
Safety and Efficacy of Reduced Dose of Enzalutamide in Patients with Castration-Resistant Prostate Cancer: A Systematic Review

 , , , , , , , and
, , , , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Methods
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Analysis of Results
3. Results
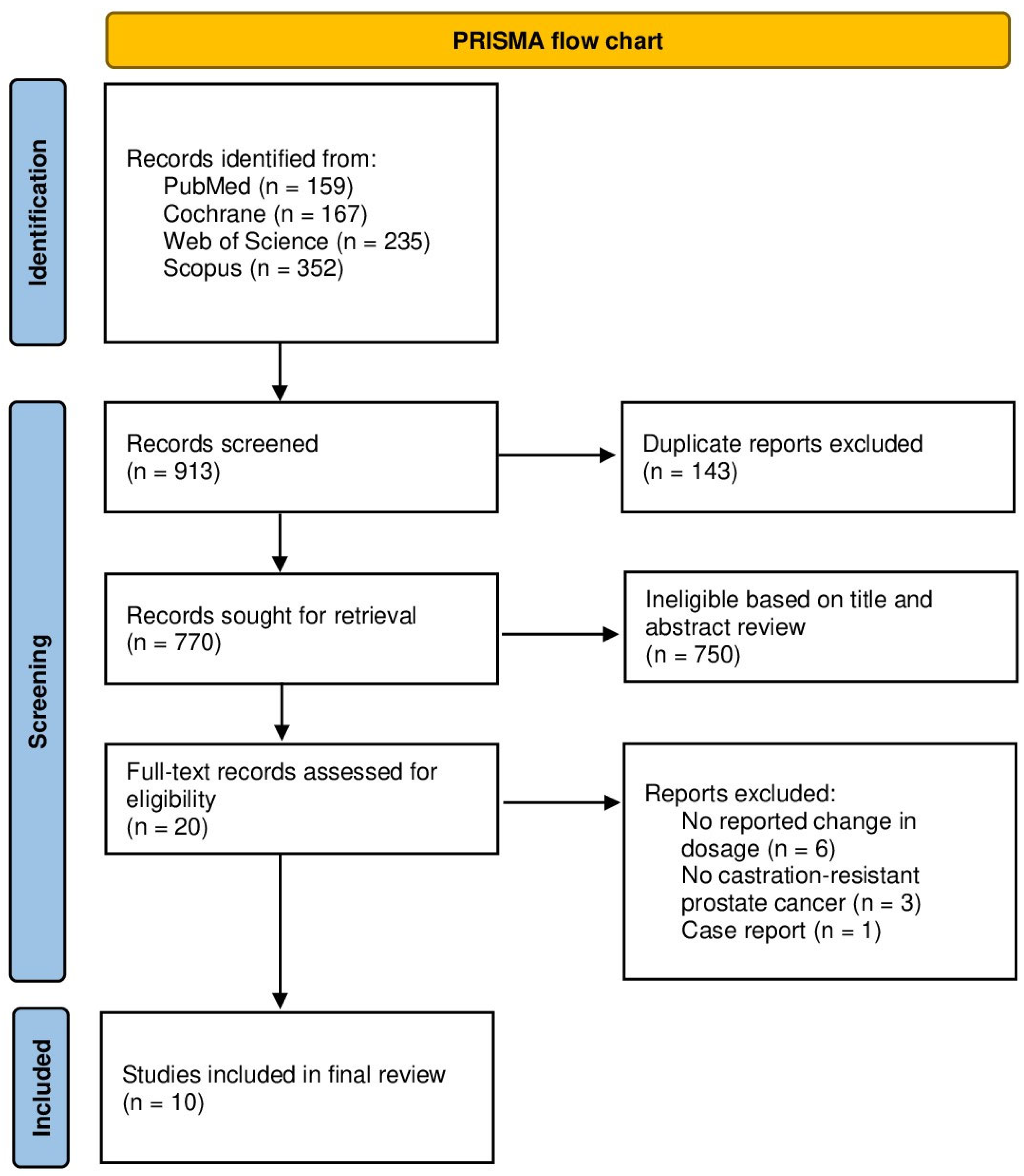
3.1. Evidence Synthesis
3.2. Characteristics of the Included Studies
3.3. Progression-Free Survival (PFS) and Overall Survival (OS)

{kind=link}
| Study | Country | Study Design | Dose | Age (in Years) | Population | No. of Patients |
|---|---|---|---|---|---|---|
| Scher et al., 2010 [10] | USA | Phase I–II study trial | Enzalutamide 30–600 mg | 68 (44–93) | mCRPC | 140 |
| Terada et al., 2016 [30] | Japan | Retrospective multi-institutional cohort study | Enzalutamide standard doses of 160 mg/day and lower doses (80–120 mg/day) | 69 (46–90) | CRPC | 345 Standard dose: 266 Reduced dose: 79 |
| Hori et al., 2020 [29] | Japan | Real-world cohort of Japanese patients with CRPC | Enzalutamide 160 mg/day vs. 80, 120 mg/day | 79 (69–91) | CRPC | 13 Standard dose: 4 Reduced dose: 9 |
| Vinh-Hung et al., 2020 [27] | France (Martinique) | Retrospective cohort | Enzalutamide 160 mg/day vs. ≤80 mg/day | Standard dose: 80.1 (74.7–90.3) Reduced dose: 84.3 (74.9–93.8) | mCRPC | 59 Standard dose: 43 Reduced dose: 16 |
| Miura et al., 2021 [8] | Japan | Retrospective cohort | Enzalutamide standard dose (started at 160 mg) or dose-escalation (started at 80 mg, followed by dose escalation) | Standard dose: 70.5 (63−84) Reduced dose: 78 (64−93) | CRPC | 107 Standard dose: 17 Dose-escalation: 90 |
| Freedland et al., 2021 [26] | USA | Retrospective longitudinal cohort study of US Veterans Health Administration data | Enzalutamide reduced dose <80% | 74.5 | mCRPC | 1375 |
| Tsuzuki et al., 2021 [18] | Japan | Retrospective cohort | Enzalutamide 160 mg/day vs. 40–120 mg/day | Standard dose: 76 (69–80) Reduced dose: 81 (76–84) (median, IQR) | CRPC | 233 Standard dose: 190 Reduced dose: 43 |
| Vinh-Hung et al., 2022 [28] | France (Martinique) | Retrospective cohort | Enzalutamide 160 mg/day vs. ≤80 mg/day | Standard dose: 76.5 (52.6–90.3) Reduced dose: 81.9 (58.4–93.8) | mCRPC | 111 Standard dose: 79 Reduced dose: 32 |
| Yamada et al., 2022 [25] | Japan | Retrospective cohort | Enzalutamide 160 mg/day or dose reduction from 30 to 150 mg | 75 (70–82) (median, IQR) | CRPC | 105 Standard dose: 77 Reduced dose: 28 |
| Boerrigter et al., 2024 [20] | The Netherlands | Multicentric open-label, randomized clinical trial | Enzalutamide 160 mg/day vs. 120 mg/day | Standard dose: 80 (68–88) Reduced dose: 80 (69–90) | mCRPC (48) mHSPC (4) | 52 Standard dose: 27 Reduced dose: 25 |
| Study | Summary of Methods | Efficacy Findings | Toxicity Findings |
|---|---|---|---|
