
Cognitive Behavioral Therapy for Muscle Dysmorphia and Anabolic Steroid-Related Psychopathology: A Randomized Controlled Trial

Abstract

1. Introduction
1.1. The Role of Steroid and Performance-Enhancing Drug (PED) Use
1.2. Gaps in the Literature and the Study Rationale
2. Results
Therapeutic Narrative Illustration
- Therapist:
- “You said skipping leg day feels like a failure. What’s the fear behind that thought?”
- Client:
- “It’s like… if I don’t work out, I’ll lose all control. People will think I’m weak.”
- Therapist:
- “What might be a more balanced thought?”
- Client:
- “That one missed session won’t undo years of progress.”
- Client:
- “At first, all I saw was weakness. But when I looked longer, I noticed my shoulders are broader than I give myself credit for.”
- Therapist:
- “That shift—was it based on emotion or observation?”
- Client:
- “Observation. It felt different. More neutral.”
- Therapist:
- “What might help when the urge to measure your arms comes up?”
- Client:
- “Writing down what I’m feeling first. I did that once and realized I was just anxious about work.”
3. Discussion
3.1. Interpretation and Theoretical Implications
3.2. Comparison with Previous Studies
3.3. Clinical Implications
3.4. Limitations
4. Methods
4.1. Study Design
4.2. G*Power Analysis
4.3. Inclusion and Exclusion Criteria
4.4. Participants and Recruitment
4.5. Randomization Procedure
4.6. Handling of Missing Data
4.7. Measurement Tools
4.7.1. Muscle Dysmorphic Disorder Inventory (MDDI)
4.7.2. Bodybuilder Image Grid (BIG)
4.7.3. Kessler Psychological Distress Scale (K10)
4.7.4. Patient Health Questionnaire-9 (PHQ-9)
4.7.5. Eating Disorder Examination Questionnaire (EDE-Q)
4.7.6. Exercise Addiction Inventory (EAI)
4.8. Intervention
4.9. Procedure
4.10. Therapists and Quality Assurance
4.11. Statistical Analyses
4.12. Ethical Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MD | Muscle Dysmorphia |
| AAS | Anabolic–Androgenic Steroids |
| PEDs | Performance-Enhancing Drugs |
| CBT | Cognitive Behavioral Therapy |
| BDI-II | Beck Depression Inventory-II |
| BAI | Beck Anxiety Inventory |
| EDE-Q | Eating Disorder Examination Questionnaire |
| EAI | Exercise Addiction Inventory |
| MDDI | Muscle Dysmorphic Disorder Inventory |
| BIG | Bodybuilder Image Grid |
References
- Schulte, J.; Schulz, C.; Wilhelm, S.; Buhlmann, U. Treatment utilization and treatment barriers in individuals with body dysmorphic disorder. BMC Psychiatry 2020, 20, 69. [Google Scholar] [CrossRef] [PubMed]
- Cadman, J.; Turner, C. A clinician’s quick guide to evidence-based approaches: Body dysmorphic disorder. Clin. Psychol. 2025, 29, 103–108. [Google Scholar] [CrossRef]
- Czepczor-Bernat, K.; Modrzejewska, A.; Modrzejewska, J. #BodyPositivity: The role of body appreciation and body mass index for muscle dysmorphia, body attitudes and exercise motives among men. Nutrients 2025, 17, 1177. [Google Scholar] [CrossRef] [PubMed]
- Sandgren, S.S.; Lavallee, D. Muscle dysmorphia research neglects DSM-5 diagnostic criteria. J. Loss Trauma 2018, 23, 211–243. [Google Scholar] [CrossRef]
- Çınaroğlu, M. Exercise, anabolic steroid dependence, muscle dysmorphia, performance enhancement drug abuse. Nişantaşı Univ. J. Soc. Sci. 2023, 11, 443–454. [Google Scholar] [CrossRef]
