
Revolutionizing Prostate Cancer Detection: The Role of Approved PSMA-PET Imaging Agents




Abstract

1. Introduction
2. Chemical Overview
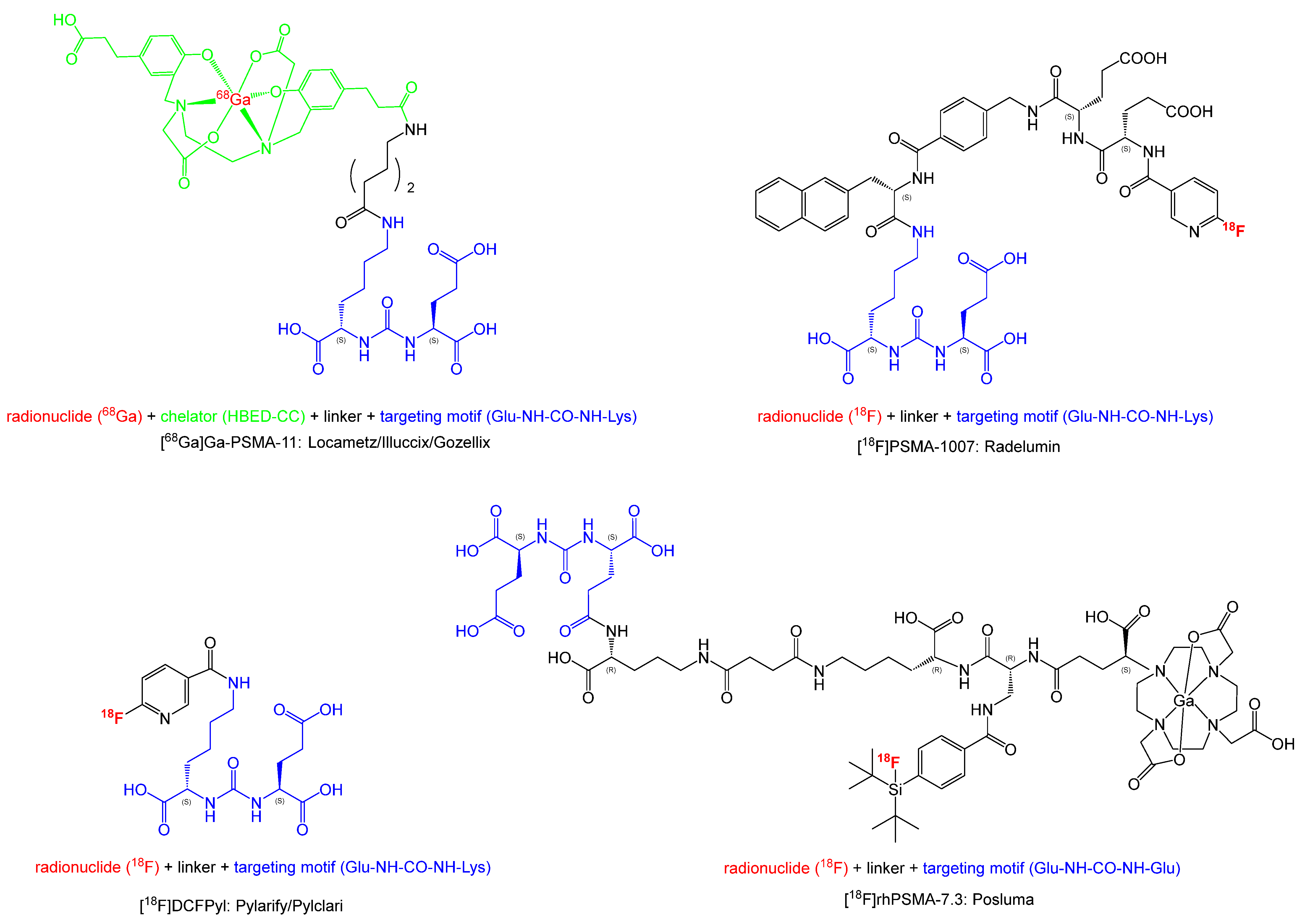
2.1. Names, Chemical Structures and Properties
- [18F]PSMA-1007: (3S,10S,14S)-1-[4-[[(2S)-4-carboxy-2-[(2S)-4-carboxy-2-(6-[18F]fluoropyridin-3-amido)butanamido]butanamido]methyl]phenyl]-3-[(naphthalen-2-yl)methyl]-1,4,12-trioxo-2,5,11,13-tetraazahexadecane-10,14,16-tricarboxylic acid
- [68Ga]Ga-PSMA-11: [68Ga]gallium (3S,7S)-22-[3-[[[2-[[[5-(2-carboxyethyl)-2-hydroxyphenyl]-methyl](carboxymethyl)amino]ethyl](carboxymethyl)amino]-methyl]-4-hydroxyphenyl]-5,13,20-trioxo-4,6,12,19-tetraazadocosane-1,3,7-tricarboxylic acid
- [18F]DCFPyL: 2-(3-{1-carboxy-5-[(6-[18F]fluoro-pyridine-3-carbonyl)amino]-pentyl} [18]ureido)-pentanedioic acid
- [18F]rhPSMA-7.3: gallate(6-), [(4S,8S,13R,27R,30R,35S)-35-[4,10-bis[(carboxy-kO)me-thyl]-7-(carboxymethyl)-1,4,7,10-tetraazacyclododec-1-yl-kN1,kN4,kN7,kN10]-30-[[[4-[bis(1,1dimethylethyl)fluoro-18F-silyl]benzoyl]amino]methyl]-1,36-dihydroxy-1,6,11,18,21,29,32,36-octaoxo-5,7,12,17,22,28,31-heptaazahexatriacontane-4,8,13,27-tetracarboxylato(9-)]-, hydrogen (1:6)
2.2. Radionuclides
2.3. GMP-Compliant Synthesis
2.4. End-Product Specifications and Quality Control
3. Medicinal and Pharmaceutical Overview
3.1. Clinical Indication
- (i)
- Primary staging of patients with high-risk PCa before curative initial treatment
- (ii)
- The detection of suspected PCa recurrence in patients with rising PSA levels after a curative initial treatment (e.g., radical prostatectomy–RP, external beam radiation therapy–EBRT).
3.2. Application
3.3. Pharmacology, Pharmacokinetics and Toxicology
3.4. Comparative Studies

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Imaging Agent | Clinical Trial | Phase | Publication Year | Number of Patients | Type of Patient | Main Findings | Ref. |
|---|---|---|---|---|---|---|---|
| Posluma®: [18F]rhPSMA-7.3 | NCT03995888 | 1 | 2021 | 6 | Healthy volunteers | No clinically detectable pharmacological effects were observed after injection of 220 MBq. The mean effective dose received by the patients was 0.0141 mSv/MBq which is favorable for diagnostics by PET and lower than for other PET PSMA agents. | [80] |
| LIGHTHOUSE NCT04186819 | 3 | 2021 | 335 | High risk PCa | Confirmation of the safety and accuracy of detection of lesions in high risk PCa in patients with a large range of PSA levels. Confirmation of the safety and accuracy of detection of lesions in recurrent PCa in patients with a large range of PSA levels. | [81] | |
| SPOTLIGHT NCT04186845 | 3 | 2021 | 389 | Recurrent PCa | [100] [101] | ||
| Radelumin®: [18F]PSMA-1007 | 1/2 | 2017 | 3 10 | Healthy volunteers PCa patients | Comparable performance of [18F]PSMA-1007 and [68Ga]Ga-PSMA-11. | [102] | |
| 1/2 | 2023 | 3 13 | Healthy volunteers PCa patients | Safe and well tolerated tracer, high accuracy in the diagnoses for primary and metastatic lesions. | [103] | ||
| 2 | 2019 | 40 | After RP or radiation beam therapy | Scan positivity is dependent on PSA level. Moderate detection of tumor lesion (60%) at low PSA levels < 0.2 ng/mL. | [90] | ||
| 3 | 2021 | 175 | PCa | Detection efficiency of 80%. | [104] | ||
| Locametz®/ Illuccix®/GozellixTM: [68Ga]Ga-PSMA-11 | NCT03001869 | 2023 | Completed–No results posted. | ||||
| NCT02659527 | 3 | 2018 | 145 | BCR PCa patients after RP | Detection efficiency of 85%. | [105] | |
| NCT03353740 and NCT02940262 | 3 | 2020 | 635 | BCR PCa patients after RP and/or radiation therapy | High detection rates of 75% and positive prediction values between 84 and 92%. | [87] | |
| 3 | 2017 | 1007 | Recurrent PCa | No adverse clinical side effects observed. Same conclusions, significantly higher detection of lesions compared to other already approved tracers, detection rate increases as the PSA level increases. | [106] | ||
| NCT03582774 PSMA-SRT | 3 | 2025 | 193 | Recurrent PCa after RP | Actively recruiting for [68Ga]Ga-PSMA-11 PET/CT for PCa salvage radiotherapy planning. | [107] | |
| 2015 | 70 | Restaging PCa | Good detection rate even at low PSA level (85%). | [108] | |||
| 2015 | 248 | BCR PCa patients after RP | PSA level ≥ 0.2 ng/mL. [68Ga]Ga-PSMA-11 surpasses other imaging modalities for restaging PCa detection and higher detection efficacy compared to other tracers. 89.5% of detection when PSA level ≥ 1.0 ng/mL. | [88] | |||
| BCR PCa patients after RP | [68Ga]Ga-PSMA-11 surpasses other imaging modalities for restaging PCa detection and higher detection efficacy compared to other tracers as concluded by Eiber et al. [88]. | [109] | |||||
| Pylarify®/Pylclari®: [18F]DCFPyL | NCT02523924 | 2 | 2020 | 31 | RP BCa patients | Prospective study, proved good detection of lesions even at low PSA level. | [110] |
| 2 | 2018 | 248 | BCR PCa patients | Early detection even at low PSA level (<0.5 ng/mL). Results comparable to those of [68Ga]Ga-PSMA-11 and [18F]PSMA-1007. | [111] | ||
| NCT03181867 | 2 | 2019 | 800 | BCR patients | 90% detection rate for PSA level > 0.5 ng/mL. | [112] | |
| NCT02899312 | 3 | 2019 | 2244 | BCR after RP | This study confirmed the safety of use and the good sensitivity of this tracer for small lesion detection | [113] | |
| OSPREY NCT02981368 | 2/3 | 2021 | 385 | high risk and recurrent/metastatic PCa. | High positive prediction values (78.1–90.5%). | [84] | |
| CONDOR NCT03739684 | 3 | 2021 | 208 | BCR PCa after RP of radiotherapy | Confirmation of the accuracy of recurrence or metastases lesion detection from previous clinical trials, study even with patients with low PSA levels. [18F]DCFPyL has similar safety and performance compared to [68Ga]Ga-PSMA-11. | [89] | |
| NCT03232164 | 3 | 2024 | 167 | Pilot studies for PET/CT and PET/MRI. No results posted. |
| Imaging Agent | Clinical Trials | Phase | Year | Number of Patients | Type of Patient | Main Findings | Ref. |
|---|---|---|---|---|---|---|---|
| [68Ga]Ga-PSMA-11 and [18F]fluorocholine | 2016 | 32 | BCR PCa patient after RP | 43% of patients with a negative [18F]fluorocholine PET/CT scan have been diagnosed with PCa lesions using [68Ga]Ga-PSMA-11 PET/CT and confirmed with other diagnosis techniques. [68Ga]Ga-PSMA-11 outperformed [18F]fluorocholine. | [91] | ||
| [18F]PSMA-1007 and [18F]fluorocholine | NCT04102553 | 3 | 2022 | 190 | BCR PCa patients | Significantly higher detection rate for [18F]PSMA-1007 than [18F]fluorocholine especially at low PSA levels. | [114] |
| NCT04742361 | 3 | 2024 | Actively recruiting. | ||||
| [18F]PSMA-1007 and [18F]FDG | 2024 | 42 | RP PCa | [18F]PSMA-1007 outperformed the detection of primary tumors in the prostate glands. | [115] | ||
| 2021 | 21 | Significantly more tumor lesion and benign lesion uptake for [18F]PSMA-1007. | [116] | ||||
