The Impact of Hormonal Replacement Treatment in Postmenopausal Women with Uterine Fibroids: A State-of-the-Art Review of the Literature

 , ,
, , 
 , and
, and
Abstract
1. Introduction
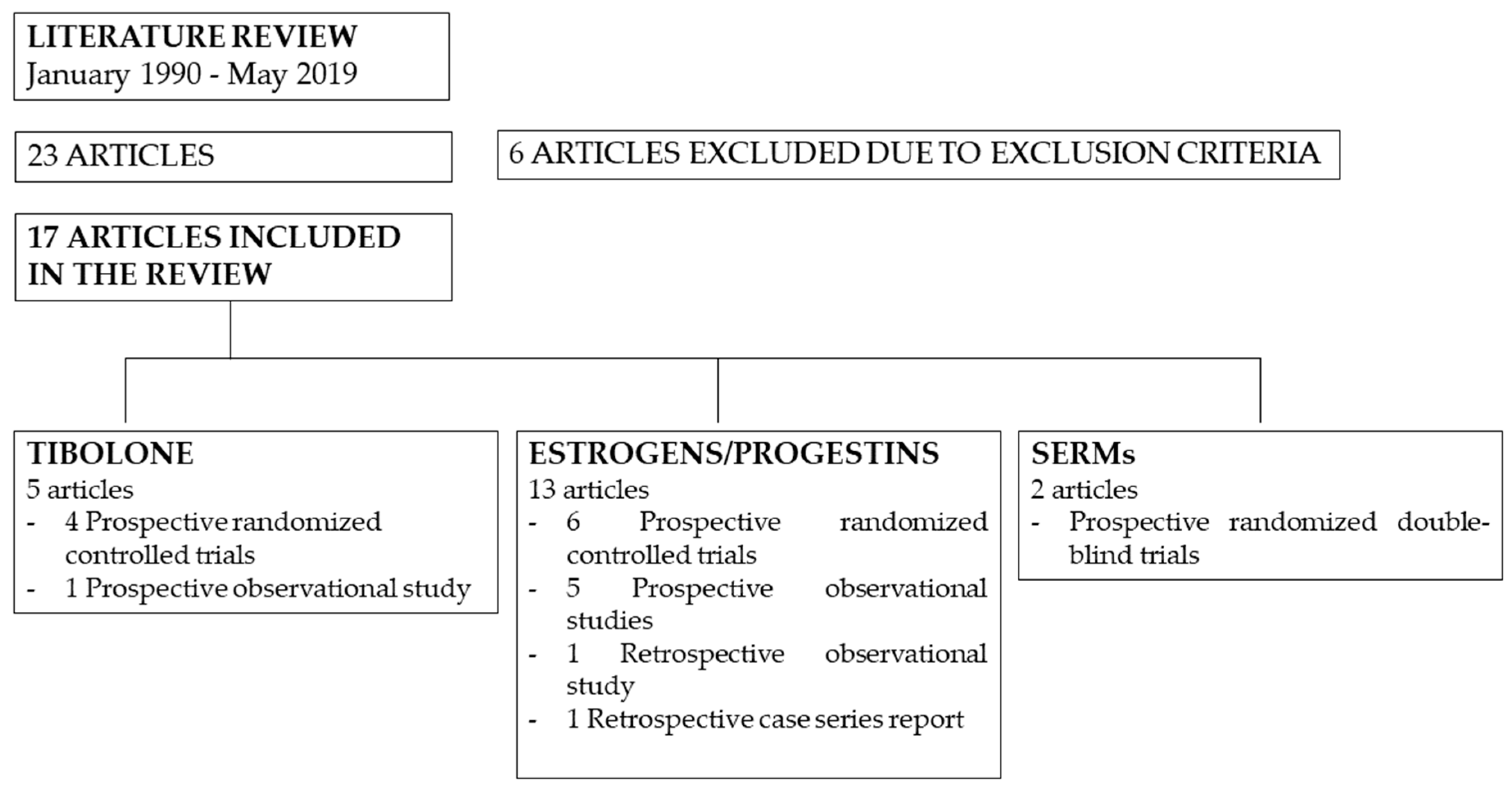
2. Materials and Methods
Search Strategy and Selection Criteria
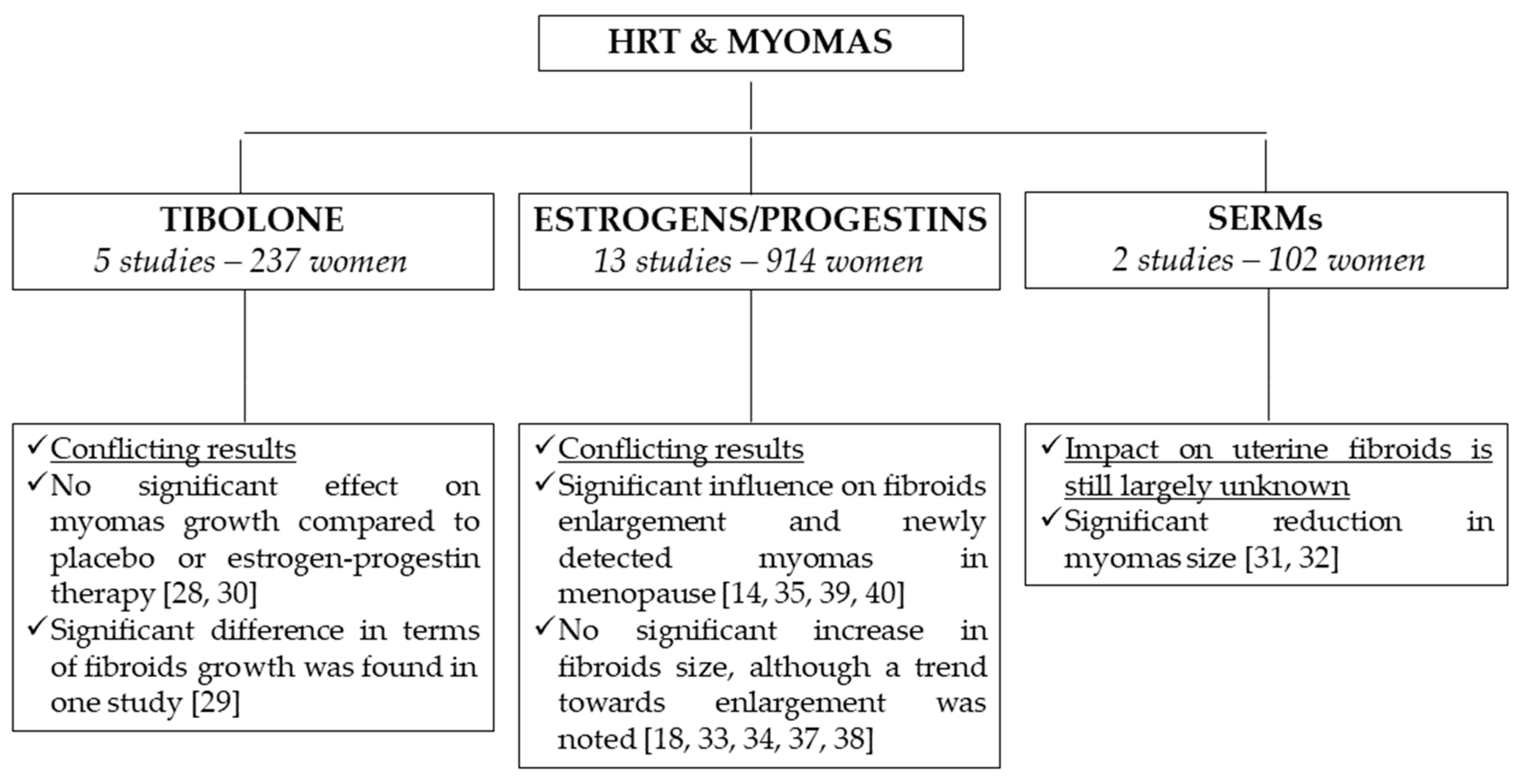
3. Results
3.1. Tibolone
3.2. Estrogens/Progestins
3.3. The Role of Progestins
3.4. SERM
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Moravek, M.B.; Bulun, S.E. Endocrinology of Uterine Fibroids: Steroid Hormones, Stem Cells, and Genetic Contribution. Curr. Opin. Obstet. Gynecol. 2015, 27, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Seracchioli, R.; Colombo, F.; Bagnoli, A.; Govoni, F.; Missiroli, S.; Venturoli, S. Laparoscopic myomectomy for fibroids penetrating the uterine cavity: Is it a safe procedure? BJOG Int. J. Obstet. Gynaecol. 2003, 110, 236–240. [Google Scholar] [CrossRef]
- Seracchioli, R.; Manuzzi, L.; Vianello, F.; Gualerzi, B.; Savelli, L.; Paradisi, R.; Venturoli, S. Obstetric and delivery outcome of pregnancies achieved after laparoscopic myomectomy. Fertil. Steril. 2006, 86, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Seracchioli, R. Fertility and obstetric outcome after laparoscopic myomectomy of large myomata: A randomized comparison with abdominal myomectomy. Hum. Reprod. 2000, 15, 2663–2668. [Google Scholar] [CrossRef] [PubMed]
- Townsend, D.E.; Sparkes, R.S.; Baluda, M.C.; McClelland, G. Unicellular histogenesis of uterine leiomyomas as determined by electrophoresis by glucose-6-phosphate dehydrogenase. Am. J. Obstet. Gynecol. 1970, 107, 1168–1173. [Google Scholar] [CrossRef]
- Wise, L.A.; Palmer, J.R.; Harlow, B.L.; Spiegelman, D.; Stewart, E.A.; Adams-Campbell, L.L.; Rosenberg, L. Reproductive Factors, Hormonal Contraception, and Risk of Uterine Leiomyomata in African-American Women: A Prospective Study. Am. J. Epidemiol. 2004, 159, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Marshall, L.M.; Spiegelman, D.; Goldman, M.B.; E Manson, J.; Colditz, G.A.; Barbieri, R.L.; Stampfer, M.J.; Hunter, D.J. A prospective study of reproductive factors and oral contraceptive use in relation to the risk of uterine leiomyomata. Fertil. Steril. 1998, 70, 432–439. [Google Scholar] [CrossRef]
- Laughlin, S.K.; Schroeder, J.C.; Baird, D.D. New Directions in the Epidemiology of Uterine Fibroids. Semin. Reprod. Med. 2010, 28, 204–217. [Google Scholar] [CrossRef]
- Frascà, C.; Tuzzato, G.; Arena, A.; Degli Esposti, E.; Zanello, M.; Raimondo, D.; Seracchioli, R. The Role of Pelvic Ultrasound in Preoperative Evaluation for Laparoscopic Myomectomy. J. Minim. Invasive Gynecol. 2018, 25, 679–683. [Google Scholar] [CrossRef]
- Frascà, C.; Degli Esposti, E.; Arena, A.; Tuzzato, G.; Moro, E.; Martelli, V.; Seracchioli, R. Can In-Bag Manual Morcellation Represent an Alternative to Uncontained Power Morcellation in Laparoscopic Myomectomy? A Randomized Controlled Trial. Gynecol. Obstet. Investig. 2018, 83, 52–56. [Google Scholar] [CrossRef]
- Casadio, P.; Guasina, F.; Morra, C.; Talamo, M.T.; Leggieri, C.; Frisoni, J.; Seracchioli, R. Hysteroscopic myomectomy: Techniques and preoperative assessment. Minerva Ginecol. 2016, 68, 154–166. [Google Scholar] [PubMed]
