
Intraoperative Confocal Laser Endomicroscopy Detects Prostate Cancer at the Single-Cell Level with High Specificity and in Real Time: A Preclinical Proof of Concept

 , ,
, ,
Abstract

1. Introduction
2. Results
2.1. Specific NIR-pCLE Detection of PSMA-Positive Cells In Vitro
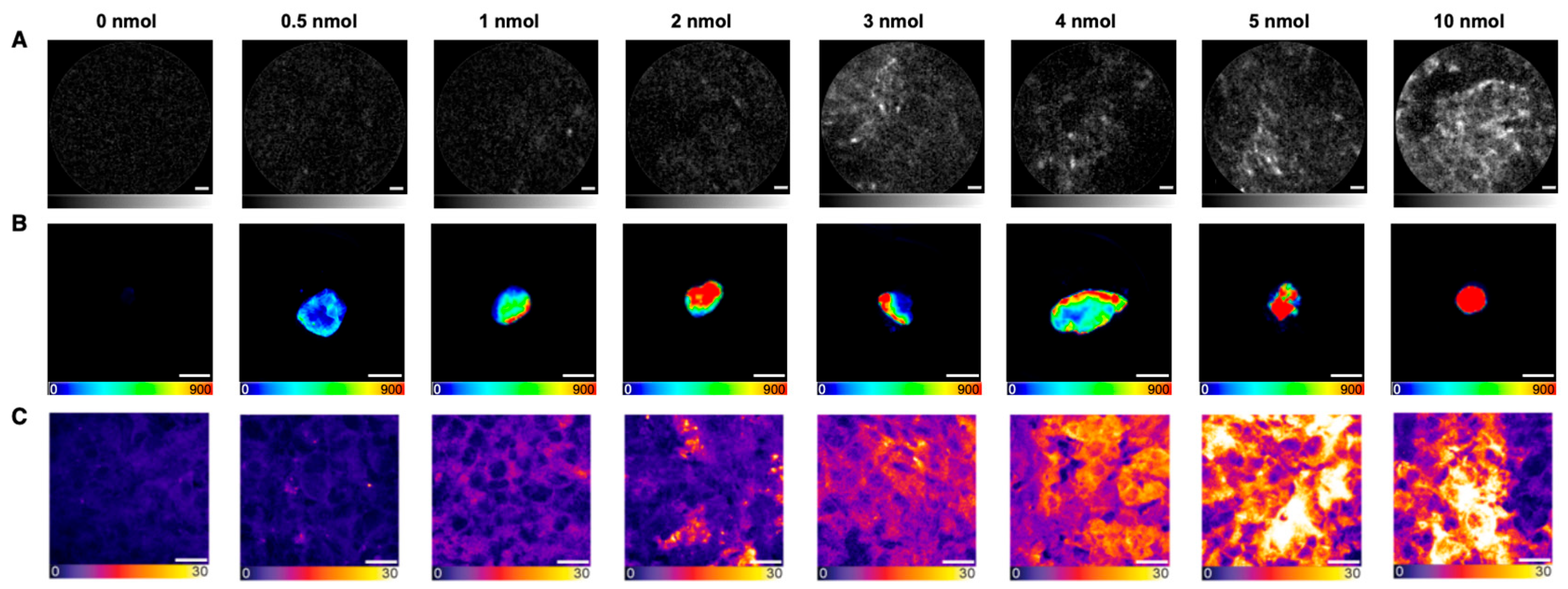
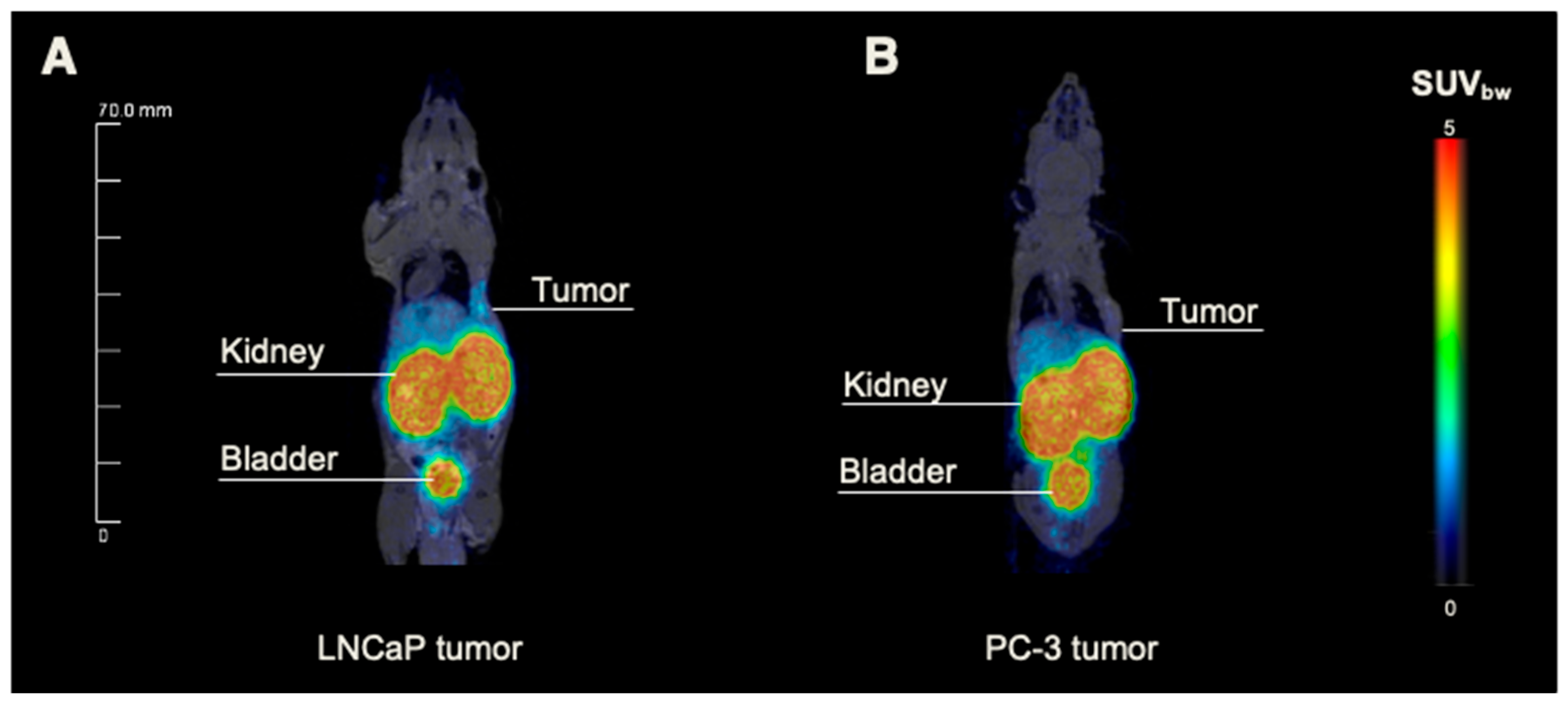
2.2. Dose Finding for PSMA-Specific NIR-pCLE Imaging In Vivo
2.3. Detection of PSMA-914 Fluorescence at the Single-Cell Level: In Vivo Proof of Concept
3. Discussion
4. Materials and Methods
4.1. Study Drug and Radiolabeling
4.2. In Vitro Imaging
4.3. In Vivo Imaging Study
4.4. Confocal Microscopy
4.5. Statistical Aspects
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BCR | Biochemical recurrence |
| CT | Computed tomography |
| EMA | European Medicines Agency |
| FDA | US Food and Drug Administration |
| mCRPC | Metastatic castration-resistant prostate cancer |
| MRI | Magnetic resonance imaging |
| NIR | Near-infrared |
| PCa | Prostate cancer |
| PET | Positron emission tomography |
| pCLE | Probe-based confocal laser endomicroscopy |
| PSM | Positive surgical margin |
| PSMA | Prostate-specific membrane antigen |
References
- Schwarzenboeck, S.M.; Rauscher, I.; Bluemel, C.; Fendler, W.P.; Rowe, S.P.; Pomper, M.G.; Afshar-Oromieh, A.; Herrmann, K.; Eiber, M. PSMA Ligands for PET Imaging of Prostate Cancer. J. Nucl. Med. 2017, 58, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.J.; Maurer, T.; Perera, M.; Eiber, M.; Hope, T.A.; Ost, P.; Siva, S.; Hofman, M.S.; Murphy, D.G.; Emmett, L.; et al. Using PSMA imaging for prognostication in localized and advanced prostate cancer. Nat. Rev. Urol. 2023, 20, 23–47. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, S.; Williams, G.; Williams, E.; Ehrlich, K.; Stone, J.; Finlayson, N.; Bradley, M.; Thomson, R.R.; Akram, A.R.; Dhaliwal, K. Solitary pulmonary nodule imaging approaches and the role of optical fibre-based technologies. Eur. Respir. J. 2021, 57, 2002537. [Google Scholar] [CrossRef]