| [68Ga]Ga-PSMA-11 and [18F]fluciclovine | NCT03515577 | 2020 | 50 | BCR PCa | Detection rate in patients with low PSA level (≤2.0 ng/mL) is significantly lower for [18F]fluciclovine than [68Ga]Ga-PSMA-11 and up to twice lower for lesions in the pelvic lymph nodes region. | [117] | |
| [18F]PSMA-1007 and [18F]fluciclovine | NCT04239742 | 2 | 2020 | 50 | PCa | [18F]PSMA-1007 outperformed [18F]fluciclovine to detect lesions (68% vs 42%). | [118] |
| [18F]PSMA-1007 and [68Ga]Ga-PSMA-11 | NCT05079828 | 3 | 2024 | 100 | BCR PCa patient after RP | No results posted. | [119] |
| [18F]PSMA-1007 and [18F]DCFPyL | 2018 | 12 | Drug-naive or before surgery PCa patients | Equivalence of efficacy for both tracers. [18F]PSMA-1007 clearance pathway is an advantage for pelvic metastases detection. | [120] |
4. Further Candidates and Outlook
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- James, N.D.; Tannock, I.; N’Dow, J.; Feng, F.; Gillessen, S.; Ali, S.A.; Trujillo, B.; Al-Lazikani, B.; Attard, G.; Bray, F.; et al. The Lancet Commission on prostate cancer: Planning for the surge in cases. Lancet 2024, 403, 1683–1722. [Google Scholar] [CrossRef]
- Lowder, D.; Rizwan, K.; McColl, C.; Paparella, A.; Ittmann, M.; Mitsiades, N.; Kaochar, S. Racial disparities in prostate cancer: A complex interplay between socioeconomic inequities and genomics. Cancer Lett. 2022, 531, 71–82. [Google Scholar] [CrossRef]
- Rebbeck, T.R. Prostate Cancer Disparities by Race and Ethnicity: From Nucleotide to Neighborhood. Cold Spring Harb. Perspect. Med. 2018, 8, a030387. [Google Scholar] [CrossRef]
- Robinson, D.; Van Allen, E.M.; Wu, Y.M.; Schultz, N.; Lonigro, R.J.; Mosquera, J.M.; Montgomery, B.; Taplin, M.E.; Pritchard, C.C.; Attard, G.; et al. Integrative clinical genomics of advanced prostate cancer. Cell 2015, 161, 1215–1228. [Google Scholar] [CrossRef] [PubMed]
- Armenia, J.; Wankowicz, S.A.M.; Liu, D.; Gao, J.; Kundra, R.; Reznik, E.; Chatila, W.K.; Chakravarty, D.; Han, G.C.; Coleman, I.; et al. The long tail of oncogenic drivers in prostate cancer. Nat. Genet. 2018, 50, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Descotes, J.L. Diagnosis of prostate cancer. Asian J. Urol. 2019, 6, 129–136. [Google Scholar] [CrossRef]
- Okotie, O.T.; Roehl, K.A.; Han, M.; Loeb, S.; Gashti, S.N.; Catalona, W.J. Characteristics of prostate cancer detected by digital rectal examination only. Urology 2007, 70, 1117–1120. [Google Scholar] [CrossRef]
- Morote, J.; Paesano, N.; Picola, N.; Munoz-Rodriguez, J.; Ruiz-Plazas, X.; Munoz-Rivero, M.V.; Celma, A.; Garcia-de Manuel, G.; Miro, B.; Abascal, J.M.; et al. The Role of Digital Rectal Examination for Early Detection of Significant Prostate Cancer in the Era of Magnetic Resonance Imaging. Life 2024, 14, 1359. [Google Scholar] [CrossRef]
- Gosselaar, C.; Kranse, R.; Roobol, M.J.; Roemeling, S.; Schroder, F.H. The interobserver variability of digital rectal examination in a large randomized trial for the screening of prostate cancer. Prostate 2008, 68, 985–993. [Google Scholar] [CrossRef]
- Lilja, H.; Ulmert, D.; Vickers, A.J. Prostate-specific antigen and prostate cancer: Prediction, detection and monitoring. Nat. Rev. Cancer 2008, 8, 268–278. [Google Scholar] [CrossRef]
- Benelli, A.; Vaccaro, C.; Guzzo, S.; Nedbal, C.; Varca, V.; Gregori, A. The role of MRI/TRUS fusion biopsy in the diagnosis of clinically significant prostate cancer. Ther. Adv. Urol. 2020, 12, 1756287220916613. [Google Scholar] [CrossRef]
- Borofsky, S.; George, A.K.; Gaur, S.; Bernardo, M.; Greer, M.D.; Mertan, F.V.; Taffel, M.; Moreno, V.; Merino, M.J.; Wood, B.J.; et al. What Are We Missing? False-Negative Cancers at Multiparametric MR Imaging of the Prostate. Radiology 2018, 286, 186–195. [Google Scholar] [CrossRef]
- Chow, K.M.; So, W.Z.; Lee, H.J.; Lee, A.; Yap, D.W.T.; Takwoingi, Y.; Tay, K.J.; Tuan, J.; Thang, S.P.; Lam, W.; et al. Head-to-head Comparison of the Diagnostic Accuracy of Prostate-specific Membrane Antigen Positron Emission Tomography and Conventional Imaging Modalities for Initial Staging of Intermediate- to High-risk Prostate Cancer: A Systematic Review and Meta-analysis. Eur. Urol. 2023, 84, 36–48. [Google Scholar] [CrossRef]
- Islam, R.; Desai, S.; Moran, M.; Golombos, D.M. The Role of PSMA PET Imaging in Prostate Cancer: Current Applications and Future Directions. Curr. Urol. Rep. 2025, 26, 46. [Google Scholar] [CrossRef]
- Horoszewicz, J.S.; Leong, S.S.; Kawinski, E.; Karr, J.P.; Rosenthal, H.; Chu, T.M.; Mirand, E.A.; Murphy, G.P. LNCaP model of human prostatic carcinoma. Cancer Res. 1983, 43, 1809–1818. [Google Scholar]
- Evans, J.C.; Malhotra, M.; Cryan, J.F.; O’Driscoll, C.M. The therapeutic and diagnostic potential of the prostate specific membrane antigen/glutamate carboxypeptidase II (PSMA/GCPII) in cancer and neurological disease. Br. J. Pharmacol. 2016, 173, 3041–3079. [Google Scholar] [CrossRef]
- Kinoshita, Y.; Kuratsukuri, K.; Landas, S.; Imaida, K.; Rovito, P.M., Jr.; Wang, C.Y.; Haas, G.P. Expression of prostate-specific membrane antigen in normal and malignant human tissues. World J. Surg. 2006, 30, 628–636. [Google Scholar] [CrossRef]
- Chang, S.S.; O’Keefe, D.S.; Bacich, D.J.; Reuter, V.E.; Heston, W.D.; Gaudin, P.B. Prostate-specific membrane antigen is produced in tumor-associated neovasculature. Clin. Cancer Res. 1999, 5, 2674–2681. [Google Scholar]
- Wurzer, A.; Di Carlo, D.; Schmidt, A.; Beck, R.; Eiber, M.; Schwaiger, M.; Wester, H.J. Radiohybrid Ligands: A Novel Tracer Concept Exemplified by 18F- or 68Ga-Labeled rhPSMA Inhibitors. J. Nucl. Med. 2020, 61, 735–742. [Google Scholar] [CrossRef]
- Schuhmacher, J.; Klivenyi, G.; Hull, W.E.; Matys, R.; Hauser, H.; Kalthoff, H.; Schmiegel, W.H.; Maier-Borst, W.; Matzku, S. A bifunctional HBED-derivative for labeling of antibodies with 67Ga, 111In and 59Fe. Comparative biodistribution with 111In-DPTA and 131I-labeled antibodies in mice bearing antibody internalizing and non-internalizing tumors. Int. J. Rad. Appl. Instrum. B 1992, 19, 809–824. [Google Scholar] [CrossRef]
- Eder, M.; Neels, O.; Muller, M.; Bauder-Wust, U.; Remde, Y.; Schafer, M.; Hennrich, U.; Eisenhut, M.; Afshar-Oromieh, A.; Haberkorn, U.; et al. Novel Preclinical and Radiopharmaceutical Aspects of [68Ga]Ga-PSMA-HBED-CC: A New PET Tracer for Imaging of Prostate Cancer. Pharmaceuticals 2014, 7, 779–796. [Google Scholar] [CrossRef]
- Cardinale, J.; Martin, R.; Remde, Y.; Schafer, M.; Hienzsch, A.; Hubner, S.; Zerges, A.M.; Marx, H.; Hesse, R.; Weber, K.; et al. Procedures for the GMP-Compliant Production and Quality Control of [18F]PSMA-1007: A Next Generation Radiofluorinated Tracer for the Detection of Prostate Cancer. Pharmaceuticals 2017, 10, 77. [Google Scholar] [CrossRef]
- Dornan, M.H.; Simard, J.M.; Leblond, A.; Juneau, D.; Delouya, G.; Saad, F.; Menard, C.; DaSilva, J.N. Simplified and robust one-step radiosynthesis of [18F]DCFPyL via direct radiofluorination and cartridge-based purification. J. Label. Comp. Radiopharm. 2018, 61, 757–763. [Google Scholar] [CrossRef]