| Scher et al., 2010 [10] | Phase I–II trial evaluating doses between 30 and 600 mg/day to determine maximum tolerated dose and antitumor effects. | PSA reduction ≥50% in 56% of patients. Median time to radiological progression: 47 weeks. | Grade 3–4 fatigue: 11% (dose-dependent). Resolved after dose reduction. |
| Terada et al., 2016 [30] | Retrospective cohort study comparing patients on standard dose (160 mg/day) vs. reduced dose (<160 mg/day). | PSA reduction ≥50% in 57% of patients. Median PSA progression-free survival: 163 days. | AEs (fatigue, appetite loss): 49%. Discontinuation due to AEs: 18%. Older age and lower doses are associated with fewer AEs. |
| Hori et al., 2020 [29] | Real-world study comparing efficacy and safety in CRPC patients on doses ranging from 80 to 160 mg/day. | PSA decrement ≥50% in 92% of patients. | AEs were mild (>20%). No significant safety concerns in Japanese CRPC patients. |
| Vinh-Hung et al., 2020 [27] | Retrospective study comparing patients on standard dose (160 mg/day) and low dose (<80 mg/day). | PSA reduction ≥50% in 67% (low dose) vs. 45% (standard dose). Median PFS: 11.2 months (low dose) vs. 11.9 months (standard dose). | Low-dose is associated with reduced toxicity in elderly, poor-performance patients. |
| Miura et al., 2021 [8] | Patients were divided into standard-dose (160 mg/day) and dose-escalation (80 mg/day, gradually increasing to 160 mg/day) groups. | Median TTF: 10.4 months (standard dose) vs. 18.0 months (dose escalation). | Grade ≥3 AEs: 23.5% (standard dose) vs. 6.7% (dose escalation). AEs (any grade): 88.2% (standard dose) vs. 63.3%. Discontinuation due to AEs: 35.3% (standard dose) vs. 12.2%. |
| Tsuzuki et al., 2021 [18] | Retrospective analysis comparing standard dose (160 mg/day) and reduced dose (40–120 mg/day) in CRPC patients. | PSA response rate: −66.3% (reduced dose) vs. −87.4% (standard dose). | AE incidence: 22.6% (reduced dose) vs. 34.4% (standard dose). No significant difference. |
| Freedland et al., 2021 [26] | Large retrospective analysis using US Veterans Health Administration data to assess the impact of relative dose intensity on outcomes. | Dose reductions (RDI <80%) are associated with an 8.8% higher risk of PSA progression. | Dose reductions increased PSA progression risk. Patient adherence is recommended. |
| Vinh-Hung et al., 2022 [28] | Subgroup analysis of patients receiving standard (160 mg/day) vs. low-dose (<80 mg/day) therapy. | OS and PFS did not differ between low and standard doses. The low dose showed better longevity (5.3 years). | Low dose is associated with fewer AEs, particularly in patients with comorbidities and poor performance. |