- Mauermann, J.; Fradet, V.; Lacombe, L.; Dujardin, T.; Tiguert, R.; Tetu, B.; Fradet, Y. The impact of solitary and multiple positive surgical margins on hard clinical end points in 1712 adjuvant treatment-naive pT2-4 N0 radical prostatectomy patients. Eur. Urol. 2013, 64, 19–25. [Google Scholar] [CrossRef]
- Boorjian, S.A.; Karnes, R.J.; Crispen, P.L.; Carlson, R.E.; Rangel, L.J.; Bergstralh, E.J.; Blute, M.L. The impact of positive surgical margins on mortality following radical prostatectomy during the prostate specific antigen era. J. Urol. 2010, 183, 1003–1009. [Google Scholar] [CrossRef]
- Novara, G.; Ficarra, V.; Mocellin, S.; Ahlering, T.E.; Carroll, P.R.; Graefen, M.; Guazzoni, G.; Menon, M.; Patel, V.R.; Shariat, S.F.; et al. Systematic review and meta-analysis of studies reporting oncologic outcome after robot-assisted radical prostatectomy. Eur. Urol. 2012, 62, 382–404. [Google Scholar] [CrossRef] [PubMed]
- Zorn, K.C.; Gallina, A.; Hutterer, G.C.; Walz, J.; Shalhav, A.L.; Zagaja, G.P.; Valiquette, L.; Gofrit, O.N.; Orvieto, M.A.; Taxy, J.B.; et al. External validation of a nomogram for prediction of side-specific extracapsular extension at robotic radical prostatectomy. J. Endourol. 2007, 21, 1345–1351. [Google Scholar] [CrossRef]
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef]
- Hofman, M.S.; Emmett, L.; Sandhu, S.; Iravani, A.; Joshua, A.M.; Goh, J.C.; Pattison, D.A.; Tan, T.H.; Kirkwood, I.D.; Ng, S.; et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomised, open-label, phase 2 trial. Lancet 2021, 397, 797–804. [Google Scholar] [CrossRef]
- Banerjee, S.R.; Pullambhatla, M.; Byun, Y.; Nimmagadda, S.; Foss, C.A.; Green, G.; Fox, J.J.; Lupold, S.E.; Mease, R.C.; Pomper, M.G. Sequential SPECT and optical imaging of experimental models of prostate cancer with a dual modality inhibitor of the prostate-specific membrane antigen. Angew. Chem. Int. Ed. Engl. 2011, 50, 9167–9170. [Google Scholar] [CrossRef]