- Gower-Fry, L.; Kronemann, T.; Dorian, A.; Pu, Y.; Jaworski, C.; Wangler, C.; Bartenstein, P.; Beyer, L.; Lindner, S.; Jurkschat, K.; et al. Recent Advances in the Clinical Translation of Silicon Fluoride Acceptor (SiFA) 18F-Radiopharmaceuticals. Pharmaceuticals 2021, 14, 701. [Google Scholar] [CrossRef]
- Wurzer, A.; Parzinger, M.; Konrad, M.; Beck, R.; Gunther, T.; Felber, V.; Farber, S.; Di Carlo, D.; Wester, H.J. Preclinical comparison of four [18F,(nat)Ga]rhPSMA-7 isomers: Influence of the stereoconfiguration on pharmacokinetics. EJNMMI Res. 2020, 10, 149. [Google Scholar] [CrossRef]
- Sanchez-Crespo, A. Comparison of Gallium-68 and Fluorine-18 imaging characteristics in positron emission tomography. Appl. Radiat. Isot. 2013, 76, 55–62. [Google Scholar] [CrossRef]
- Ashhar, Z.; Ahmad Fadzil, M.F.; Othman, M.F.; Yusof, N.A.; Abdul Onny, M.A.; Mat Ail, N.; Abd Rahman, S.F. Cyclotron Production of Gallium-68 Radiopharmaceuticals Using the 68Zn(p,n)68Ga Reaction and Their Regulatory Aspects. Pharmaceutics 2022, 15, 70. [Google Scholar] [CrossRef]
- EDQM. European Pharmacopeia Monograph. In “Gallium (68Ga) Chloride (Accelerator-Produced) Solution for Radiolabelling” (01/2021:3109), 11th ed.; EDQM—European Directorate for the Quality of Medicines & HealthCare: Strasbourg, France, 2023. [Google Scholar]
- IAEA TECDOC “Production and Quality Control of Fluorine-18 Labelled Radiopharmaceuticals”. Available online: https://www.iaea.org/publications/14925/production-and-quality-control-of-fluorine-18-labelled-radiopharmaceuticals (accessed on 25 April 2025).
- Scott, P.J.; Hockley, B.G.; Kung, H.F.; Manchanda, R.; Zhang, W.; Kilbourn, M.R. Studies into radiolytic decomposition of fluorine-18 labeled radiopharmaceuticals for positron emission tomography. Appl. Radiat. Isot. 2009, 67, 88–94. [Google Scholar] [CrossRef]
- Schmitt, S.; Moreau, E. Radiochemistry with {Al18F}2+: Current status and optimization perspectives for efficient radiofluorination by complexation. Coordin. Chem. Rev. 2023, 480, 215028. [Google Scholar] [CrossRef]
- Patt, M.; Decristoforo, C.; de Martini, A.; Koole, M.; Oyen, W.J.G.; Kiss, O.C. The revision of the pharmaceutical legislation—It is time to act for nuclear medicine in Europe. Eur. J. Nucl. Med. Mol. Imaging 2023, 51, 20–24. [Google Scholar] [CrossRef]
- Ravert, H.T.; Holt, D.P.; Chen, Y.; Mease, R.C.; Fan, H.; Pomper, M.G.; Dannals, R.F. An improved synthesis of the radiolabeled prostate-specific membrane antigen inhibitor, [18F]DCFPyL. J. Label. Comp. Radiopharm. 2016, 59, 439–450. [Google Scholar] [CrossRef] [PubMed]
- Hoareau, R.; Bach-Gansmo, T.; Cumming, P.; Olberg, D.E. A new automated and putatively versatile synthesis of the PSMA-ligand derivative [18F]DCFPyL using the FASTlab(TM) synthesizer. EJNMMI Radiopharm. Chem. 2022, 7, 10. [Google Scholar] [CrossRef] [PubMed]
- Bouvet, V.; Wuest, M.; Jans, H.S.; Janzen, N.; Genady, A.R.; Valliant, J.F.; Benard, F.; Wuest, F. Automated synthesis of [18F]DCFPyL via direct radiofluorination and validation in preclinical prostate cancer models. EJNMMI Res. 2016, 6, 40. [Google Scholar] [CrossRef] [PubMed]
- Shamni, O.; Nebeling, B.; Grievink, H.; Mishani, E. Fine-tuning of the automated [18F]PSMA-1007 radiosynthesis. J. Label. Comp. Radiopharm. 2019, 62, 252–258. [Google Scholar] [CrossRef]
- Maisto, C.; Morisco, A.; de Marino, R.; Squame, E.; Porfidia, V.; D’Ambrosio, L.; Di Martino, D.; Gaballo, P.; Aurilio, M.; Buonanno, M.; et al. On site production of [18F]PSMA-1007 using different [18F]fluoride activities: Practical, technical and economical impact. EJNMMI Radiopharm. Chem. 2021, 6, 36. [Google Scholar] [CrossRef]
- Naka, S.; Watabe, T.; Kurimoto, K.; Uemura, M.; Soeda, F.; Neels, O.C.; Kopka, K.; Tatsumi, M.; Kato, H.; Nonomura, N.; et al. Automated [18F] PSMA-1007 production by a single use cassette-type synthesizer for clinical examination. EJNMMI Radiopharm. Chem. 2020, 5, 18. [Google Scholar] [CrossRef]
- Wurzer, A.; Di Carlo, D.; Herz, M.; Richter, A.; Robu, S.; Schirrmacher, R.; Mascarin, A.; Weber, W.; Eiber, M.; Schwaiger, M.; et al. Automated synthesis of [18F]Ga-rhPSMA-7/ -7.3: Results, quality control and experience from more than 200 routine productions. EJNMMI Radiopharm. Chem. 2021, 6, 4. [Google Scholar] [CrossRef]
- Blok, S.; Wängler, C.; Bartenstein, P.; Jurkschat, K.; Schirrmacher, R.; Lindner, S. Good practices for the automated production of 18F-SiFA radiopharmaceuticals. EJNMMI Radiopharm. Chem. 2023, 8, 25. [Google Scholar] [CrossRef]
- FDA Drug Approval Package for “POSLUMA (Flotufolastat F 18) Injection”. Available online: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=216023 (accessed on 6 May 2025).
- Prescribing Information for PYLARIFY®. Available online: https://www.pylarify.com/sites/default/files/resources/prescribing-information.pdf (accessed on 21 April 2025).
- FDA Drug Approval Package for PYLARIFY®. Available online: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=214793 (accessed on 6 May 2025).
- Fuscaldi, L.L.; Sobral, D.V.; Durante, A.C.R.; Mendonca, F.F.; Miranda, A.C.C.; da Cunha, M.L.; Malavolta, L.; Mejia, J.; de Barboza, M.F. Standardization of the [68Ga]Ga-PSMA-11 Radiolabeling Protocol in an Automatic Synthesis Module: Assessments for PET Imaging of Prostate Cancer. Pharmaceuticals 2021, 14, 385. [Google Scholar] [CrossRef]
- FDA Drug Approval Package for “ILLUCCIX® (Kit for the Preparation of Gallium Ga 68 Gozetotide Injection)”. Available online: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=214032 (accessed on 14 April 2025).
- Press Release Telix Pharmaceuticals. Available online: https://telixpharma.com/news-views/illuccix-receives-european-approval/#_ftn1 (accessed on 14 April 2025).
- FDA Drug Approval Package for “GOZELLIXTM (Kit for the Preparation of Gallium Ga 68 Gozetotide Injection)”. Available online: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=219592. (accessed on 6 May 2025).
- FDA Drug Approval Package for “LOCAMETZ® (Kit for the Preparation of Gallium Ga 68 Gozetotide Injection”. Available online: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=215841 (accessed on 14 April 2025).
- Product Information—LOCAMETZ®. Available online: https://www.ema.europa.eu/en/documents/product-information/locametz-epar-product-information_en.pdf. (accessed on 21 April 2025).
- Wang, I.E.; Morrissette, L.J.; Wong, K.K.; Brooks, A.F.; Dakanali, M.; Scott, P.J.H. A comparison of routine [68Ga]Ga-PSMA-11 preparation using Locametz and Illuccix kits. EJNMMI Radiopharm. Chem. 2024, 9, 87. [Google Scholar] [CrossRef] [PubMed]
- Distribution Sites of Pylarify in the US. Available online: https://www.pylarify.com/support/imaging-site-locator (accessed on 15 April 2025).
- Distribution Sites of Pylclari in Europe. Available online: https://www.curiumpharma.com/product/pylclari/ (accessed on 15 April 2025).