| Yamada et al., 2022 [25] | Retrospective study comparing outcomes in patients on standard (160 mg/day) vs. reduced dose (<160 mg/day). | Median PFS: 12.1 months (standard dose) vs. 7.2 months (reduced dose). Reduced doses showed inferior oncological outcomes. | Dose reduction increased the risk of disease progression but did not affect OS. |
| Boerrigter et al., 2024 [20] | Prospective trial comparing reduced dose (120 mg/day) and standard dose (160 mg/day) in prostate cancer patients. | Reduced dose maintained efficacy. No significant interference with efficacy endpoints. | The reduced dose is associated with less fatigue, cognitive, and depressive symptoms. The standard dose showed worsening side effects over 24 weeks. |
3.4. Toxicity and Treatment Adherence
3.5. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADT | Androgen deprivation therapy |
| AEs | Adverse events |
| AR | Androgen receptor |
| ARPI | Androgen receptor pathway inhibitor |
| CI | Confidence Interval |
| CRPC | Castration-resistant prostate cancer |
| CV | Cardiovascular |
| HSPC | Hormone-sensitive prostate cancer |
| HR | Hazard ratio |
| IQR | Interquartile range |
| MFS | Metastasis-free survival |
| NOS | Newcastle–Ottawa Scale |
| OS | Overall survival |
| PFS | Progression-free survival |
| PRISMA | Preferred Reporting Items for Systematic reviews and Meta-Analyses |
| PSA | Prostate-specific antigen |
| RoB | Risk of bias |
| RoB2 | Risk of bias 2 tool |
| RCT | Randomized controlled trial |
| ENZA | Enzalutamide |
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef]
- Shore, N.D.; Moul, J.W.; Pienta, K.J.; Czernin, J.; King, M.T.; Freedland, S.J. Biochemical recurrence in patients with prostate cancer after primary definitive therapy: Treatment based on risk stratification. Prostate Cancer Prostatic Dis. 2024, 27, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Artibani, W.; Porcaro, A.B.; De Marco, V.; Cerruto, M.A.; Siracusano, S. Management of Biochemical Recurrence after Primary Curative Treatment for Prostate Cancer: A Review. Urol. Int. 2017, 100, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Helgstrand, J.T.; Røder, M.A.; Klemann, N.; Toft, B.G.; Lichtensztajn, D.Y.; Brooks, J.D.; Brasso, K.; Vainer, B.; Iversen, P. Trends in incidence and 5-year mortality in men with newly diagnosed, metastatic prostate cancer—A population-based analysis of 2 national cohorts. Cancer 2018, 124, 2931–2938. [Google Scholar] [CrossRef] [PubMed]
- Posdzich, P.; Darr, C.; Hilser, T.; Wahl, M.; Herrmann, K.; Hadaschik, B.; Grünwald, V. Metastatic Prostate Cancer-A Review of Current Treatment Options and Promising New Approaches. Cancers 2023, 15, 461. [Google Scholar] [CrossRef]
- Tilki, D.; Schaeffer, E.M.; Evans, C.P. Understanding Mechanisms of Resistance in Metastatic Castration-resistant Prostate Cancer: The Role of the Androgen Receptor. Eur. Urol. Focus 2016, 2, 499–505. [Google Scholar] [CrossRef]