- Nelson, B.S.; Hildebrandt, T.; Wallisch, P. Anabolic–androgenic steroid use is associated with psychopathy, risk-taking, anger, and physical problems. Sci. Rep. 2022, 12, 9133. [Google Scholar] [CrossRef] [PubMed]
- Snorrason, I.; Beard, C.; Christensen, K.; Bjornsson, A.S.; Björgvinsson, T. Body dysmorphic disorder and major depressive episode have comorbidity-independent associations with suicidality in an acute psychiatric setting. J. Affect. Disord. 2019, 259, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Duran, S.; Öz, Y.C. Examination of the association of muscle dysmorphia (bigorexia) and social physique anxiety in the male bodybuilders. Perspect. Psychiatr. Care 2022, 58, e12871. [Google Scholar] [CrossRef] [PubMed]
- Badenes-Ribera, L.; Rubio-Aparicio, M.; Sanchez-Meca, J.; Fabris, M.A.; Longobardi, C. The association between muscle dysmorphia and eating disorder symptomatology: A systematic review and meta-analysis. J. Behav. Addict. 2019, 8, 351–371. [Google Scholar] [CrossRef] [PubMed]
- Ceto, E.; Yigitoglu, P.H.; Yavuz, H.U. Relationship between anabolic–androgenic steroid use, aggression, and narcissism in male bodybuilders. Medicina 2025, 61, 241. [Google Scholar] [CrossRef] [PubMed]
- Laskowski, N.M.; Zaiser, C.; Müller, R.; Brandt, G.; Paslakis, G. Mapping the pathway to anabolic-androgenic steroids (AAS) use. Compr. Psychiatry 2025, 125, 152602. [Google Scholar] [CrossRef] [PubMed]
- Bond, P.; Smit, D.L.; de Ronde, W. Anabolic–androgenic steroids: How do they work and what are the risks? Front. Endocrinol. 2022, 13, 1059473. [Google Scholar] [CrossRef] [PubMed]
- Linhares, B.L.; Miranda, E.P.; Cintra, A.R.; Reges, R.; Torres, L.O. Use, misuse and abuse of testosterone and other androgens. Sex. Med. Rev. 2022, 10, 583–595. [Google Scholar] [CrossRef] [PubMed]
- Tauchen, J.; Jurášek, M.; Huml, L.; Rimpelová, S. Medicinal use of testosterone and related steroids revisited. Molecules 2021, 26, 1032. [Google Scholar] [CrossRef] [PubMed]
- Paasch, R.; Mau, G.; Korol, O. Perspectives, motivations and behaviors of amateur bodybuilders regarding doping and anti-doping: A systematic review. Perform. Enhanc. Health 2025, 13, 100336. [Google Scholar] [CrossRef]
- Berger, K.; Schiefner, F.; Rudolf, M.; Awiszus, F.; Junne, F.; Vogel, M.; Lohmann, C.H. Long-term effects of doping with anabolic steroids during adolescence on physical and mental health. Orthopädie 2024, 53, 608–616. [Google Scholar] [CrossRef] [PubMed]
- Di Girolamo, F.G.; Biasinutto, C.; Mangogna, A.; Fiotti, N.; Vinci, P.; Pisot, R.; Biolo, G. Metabolic consequences of anabolic steroids, insulin, and growth hormone abuse in recreational bodybuilders: Implications for the World Anti-Doping Agency Passport. Sports Med.-Open 2024, 10, 28. [Google Scholar] [CrossRef] [PubMed]
- Wen, J.; Syed, B.; Leapart, J.; Shehabat, M.; Ansari, U.; Akhtar, M.; Pai, D. Selective androgen receptor modulators (SARMs) effects on physical performance: A systematic review of randomized control trials. Clin. Endocrinol. 2025, 102, 3–27. [Google Scholar] [CrossRef] [PubMed]
- McCullough, D.; Webb, R.; Enright, K.J.; Lane, K.E.; McVeigh, J.; Stewart, C.E.; Davies, I.G. How the love of muscle can break a heart: Impact of anabolic androgenic steroids on skeletal muscle hypertrophy, metabolic and cardiovascular health. Rev. Endocr. Metab. Disord. 2021, 22, 389–405. [Google Scholar] [CrossRef] [PubMed]