- Distribution Sites of Poslumay in the US. Available online: https://www.siemens-healthineers.com/en-us/molecular-imaging/petnet (accessed on 15 April 2025).
- Product Information—RADELUMIN®. Available online: https://abx.de/_Resources/Persistent/4/d/7/f/4d7ff1ffb656143c2db949b262ef2872fdf19c03/SmPC%20Radelumin%202000%20Germany.pdf (accessed on 21 April 2025).
- EDQM. European Pharmacopeia Monograph. In “Gallium 68 PSMA-11 Injection Solution” (04/2021:3044) and “PSMA-1007 (18F) Injection” (07/2021:3116), 11th ed.; EDQM—European Directorate for the Quality of Medicines & HealthCare: Strasbourg, France, 2023. [Google Scholar]
- Product Information—Pylclari®. Available online: https://www.ema.europa.eu/en/documents/product-information/pylclari-epar-product-information_en.pdf. (accessed on 21 April 2025).
- Freedland, S.J.; Humphreys, E.B.; Mangold, L.A.; Eisenberger, M.; Dorey, F.J.; Walsh, P.C.; Partin, A.W. Risk of prostate cancer-specific mortality following biochemical recurrence after radical prostatectomy. JAMA 2005, 294, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Kupelian, P.A.; Buchsbaum, J.C.; Elshaikh, M.; Reddy, C.A.; Zippe, C.; Klein, E.A. Factors affecting recurrence rates after prostatectomy or radiotherapy in localized prostate carcinoma patients with biopsy Gleason score 8 or above. Cancer 2002, 95, 2302–2307. [Google Scholar] [CrossRef]
- Cornford, P.; van den Bergh, R.C.N.; Briers, E.; van den Broeck, T.; Brunckhorst, O.; Darraugh, J.; Eberli, D.; Meerleer, G.d.; Santis, M.d.; Farolfi, A.; et al. EAU-EANM-ESTRO-ESUR-ISUP-SIOG Guidelines on Prostate Cancer-2024 Update. Part I: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2024, 86, 148–163. [Google Scholar] [CrossRef]
- Lowrance, W.T.; Breau, R.H.; Chou, R.; Chapin, B.F.; Crispino, T.; Dreicer, R.; Jarrard, D.F.; Kibel, A.S.; Morgan, T.M.; Morgans, A.K.; et al. Advanced Prostate Cancer: AUA/ASTRO/SUO Guideline PART I. J. Urol. 2021, 205, 14–21. [Google Scholar] [CrossRef]
- Sanda, M.G.; Cadeddu, J.A.; Kirkby, E.; Chen, R.C.; Crispino, T.; Fontanarosa, J.; Freedland, S.J.; Greene, K.; Klotz, L.H.; Makarov, D.V.; et al. Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline. Part I: Risk Stratification, Shared Decision Making, and Care Options. J. Urol. 2018, 199, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, E.M.; Srinivas, S.; Adra, N.; An, Y.; Barocas, D.; Bitting, R.; Bryce, A.; Chapin, B.; Cheng, H.H.; D’Amico, A.V.; et al. Prostate Cancer, Version 4.2023, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2023, 21, 1067–1096. [Google Scholar] [CrossRef]
- Trabulsi, E.J.; Rumble, R.B.; Jadvar, H.; Hope, T.; Pomper, M.; Turkbey, B.; Rosenkrantz, A.B.; Verma, S.; Margolis, D.J.; Froemming, A.; et al. Optimum Imaging Strategies for Advanced Prostate Cancer: ASCO Guideline. J. Clin. Oncol. 2020, 38, 1963–1996. [Google Scholar] [CrossRef]
- Virgo, K.S.; Rumble, R.B.; Wit, R.d.; Mendelson, D.S.; Smith, T.J.; Taplin, M.-E.; Wade, J.L.; Bennett, C.L.; Scher, H.I.; Nguyen, P.L.; et al. Initial Management of Noncastrate Advanced, Recurrent, or Metastatic Prostate Cancer: ASCO Guideline Update. J. Clin. Oncol. 2021, 39, 1274–1305. [Google Scholar] [CrossRef]
- Shore, N.D.; Moul, J.W.; Pienta, K.J.; Czernin, J.; King, M.T.; Freedland, S.J. Biochemical recurrence in patients with prostate cancer after primary definitive therapy: Treatment based on risk stratification. Prostate Cancer Prostatic Dis. 2024, 27, 192–201. [Google Scholar] [CrossRef]
- Tourinho-Barbosa, R.; Srougi, V.; Nunes-Silva, I.; Baghdadi, M.; Rembeyo, G.; Eiffel, S.S.; Barret, E.; Rozet, F.; Galiano, M.; Cathelineau, X.; et al. Biochemical recurrence after radical prostatectomy: What does it mean? Int. Braz. J. Urol. 2018, 44, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Jin, W.; Wang, R.; Zhao, R.; Zhu, L.; Kung, H.F. 68Ga/177Lu-Labeled Bivalent Agents for Targeting Hypoxia and PSMA-Binding in Prostate Cancer. J. Med. Chem. 2024, 67, 13491–13506. [Google Scholar] [CrossRef] [PubMed]
- Pillai, M.R.A.; Nanabala, R.; Joy, A.; Sasikumar, A.; Russ Knapp, F.F. Radiolabeled enzyme inhibitors and binding agents targeting PSMA: Effective theranostic tools for imaging and therapy of prostate cancer. Nucl. Med. Biol. 2016, 43, 692–720. [Google Scholar] [CrossRef]
- Davis, M.I.; Bennett, M.J.; Thomas, L.M.; Bjorkman, P.J. Crystal structure of prostate-specific membrane antigen, a tumor marker and peptidase. Proc. Natl. Acad. Sci. USA 2005, 102, 5981–5986. [Google Scholar] [CrossRef] [PubMed]
- Berger, I.; Annabattula, C.; Lewis, J.; Shetty, D.V.; Kam, J.; Maclean, F.; Arianayagam, M.; Canagasingham, B.; Ferguson, R.; Khadra, M.; et al. 68Ga-PSMA PET/CT vs. mpMRI for locoregional prostate cancer staging: Correlation with final histopathology. Prostate Cancer Prostatic Dis. 2018, 21, 204–211. [Google Scholar] [CrossRef]
- Bouchelouche, K.; Choyke, P.L. Advances in prostate-specific membrane antigen PET of prostate cancer. Curr. Opin. Oncol. 2018, 30, 189–196. [Google Scholar] [CrossRef]
- Corfield, J.; Perera, M.; Bolton, D.; Lawrentschuk, N. 68Ga-prostate specific membrane antigen (PSMA) positron emission tomography (PET) for primary staging of high-risk prostate cancer: A systematic review. World J. Urol. 2018, 36, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Cuccurullo, V.; Di Stasio, G.D.; Mansi, L. Nuclear Medicine in Prostate Cancer: A New Era for Radiotracers. World J. Nucl. Med. 2018, 17, 70–78. [Google Scholar] [CrossRef]
- Li, R.; Ravizzini, G.C.; Gorin, M.A.; Maurer, T.; Eiber, M.; Cooperberg, M.R.; Alemozzaffar, M.; Tollefson, M.K.; Delacroix, S.E.; Chapin, B.F. The use of PET/CT in prostate cancer. Prostate Cancer Prostatic Dis. 2018, 21, 4–21. [Google Scholar] [CrossRef]
- Allach, Y.; Banda, A.; van Gemert, W.; Groot, M.d.; Derks, Y.; Schilham, M.; Hoepping, A.; Perk, L.; Gotthardt, M.; Janssen, M.; et al. An Explorative Study of the Incidental High Renal Excretion of [18F]PSMA-1007 for Prostate Cancer PET/CT Imaging. Cancers 2022, 14, 2076. [Google Scholar] [CrossRef]
- Strauss, D.S.; Sachpekidis, C.; Kopka, K.; Pan, L.; Haberkorn, U.; Dimitrakopoulou-Strauss, A. Pharmacokinetic studies of [68Ga]Ga-PSMA-11 in patients with biochemical recurrence of prostate cancer: Detection, differences in temporal distribution and kinetic modelling by tissue type. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4472–4482. [Google Scholar] [CrossRef] [PubMed]
- Giesel, F.L.; Hadaschik, B.; Cardinale, J.; Radtke, J.; Vinsensia, M.; Lehnert, W.; Kesch, C.; Tolstov, Y.; Singer, S.; Grabe, N.; et al. F-18 labelled PSMA-1007: Biodistribution, radiation dosimetry and histopathological validation of tumor lesions in prostate cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 678–688. [Google Scholar] [CrossRef] [PubMed]
- Dias, A.H.; Jochumsen, M.R.; Zacho, H.D.; Munk, O.L.; Gormsen, L.C. Multiparametric dynamic whole-body PSMA PET/CT using [68Ga]Ga-PSMA-11 and [18F]PSMA-1007. EJNMMI Res. 2023, 13, 31. [Google Scholar] [CrossRef] [PubMed]
- Tolvanen, T.; Kalliokoski, K.; Malaspina, S.; Kuisma, A.; Lahdenpohja, S.; Postema, E.J.; Miller, M.P.; Scheinin, M. Safety, Biodistribution, and Radiation Dosimetry of 18F-rhPSMA-7.3 in Healthy Adult Volunteers. J. Nucl. Med. 2021, 62, 679–684. [Google Scholar] [CrossRef]
- Penny, R.; Fongenie, B.; Davis, P.; Sykes, J. Normal-organ distribution of PSMA-targeting PET radiopharmaceutical 18F-flotufolastat: A post hoc analysis of the LIGHTHOUSE and SPOTLIGHT studies. Am. J. Nucl. Med. Mol. Imaging 2024, 14, 337–344. [Google Scholar] [CrossRef]
- Hope, T.A.; Jadvar, H. PSMA PET AUC Updates: Inclusion of rh-PSMA-7.3. J. Nucl. Med. 2024, 65, 540. [Google Scholar] [CrossRef]
- Langbein, T.; Wang, H.; Rauscher, I.; Kroenke, M.; Knorr, K.; Wurzer, A.; Schwamborn, K.; Maurer, T.; Horn, T.; Haller, B.; et al. Utility of 18F-rhPSMA-7.3 PET for Imaging of Primary Prostate Cancer and Preoperative Efficacy in N-Staging of Unfavorable Intermediate- to Very High-Risk Patients Validated by Histopathology. J. Nucl. Med. 2022, 63, 1334–1342. [Google Scholar] [CrossRef]
- Pienta, K.J.; Gorin, M.A.; Rowe, S.P.; Carroll, P.R.; Pouliot, F.; Probst, S.; Saperstein, L.; Preston, M.A.; Alva, A.S.; Patnaik, A.; et al. A Phase 2/3 Prospective Multicenter Study of the Diagnostic Accuracy of Prostate Specific Membrane Antigen PET/CT with 18F-DCFPyL in Prostate Cancer Patients (OSPREY). J. Urol. 2021, 206, 52–61. [Google Scholar] [CrossRef]
- Dimitrakopoulou-Strauss, A. (German Cancer Research Center, Heidelberg, Germany). Personal Communication, 2025.