- Komura, K.; Sweeney, C.J.; Inamoto, T.; Ibuki, N.; Azuma, H.; Kantoff, P.W. Current treatment strategies for advanced prostate cancer. Int. J. Urol. 2018, 25, 220–231. [Google Scholar] [CrossRef]
- Miura, R.; Hirabatake, M.; Irie, K.; Ikesue, H.; Muroi, N.; Kawakita, M.; Hashida, T. Safety evaluation of enzalutamide dose-escalation strategy in patients with castration-resistant prostate cancer. Urol. Oncol. 2021, 39, 233.e15–233.e20. [Google Scholar] [CrossRef]
- Zhang, D.; Weng, H.; Zhu, Z.; Gong, W.; Ma, Y. Evaluating first-line therapeutic strategies for metastatic castration-resistant prostate cancer: A comprehensive network meta-analysis and systematic review. Front. Oncol. 2024, 14, 1378993. [Google Scholar] [CrossRef]
- Scher, H.I.; Beer, T.M.; Higano, C.S.; Anand, A.; Taplin, M.E.; Efstathiou, E.; Rathkopf, D.; Shelkey, J.; Yu, E.Y.; Alumkal, J.; et al. Antitumour activity of MDV3100 in castration-resistant prostate cancer: A phase 1-2 study. Lancet 2010, 375, 1437–1446. [Google Scholar] [CrossRef]
- Beer, T.M.; Armstrong, A.J.; Rathkopf, D.; Loriot, Y.; Sternberg, C.N.; Higano, C.S.; Iversen, P.; Evans, C.P.; Kim, C.-S.; Kimura, G.; et al. Enzalutamide in Men with Chemotherapy-naïve Metastatic Castration-resistant Prostate Cancer: Extended Analysis of the Phase 3 PREVAIL Study. Eur. Urol. 2017, 71, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Scher, H.I.; Fizazi, K.; Saad, F.; Taplin, M.-E.; Sternberg, C.N.; Miller, K.; De Wit, R.; Mulders, P.; Chi, K.N.; Shore, N.D.; et al. Increased Survival with Enzalutamide in Prostate Cancer after Chemotherapy. New Engl. J. Med. 2012, 367, 1187–1197. [Google Scholar] [CrossRef] [PubMed]
- Sternberg, C.N.; Fizazi, K.; Saad, F.; Shore, N.D.; Giorgi, U.D.; Penson, D.F.; Ferreira, U.; Efstathiou, E.; Madziarska, K.; Kolinsky, M.P.; et al. Enzalutamide and Survival in Nonmetastatic, Castration-Resistant Prostate Cancer. New Engl. J. Med. 2020, 382, 2197–2206. [Google Scholar] [CrossRef] [PubMed]
- Penson, D.F.; Armstrong, A.J.; Concepcion, R.; Agarwal, N.; Olsson, C.; Karsh, L.; Dunshee, C.; Wang, F.; Wu, K.; Krivoshik, A.; et al. Enzalutamide Versus Bicalutamide in Castration-Resistant Prostate Cancer: The STRIVE Trial. J. Clin. Oncol. 2016, 34, 2098–2106. [Google Scholar] [CrossRef]
- Shore, N.D.; Chowdhury, S.; Villers, A.; Klotz, L.; Siemens, D.R.; Phung, D.; van Os, S.; Hasabou, N.; Wang, F.; Bhattacharya, S.; et al. Efficacy and safety of enzalutamide versus bicalutamide for patients with metastatic prostate cancer (TERRAIN): A randomised, double-blind, phase 2 study. Lancet Oncol. 2016, 17, 153–163. [Google Scholar] [CrossRef]
- Freedland, S.J.; de Almeida Luz, M.; De Giorgi, U.; Gleave, M.; Gotto, G.T.; Pieczonka, C.M.; Haas, G.P.; Kim, C.-S.; Ramirez-Backhaus, M.; Rannikko, A.; et al. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. New Engl. J. Med. 2023, 389, 1453–1465. [Google Scholar] [CrossRef]