- Leciejewska, N.; Jędrejko, K.; Gómez-Renaud, V.M.; Manríquez-Núñez, J.; Muszyńska, B.; Pokrywka, A. Selective androgen receptor modulator use and related adverse events including drug-induced liver injury: Analysis of suspected cases. Eur. J. Clin. Pharmacol. 2024, 80, 185–202. [Google Scholar] [CrossRef] [PubMed]
- Bonnecaze, A.K.; O’Connor, T.; Burns, C.A. Harm reduction in male patients actively using anabolic androgenic steroids (AAS) and performance-enhancing drugs (PEDs): A review. J. Gen. Intern. Med. 2021, 36, 2055–2064. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, V.G.; Justus, J.S.; Portela, L.V.C.; Rodolphi, M.S. Synaptic and extrasynaptic mitochondria: Features and impact of high anabolic-androgenic steroids use. In Handbook of Substance Misuse and Addictions: From Biology to Public Health; Springer: Cham, Switzerland, 2022; pp. 1–21. [Google Scholar]
- Karagun, B.; Altug, S. Anabolic-androgenic steroids are linked to depression and anxiety in male bodybuilders: The hidden psychogenic side of anabolic androgenic steroids. Ann. Med. 2024, 56, 2337717. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.F.; Chan, C.H.; Lin, C.H. Psychiatric complications of androgenic–anabolic steroid use in powerlifters. Indian J. Psychiatry 2025, 67, 542–544. [Google Scholar] [CrossRef] [PubMed]
- Chegeni, R.; Pallesen, S.; McVeigh, J.; Sagoe, D. Anabolic-androgenic steroid administration increases self-reported aggression in healthy males: A systematic review and meta-analysis of experimental studies. Psychopharmacology 2021, 238, 1911–1922. [Google Scholar] [CrossRef] [PubMed]
- Ünler, M.; Ekmekçi Ertek, İ.; Coşar, B.; Arıkan, Z. A case of psychosis with catatonic features triggered by human chorionic gonadotropin after anabolic steroid abuse. Psychiatr. Danub. 2022, 34, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Vilar Neto, J.D.O.; da Silva, C.A.; Bruno da Silva, C.A.; Pinto, D.V.; Caminha, J.D.S.R.; de Matos, R.S.; De Francesco Daher, E. Anabolic androgenic steroid-induced hypogonadism, a reversible condition in male individuals? A systematic review. Andrologia 2021, 53, e14062. [Google Scholar] [CrossRef] [PubMed]
- Cuadrado, J.; Laulan, P.; Sentenac, C.; Legigan, C.; Michel, G. “Bigger, stronger, sicker”, integrative psychological assessment for muscle dysmorphia: Case studies of two young women bodybuilders. Psychiatry Res. Case Rep. 2024, 3, 100212. [Google Scholar] [CrossRef]
- Çınaroğlu, M. Hormonal catalysts in the addiction cycle of muscle dysmorphia: A neuroendocrine perspective. J. Neurobehav. Sci. 2024, 11, 1–9. [Google Scholar] [CrossRef]
- MacPhail, D.C.; Oberle, C.D. Seeing shred: Differences in muscle dysmorphia, orthorexia nervosa, depression, and obsessive-compulsive tendencies among groups of weightlifting athletes. Perform. Enhanc. Health 2022, 10, 100213. [Google Scholar] [CrossRef]
- Gaudiano, M.C.; Aureli, F.; Manna, L.; Borioni, A.; Maccelli, A.; Raimondo, M.; Bartolomei, M. Illegal products containing selective androgen receptor modulators purchased online from Italy: Health risks for consumers. Sex. Med. 2024, 12, qfae018. [Google Scholar] [CrossRef] [PubMed]
- Hahamyan, H.A.; Vasireddi, N.; Voos, J.E.; Calcei, J.G. Social media’s impact on widespread SARMs abuse. Physician Sportsmed. 2023, 51, 291–293. [Google Scholar] [CrossRef] [PubMed]