- Seracchioli, R.; Venturoli, S.; Colombo, F.; Bagnoli, A.; Vianello, F.; Govoni, F.; Guerrini, M.; Gualerzi, B. GnRH Agonist Treatment before Total Laparoscopic Hysterectomy for Large Uteri. J. Am. Assoc. Gynecol. Laparosc. 2003, 10, 316–319. [Google Scholar] [CrossRef]
- Segars, J.H.; Parrott, E.C.; Nagel, J.D.; Guo, X.C.; Gao, X.; Birnbaum, L.S.; Pinn, V.W.; Dixon, D. Proceedings from the Third National Institutes of Health International Congress on Advances in Uterine Leiomyoma Research: Comprehensive review, conference summary and future recommendations. Hum. Reprod. Updat. 2014, 20, 309–333. [Google Scholar] [CrossRef] [PubMed]
- Sener, A.B.; Seçkin, N.C.; Ozmen, S.; Gökmen, O.; Doğu, N.; Ekici, E. The effects of hormone replacement therapy on uterine fibroids in postmenopausal women. Fertil. Steril. 1996, 65, 354–357. [Google Scholar] [PubMed]
- Wu, J.; Cheng, Y. Research on the relationship between estrogen receptor, progesterone receptor, cell proliferation associated antigen in uterine leiomyoma and nuclear body density of myoma, serum reproductive hormone concentrations. Zhonghua fu Chan ke za Zhi 1995, 30, 603–607. [Google Scholar] [PubMed]
- Rein, M.S. Advances in Uterine Leiomyoma Research: The Progesterone Hypothesis. Environ. Health Perspect. 2000, 108, 791–793. [Google Scholar] [CrossRef] [PubMed]
- Shozu, M.; Murakami, K.; Inoue, M. Aromatase and Leiomyoma of the Uterus. Semin. Reprod. Med. 2004, 22, 51–60. [Google Scholar] [PubMed]
- Chang, I.J.; Hong, G.Y.; Oh, Y.L.; Kim, B.R.; Park, S.N.; Lee, H.-H.; Na, Y.-J.; Namkung, J. Effects of Menopausal Hormone Therapy on Uterine Myoma in Menopausal Women. J. Menopausal Med. 2013, 19, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Gregoriou, O.; Vitoratos, N.; Papadias, C.; Konidaris, S.; Costomenos, D.; Chryssikopoulos, A. Effect of tibolone on postmenopausal women with myomas. Maturitas 1997, 27, 187–191. [Google Scholar] [CrossRef]
- Cermik, D.; Arici, A.; Taylor, H.S. Coordinated regulation of HOX gene expression in myometrium and uterine leiomyoma. Fertil. Steril. 2002, 78, 979–984. [Google Scholar] [CrossRef]
- Srinivasan, V.; Martens, M.G. Hormone therapy in menopausal women with fibroids: Is it safe? Menopause 2018, 25, 930–936. [Google Scholar] [CrossRef] [PubMed]
- Brandon, D.D.; Bethea, C.L.; Strawn, E.Y.; Novy, M.J.; Burry, K.A.; Harrington, M.S.; Erickson, T.E.; Warner, C.; Keenan, E.J.; Clinton, G.M. Progesterone receptor messenger ribonucleic acid and protein are overexpressed in human uterine leiomyomas. Am. J. Obstet. Gynecol. 1993, 169, 78–85. [Google Scholar] [CrossRef]
- Nisolle, M.; Gillerot, S.; Casanas-Roux, F.; Squifflet, J.; Berliere, M.; Donnez, J. Immunohistochemical study of the proliferation index, oestrogen receptors and progesterone receptors A and B in leiomyomata and normal myometrium during the menstrual cycle and under gonadotrophin-releasing hormone agonist therapy. Hum. Reprod. 1999, 14, 2844–2850. [Google Scholar] [CrossRef] [PubMed]