- Afshar-Oromieh, A.; Avtzi, E.; Giesel, F.L.; Holland-Letz, T.; Linhart, H.G.; Eder, M.; Eisenhut, M.; Boxler, S.; Hadaschik, B.A.; Kratochwil, C.; et al. The diagnostic value of PET/CT imaging with the 68Ga-labelled PSMA ligand HBED-CC in the diagnosis of recurrent prostate cancer. Eur. J. Nucl. Med. Mol. Imaging. 2015, 42, 197–209. [Google Scholar] [CrossRef]
- Fendler, W.P.; Calais, J.; Eiber, M.; Flavell, R.R.; Mishoe, A.; Feng, F.Y.; Nguyen, H.G.; Reiter, R.E.; Rettig, M.B.; Okamoto, S.; et al. Assessment of 68Ga-PSMA-11 PET Accuracy in Localizing Recurrent Prostate Cancer: A Prospective Single-Arm Clinical Trial. JAMA Oncol. 2019, 5, 856–863. [Google Scholar] [CrossRef]
- Eiber, M.; Maurer, T.; Souvatzoglou, M.; Beer, A.J.; Ruffani, A.; Haller, B.; Graner, F.-P.; Kübler, H.; Haberkorn, U.; Eisenhut, M.; et al. Evaluation of Hybrid 68Ga-PSMA Ligand PET/CT in 248 Patients with Biochemical Recurrence After Radical Prostatectomy. J. Nucl. Med. 2015, 56, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.J.; Rowe, S.P.; Gorin, M.A.; Saperstein, L.; Pouliot, F.; Josephson, D.; Wong, J.Y.C.; Pantel, A.R.; Cho, S.Y.; Gage, K.L.; et al. Diagnostic Performance of 18F-DCFPyL-PET/CT in Men with Biochemically Recurrent Prostate Cancer: Results from the CONDOR Phase III, Multicenter Study. Clin. Cancer Res. 2021, 27, 3674–3682. [Google Scholar] [CrossRef] [PubMed]
- Witkowska-Patena, E.; Giżewska, A.; Dziuk, M.; Miśko, J.; Budzyńska, A.; Walęcka-Mazur, A. Diagnostic performance of 18F-PSMA-1007 PET/CT in biochemically relapsed patients with prostate cancer with PSA levels ≤ 2.0 ng/ml. Prostate Cancer Prostatic Dis. 2020, 23, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Bluemel, C.; Krebs, M.; Polat, B.; Linke, F.; Eiber, M.; Samnick, S.; Lapa, C.; Lassmann, M.; Riedmiller, H.; Czernin, J.; et al. 68Ga-PSMA-PET/CT in Patients with Biochemical Prostate Cancer Recurrence and Negative 18F-Choline-PET/CT. Clin. Nucl. Med. 2016, 41, 515. [Google Scholar] [CrossRef]
- Rizzo, A.; Morbelli, S.; Albano, D.; Fornarini, G.; Cioffi, M.; Laudicella, R.; Dondi, F.; Grimaldi, S.; Bertagna, F.; Racca, M.; et al. The Homunculus of unspecific bone uptakes associated with PSMA-targeted tracers: A systematic review-based definition. Eur. J. Nucl. Med. Mol. Imaging 2024, 51, 3753–3764. [Google Scholar] [CrossRef]
- Grünig, H.; Maurer, A.; Thali, Y.; Kovacs, Z.; Strobel, K.; Burger, I.A.; Müller, J. Focal unspecific bone uptake on [18F]-PSMA-1007 PET: A multicenter retrospective evaluation of the distribution, frequency, and quantitative parameters of a potential pitfall in prostate cancer imaging. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4483–4494. [Google Scholar] [CrossRef]
- Sahlmann, C.-O.; Meller, B.; Bouter, C.; Ritter, C.O.; Ströbel, P.; Lotz, J.; Trojan, L.; Meller, J.; Hijazi, S. Biphasic 68Ga-PSMA-HBED-CC-PET/CT in patients with recurrent and high-risk prostate carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 898–905. [Google Scholar] [CrossRef]
- Afshar-Oromieh, A.; Zechmann, C.M.; Malcher, A.; Eder, M.; Eisenhut, M.; Linhart, H.G.; Holland-Letz, T.; Hadaschik, B.A.; Giesel, F.L.; Debus, J.; et al. Comparison of PET imaging with a [69]Ga-labelled PSMA ligand and [18]F-choline-based PET/CT for the diagnosis of recurrent prostate cancer. Eur. J. Nucl. Med. Mol. Imaging. 2014, 41, 11–20. [Google Scholar] [CrossRef]
- Treglia, G.; Pereira Mestre, R.; Ferrari, M.; Bosetti, D.G.; Pascale, M.; Oikonomou, E.; De Dosso, S.; Jermini, F.; Prior, J.O.; Roggero, E.; et al. Radiolabelled choline versus PSMA PET/CT in prostate cancer restaging: A meta-analysis. Am. J. Nucl. Med. Mol. Imaging 2019, 9, 127–139. [Google Scholar]
- Yu, W.; Zhao, M.; Deng, Y.; Liu, S.; Du, G.; Yan, B.; Zhao, Z.; Sun, N.; Guo, J. Meta-analysis of 18 F-PSMA-1007 PET/CT, 18 F-FDG PET/CT, and 68Ga-PSMA PET/CT in diagnostic efficacy of prostate Cancer. Cancer Imaging 2023, 23, 77. [Google Scholar] [CrossRef]
- Scarsbrook, A.F.; Bottomley, D.; Teoh, E.J.; Bradley, K.M.; Payne, H.; Afaq, A.; Bomanji, J.; Van As, N.; Chua, S.; Hoskin, P.; et al. Effect of 18F-Fluciclovine Positron Emission Tomography on the Management of Patients With Recurrence of Prostate Cancer: Results from the FALCON Trial. Int. J. Radiat. Oncol. Biol. Phys. 2020, 107, 316–324. [Google Scholar] [CrossRef]
- Wang, R.; Shen, G.; Huang, M.; Tian, R. The Diagnostic Role of 18F-Choline, 18F-Fluciclovine and 18F-PSMA PET/CT in the Detection of Prostate Cancer with Biochemical Recurrence: A Meta-Analysis. Front. Oncol. 2021, 11, 684629. [Google Scholar] [CrossRef] [PubMed]
- Jani, A.B.; Ravizzini, G.C.; Gartrell, B.A.; Siegel, B.A.; Twardowski, P.; Saltzstein, D.; Fleming, M.T.; Chau, A.; Davis, P.; Chapin, B.F.; et al. Diagnostic Performance and Safety of 18F-rhPSMA-7.3 Positron Emission Tomography in Men with Suspected Prostate Cancer Recurrence: Results from a Phase 3, Prospective, Multicenter Study (SPOTLIGHT). J. Urol. 2023, 210, 299–311. [Google Scholar] [CrossRef] [PubMed]
- Lowentritt, B.H.; Jani, A.B.; Helfand, B.T.; Uchio, E.M.; Morris, M.A.; Michalski, J.M.; Chau, A.; Davis, P.; Chapin, B.F.; Schuster, D.M. Impact of Clinical Factors on 18F-Flotufolastat Detection Rates in Men with Recurrent Prostate Cancer: Exploratory Analysis of the Phase 3 SPOTLIGHT Study. Adv. Radiat. Oncol. 2024, 9, 101532. [Google Scholar] [CrossRef] [PubMed]
- Giesel, F.L.; Knorr, K.; Spohn, F.; Will, L.; Maurer, T.; Flechsig, P.; Neels, O.; Schiller, K.; Amaral, H.; Weber, W.A.; et al. Detection Efficacy of 18F-PSMA-1007 PET/CT in 251 Patients with Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy. J. Nucl. Med. 2019, 60, 362–368. [Google Scholar] [CrossRef]
- Tateishi, U.; Kimura, K.; Tsuchiya, J.; Kano, D.; Watabe, T.; Nonomura, N.; Saito, K.; Yokoyama, K.; Yamagiwa, K.; Adachi, T.; et al. Phase I/IIa trial of 18F-prostate specific membrane antigen (PSMA) 1007 PET/CT in healthy volunteers and prostate cancer patients. Jpn. J. Clin. Oncol. 2024, 54, 282–291. [Google Scholar] [CrossRef]
- Ahmadi Bidakhvidi, N.; Laenen, A.; Jentjens, S.; Deroose, C.M.; Van Laere, K.; De Wever, L.; Mai, C.; Berghen, C.; De Meerleer, G.; Haustermans, K.; et al. Parameters predicting [18F]PSMA-1007 scan positivity and type and number of detected lesions in patients with biochemical recurrence of prostate cancer. EJNMMI Res. 2021, 11, 41. [Google Scholar] [CrossRef]
- Grubmüller, B.; Baltzer, P.; D’Andrea, D.; Korn, S.; Haug, A.R.; Hacker, M.; Grubmüller, K.H.; Goldner, G.M.; Wadsak, W.; Pfaff, S.; et al. 68Ga-PSMA 11 ligand PET imaging in patients with biochemical recurrence after radical prostatectomy—Diagnostic performance and impact on therapeutic decision-making. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 235–242. [Google Scholar] [CrossRef]