- Hahamyan, H.A.; Basaria, S. Selective androgen receptor modulators—Transformative drugs or heralds of the next drug epidemic? JAMA 2024, 331, 1359–1360. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, M.; Zamani, Z.; Bagheri, E. Early maladaptive schemas, cognitive fusion, and anabolic-androgenic steroid use attitudes: The mediating role of muscle dysmorphia in Iran. J. Clin. Sport Psychol. 2024, 1, 396–413. [Google Scholar] [CrossRef]
- Skoufa, L.; Barkoukis, V.; Lazuras, L.; Tsorbatzoudis, H. Effect of muscle dysmorphia on image-and-performance-enhancement drugs use intentions in a non-clinical sample: The role of social cognition. Perform. Enhanc. Health 2021, 9, 100204. [Google Scholar] [CrossRef]
- Gawash, A.; Zia, H.; Al-Shehab, U.; Lo, D.F. Association of body dysmorphic–induced anabolic-androgenic steroid use with mental health outcomes: A systematic review. Prim. Care Companion CNS Disord. 2023, 25, 49582. [Google Scholar] [CrossRef] [PubMed]
- Burmeister, M.A. Bigorexia nervosa review. US Pharm. 2025, 50, 4–11. [Google Scholar]
- Çınaroğlu, M. Muscle dysmorphia and long-term anabolic steroid abuse: A 20-year case report. Topkapı Soc. Sci. J. 2024, 3, 9–13. [Google Scholar]
- Grunewald, W.; Blashill, A.J. Muscle dysmorphia. In Eating Disorders in Boys and Men; Musolino, J., Ed.; Routledge: London, UK, 2021; pp. 103–115. [Google Scholar]
- Zaami, S.; Minutillo, A.; Sirignano, A.; Marinelli, E. Effects of appearance-and performance-enhancing drugs on personality traits. Front. Psychiatry 2021, 12, 730167. [Google Scholar] [CrossRef] [PubMed]
- Zhao, F.; Guo, Z.; Bo, Y.; Feng, L.; Zhao, J. Is cognitive behavioral therapy an efficacious treatment for psychological interventions in body dysmorphic disorders? A meta-analysis based on current evidence from randomized controlled trials. J. Affect. Disord. 2024, 352, 237–249. [Google Scholar] [CrossRef] [PubMed]
- Kaidesoja, M.; Cooper, Z.; Fordham, B. Cognitive behavioral therapy for eating disorders: A map of the systematic review evidence base. Int. J. Eat. Disord. 2023, 56, 295–313. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.; Melkonian, M.; Karin, E.; Dear, B.F.; Titov, N.; Wootton, B.M. Predictors of response to cognitive behavioural therapy (CBT) for individuals with obsessive-compulsive disorder (OCD): A systematic review. Behav. Cogn. Psychother. 2023, 51, 302–319. [Google Scholar] [CrossRef] [PubMed]
- Gestsdottir, S.; Kristjansdottir, H.; Sigurdsson, H.; Sigfusdottir, I.D. Prevalence, mental health and substance use of anabolic steroid users: A population-based study on young individuals. Scand. J. Public Health 2021, 49, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Çınaroğlu, M.; Yılmazer, E.; Ülker, S.V.; Ahlatcıoğlu, E.N.; Sayar, G.H. Efficacy of cognitive-behavioral therapy in reducing muscle dysmorphia symptoms among Turkish gym goers: A pilot study. Acta Psychol. 2024, 250, 104542. [Google Scholar] [CrossRef] [PubMed]
- Martenstyn, J.A.; Russell, J.; Tran, C.; Griffiths, S.; Maguire, S. Evaluation of an 8-week telehealth cognitive-behavioural therapy (CBT) program for adults with muscle dysmorphia: A pilot and feasibility study. Body Image 2025, 52, 101842. [Google Scholar] [CrossRef] [PubMed]
- Martenstyn, J.A.; Aouad, P.; Touyz, S.; Maguire, S. Treatment of compulsive exercise in eating disorders and muscle dysmorphia: A systematic review and meta-analysis. Clin. Psychol. Sci. Pract. 2022, 29, 143. [Google Scholar] [CrossRef]