- Plewka, D.; Marczyński, J.; Morek, M.; Bogunia, E.; Plewka, A. Receptors of Hypothalamic-Pituitary-Ovarian-Axis Hormone in Uterine Myomas. BioMed Res. Int. 2014, 2014, 521313. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Research on the Menopause in the 1990s. Report of a WHO Scientific Group; WHO Technical Report Series; World Health Organization: Geneva, Switzerland, 1996; Volume 866, pp. 1–107. [Google Scholar]
- Grisendi, V.; Spada, E.; Argento, C.; Plebani, M.; Milani, S.; Seracchioli, R.; Volpe, A.; La Marca, A. Age-specific reference values for serum FSH and estradiol levels throughout the reproductive period. Gynecol. Endocrinol. 2014, 30, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Gregoriou, O.; Konidaris, S.; Botsis, D.; Papadias, C.; Makrakis, E.; Creatsas, G. Long term effects of Tibolone on postmenopausal women with uterine myomas. Maturitas 2001, 40, 95–99. [Google Scholar] [CrossRef]
- De Aloysio, D.; Altieri, P.; Penacchioni, P.; Salgarello, M.; Ventura, V. Bleeding patterns in recent postmenopausal outpatients with uterine myomas: Comparison between two regimens of HRT. Maturitas 1998, 29, 261–264. [Google Scholar] [CrossRef]
- Fedele, L.; Bianchi, S.; Raffaelli, R.; Zanconato, G. A randomized study of the effects of tibolone and transdermal estrogen replacement therapy in postmenopausal women with uterine myomas. Eur. J. Obstet. Gynecol. Reprod. Biol. 2000, 88, 91–94. [Google Scholar] [CrossRef]
- Simsek, T.; Karakus, C.; Trak, B. Impact of different hormone replacement therapy regimens on the size of myoma uteri in postmenopausal period Tibolone versus transdermal hormonal replacement system. Maturitas 2002, 42, 243–246. [Google Scholar] [CrossRef]
- Palomba, S.; Sammartino, A.; Di Carlo, C.; Affinito, P.; Zullo, F.; Nappi, C. Effects of raloxifene treatment on uterine leiomyomas in postmenopausal women. Fertil. Steril. 2001, 76, 38–43. [Google Scholar] [CrossRef]
- Palomba, S.; Orio, F.; Russo, T.; Falbo, A.; Tolino, A.; Lombardi, G.; Cimini, V.; Zullo, F. Antiproliferative and proapoptotic effects of raloxifene on uterine leiomyomas in postmenopausal women. Fertil. Steril. 2005, 84, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Colacurci, N.; De Franciscis, P.; Cobellis, L.; Nazzaro, G.; De Placido, G. Effects of hormone replacement therapy on postmenopausal uterine myoma. Maturitas 2000, 35, 167–173. [Google Scholar] [CrossRef]
- Palomba, S.; Sena, T.; Noia, R.; Carlo, C.D.; Zullo, F.; Mastrantonio, P. Transdermal Hormone Replacement Therapy in Postmenopausal Women with Uterine Leiomyomas. Obstet. Gynecol. 2001, 98, 1053–1058. [Google Scholar] [PubMed]
- Polatti, F.; Viazzo, F.; Colleoni, R.; Nappi, R.E. Uterine myoma in postmenopause: A comparison between two therapeutic schedules of HRT. Maturitas 2000, 37, 27–32. [Google Scholar] [CrossRef]
- Ylöstalo, P.; Granberg, S.; Bäckström, A.-C.; Hirsjärvi-Lahti, T. Uterine findings by transvaginal sonography during percutaneous estrogen treatment in postmenopausal women. Maturitas 1996, 23, 313–317. [Google Scholar] [CrossRef]
- Schwartz, L.B.; Simcha, L.; Meryl, M.; Nactigall, L.E.; Horan, C.; Goldstein, S.R. Does the Use of Postmenopausal Hormone Replacement Therapy Influence the Size of Uterine Leiomyomata? A Preliminary Report. Menopause 1996, 3, 38–41. [Google Scholar] [CrossRef]
