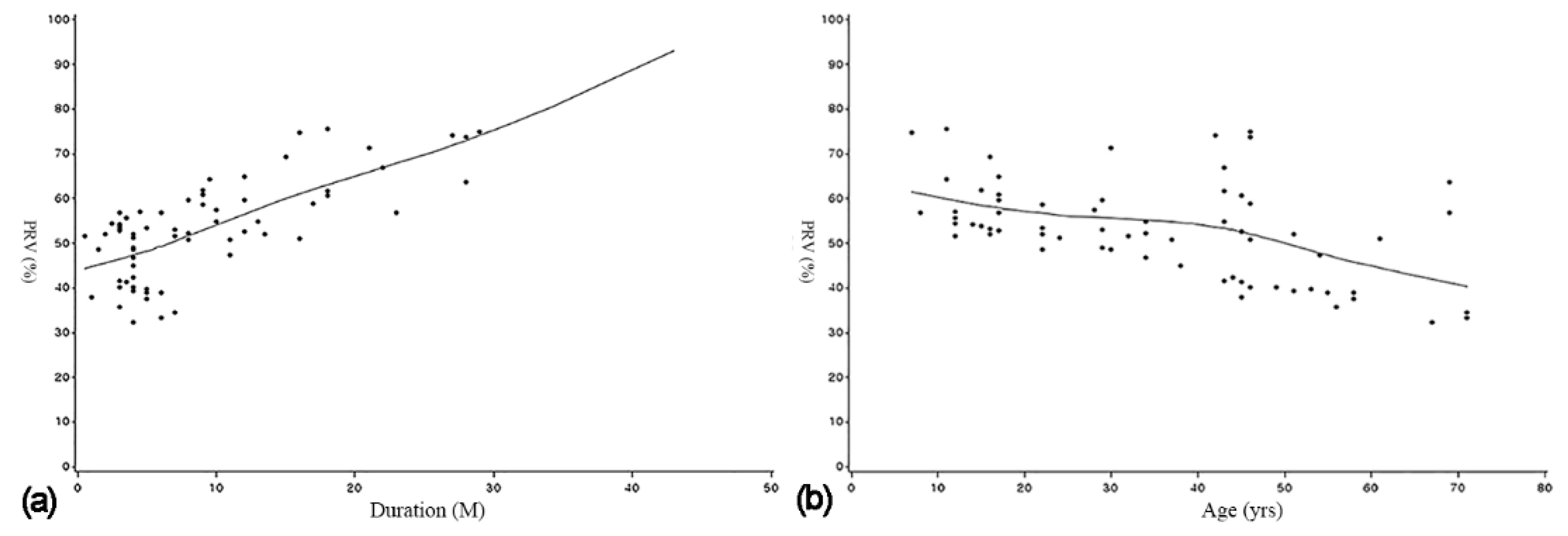
- Decompression was more effective when the procedure was applied for a long period, in younger patients, and in the posterior maxilla.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Asutay, F.; Atalay, Y.; Turamanlar, O.; Horata, E.; Burdurlu, M.C. Three-Dimensional Volumetric Assessment of the Effect of Decompression on Large Mandibular Odontogenic Cystic Lesions. J. Oral Maxillofac. Surg. 2016, 74, 1159–1166. [Google Scholar] [CrossRef] [PubMed]
- Marin, S.; Kirnbauer, B.; Rugani, P.; Mellacher, A.; Payer, M.; Jakse, N. The effectiveness of decompression as initial treatment for jaw cysts: A 10-year retrospective study. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e47–e52. [Google Scholar] [CrossRef] [PubMed]
- Jeong, H.G.; Hwang, J.J.; Lee, S.H.; Nam, W. Effect of decompression for patients with various jaw cysts based on a three-dimensional computed tomography analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 123, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Schlieve, T.; Miloro, M.; Kolokythas, A. Does Decompression of Odontogenic Cysts and Cystlike Lesions Change the Histologic Diagnosis? J. Oral Maxillofac. Surg. 2014, 72, 1094–1095. [Google Scholar] [CrossRef]
- Park, H.S.; Song, I.S.; Seo, B.M.; Lee, J.H.; Kim, M.J. The Effectiveness of Decompression for Patients with Dentigerous Cysts, Keratocystic Odontogenic Tumors, and Unicystic Ameloblastoma. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 260–265. [Google Scholar] [CrossRef]
- de Molon, R.S.; Verzola, M.H.; Pires, L.C.; Mascarenhas, V.I.; da Silva, R.B.; Cirelli, J.A.; Barbeiro, R.H. Five years follow-up of a keratocyst odontogenic tumor treated by marsupialization and enucleation: A case report and literature review. Contemp Clin. Dent. 2015, 6 (Suppl. 1), S106–S110. [Google Scholar] [CrossRef]
- Nakamura, N.; Mitsuyasu, T.; Mitsuyasu, Y.; Taketomi, T.; Higuchi, Y.; Ohishi, M. Marsupialization for odontogenic keratocysts: Long-term follow-up analysis of the effects and changes in growth characteristics. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 94, 543–553. [Google Scholar] [CrossRef]
- Schmidt, B.L.; Pogrel, M.A. The Use of Enucleation and Liquid Nitrogen Cryotherapy in the Management of Odontogenic Keratocysts. J. Oral Maxillofac. Surg. 2001, 59, 720–725. [Google Scholar] [CrossRef]
- Marker, P.; Brondum, N.; Clausen, P.P.; Bastian, H.L. Treatment of large odontogenic keratocysts by decompression and later cystectomy: A long-term follow-up and a histologic study of 23 cases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1996, 82, 122–131. [Google Scholar] [CrossRef]
- Enislidis, G.; Fock, N.; Sulzbacher, I.; Ewers, R. Conservative Treatment of Large Cystic Lesions of the Mandible: A Prospective Study of the Effect of Decompression. Br. J. Oral Maxillofac. Surg. 2004, 42, 546–550. [Google Scholar] [CrossRef]