- Scarth, M.; Havnes, I.A.; Jørstad, M.L.; Bjørnebekk, A. Psychological traits associated with anabolic androgenic steroid use and dependence: An exploratory cross-sectional study among female athletes. BMC Women’s Health 2025, 25, 214. [Google Scholar] [CrossRef] [PubMed]
- Scarth, M.; Havnes, I.A.; Bjørnebekk, A. Anabolic-androgenic steroid use disorder: Case for recognition as a substance use disorder with specific diagnostic criteria. Br. J. Psychiatry 2025, 1, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Alzahrani, M.A.; Alali, S.; Alghuyaythat, W.K.Z.; Alotibi, A.N.A.; Alosailan, A.M.; Alshamrani, O.A.; Almannie, R. Anabolic-androgenic steroid use in Saudi Arabia and its impact on sexual and reproductive health: A systematic review. J. Pioneer. Med. Sci. 2025, 14, 41–53. [Google Scholar] [CrossRef]
- Siudziński, P.; Łyko, M.; Skoczylas, A.; Kurasz, J.; Maj, W.; Tomaszewska, W.; Golińska, M. Do anabolic androgenic steroids really cause harm? A comprehensive examination of adverse effects. Qual. Sport 2025, 37, 57735. [Google Scholar] [CrossRef]
- Prnjak, K.; Jukic, I.; Mitchison, D.; Griffiths, S.; Hay, P. Body image as a multidimensional concept: A systematic review of body image facets in eating disorders and muscle dysmorphia. Body Image 2022, 42, 347–360. [Google Scholar] [CrossRef] [PubMed]
- Möllmann, A.; Heinrichs, N.; Herwig, A. A conceptual framework on body representations and their relevance for mental disorders. Front. Psychol. 2024, 14, 1231640. [Google Scholar] [CrossRef] [PubMed]
- Pope, H.G., Jr.; Gruber, A.J.; Choi, P.; Olivardia, R.; Phillips, K.A. Muscle dysmorphia: An underrecognized form of body dysmorphic disorder. Psychosomatics 1997, 38, 548–557. [Google Scholar] [CrossRef] [PubMed]
- Longobardi, C.; Prino, L.E.; Fabris, M.A.; Settanni, M. Muscle dysmorphia and psychopathology: Findings from an Italian sample of male bodybuilders. Psychiatry Res. 2017, 256, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Cash, T.F. Cognitive-behavioral perspectives on body image. In Encyclopedia of Body Image and Human Appearance; Elsevier: Amsterdam, The Netherlands, 2012; Volume 1, pp. 334–342. [Google Scholar]
- Egan, S.J.; Shafran, R. Cognitive-behavioral treatment for perfectionism. In The Psychology of Perfectionism; Elsevier: Amsterdam, The Netherlands, 2017; pp. 284–305. [Google Scholar]
- Clark, D.A. Finding the self in a cognitive behavioral perspective. In The Self in Understanding and Treating Psychological Disorders; Guilford Press: New York, NY, USA, 2016; pp. 40–49. [Google Scholar]
- Castonguay, A.L.; Pila, E.; Wrosch, C.; Sabiston, C.M. Body-related self-conscious emotions relate to physical activity motivation and behavior in men. Am. J. Men’s Health 2015, 9, 209–221. [Google Scholar] [CrossRef] [PubMed]
- Readdy, T.; Cardinal, B.J.; Watkins, P.L. Muscle dysmorphia, gender role stress, and sociocultural influences: An exploratory study. Res. Q. Exerc. Sport 2011, 82, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Cerea, S.; Bottesi, G.; Pacelli, Q.F.; Paoli, A.; Ghisi, M. Muscle dysmorphia and its associated psychological features in three groups of recreational athletes. Sci. Rep. 2018, 8, 8877. [Google Scholar] [CrossRef] [PubMed]
- Dennis, A.; Ogden, J. The role of emotion regulation in body-focused gratitude: Impacts on well-being, body compassion, and behavioural intentions. Int. J. Appl. Posit. Psychol. 2025, 10, 27. [Google Scholar] [CrossRef]