- Yang, C.; Lee, J.; Hsu, S.; Kuo, C.; Tsai, E. Effect of hormone replacement therapy on uterine fibroids in postmenopausal women—A 3-year study. Maturitas 2002, 43, 35–39. [Google Scholar] [CrossRef]
- Frigo, P.; Eppel, W.; Asseryanis, E.; Sator, M.; Golaszewski, T.; Gruber, D.; Lang, C.; Huber, J. The effects of hormone substitution in depot form on the uterus in a group of 50 perimenopausal women—A vaginosonographic study. Maturitas 1995, 21, 221–225. [Google Scholar] [CrossRef]
- Palomba, S.; Sena, T.; Morelli, M.; Noia, R.; Zullo, F.; Mastrantonio, P. Effect of different doses of progestin on uterine leiomyomas in postmenopausal women. Eur. J. Obstet. Gynecol. Reprod. Biol. 2002, 102, 199–201. [Google Scholar] [CrossRef]
- Huang, K.-E.; Baber, R. Updated clinical recommendations for the use of tibolone in Asian women. Climacteric 2010, 13, 317–327. [Google Scholar] [CrossRef]
- An, K.-C. Selective Estrogen Receptor Modulators. Asian Spine J. 2016, 10, 787–791. [Google Scholar] [CrossRef] [PubMed]
- Del Pup, L. Ospemifene: A safe treatment of vaginal atrophy. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 3934–3944. [Google Scholar] [PubMed]
- Johnson, K.; Hauck, F. Conjugated Estrogens/Bazedoxifene (Duavee) for Menopausal Symptoms. Am. Fam. Physician 2016, 93, 307–314. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Author | Study Design (Duration of HRT) and Objective | Patients | Type of HRT | Baseline | Follow-Up | p Value | Other Findings |
|---|---|---|---|---|---|---|---|
| Chang et al. (2013) [18] | Retrospective observational study (12 months) Myoma volume assessed every 6 months | 38 women with uterine fibroids HRT (n = 32) No HRT (n = 6) | Oral estrogen (n = 22) 0.625 mg CEE daily Estradiol-17-valerate Transdermal estrogen (n = 10) 50 mcg 17-β-estradiol patch 1.5 mg 17-β-estradiol gel MPA 5 mg Micronized progesterone 200 mg Continuous combined pattern (n = 16) Sequential cyclic pattern (n = 16) | Myoma volume (cm3) Control: 17.6 ± 26.8 HRT: 19.5 ± 24.5 | Myoma volume (cm3) 6 months | Increase in size HRT: 9/32 (28.1%) No change in size HRT: 13/32 (40.6%) Decrease in size HRT: 10/32 (31.3%) | |
| Control: 16.5 ± 23.2 | NS | ||||||
| HRT: 24.7 ± 35.1 | NS | ||||||
| 12 months | |||||||
| Control: 21.1 ± 34.6 | NS | ||||||
| HRT: 28.5 ± 56.4 | NS | ||||||
| Colacurci et al. (2000) [33] | Prospective observational study (12 months) Myoma size and uterine arteries pulsatility index (PI) | 60 menopausal on HRT Group A (n = 20). No uterine fibroids Group B (n = 15) Single asymptomatic fibroid < 3 cm, IM or SS
Group C (n = 18) Single asymptomatic fibroid >3 cm, IM or SS
| Continuous transdermal 17-beta-estradiol 0.05 mg/day plus nomegestrol acetate 5 mg/day sequentially added (days 17 to 28) | Myoma volume (cm3) B + C: 24.1 ± 20.0 Uterine artery PI A: 2.4 ± 0.5* B: 1.7 ± 0.2* C: 1.6 ± 0.3* | Myoma volume (cm3) 3 months | Increased in volume B: 2/33 (6.1%) C: 6/33 (18.1%) Total: 8/33 (24.2%) | |
| 26.1 ± 22.3 | NS | ||||||
| 6 months | |||||||
| 26.6 ± 25.6 | NS | ||||||
| 9 months | |||||||
| 27.8 ± 28.0 | NS | ||||||
| 12 months | |||||||
| 28.8 ± 30.0 | NS | ||||||
| Uterine artery PI 3 months | |||||||
| A: 2.2 ± 0.3 | NS | ||||||
| B: 1.9 ± 0.2 # | <0.01 | ||||||
| C: 1.9 ± 0.2 # | <0.01 | ||||||