- Afshar-Oromieh, A.; Holland-Letz, T.; Giesel, F.L.; Kratochwil, C.; Mier, W.; Haufe, S.; Debus, N.; Eder, M.; Eisenhut, M.; Schäfer, M.; et al. Diagnostic performance of 68Ga-PSMA-11 (HBED-CC) PET/CT in patients with recurrent prostate cancer: Evaluation in 1007 patients. Eur. J. Nucl. Med. Mol. Imaging. 2017, 44, 1258–1268. [Google Scholar] [CrossRef]
- Calais, J.; Czernin, J.; Fendler, W.P.; Elashoff, D.; Nickols, N.G. Randomized prospective phase III trial of 68Ga-PSMA-11 PET/CT molecular imaging for prostate cancer salvage radiotherapy planning [PSMA-SRT]. BMC Cancer 2019, 19, 18. [Google Scholar] [CrossRef]
- Ceci, F.; Uprimny, C.; Nilica, B.; Geraldo, L.; Kendler, D.; Kroiss, A.; Bektic, J.; Horninger, W.; Lukas, P.; Decristoforo, C.; et al. 68Ga-PSMA PET/CT for restaging recurrent prostate cancer: Which factors are associated with PET/CT detection rate? Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1284–1294. [Google Scholar] [CrossRef] [PubMed]
- Dyankova, M.; Dancheva, Z.; Dokova, K.; Klisarova, A. Evaluation of hybrid PET/CT imaging with the 68Ga-labelled PSMA ligand in patients with prostate cancer and biochemical progression in the low-range values of PSA after radical prostatectomy. Scr. Sci. Med. 2022, 54, 29–39. [Google Scholar] [CrossRef]
- Rowe, S.P.; Campbell, S.P.; Mana-Ay, M.; Szabo, Z.; Allaf, M.E.; Pienta, K.J.; Pomper, M.G.; Ross, A.E.; Gorin, M.A. Prospective Evaluation of PSMA-Targeted 18F-DCFPyL PET/CT in Men with Biochemical Failure After Radical Prostatectomy for Prostate Cancer. J. Nucl. Med. 2020, 61, 58–61. [Google Scholar] [CrossRef] [PubMed]
- Wondergem, M.; Jansen, B.H.E.; Van Der Zant, F.M.; Van Der Sluis, T.M.; Knol, R.J.J.; Van Kalmthout, L.W.M.; Hoekstra, O.S.; Van Moorselaar, R.J.A.; Oprea-Lager, D.E.; Vis, A.N. Early lesion detection with 18F-DCFPyL PET/CT in 248 patients with biochemically recurrent prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1911–1918. [Google Scholar] [CrossRef]
- Mena, E.; Lindenberg, M.L.; Turkbey, I.B.; Shih, J.H.; Harmon, S.A.; Lim, I.; Lin, F.; Adler, S.; Eclarinal, P.; McKinney, Y.L.; et al. 18F-DCFPyL PET/CT Imaging in Patients with Biochemically Recurrent Prostate Cancer After Primary Local Therapy. J. Nucl. Med. 2020, 61, 881–889. [Google Scholar] [CrossRef]
- Rousseau, E.; Wilson, D.; Lacroix-Poisson, F.; Krauze, A.; Chi, K.; Gleave, M.; McKenzie, M.; Tyldesley, S.; Goldenberg, S.L.; Bénard, F. A Prospective Study on 18F-DCFPyL PSMA PET/CT Imaging in Biochemical Recurrence of Prostate Cancer. J. Nucl. Med. 2019, 60, 1587–1593. [Google Scholar] [CrossRef]
- Olivier, P.; Giraudet, A.-L.; Skanjeti, A.; Merlin, C.; Weinmann, P.; Rudolph, I.; Hoepping, A.; Gauthé, M. Phase III Study of 18F-PSMA-1007 Versus 18F-Fluorocholine PET/CT for Localization of Prostate Cancer Biochemical Recurrence: A Prospective, Randomized, Crossover Multicenter Study. J. Nucl. Med. 2023, 64, 579–585. [Google Scholar] [CrossRef]
- Kim, J.; Lee, S.; Kim, D.; Kim, H.J.; Oh, K.T.; Kim, S.J.; Choi, Y.D.; Giesel, F.L.; Kopka, K.; Hoepping, A.; et al. Combination of [18F]FDG and [18F]PSMA-1007 PET/CT predicts tumour aggressiveness at staging and biochemical failure postoperatively in patients with prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2024, 51, 1763–1772. [Google Scholar] [CrossRef]
- Zhou, X.; Li, Y.; Jiang, X.; Wang, X.; Chen, S.; Shen, T.; You, J.; Lu, H.; Liao, H.; Li, Z.; et al. Intra-Individual Comparison of 18F-PSMA-1007 and 18F-FDG PET/CT in the Evaluation of Patients With Prostate Cancer. Front. Oncol. 2021, 10, 585213. [Google Scholar] [CrossRef]
- Calais, J.; Ceci, F.; Eiber, M.; Hope, T.A.; Hofman, M.S.; Rischpler, C.; Bach-Gansmo, T.; Nanni, C.; Savir-Baruch, B.; Elashoff, D.; et al. 18F-fluciclovine PET-CT and 68Ga-PSMA-11 PET-CT in patients with early biochemical recurrence after prostatectomy: A prospective, single-centre, single-arm, comparative imaging trial. Lancet Oncol. 2019, 20, 1286–1294. [Google Scholar] [CrossRef]
- Loeff, C.C.; van Gemert, W.; Privé, B.M.; van Oort, I.M.; Hermsen, R.; Somford, D.M.; Nagarajah, J.; Heijmen, L.; Janssen, M.J.R. [18F]PSMA-1007 PET for biochemical recurrence of prostate cancer, a comparison with [18F]Fluciclovine. EJNMMI Rep. 2024, 8, 38. [Google Scholar] [CrossRef] [PubMed]
- Alberts, I.; Bütikofer, L.; Rominger, A.; Afshar-Oromieh, A. A randomised, prospective and head-to-head comparison of [68Ga]Ga-PSMA-11 and [18F]PSMA-1007 for the detection of recurrent prostate cancer in PSMA-ligand PET/CT-Protocol design and rationale. PLoS ONE 2022, 17, e0270269. [Google Scholar] [CrossRef] [PubMed]
- Giesel, F.L.; Will, L.; Lawal, I.; Lengana, T.; Kratochwil, C.; Vorster, M.; Neels, O.; Reyneke, F.; Haberkon, U.; Kopka, K.; et al. Intraindividual Comparison of 18F-PSMA-1007 and 18F-DCFPyL PET/CT in the Prospective Evaluation of Patients with Newly Diagnosed Prostate Carcinoma: A Pilot Study. J. Nucl. Med. 2018, 59, 1076–1080. [Google Scholar] [CrossRef] [PubMed]
- Rowe, S.P.; Gage, K.L.; Faraj, S.F.; Macura, K.J.; Cornish, T.C.; Gonzalez-Roibon, N.; Guner, G.; Munari, E.; Partin, A.W.; Pavlovich, C.P.; et al. 18F-DCFBC PET/CT for PSMA-Based Detection and Characterization of Primary Prostate Cancer. J. Nucl. Med. 2015, 56, 1003–1010. [Google Scholar] [CrossRef]
- Turkbey, B.; Mena, E.; Lindenberg, L.; Adler, S.; Bednarova, S.; Berman, R.; Ton, A.T.; McKinney, Y.; Eclarinal, P.; Hill, C.; et al. 18F-DCFBC Prostate-Specific Membrane Antigen-Targeted PET/CT Imaging in Localized Prostate Cancer: Correlation With Multiparametric MRI and Histopathology. Clin. Nucl. Med. 2017, 42, 735–740. [Google Scholar] [CrossRef]
- Dietlein, F.; Hohberg, M.; Kobe, C.; Zlatopolskiy, B.D.; Krapf, P.; Endepols, H.; Täger, P.; Hammes, J.; Heidenreich, A.; Neumaier, B.; et al. An 18F-Labeled PSMA Ligand for PET/CT of Prostate Cancer: First-in-Humans Observational Study and Clinical Experience with 18F-JK-PSMA-7 During the First Year of Application. J. Nucl. Med. 2020, 61, 202–209. [Google Scholar] [CrossRef]
- Zlatopolskiy, B.D.; Endepols, H.; Krapf, P.; Guliyev, M.; Urusova, E.A.; Richarz, R.; Hohberg, M.; Dietlein, M.; Drzezga, A.; Neumaier, B. Discovery of 18F-JK-PSMA-7, a PET Probe for the Detection of Small PSMA-Positive Lesions. J. Nucl. Med. 2019, 60, 817–823. [Google Scholar] [CrossRef]
- Piron, S.; De Man, K.; Schelfhout, V.; Van Laeken, N.; Kersemans, K.; Achten, E.; De Vos, F.; Ost, P. Optimization of PET protocol and interrater reliability of 18F-PSMA-11 imaging of prostate cancer. EJNMMI Res. 2020, 10, 14. [Google Scholar] [CrossRef]
- Liu, T.; Liu, C.; Xu, X.; Liu, F.; Guo, X.; Li, N.; Wang, X.; Yang, J.; Yang, X.; Zhu, H.; et al. Preclinical Evaluation and Pilot Clinical Study of Al18F-PSMA-BCH for Prostate Cancer PET Imaging. J. Nucl. Med. 2019, 60, 1284–1292. [Google Scholar] [CrossRef]