- Joensberg, E.; Fagermyr, H.; Haugen, T.; Sandgren, S.S. The associations between passion for resistance training and muscle dysmorphia. Perform. Enhanc. Health 2025, 13, 100343. [Google Scholar] [CrossRef]
- Cooper, M.; Eddy, K.T.; Thomas, J.J.; Franko, D.L.; Carron-Arthur, B.; Keshishian, A.C.; Griffiths, K.M. Muscle dysmorphia: A systematic and meta-analytic review of the literature to assess diagnostic validity. Int. J. Eat. Disord. 2020, 53, 1583–1604. [Google Scholar] [CrossRef] [PubMed]
- Fagan, H.A.; Baldwin, D.S. Pharmacological treatment of generalised anxiety disorder: Current practice and future directions. Expert Rev. Neurother. 2023, 23, 535–548. [Google Scholar] [CrossRef] [PubMed]
- Chandler, C.G.; Grieve, F.G.; Derryberry, W.P.; Pegg, P.O. Are anxiety and obsessive-compulsive symptoms related to muscle dysmorphia. Int. J. Men’s Health 2009, 8, 143–154. [Google Scholar] [CrossRef]
- Foroughi, A.; Khanjani, S.; Asl, E.M. Relationship of concern about body dysmorphia with external shame, perfectionism, and negative affect: The mediating role of self-compassion. Iran. J. Psychiatry Behav. Sci. 2019, 13, e80186. [Google Scholar] [CrossRef]
- Greenway, C.W.; Price, C. Muscle dysmorphia and self-esteem in former and current users of anabolic-androgenic steroids. Perform. Enhanc. Health 2020, 7, 100154. [Google Scholar] [CrossRef]
- Bertozzi, G.; Salerno, M.; Pomara, C.; Sessa, F. Neuropsychiatric and behavioral involvement in AAS abusers. A literature review. Medicina 2019, 55, 396. [Google Scholar] [CrossRef] [PubMed]
- Foster, A.; Shorter, G.; Griffiths, M. Muscle dysmorphia: Could it be classified as an addiction to body image? J. Behav. Addict. 2015, 4, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Flament, M.F.; Hill, E.M.; Buchholz, A.; Henderson, K.; Tasca, G.A.; Goldfield, G. Internalization of the thin and muscular body ideal and disordered eating in adolescence: The mediation effects of body esteem. Body Image 2012, 9, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Schoenenberg, K.; Engelkamp, J.E.; Staufenbiel, T.; Martin, A.; Ebert, D.D.; Hartmann, A.S. Efficacy of an internet-based, therapist-guided cognitive behavioral therapy intervention for adolescents and young adults with body dysmorphic disorder: A randomized controlled trial. BMC Psychiatry 2025, 25, 374. [Google Scholar] [CrossRef] [PubMed]
- Ganson, K.T.; Testa, A.; Rodgers, R.F.; Nagata, J.M. Associations between muscularity-oriented social media content and muscle dysmorphia among boys and men. Body Image 2025, 53, 101903. [Google Scholar] [CrossRef] [PubMed]
- de Tena, A.R.; Badenes-Ribera, L. Body dissatisfaction, muscle dysmorphia, eating disorder and self-esteem in Spanish men of different sexual orientations. Curr. Psychol. 2025, 1–15. [Google Scholar] [CrossRef]
- Dal Lago, D.; Ottoboni, G.; Marzocchi, M.; Tessari, A. Perceiving the body differently: Cognitive processing and muscle dysmorphia tendencies. In Perceiving the Body Differently: Cognitive Processing and Muscle Dysmorphia Tendencies; Springer: Cham, Switzerland, 2025. [Google Scholar]