| 6 months | |||||||
| A: 2.3 ± 0.3 | NS | ||||||
| B: 1.9 ± 0.2 | |||||||
| C: 1.9 ± 0.2 | |||||||
| 9 months | NS | ||||||
| A: 2.2 ± 0.3 | |||||||
| B: 1.9 ± 0.2 | |||||||
| C: 1.9 ± 0.2 | |||||||
| 12 months | NS | ||||||
| A: 2.2 ± 0.3 | |||||||
| B: 1.9 ± 0.2 | |||||||
| C: 1.9 ± 0.2 | |||||||
| De Aloysio et al. (1998) [28] | Prospective randomized controlled trial (12 months) Myoma size and bleeding patterns | 50 women, 47 completed the study 1 to 4 asymptomatic submucous or intramural leiomyomas with the longest diameter ranging from 3 to 8 cm | Group A (n = 24): Tibolone 2.5 mg/day Group B (n = 23): CEE 0.625 mg/day plus MPA 5 mg/day. | NA | NA—no difference in terms of size | Irregular bleeding incidence A: 22.6% of cycles B: 29.7% of cycles Irregular spotting incidence A: 2.4% B: 4.7% Bleeding and spotting lengths did not differ between the two groups | |
| Fedele et al. (2000) [29] | Prospective randomized controlled trial (12 months) Uterine and myoma size, myoma number. Symptoms and menstrual patterns. | 38 women with 1 or more uterine myomas, at least one with a diameter ≥3 cm. | Group A (n = 20): Transdermal estradiol-releasing system, 50 mcg/day + oral MPA 10 mg/day for 12 days/month Group B (n = 18): Tibolone 2.5 mg/day. | No. of myomas A: 1.75 ± 0.79 B: 1.62 ± 0.82 Volume of largest (cm3) A: 26.8 ± 12.5 B: 28.1 ± 14.1 | No. of myomas 6 months | ||
| A: 1.95 ± 0.94 | NS | ||||||
| B: 1.70 ± 0.91 | NS | ||||||
| 12 months | |||||||
| A: 2.15 ± 0.93 # | <0.01 | ||||||
| B: 1.67 ± 0.85 | NS | ||||||
| Volume of largest (cm3) | |||||||
| 6 months | |||||||
| A: 32.5 ± 14.2 # | <0.01 | ||||||
| B: 30.2 ± 12.8 | NS | ||||||
| 12 months | |||||||
| A: 35.8 ± 0.17 # | <0.01 | ||||||
| B: 30.6 ± 16.2 | NS | ||||||
| Frigo et al. (1995) [39] | Prospective observational trial (12 months) Myoma size and number | 50 perimenopausal women | 4 mg estradiol-valerate + 200 mg prasteronenantate intramuscular injections every 6-10 weeks | Mean diameter (mm) | Mean diameter (mm) | ||
| 29.4 mm | 35.0 mm | <0.01 | |||||
| Mean number | Mean number | ||||||
| 2.2. | 3.5 | NS | |||||
| Gregoriou et al. (1997) [19] | Prospective randomized controlled trial (12 months) Myoma size | 40 women with at least 1 myoma measuring >20 mm | Group A (n = 20): Tibolone 2.5 mg/day Group B (n = 20): no treatment | Myoma volume (cm3) | Myoma volume (cm3) 12 months | Increase in size A: 3/20 (15%) B: 2/20 (10%) Constant size A: 14/20 (70%) B: 15/20 (75%) Decrease in size A: 3/20 (15%) B: 3/20 (15%) | |
| A: 102.6 | A: 98.2 | NS | |||||
| B: 118.4 | B: 117.5 | NS | |||||
| Gregoriou et al. (2001) [27] | Prospective observational study (36 months) Myoma size and uterine arteries PI | 66 women Group A (n = 20) No myomas Group B (n = 23) Single asymptomatic IM-SS myoma ≤2 cm Group C (n = 23) Single asymptomatic IM-SS myoma 2–5 cm | Tibolone 2.5 mg/day | Myoma volume (cm3) B: 15.8 ± 1.4 C: 28.2 ± 1.6 Uterine artery PI A: 2.44 ± 0.35 * B: 1.62 ± 0.25 * C: 1.72 ± 0.23 * | Myoma volume | Increase in size B: 2/23 (8.7%) C: 3/23 (13.1%) Constant size B: 21/23 (91.3%) C: 20/23 (86.9%) | |
| NA | |||||||
| Uterine artery PI 6 months | |||||||
| A: 2.25 ± 0.31 # | <0.01 | ||||||
| B: 1.83 ± 0.21 # | <0.01 | ||||||