- Zechmann, C.M.; Afshar-Oromieh, A.; Armor, T.; Stubbs, J.B.; Mier, W.; Hadaschik, B.; Joyal, J.; Kopka, K.; Debus, J.; Babich, J.W.; et al. Radiation dosimetry and first therapy results with a 124I/131I-labeled small molecule (MIP-1095) targeting PSMA for prostate cancer therapy. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1280–1292. [Google Scholar] [CrossRef]
- Suh, M.; Ryoo, H.G.; Kang, K.W.; Jeong, J.M.; Jeong, C.W.; Kwak, C.; Cheon, G.J. Phase I Clinical Trial of Prostate-Specific Membrane Antigen-Targeting 68Ga-NGUL PET/CT in Healthy Volunteers and Patients with Prostate Cancer. Korean J. Radiol. 2022, 23, 911. [Google Scholar] [CrossRef] [PubMed]
- Afshar-Oromieh, A.; Hetzheim, H.; Kratochwil, C.; Benesova, M.; Eder, M.; Neels, O.C.; Eisenhut, M.; Kübler, W.; Holland-Letz, T.; Giesel, F.L.; et al. The Theranostic PSMA Ligand PSMA-617 in the Diagnosis of Prostate Cancer by PET/CT: Biodistribution in Humans, Radiation Dosimetry, and First Evaluation of Tumor Lesions. J. Nucl. Med. 2015, 56, 1697–1705. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zang, J.; Wang, H.; Liu, Q.; Li, F.; Lin, Y.; Huo, L.; Jacobson, O.; Niu, G.; Fan, X.; et al. Pretherapeutic 68Ga-PSMA-617 PET May Indicate the Dosimetry of 177Lu-PSMA-617 and 177Lu-EB-PSMA-617 in Main Organs and Tumor Lesions. Clin. Nucl. Med. 2019, 44, 431. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Gai, Y.; Liu, Q.; Ruan, W.; Liu, F.; Hu, F.; Zhang, X.; Lan, X. Optimized Application of 68Ga-Prostate-Specific Membrane Antigen-617 Whole-Body PET/CT and Pelvic PET/MR in Prostate Cancer Initial Diagnosis and Staging. Front. Med. 2021, 8, 657619. [Google Scholar] [CrossRef]
- Frenzel, T.; Tienken, M.; Abel, M.; Berliner, C.; Klutmann, S.; Beyersdorff, D.; Schwarz, R.; Krüll, A.; Bannas, P. The impact of [68Ga]PSMA I&T PET/CT on radiotherapy planning in patients with prostate cancer. Strahlenther. Onkologie 2018, 194, 646–654. [Google Scholar] [CrossRef]
- Schmuck, S.; Klot, C.A.v.; Henkenberens, C.; Sohns, J.M.; Christiansen, H.; Wester, H.-J.; Ross, T.L.; Bengel, F.M.; Derlin, T. Initial Experience with Volumetric 68Ga-PSMA I&T PET/CT for Assessment of Whole-Body Tumor Burden as a Quantitative Imaging Biomarker in Patients with Prostate Cancer. J. Nucl. Med. 2017, 58, 1962–1968. [Google Scholar] [CrossRef]
- Weineisen, M.; Schottelius, M.; Simecek, J.; Baum, R.P.; Yildiz, A.; Beykan, S.; Kulkarni, H.R.; Lassmann, M.; Klette, I.; Eiber, M.; et al. 68Ga- and 177Lu-Labeled PSMA I&T: Optimization of a PSMA-Targeted Theranostic Concept and First Proof-of-Concept Human Studies. J. Nucl. Med. 2015, 56, 1169–1176. [Google Scholar] [CrossRef]
- Cytawa, W.; Seitz, A.K.; Kircher, S.; Fukushima, K.; Tran-Gia, J.; Schirbel, A.; Bandurski, T.; Lass, P.; Krebs, M.; Połom, W.; et al. 68Ga-PSMA I&T PET/CT for primary staging of prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 168–177. [Google Scholar] [CrossRef]
- Gühne, F.; Radke, S.; Winkens, T.; Kühnel, C.; Greiser, J.; Seifert, P.; Drescher, R.; Freesmeyer, M. Differences in Distribution and Detection Rate of the [68Ga]Ga-PSMA Ligands PSMA-617, -I&T and -11—Inter-Individual Comparison in Patients with Biochemical Relapse of Prostate Cancer. Pharmaceuticals 2022, 15, 9. [Google Scholar] [CrossRef]
- Privé, B.M.; Derks, Y.H.W.; Rosar, F.; Franssen, G.M.; Peters, S.M.B.; Khreish, F.; Bartholomä, M.; Maus, S.; Gotthardt, M.; Laverman, P.; et al. 89Zr-labeled PSMA ligands for pharmacokinetic PET imaging and dosimetry of PSMA-617 and PSMA-I&T: A preclinical evaluation and first in man. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 2064–2076. [Google Scholar] [CrossRef]
- Grubmüller, B.; Baum, R.P.; Capasso, E.; Singh, A.; Ahmadi, Y.; Knoll, P.; Floth, A.; Righi, S.; Zandieh, S.; Meleddu, C.; et al. 64Cu-PSMA-617 PET/CT Imaging of Prostate Adenocarcinoma: First In-Human Studies. Cancer Biother. Radiopharm. 2016, 31, 277–286. [Google Scholar] [CrossRef]
- Hoberück, S.; Wunderlich, G.; Michler, E.; Hölscher, T.; Walther, M.; Seppelt, D.; Platzek, I.; Zöphel, K.; Kotzerke, J. Dual-time-point 64Cu-PSMA-617-PET/CT in patients suffering from prostate cancer. J. Label. Compd. Radiopharm. 2019, 62, 523–532. [Google Scholar] [CrossRef]
- Cantiello, F.; Crocerossa, F.; Russo, G.I.; Gangemi, V.; Ferro, M.; Vartolomei, M.D.; Lucarelli, G.; Mirabelli, M.; Scafuro, C.; Ucciero, G.; et al. Comparison Between 64Cu-PSMA-617 PET/CT and 18F-Choline PET/CT Imaging in Early Diagnosis of Prostate Cancer Biochemical Recurrence. Clin. Genitourin. Cancer 2018, 16, 385–391. [Google Scholar] [CrossRef] [PubMed]
- SOLAR: Copper Cu64 PSMA I&T Injection in Patients with Histologically Proven Metastatic Prostate Cancer. Available online: https://www.curiumpharma.com/resources/current-clinical-trials/solar-clinical-trial/ (accessed on 19 April 2025).
- Bernabeu, T.B.; Mansi, R.; Pozzo, L.D.; Zanger, S.; Gaonkar, R.H.; McDougall, L.; Rose, F.D.; Jaafar-Thiel, L.; Herz, M.; Eiber, M.; et al. 61Cu-PSMA–Targeted PET for Prostate Cancer: From Radiotracer Development to First-in-Human Imaging. J. Nucl. Med. 2024, 65, 1427–1434. [Google Scholar] [CrossRef] [PubMed]
- NUCLIDIUM Announces First Patient Imaged in Phase 1 Study Evaluating 61Cu-based Radiotracer in Patients with PSMA-positive Prostate Cancer—Nuclidium. Available online: https://nuclidium.com/nuclidium-announces-first-patient-imaged-in-phase-1-study-evaluating-61cu-based-radiotracer-in-patients-with-psma-positive-prostate-cancer/ (accessed on 19 April 2025).
- Yang, N.; Guo, X.-y.; Ding, J.; Wang, F.; Liu, T.-l.; Zhu, H.; Yang, Z. Copper-64 Based PET-Radiopharmaceuticals: Ways to Clinical Translational. Semin. Nucl. Med. 2024, 54, 792–800. [Google Scholar] [CrossRef]
- Liu, H.; Zhang, X.; Zhang, J.; Pan, Y.; Wen, H.; Xu, X.; Wu, S.; Wang, Y.; Zhang, C.; Ma, G.; et al. Comparison of 64Cu-DOTA-PSMA-3Q and 64Cu-NOTA-PSMA-3Q utilizing NOTA and DOTA as bifunctional chelators in prostate cancer: Preclinical assessment and preliminary clinical PET/CT imaging. Eur. J. Nucl. Med. Mol. Imaging 2025, 52, 2792–2803. [Google Scholar] [CrossRef]
- Chen, F.; Zhang, H.; Zhan, Y.; Huang, X.; He, Z.; Ma, D.; Tang, T.; Li, S. Preclinical and clinical evaluation of [64Cu]Cu-PSMA-Q PET/CT for prostate cancer detection and its comparison with [18F]FDG imaging. Sci. Rep. 2025, 15, 14431. [Google Scholar] [CrossRef] [PubMed]
- Clarity Receives, U.S. FDA Fast Track Designation for Cu-64 SAR-bisPSMA in Biochemical Recurrence of Prostate Cancer. Available online: https://www.claritypharmaceuticals.com/news/ftd-2/ (accessed on 19 April 2025).
- Registrational Phase III CLARIFY Trial in Prostate Cancer Commences. Available online: https://www.claritypharmaceuticals.com/news/clarifyphase3/ (accessed on 11 June 2025).
- 64Cu-SAR-bisPSMA and 67Cu-SAR-bisPSMA for Identification and Treatment of PSMA-Expressing Metastatic Castrate Resistant Prostate Cancer (SECuRE). Available online: https://clinicaltrials.gov/study/NCT04868604 (accessed on 19 April 2025).