- Greenberg, J.L.; Jacobson, N.C.; Hoeppner, S.S.; Bernstein, E.E.; Snorrason, I.; Schwartzberg, A.; Wilhelm, S. Early response to cognitive behavioral therapy for body dysmorphic disorder as a predictor of outcomes. J. Psychiatr. Res. 2022, 152, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Snorrason, I.; Hoeppner, S.S.; Klare, D.; Weingarden, H.; Greenberg, J.L.; Berger-Gutierrez, R.M.; Wilhelm, S. Long-term outcomes of smartphone-delivered cognitive behavior therapy for body dysmorphic disorder: A one-year naturalistic follow-up. Internet Interv. 2025, 39, 100803. [Google Scholar] [CrossRef] [PubMed]
- Altun, Y.; Özen, M.; Kuloğlu, M.M. Psikolojik Sıkıntı Ölçeğinin Türkçe uyarlaması: Geçerlilik ve güvenilirlik çalışması. Anadolu Psikiyatr. Derg. 2019, 20, 23–31. (In Turkish) [Google Scholar]
- Pope, C.G.; Pope, H.G.; Menard, W.; Fay, C.; Olivardia, R.; Phillips, K.A. Clinical features of muscle dysmorphia among males with body dysmorphic disorder. Body Image 2005, 2, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Piacentino, D.; Kotzalidis, G.D.; Del Casale, A.; Aromatario, M.R.; Pomara, C.; Girardi, P.; Sani, G. Anabolic-androgenic steroid use and psychopathology in athletes: A systematic review. Curr. Neuropharmacol. 2015, 13, 101–121. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.; O’Connor, K.; Aardema, F.; Bélanger, C.; Courchesne, C. The role of emotion regulation in body-focused repetitive behaviours. Cogn. Behav. Ther. 2016, 9, e7. [Google Scholar] [CrossRef]
- Hildebrandt, T.; Langenbucher, J.; Schlundt, D.G. Muscularity concerns among men: Development of attitudinal and perceptual measures. Body Image 2004, 1, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Devrim, A.; Bilgic, P. Validity and reliability study of Turkish version of “Muscle Dysmorphic Disorder Inventory” and “Bodybuilder Image Grid” scales. Curr. Nutr. Food Sci. 2019, 15, 517–524. [Google Scholar] [CrossRef]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E. Kessler Psychological Distress Scale (K10); Harvard Medical School: Boston, MA, USA, 1996. [Google Scholar]
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a measure of current depression in the general population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Güleç, M.Y.; Güleç, H.; Şimşek, G.; Turhan, M.; Sünbül, E.A. Psychometric properties of the Turkish version of the Patient Health Questionnaire–Somatic, Anxiety, and Depressive Symptoms. Compr. Psychiatry 2012, 53, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Fairburn, C.G.; Beglin, S.J. Eating disorder examination questionnaire. Cogn. Behav. Ther. Eat. Disord. 2008, 309, 509–528. [Google Scholar]
- Yucel, B.; Polat, A.; Ikiz, T.; Dusgor, B.P.; Yavuz, A.E.; Berk, O.S. The Turkish version of the Eating Disorder Examination Questionnaire: Reliability and validity in adolescents. Eur. Eat. Disord. Rev. 2011, 19, 509–511. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, M.D.; Szabo, A.; Terry, A. The exercise addiction inventory: A quick and easy screening tool for health practitioners. Br. J. Sports Med. 2005, 39, e30. [Google Scholar] [CrossRef] [PubMed]
- Aydın, D.; Baltacı, U.B.; Erzen, E.; Szabo, A.; Griffiths, M.D. The Turkish version of the Exercise Addiction Inventory: Validity and reliability. Addicta Turk. J. Addict. 2023, 10, 184–193. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | CBT Group (n = 30) | Control Group (n = 29) | p-Value |
|---|---|---|---|
| Age, mean (SD) | 27.8 (6.2) | 28.5 (5.9) | 0.618 |
| Education, years, mean (SD) | 14.1 (2.4) | 14.5 (2.7) | 0.522 |
| MDDI Total, mean (SD) | 42.3 (6.8) | 41.7 (7.1) | 0.701 |