| C: 1.91 ± 0.22 # | <0.01 | ||||||
| 36 months | |||||||
| A: 2.22 ± 0.29 | NS | ||||||
| B: 1.86 ± 0.20 | NS | ||||||
| C: 1.94 ± 0.20 | NS | ||||||
| Palomba et al. (2001) [34] | Prospective nonrandomized observational trial (12 months) Myomas size Uterine bleeding pattern | 92 women Group A (n = 31) With 1 or 2 IM-SS myomas > 20 mm Group B (n = 31) With 1 or 2 IM-SS myomas > 20 mm Group C (n = 30) No leiomyomas | Group A Transdermal estradiol patches (50 mcg/day) plus oral MPA (2.5 mg/day), continuously added Group B Placebo (calcium carbonate) Group C Transdermal estradiol patches (50 mcg/day) plus oral MPA (2.5 mg/day), continuously added | Myoma volume (cm3) A: 141.7 ± 37.8 B: 150.3 ± 58.7 | Myoma volume (cm3) 12 months | Increase in size A: 8/31 (25.8%) B: 6/31 (19.4%) Unchanged A: 17/31 (54.8%) B: 19/31 (61.3%) Decreased in size A: 6/31 (19.4%) B: 6/31 (19.4%) | |
| A: 147.5 ± 53.3 | NS | ||||||
| B: 156.0 ± 72.5 | NS | ||||||
| Amenorrhea (incidence) 3 months | |||||||
| A: 56.5% § | <0.05 | ||||||
| B: 87.1% | NS | ||||||
| C: 51.4% § | <0.05 | ||||||
| 12 months | |||||||
| A: 76.8% | NS | ||||||
| B: 86.0% | NS | ||||||
| C: 76.4% | NS | ||||||
| N of AUB 3 months | |||||||
| A: 0.54 ± 0.75 § | <0.05 | ||||||
| B: 0.22 ± 0.21 | NS | ||||||
| C: 0.61 ± 0.74 § | <0.05 | ||||||
| 12 months | |||||||
| A: 0.23 ± 0.42 | NS | ||||||
| B: 0.19 ± 0.19 | NS | ||||||
| C: 0.24 ± 0.43 | NS | ||||||
| Severity of AUB 3 months | |||||||
| A: 1.51 ± 0.56 § | <0.05 | ||||||
| B: 0.92 ± 0.23 | NS | ||||||
| C: 1.64 ± 0.68 § | <0.05 | ||||||
| 12 months | |||||||
| A: 1.06 ± 0.25 | NS | ||||||
| B: 0.86 ± 0.22 | NS | ||||||
| C: 1.05 ± 0.24 | NS | ||||||
| Palomba et al. (2002) [40] | Prospective randomized controlled trial (12 months) Myomas size Uterine bleeding pattern | 27 women with 1–2 uterine leiomyomas > 20 mm | Group A (n = 14) Oral micronized estradiol 2 mg/day plus MPA 2.5 mg/day Group B (n = 13) Oral micronized estradiol 2 mg/day plus MPA 5 mg/day | Myoma dimensions (mm) A: 186.6 ± 77.6 B: 169.7 ± 85.1 | Myoma dimensions (mm) | Increased in size A: 3/14 (21.4%) B: 7/13 (53.8%) Unchanged A: 8/14 (57.1%) B: 4/13 (30.8%) Decreased in size A: 3/13 (23.1%) B: 2/14 (14.3%) | |
| 12 months | |||||||
| A: 198.6 ± 97.6 | NS | ||||||
| B: 201.3 ± 93.8 * | <0.05 | ||||||
| Amenorrhea | |||||||
| 3 months | |||||||
| A: 51.3% § | <0.05 | ||||||
| B: 52.4% § | <0.05 | ||||||
| 12 months | |||||||
| A: 76.9% | NS | ||||||
| B: 80.9% | NS | ||||||
| N of AUB | |||||||
| 3 months | |||||||
| A: 0.59 ± 0.81 § | <0.05 | ||||||
| B: 0.63 ± 0.86 § | <0.05 | ||||||
| 12 months | |||||||
| A: 0.21 ± 0.41 | NS | ||||||
| B: 0.24 ± 0.43 | NS | ||||||
| Severity of AUB | |||||||
| 3 months | |||||||
| A: 1.53 ± 0.71 § | <0.05 | ||||||
| B: 1.58 ± 0.66 § | <0.05 | ||||||
| 12 months | |||||||
| A: 1.12 ± 0.32 | NS | ||||||
| B: 1.13 ± 0.35 | NS | ||||||
| Palomba et al. (2001) [31] | Prospective randomized double-blind trial (12 months: 12 cycles of 28 days) Myoma size Amenorrhea AUB number and severity | 62 postmenopausal women with 1-2 leiomyomas measuring > 20 mm | Group A (n = 31) Raloxifene 60 mg/day Group B (n = 31) Placebo | Myoma volume (cm3) A: 127.1 ± 38.2 B: 138.6 ± 55.7 | Myoma volume (cm3) NA, significantly reduced Amenorrhea incidence and AUB number and severity: comparable within and between groups | <0.05 | Decreased in size 3 cycles 1/31 (3.2%) 6 cycles 13/31 (41.9%) 9 cycles 24/31 (77.4%) 12 cycles 26/31 (83.9%) |