- Schottelius, M.; Wurzer, A.; Wissmiller, K.; Beck, R.; Koch, M.; Gorpas, D.; Notni, J.; Buckle, T.; van Oosterom, M.N.; Steiger, K.; et al. Synthesis and Preclinical Characterization of the PSMA-Targeted Hybrid Tracer PSMA-I&F for Nuclear and Fluorescence Imaging of Prostate Cancer. J. Nucl. Med. 2019, 60, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Baranski, A.C.; Schafer, M.; Bauder-Wust, U.; Roscher, M.; Schmidt, J.; Stenau, E.; Simpfendorfer, T.; Teber, D.; Maier-Hein, L.; Hadaschik, B.; et al. PSMA-11-Derived Dual-Labeled PSMA Inhibitors for Preoperative PET Imaging and Precise Fluorescence-Guided Surgery of Prostate Cancer. J. Nucl. Med. 2018, 59, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Eder, A.C.; Schafer, M.; Schmidt, J.; Bauder-Wust, U.; Roscher, M.; Leotta, K.; Haberkorn, U.; Kopka, K.; Eder, M. Rational Linker Design to Accelerate Excretion and Reduce Background Uptake of Peptidomimetic PSMA-Targeting Hybrid Molecules. J. Nucl. Med. 2021, 62, 1461–1467. [Google Scholar] [CrossRef] [PubMed]
- Eder, A.C.; Omrane, M.A.; Stadlbauer, S.; Roscher, M.; Khoder, W.Y.; Gratzke, C.; Kopka, K.; Eder, M.; Meyer, P.T.; Jilg, C.A.; et al. The PSMA-11-derived hybrid molecule PSMA-914 specifically identifies prostate cancer by preoperative PET/CT and intraoperative fluorescence imaging. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2057–2058. [Google Scholar] [CrossRef]
- Lopez, A.; Zlatev, D.V.; Mach, K.E.; Bui, D.; Liu, J.J.; Rouse, R.V.; Harris, T.; Leppert, J.T.; Liao, J.C. Intraoperative Optical Biopsy during Robotic Assisted Radical Prostatectomy Using Confocal Endomicroscopy. J. Urol. 2016, 195 Pt 1, 1110–1117. [Google Scholar] [CrossRef]
- Wijmans, L.; Yared, J.; de Bruin, D.M.; Meijer, S.L.; Baas, P.; Bonta, P.I.; Annema, J.T. Needle-based confocal laser endomicroscopy for real-time diagnosing and staging of lung cancer. Eur. Respir. J. 2019, 53, 1801520. [Google Scholar] [CrossRef]
- Pierangelo, A.; Fuks, D.; Validire, P.; Benali, A.; Gayet, B. Diagnostic accuracy of confocal laser endomicroscopy for the characterization of liver nodules. Eur. J. Gastroenterol. Hepatol. 2017, 29, 42–47. [Google Scholar] [CrossRef]