- Müller, C.; Singh, A.; Umbricht, C.A.; Kulkarni, H.R.; Johnston, K.; Benešová, M.; Senftleben, S.; Müller, D.; Vermeulen, C.; Schibli, R.; et al. Preclinical Investigations and First-in-Human Application of 152Tb-PSMA-617 for PET/CT Imaging of Prostate Cancer. EJNMMI Res. 2019, 9, 68. [Google Scholar] [CrossRef]
- Eppard, E.; de la Fuente, A.; Benešová, M.; Khawar, A.; Bundschuh, R.A.; Gärtner, F.C.; Kreppel, B.; Kopka, K.; Essler, M.; Rösch, F. Clinical Translation and First In-Human Use of [44Sc]Sc-PSMA-617 for PET Imaging of Metastasized Castrate-Resistant Prostate Cancer. Theranostics 2017, 7, 4359–4369. [Google Scholar] [CrossRef]
- Khawar, A.; Eppard, E.; Sinnes, J.P.; Roesch, F.; Ahmadzadehfar, H.; Kürpig, S.; Meisenheimer, M.; Gaertner, F.C.; Essler, M.; Bundschuh, R.A. [44Sc]Sc-PSMA-617 Biodistribution and Dosimetry in Patients With Metastatic Castration-Resistant Prostate Carcinoma. Clin. Nucl. Med. 2018, 43, 323. [Google Scholar] [CrossRef]
- Kepenek, F.; Can, C.; Kömek, H.; Kaplan, İ.; Gündoğan, C.; Ebinç, S.; Güzel, Y.; Agüloglu, N.; Karaoglan, H.; Taşdemir, B. Combination of [68Ga]Ga-PSMA PET/CT and [18F]FDG PET/CT in demonstrating dedifferentiation in castration-resistant prostate cancer. Médecine Nucléaire 2023, 47, 193–199. [Google Scholar] [CrossRef]
- Khreish, F.; Ribbat, K.; Bartholomä, M.; Maus, S.; Stemler, T.; Hierlmeier, I.; Linxweiler, J.; Schreckenberger, M.; Ezziddin, S.; Rosar, F. Value of Combined PET Imaging with [18F]FDG and [68Ga]Ga-PSMA-11 in mCRPC Patients with Worsening Disease during [177Lu]Lu-PSMA-617 RLT. Cancers 2021, 13, 4134. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Wang, Y.; Zhu, Y.; Shi, Y.; Xu, L.; Huang, G.; Liu, J. The Added Value of 18F-FDG PET/CT Compared with 68Ga-PSMA PET/CT in Patients with Castration-Resistant Prostate Cancer. J. Nucl. Med. 2022, 63, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Zhang, T.; Chen, S.; Bu, T.; Zhao, J.; Ni, X.; Shi, B.; Gan, H.; Wei, Y.; Wang, Q.; et al. Nomogram to predict the presence of PSMA-negative but FDG-positive lesion in castration-resistant prostate cancer: A multicenter cohort study. Ther. Adv. Med. Oncol. 2024, 16, 17588359231220506. [Google Scholar] [CrossRef]
- Mapelli, P.; Ghezzo, S.; Samanes Gajate, A.M.; Preza, E.; Brembilla, G.; Cucchiara, V.; Ahmed, N.; Bezzi, C.; Presotto, L.; Bettinardi, V.; et al. Preliminary Results of an Ongoing Prospective Clinical Trial on the Use of 68Ga-PSMA and 68Ga-DOTA-RM2 PET/MRI in Staging of High-Risk Prostate Cancer Patients. Diagnostics 2021, 11, 2068. [Google Scholar] [CrossRef]

| Working Name | Trade Name | Other Name | Company |
|---|---|---|---|
| [68Ga]Ga-PSMA-11 | Locametz®/Illuccix®/GozellixTM | Gallium Ga 68 gozetotide | Novartis AG (Basel, Switzerland)/Telix Pharmaceuticals, Ltd. (Melbourne, Australia) |
| [18F]DCFPyL | Pylarify®/Pylclari® | Piflufolastat F 18 | Progenics Pharmaceuticals, Inc. (New York, NY, USA)/Curium PET France SA (Paris, France) |
| [18F]PSMA-1007 | Radelumin® | - | ABX GmbH (Radeberg, Germany) |
| [18F]rhPSMA-7.3 | Posluma® | Flotufolastat F 18 gallium | Blue Earths Diagnostics, Ltd. (Oxford, UK) |
| Imaging Agent | pH Value | Radioactivity Concentration [MBq/mL] | Amount of Carrier [µg/GBq] |
|---|---|---|---|
| Radelumin®: [18F]PSMA-1007 | 4.5–8.5 | 1300 or 2000 | - |
| Pylarify®/Pylclari®: [18F]DCFPyL | 4.5–7.5 (EU) 4.5–7.0 (US) | 1000 or 1500 (EU) 37–2960 (US) | - 0.27 (US) |
| Posluma®: [18F]rhPSMA-7.3 | 4.0–6.0 | 296–5846 | 3.42 |
| Imaging Agent | Recommended Activity for Adults per Injection | Volume Limit [mL] | Imaging Window [min p.i.] |
|---|---|---|---|
| Radelumin®: [18F]PSMA-1007 | EMA: 3.6–4.4 MBq/kg e.g., 70 kg patient: 252–308 MBq Maximum: 450 MBq regardless of patient weight | ≤10 | 90–120 |
| FDA: Not approved yet | |||
| Posluma®: [18F]rhPSMA-7.3 | EMA: Not approved yet | ≤5 (undiluted) | 60 |
| FDA: Fixed dose of 296 MBq No weight-based adjustments | |||
| Locametz®/Illuccix®/GozellixTM: [68Ga]Ga-PSMA-11 | 1.8–2.2 MBq/kg Minimum: 111 MBq Maximum: 259 MBq | None † | 50–100 |
| Pylarify®/Pylclari®: [18F]DCFPyL | EMA: 3–5 MBq/kg e.g., 70 kg patient: 210–350 MBq Minimum: 190 MBq Maximum: 360 MBq | 0.2–10 | 90–120 |
| FDA: Recommended dose of 333 MBq Minimum: 296 MBq Maximum: 370 MBq | None † | 60–90 |
| Critical Organ | Radelumin® [18F]PSMA-1007 | Posluma® [18F]rhPSMA-7.3 | Locametz®/Illuccix®/GozellixTM [68Ga]Ga-PSMA-11 | Pylclari®/Pylarify® [18F]DCFPyL † |
|---|---|---|---|---|
| Mean Absorbed Doses [mGy/MBq] | ||||
| Adrenals | 0.0349 | 0.184 | 0.0156 | 0.0326 |
| Bone surfaces | N.A. | N.A. | N.A. | 0.00662 |
| Brain | 0.0030 | 0.002 | 0.0104 | 0.00215 |
| Breast | N.A. | 0.004 | 0.0103 | 0.00767 |
| Gallbladder | 0.1400 | 0.017 | 0.0157 | 0.0255 |
| Gastrointestinal tract | ||||
| Stomach | 0.0170 | 0.012 | 0.0129 | 0.0127 |
| Small intestine | 0.0334 | 0.012 | 0.014 | 0.0101 |
| Lower colon | 0.0239 | 0.007 | 0.0134 | 0.0101 |
| Upper colon | 0.0176 | 0.01 | N.A. | 0.0125 |
| Heart wall | 0.0259 | 0.02 | 0.012 | 0.0178 |
| Kidneys | 0.1030 | 0.0172 | 0.3714 | 0.124 |
| Liver | 0.0883 | 0.062 | 0.0409 | 0.0388 |
| Lungs | 0.0147 | 0.01 | 0.0111 | 0.0121 |
| Muscles | 0.0103 | 0.006 | 0.0103 | 0.00714 |
| Pancreas | 0.0677 | 0.028 | 0.0147 | 0.0183 |
| Red marrow | 0.0121 | 0.01 | 0.0114 | 0.00851 |
| Skin | N.A. | 0.002 | 0.0091 | 0.0054 |
| Spleen | 0.0851 | 0.083 | 0.065 | 0.0283 |
| Testes | 0.0074 | 0.005 | 0.0111 | 0.00638 |
| Thymus | 0.0106 | 0.01 | 0.0105 | 0.00769 |
| Thyroid | 0.0151 | 0.01 | 0.0104 | 0.00687 |
| Urinary bladder | 0.0212 | 0.006 | 0.0982 | 0.00712 |
| Effective dose [mSv/MBq] | 0.0191 | 0.014 | 0.0169 | 0.0121 |
| Imaging Agent | Administered Activity [MBq] | Effective Dose [mSv] | Critical Organs | Radiation Doses [mGy] |
|---|---|---|---|---|
| Radelumin®: [18F]PSMA-1007 | 280 A | 5.3 | Gallbladder | 39 |
| Kidneys | 29 | |||
| Liver | 25 | |||
| Posluma®: [18F]rhPSMA-7.3 | 296 B | 4.1 | Adrenal glands | 54.3 |
| Kidneys | 51 | |||
| Submandibular glands | 43.8 | |||
| Locametz®/Illuccix®/GozellixTM: [68Ga]Ga-PSMA-11 | 259 C | 4.4 | Kidneys | 96.2 |
| Urinary bladder | 25.4 | |||
| Spleen | 16.8 | |||
| Pylarify®/Pylclari®: [18F]DCFPyL | 360 D | 4.4 | Kidneys | 44.6 |
| Liver | 14 | |||
| Spleen | 10.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hennrich, U.; Wagner, L.; Taş, H.; Kovacs, L.; Benešová-Schäfer, M. Revolutionizing Prostate Cancer Detection: The Role of Approved PSMA-PET Imaging Agents. Pharmaceuticals 2025, 18, 906. https://doi.org/10.3390/ph18060906
Hennrich U, Wagner L, Taş H, Kovacs L, Benešová-Schäfer M. Revolutionizing Prostate Cancer Detection: The Role of Approved PSMA-PET Imaging Agents. Pharmaceuticals. 2025; 18(6):906. https://doi.org/10.3390/ph18060906
Chicago/Turabian StyleHennrich, Ute, Laurène Wagner, Harun Taş, Luciana Kovacs, and Martina Benešová-Schäfer. 2025. "Revolutionizing Prostate Cancer Detection: The Role of Approved PSMA-PET Imaging Agents" Pharmaceuticals 18, no. 6: 906. https://doi.org/10.3390/ph18060906
APA StyleHennrich, U., Wagner, L., Taş, H., Kovacs, L., & Benešová-Schäfer, M. (2025). Revolutionizing Prostate Cancer Detection: The Role of Approved PSMA-PET Imaging Agents. Pharmaceuticals, 18(6), 906. https://doi.org/10.3390/ph18060906