| Palomba et al. (2005) [32] | Prospective randomized double-blind trial (84 days: 3 cycles of 28 days) Myoma size | 40 postmenopausal women with 1-2 intramural uterine leiomyomas, one measuring >2 cm | Treatment group (TG) (n = 20) Raloxifene hydrochloride 180 mg/day Control group (CG) (n = 20) Placebo | Myoma volume (cm3) TG: 141.7 ± 37.8 CG: 150.3 ± 58.7 | Myoma volume (cm3) TG: 116.3 ± 27.4 CG: 150.4 ± 58.0 P = 0.022 (between TG and CG) | <0.05 | Mean change in leiomyoma size: TG: -17.4 ± 6.1 CG: 1.9 ± 1.1 |
| Polatti et al. (2000) [35] | Prospective randomized controlled trial (24 months) Myoma size and new formation of fibroids | 224 women No myomas Group A (n = 76) Group B (n = 74) Myomas Group C (n = 38) Group D (n = 36) | Single-phase cyclic estradiol valerate 2 mg/day and cyproterone acetate 1 mg/day for 21 days + 7-day break. Groups A and C Combined sequential cyclic transdermal estradiol 50 mcg/day and MPA 10 mg/day days 10-21, 7-day break. Groups B and D. | Myoma volume (cm3) C: 18.6 ± 1.4 D: 19.3 ± 1.3 | Myoma volume (cm3) | Group B In 4 women (5.4%) new onset of fibromas, mean size 25.4 ± 1.2 Group D Mean increase in myoma volumes of 25.3% after 24 months Group C Mean increase in myoma volumes of 4.8% after 24 mo. | |
| 12 months | |||||||
| C: 19.2 ± 1.1 # | <0.01 | ||||||
| D: 23.8 ± 0.9 * # | <0.01 | ||||||
| 24 months | |||||||
| C: 19.5 ± 1.1 # | <0.01 | ||||||
| D: 24.2 ±0.8 * # | <0.01 | ||||||
| Schwartz et al. (1996) [37] | Retrospective case series report (HRT 19.7 ± 6.3 months, Controls 9.7 ± 1.7 months) Myoma size | Case group 14 cases with uterine leiomyomas treated with HRT (23 myomas) Control group 7 cases with uterine leiomyomas untreated (8 myomas) | CEE 0.625 mg/day (m = 7) Micronized estradiol 1 mg/day (n = 5) Transdermal 50 mcg estradiol patch (n = 2). MPA (n = 11) Micronized progesterone (n = 3) Cyclical regimen (MPA 10 mg for 12 days/month) (n = 10) Continuous combined (MPA 2.5 mg/day) (n = 4) | Myoma volume (cm3) | Myoma volume (cm3) | Mean change in myoma volume Case: +13.9 ± 8.2 Control: -2.0 ± 1.9 Increase in size Case: 17/23 (73.9%) Control: 2/8 (25%) Decrease in size Case: 6/23 (26.1%) Control: 5/8 (62.5%) Unchanged Control: 1/8 (12.5%) | |
| Case: 15.7 ± 5.5 | Case: 29.6 ± 12.2 | NS | |||||
| Control: 4.5 ± 2.5 | Control: 2.5 ± 1.1 | NS | |||||
| Sener et al. (1996) [14] | Prospective randomized controlled trial (12 months) Myoma size | 40 menopausal women with at least one myoma <20 mm | Group I (n = 22) Transdermal 50 mcg/day estradiol + 5 mg MPA continuously Group II (n = 18) Oral CEE 0.625 mg + 2.5 mg MPA continuously | Myoma diameter (mm) | Myoma diameter (mm) | No difference in E2 levels between the two groups | |
| I: 14.3 ± 5.9 | I: 19.7± 12.4 # | <0.05 | |||||
| II: 15.8 ± 6.3 | II: 15.7 ± 6.7 | NS | |||||