- Kennedy, G.T.; Azari, F.S.; Bernstein, E.; Nadeem, B.; Chang, A.; Segil, A.; Carlin, S.; Sullivan, N.T.; Encarnado, E.; Desphande, C.; et al. Targeted detection of cancer at the cellular level during biopsy by near-infrared confocal laser endomicroscopy. Nat. Commun. 2022, 13, 2711. [Google Scholar] [CrossRef]
- Kennedy, G.T.; Azari, F.S.; Bernstein, E.; Nadeem, B.; Chang, A.; Segil, A.; Sullivan, N.; Encarnado, E.; Desphande, C.; Kucharczuk, J.C.; et al. Targeted detection of cancer cells during biopsy allows real-time diagnosis of pulmonary nodules. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 4194–4204. [Google Scholar] [CrossRef]
- Darr, C.; Costa, P.F.; Kahl, T.; Moraitis, A.; Engel, J.; Al-Nader, M.; Reis, H.; Kollermann, J.; Kesch, C.; Krafft, U.; et al. Intraoperative Molecular Positron Emission Tomography Imaging for Intraoperative Assessment of Radical Prostatectomy Specimens. Eur. Urol. Open Sci. 2023, 54, 28–32. [Google Scholar] [CrossRef]
- Schilham, M.G.M.; Somford, D.M.; Kusters-Vandevelde, H.V.N.; Hermsen, R.; van Basten, J.P.A.; Hoekstra, R.J.; Scheenen, T.W.J.; Gotthardt, M.; Sedelaar, J.P.M.; Rijpkema, M. Prostate-Specific Membrane Antigen-Targeted Radioguided Pelvic Lymph Node Dissection in Newly Diagnosed Prostate Cancer Patients with a Suspicion of Locoregional Lymph Node Metastases: The DETECT Trial. J. Nucl. Med. 2024, 65, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Berrens, A.C.; Scheltema, M.; Maurer, T.; Hermann, K.; Hamdy, F.C.; Knipper, S.; Dell’Oglio, P.; Mazzone, E.; de Barros, H.A.; Sorger, J.M.; et al. Delphi consensus project on prostate-specific membrane antigen (PSMA)-targeted surgery-outcomes from an international multidisciplinary panel. Eur. J. Nucl. Med. Mol. Imaging 2024, 51, 2893–2902. [Google Scholar] [CrossRef] [PubMed]
- Gorlitz, F.H.P.; Falk, H.J.; Kastrup, L.; Engelhardt, J.; Hell, S.W. A STED Microscope Designed for Routine Biomedical Applications. Prog. Electromagn. Res. 2014, 147, 57–68. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PSMA-914 [nM] | 0 | 10 | 30 | 60 | 100 | 250 | 500 | 1000 |