- Lee, S.T.; Kim, S.G.; Moon, S.Y.; Oh, J.S.; You, J.S.; Kim, J.S. The Effect of Decompression as Treatment of the Cysts in the Jaws: Retrospective Analysis. J. Korean Assoc. Oral Maxillofac. Surg. 2017, 43, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Liu, B.; Han, Q.B.; Wang, S.P.; Wang, Y.N. Changes in Bone Density and Cyst Volume After Marsupialization of Mandibular Odontogenic Keratocysts (Keratocystic Odontogenic Tumors). J. Oral Maxillofac. Surg. 2011, 69, 1361–1366. [Google Scholar] [CrossRef] [PubMed]
- Anavi, Y.; Gal, G.; Miron, H.; Calderon, S.; Allon, D.M. Decompression of odontogenic cystic lesions: Clinical long-term study of 73 cases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.F.; Wei, J.X.; Wang, S.P. Treatment of odontogenic keratocysts: A follow-up of 255 Chinese patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 94, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Maurette, P.E.; Jorge, J.; de Moraes, M. Conservative Treatment Protocol of Odontogenic Keratocyst: A Preliminary Study. J. Oral Maxillofac. Surg. 2006, 64, 379–383. [Google Scholar] [CrossRef] [PubMed]
- August, M.; Faquin, W.C.; Troulis, M.J.; Kaban, L.B. Dedifferentiation of Odontogenic Keratocyst Epithelium After Cyst Decompression. J. Oral Maxillofac. Surg. 2003, 61, 678–683. [Google Scholar] [CrossRef]
- Brondum, N.; Jensen, V.J. Recurrence of keratocysts and decompression treatment. A long-term follow-up of forty-four cases. Oral Surg. Oral Med. Oral Pathol. 1991, 72, 265–269. [Google Scholar] [CrossRef]
- Nomura, Y.; Watanabe, H.; Shirotsu, K.; Honda, E.; Sumi, Y.; Kurabayshi, T. Stability of Voxel Values from Cone-Beam Computed Tomography for Dental Use in Evaluating Bone Mineral Content. Clin. Oral Implants Res. 2013, 24, 543–548. [Google Scholar] [CrossRef]
- Bodner, L.; Bar-Ziv, J. Characteristics of bone formation following marsupialization of jaw cysts. Dentomaxillofac. Radiol. 1998, 27, 166–171. [Google Scholar] [CrossRef]
- Park, J.H.; Kwak, E.J.; You, K.S.; Jung, Y.S.; Jung, H.D. Volume change pattern of decompression of mandibular odontogenic keratocyst. Maxillofac. Plast Reconst. Surg. 2019, 41, 2. [Google Scholar] [CrossRef]
- Song, I.S.; Park, H.S.; Seo, B.M.; Lee, J.H.; Kim, M.J. Effect of Decompression on Cystic Lesions of the Mandible: 3-Dimensional Volumetric Analysis. Br. J. Oral Maxillofac. Surg. 2015, 53, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, Y.; Nakajima, T.; Kaneshiro, S.; Sakaguchi, M. Effective Treatment of the Postoperative Maxillary Cyst by Marsupialization. J. Oral Maxillofac. Surg. 1982, 40, 487–491. [Google Scholar] [CrossRef]
- Rothe, J.H.; Steffen, I.G.; Lehmkuhl, L.; Grieser, C.; Mussler, A.; Schnapauff, D.; Stelter, L.; Denecke, T. Volume measurement of liver metastases using multidetector computed tomography: Comparison of lesion diameter and volume segmentation—A phantom study. Rofo 2010, 182, 1082–1090. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.K.; Kim, J.W.; Lee, U.L.; Kim, J.W.; Lee, H. Risk Factor Analysis of Graft Failure With Concomitant Cyst Enucleation of the Jaw Bone: A Retrospective Multicenter Study. J. Oral Maxillofac. Surg Off. J. Am. Assoc. Oral Maxillofac. Surg. 2017, 75, 1668–1678. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.; Rao, S. Decompression as a Treatment for Odontogenic Cystic Lesions of the Jaw. J. Oral Maxillofac. Surg. 2014, 72, 1231. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, N.; Higuchi, Y.; Tashiro, H.; Ohishi, M. Marsupialization of Cystic Ameloblastoma: A Clinical and Histopathologic Study of the Growth Characteristics Before and After Marsupialization. J. Oral Maxillofac. Surg. 1995, 53, 748–754. [Google Scholar] [CrossRef]
- Pogrel, M.A. Treatment of Keratocysts: The Case for Decompression and Marsupialization. J. Oral Maxillofac. Surg. 2005, 63, 1667–1673. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | Number | PRV (%) | ||
|---|---|---|---|---|
| Mean | SD | |||
| Sex | Male | 37 | 55.812 | 23.72 |
| Female | 13 | 51.469 | 29.83 | |
| Location | Mandible | 29 | 52.006 | 23.95 |
| Anterior maxilla | 14 | 53.943 | 29.52 | |
| Posterior maxilla | 7 | 67.254 | 20.05 | |
| Tooth extraction | Extraction | 12 | 55.491 | 26.06 |
| No extraction | 38 | 54.428 | 25.28 | |
| Expansion of the cortical layer | Mild | 16 | 60.826 | 23.36 |
| Severe | 34 | 51.792 | 25.85 | |
| Pathological diagnosis | DC | 17 | 55.272 | 25.24 |
| RC | 26 | 55.192 | 25.27 | |
| OKC | 7 | 51.362 | 28.52 | |
| Total | 50 | 54.683 | 25.20 | |
| Parameter | p-Value with the Multiple Linear Regression Analysis | p-Value with Generalised Linear Mixed Models |
|---|---|---|
| Sex | 0.1869 | 0.7712 |
| Age (years) | 0.037 * | 0.0124 * |
| Initial cystic volume (mL) | 0.1661 | 0.1711 |
| Duration (M) | <0.0001 * | 0.0016 * |
| Location | 0.0081 * | 0.2156 |
| Tooth extraction | 0.2628 | 0.4438 |
| Expansion of cortical layer | 0.1036 | 0.4582 |
| Pathological diagnosis | 0.2803 | 0.894 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, Y.-J.; Ko, K.-S.; So, B.-K.; Kim, D.-H.; Jang, H.-S.; Kim, S.-H.; Lee, E.-S.; Lim, H.-K. Effect of Decompression on Jaw Cystic Lesions Based on Three-Dimensional Volumetric Analysis. Medicina 2020, 56, 602. https://doi.org/10.3390/medicina56110602
Kwon Y-J, Ko K-S, So B-K, Kim D-H, Jang H-S, Kim S-H, Lee E-S, Lim H-K. Effect of Decompression on Jaw Cystic Lesions Based on Three-Dimensional Volumetric Analysis. Medicina. 2020; 56(11):602. https://doi.org/10.3390/medicina56110602
Chicago/Turabian StyleKwon, Yeh-Jin, Kyeong-Soo Ko, Byung-Kyu So, Dong-Hyuck Kim, Hyon-Seok Jang, Soo-Ho Kim, Eui-Seok Lee, and Ho-Kyung Lim. 2020. "Effect of Decompression on Jaw Cystic Lesions Based on Three-Dimensional Volumetric Analysis" Medicina 56, no. 11: 602. https://doi.org/10.3390/medicina56110602
APA StyleKwon, Y.-J., Ko, K.-S., So, B.-K., Kim, D.-H., Jang, H.-S., Kim, S.-H., Lee, E.-S., & Lim, H.-K. (2020). Effect of Decompression on Jaw Cystic Lesions Based on Three-Dimensional Volumetric Analysis. Medicina, 56(11), 602. https://doi.org/10.3390/medicina56110602