| PHQ-9 Total, mean (SD) | 11.6 (4.5) | 12.1 (4.2) | 0.645 |
| K10 Total, mean (SD) | 28.4 (6.2) | 29.0 (5.7) | 0.698 |
| BIG Ideal–Current Discrepancy | 2.4 (1.1) | 2.5 (1.0) | 0.738 |
| EDE-Q Global, mean (SD) | 3.1 (1.0) | 3.0 (1.2) | 0.814 |
| EAI Total, mean (SD) | 20.7 (3.5) | 21.0 (3.7) | 0.752 |
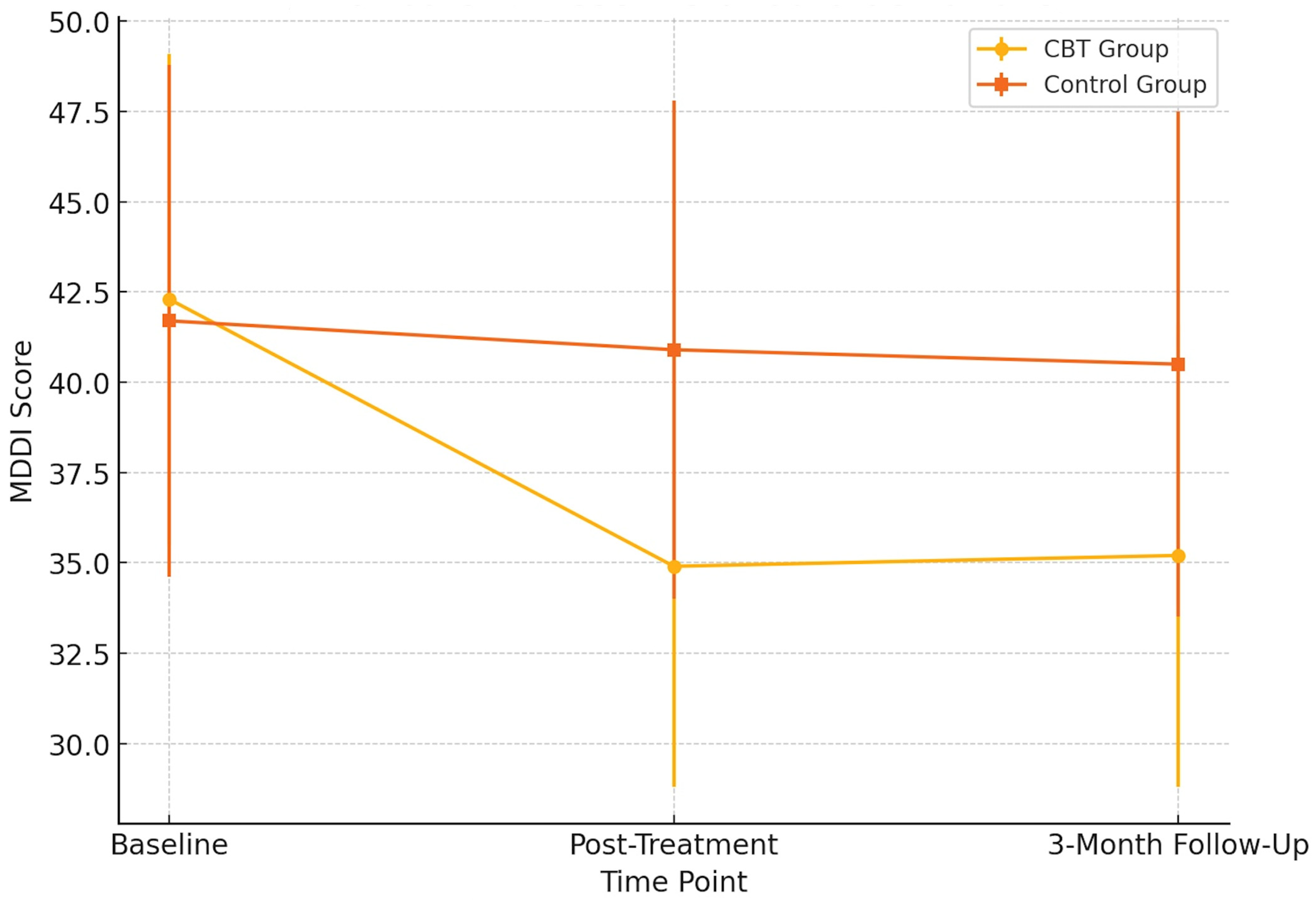
| Time Point | CBT Group (n = 30) Mean (SD) | Control Group (n = 29) Mean (SD) | F (1, 57) | p-Value | η2 Partial |
|---|---|---|---|---|---|
| Baseline | 42.3 (6.8) | 41.7 (7.1) | |||
| Post-Treatment | 34.9 (6.1) | 40.9 (6.9) | 15.72 | <0.001 | 0.216 |
| 3-Month Follow-Up | 35.2 (6.4) | 40.5 (7.0) | 13.94 | 0.001 | 0.197 |
| Measure | Group | T1 Mean (SD) | T2 Mean (SD) | T3 Mean (SD) |
|---|---|---|---|---|
| PHQ-9 | CBT (n = 30) | 14.1 (4.2) | 8.3 (3.7) | 7.1 (3.9) |
| Control (n = 29) | 13.8 (4.5) | 13.2 (4.6) | 12.6 (4.3) | |
| K10 | CBT | 28.4 (6.5) | 21.1 (5.8) | 18.7 (5.2) |
| Control | 27.9 (6.3) | 27.4 (6.0) | 26.9 (5.8) | |
| EDE-Q (Global Score) | CBT | 3.42 (0.88) | 2.26 (0.93) | 1.91 (0.95) |
| Control | 3.38 (0.85) | 3.31 (0.87) | 3.24 (0.90) | |
| EAI | CBT | 23.2 (3.9) | 18.1 (4.2) | 16.4 (4.6) |
| Control | 22.9 (4.1) | 22.3 (4.3) | 21.7 (4.0) | |
| BIG Discrepancy Score | CBT | 4.1 (1.3) | 2.4 (1.1) | 1.9 (1.2) |
| Control | 4.0 (1.4) | 3.8 (1.3) | 3.6 (1.2) |
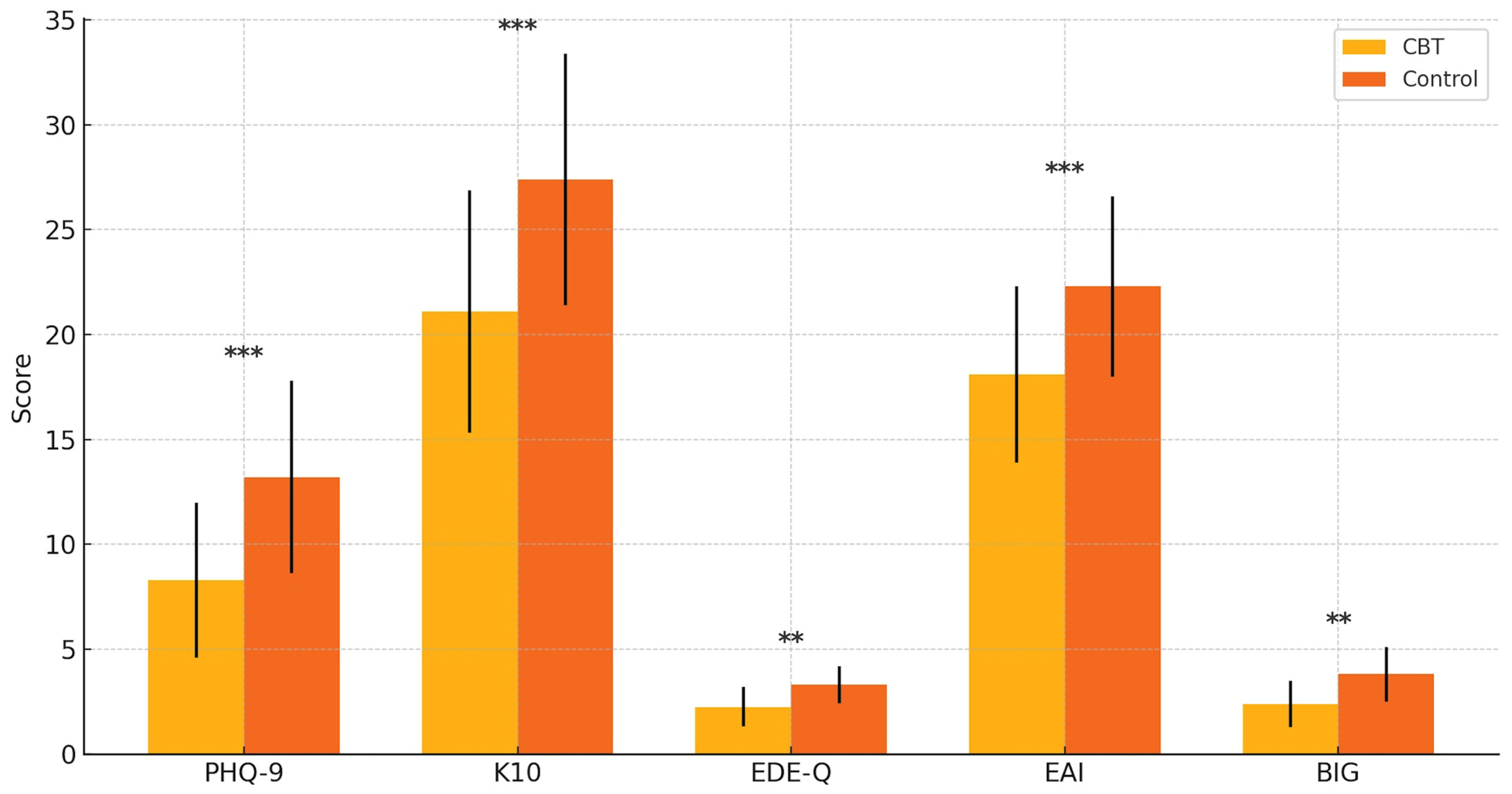
| Outcome Measure | F (Group × Time) | p-Value | Partial η2 | Interpretation |
|---|---|---|---|---|
| MDDI (Total) | 22.17 | <0.001 | 0.28 | Large effect |
| PHQ-9 | 16.35 | <0.001 | 0.23 | Large effect |
| K10 | 14.02 | <0.001 | 0.21 | Large effect |
| EDE-Q (Global) | 10.94 | 0.001 | 0.18 | Medium effect |
| EAI | 12.63 | <0.001 | 0.20 | Large effect |
| BIG Discrepancy | 9.01 | 0.004 | 0.16 | Medium effect |
| Measure | Pre-Treatment Mean (SD) | Post-Treatment Mean (SD) | t (df) | p-Value | Cohen’s d |
|---|---|---|---|---|---|
| BIG | 17.6 (2.5) | 15.8 (2.4) | 4.32 (29) | <0.001 | 0.79 |
| K10 | 29.2 (4.3) | 24.6 (3.9) | 5.10 (29) | <0.001 | 0.93 |
| PHQ-9 | 14.5 (3.8) | 10.8 (3.5) | 5.36 (29) | <0.001 | 0.98 |
| EDE-Q | 3.2 (0.7) | 2.6 (0.6) | 4.05 (29) | <0.001 | 0.74 |
| EAI | 23.4 (3.1) | 19.9 (2.8) | 5.88 (29) | <0.001 | 1.07 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Çınaroğlu, M.; Yılmazer, E.; Ülker, S.V.; Hızlı Sayar, G. Cognitive Behavioral Therapy for Muscle Dysmorphia and Anabolic Steroid-Related Psychopathology: A Randomized Controlled Trial. Pharmaceuticals 2025, 18, 1081. https://doi.org/10.3390/ph18081081
Çınaroğlu M, Yılmazer E, Ülker SV, Hızlı Sayar G. Cognitive Behavioral Therapy for Muscle Dysmorphia and Anabolic Steroid-Related Psychopathology: A Randomized Controlled Trial. Pharmaceuticals. 2025; 18(8):1081. https://doi.org/10.3390/ph18081081
Chicago/Turabian StyleÇınaroğlu, Metin, Eda Yılmazer, Selami Varol Ülker, and Gökben Hızlı Sayar. 2025. "Cognitive Behavioral Therapy for Muscle Dysmorphia and Anabolic Steroid-Related Psychopathology: A Randomized Controlled Trial" Pharmaceuticals 18, no. 8: 1081. https://doi.org/10.3390/ph18081081
APA StyleÇınaroğlu, M., Yılmazer, E., Ülker, S. V., & Hızlı Sayar, G. (2025). Cognitive Behavioral Therapy for Muscle Dysmorphia and Anabolic Steroid-Related Psychopathology: A Randomized Controlled Trial. Pharmaceuticals, 18(8), 1081. https://doi.org/10.3390/ph18081081