|---|---|---|---|---|---|---|---|---|
| LNCaP—AlveoFlexTM -C | 0.0 | 0.6 | 3.3 | 5.0 | 9.7 | 19.2 | 14.0 | 38.4 |
| LNCaP—CholangioFlexTM-C | 0.1 | 0.3 | 11.4 | 11.1 | 1.7 | 25.2 | 26.8 | 43.0 |
| LNCaP—GastroFlexTM UHD-C | 0.0 | 0.2 | 0.0 | 0.0 | 3.3 | 85.9 | 119.0 | 268.0 |
| PC-3—AlveoFlexTM -C | 0.0 | 0.1 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| PC-3—CholangioFlexTM-C | 0.0 | 0.1 | 0.1 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| PC-3—GastroFlexTM UHD-C | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eder, A.-C.; Matthias, J.; Lacombe, F.; Domogalla, L.-C.; Jacques, A.; Steinacker, N.; Christien, G.; Martin, E.; Criton, A.; Eder, M. Intraoperative Confocal Laser Endomicroscopy Detects Prostate Cancer at the Single-Cell Level with High Specificity and in Real Time: A Preclinical Proof of Concept. Pharmaceuticals 2025, 18, 841. https://doi.org/10.3390/ph18060841
Eder A-C, Matthias J, Lacombe F, Domogalla L-C, Jacques A, Steinacker N, Christien G, Martin E, Criton A, Eder M. Intraoperative Confocal Laser Endomicroscopy Detects Prostate Cancer at the Single-Cell Level with High Specificity and in Real Time: A Preclinical Proof of Concept. Pharmaceuticals. 2025; 18(6):841. https://doi.org/10.3390/ph18060841
Chicago/Turabian StyleEder, Ann-Christin, Jessica Matthias, Francois Lacombe, Lisa-Charlotte Domogalla, Antoine Jacques, Nils Steinacker, Gaetan Christien, Elodie Martin, Aline Criton, and Matthias Eder. 2025. "Intraoperative Confocal Laser Endomicroscopy Detects Prostate Cancer at the Single-Cell Level with High Specificity and in Real Time: A Preclinical Proof of Concept" Pharmaceuticals 18, no. 6: 841. https://doi.org/10.3390/ph18060841
APA StyleEder, A.-C., Matthias, J., Lacombe, F., Domogalla, L.-C., Jacques, A., Steinacker, N., Christien, G., Martin, E., Criton, A., & Eder, M. (2025). Intraoperative Confocal Laser Endomicroscopy Detects Prostate Cancer at the Single-Cell Level with High Specificity and in Real Time: A Preclinical Proof of Concept. Pharmaceuticals, 18(6), 841. https://doi.org/10.3390/ph18060841