| Simsek et al. (2002) [30] | Prospective randomized controlled trial (6 months) Myoma size | 46 women with leiomyomas | Group A (n = 24, 32 myomas) Tibolone 2.5 mg/day Group B (n = 22, 28 myomas) Transdermal estradiol 0.05 mg/day for 4 weeks + norethisterone acetate 0.25 mg/day for 2 weeks | Myoma volume (cm3) | Myoma volume (cm3) | Increased in size A: 4/32 (12.5%) NS B: 6/28 (21.4%) | |
| A: 18.6 ± 4.1 | A: 20.1 ± 4.0 | NS | |||||
| B: 23.1 ± 3.6 | B: 27.2± 3.9 | NS | |||||
| Yang et al. (2002) [38] | Prospective observational trial (36 months) Myoma size | 72 women with leiomyomas > 20 mm | HRT group (n = 37) CEE 0.625 mg/day + MPA 5 mg/day Control group (n = 35) No therapy | Myoma volume (cm3) HRT: 21.7 ± 11.7 Controls: 19.4 ± 8.7 | Myoma volume (cm3) | Increased in size 1st year HRT: 4/37 (10.8%) NS Controls: 2/35 (5.7%) 2nd year HRT: 5/37 (13.5%) Controls: 2/35 (5.7%) 3rd year HRT: 3/37 (8.1%) Controls: 1/35 (2.9%) | |
| 1st year | |||||||
| HRT: 23.2 ± 12.5 | |||||||
| Controls: 20.4 ± 9.4 | NS | ||||||
| 2nd year | |||||||
| HRT: 23.7 ± 12.8 | NS | ||||||
| Controls: 20.7 ± 9.4 | |||||||
| 3rd year | |||||||
| HRT: 23.5 ± 12.8 | NS | ||||||
| Controls: 20.1 ± 9.3 | |||||||
| Ylostalo P et al. (1996) [36] | Prospective observational trial (12 months) Myoma size | 159 patients–80 studied by TVS–19 had myomas >8 mm | Group 1 (2 months-3 years postmenopausal) 1 mg transdermal estradiol + 10 mg MPA/day for 12 days every month Group 2 (> 3 years postmenopausal) 1 mg transdermal estradiol + 10 mg MPA/day for 12 days every month Group 3 (> 3 years postmenopausal) 1 mg transdermal estradiol + 10 mg MPA/day for 12 days every 3 months | Myoma diameter (mm) 1: 14.5 ± 5.2 2: 17.0 ± 7.2 3: 17.0 ± 6.6 | Mean diameters (mm) Mean increase: 26% over the first 6 months, no further increase during the last 6 months | NA |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moro, E.; Degli Esposti, E.; Borghese, G.; Manzara, F.; Zanello, M.; Raimondo, D.; Gava, G.; Arena, A.; Casadio, P.; Meriggiola, M.C.; et al. The Impact of Hormonal Replacement Treatment in Postmenopausal Women with Uterine Fibroids: A State-of-the-Art Review of the Literature. Medicina 2019, 55, 549. https://doi.org/10.3390/medicina55090549
Moro E, Degli Esposti E, Borghese G, Manzara F, Zanello M, Raimondo D, Gava G, Arena A, Casadio P, Meriggiola MC, et al. The Impact of Hormonal Replacement Treatment in Postmenopausal Women with Uterine Fibroids: A State-of-the-Art Review of the Literature. Medicina. 2019; 55(9):549. https://doi.org/10.3390/medicina55090549
Chicago/Turabian StyleMoro, Elisa, Eugenia Degli Esposti, Giulia Borghese, Federica Manzara, Margherita Zanello, Diego Raimondo, Giulia Gava, Alessandro Arena, Paolo Casadio, Maria Cristina Meriggiola, and et al. 2019. "The Impact of Hormonal Replacement Treatment in Postmenopausal Women with Uterine Fibroids: A State-of-the-Art Review of the Literature" Medicina 55, no. 9: 549. https://doi.org/10.3390/medicina55090549
APA StyleMoro, E., Degli Esposti, E., Borghese, G., Manzara, F., Zanello, M., Raimondo, D., Gava, G., Arena, A., Casadio, P., Meriggiola, M. C., & Seracchioli, R. (2019). The Impact of Hormonal Replacement Treatment in Postmenopausal Women with Uterine Fibroids: A State-of-the-Art Review of the Literature. Medicina, 55(9), 549. https://doi.org/10.3390/medicina55090549