- Beer, T.M.; Armstrong, A.J.; Rathkopf, D.E.; Loriot, Y.; Sternberg, C.N.; Higano, C.S.; Iversen, P.; Bhattacharya, S.; Carles, J.; Chowdhury, S.; et al. Enzalutamide in Metastatic Prostate Cancer before Chemotherapy. New Engl. J. Med. 2014, 371, 424–433. [Google Scholar] [CrossRef]
- Tsuzuki, S.; Nakanishi, S.; Tamaki, M.; Oshiro, T.; Miki, J.; Yamada, H.; Shimomura, T.; Kimura, T.; Furuta, N.; Saito, S.; et al. Initial dose reduction of enzalutamide does not decrease the incidence of adverse events in castration-resistant prostate cancer. PLoS ONE 2021, 16, e0258160. [Google Scholar] [CrossRef]
- Joshua, A.M.; Shore, N.D.; Saad, F.; Chi, K.N.; Olsson, C.A.; Emmenegger, U.; Scholz, M.; Berry, W.; Mukherjee, S.D.; Winquist, E.; et al. Safety of enzalutamide in patients with metastatic castration-resistant prostate cancer previously treated with docetaxel: Expanded access in North America. Prostate 2015, 75, 836–844. [Google Scholar] [CrossRef]
- Boerrigter, E.; Overbeek, J.K.; Benoist, G.E.; Somford, D.M.; Hamberg, P.; Tol, J.; Scholtes, B.; Willemsen, A.E.; Buffart, L.M.; Kessels, R.P.; et al. A Prospective Randomised Trial to Determine the Effect of a Reduced Versus Standard Dose of Enzalutamide on Side Effects in Frail Patients with Prostate Cancer. Eur. Urol. Oncol. 2024, 7, 1376–1383. [Google Scholar] [CrossRef]
- Higgins, J.P.T.T.J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; Version 6.4 (Updated August 2023); Cochrane: Oxford, UK, 2023. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’Connell, J. The Newcastle-Ottawa Scale (NOS) for Assessing The Quality of Nonrandomised Studies in Meta-analyses; Ottawa Health Research Institute Website: Ottawa, ON, Canada, 2014; p. 7. [Google Scholar]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Yamada, S.; Shiota, M.; Blas, L.; Matsumoto, T.; Kashiwagi, E.; Takeuchi, A.; Inokuchi, J.; Shiga, K.-I.; Yokomizo, A.; Eto, M. Prognostic impact of dose reduction in androgen receptor pathway inhibitors for castration-resistant prostate cancer. Prostate Int. 2022, 10, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Freedland, S.J.; Li, S.; Pilon, D.; Bhak, R.H.; Narkhede, S.; Lefebvre, P.; Young-Xu, Y. Medication patterns of abiraterone acetate plus prednisone or enzalutamide and PSA progression in veterans with metastatic castration-resistant prostate cancer. Curr. Med. Res. Opin. 2021, 37, 635–642. [Google Scholar] [CrossRef]
- Vinh-Hung, V.; Natchagande, G.; Joachim, C.; Gorobets, O.; Drame, M.; Bougas, S.; Folefac, E.; Nguyen, N.P.; Verschraegen, C.; Yin, M. Low-Dose Enzalutamide in Late-Elderly Patients (≥75 Years Old) Presenting With Metastatic Castration-Resistant Prostate Cancer. Clin. Genitourin. Cancer 2020, 18, e660–e668. [Google Scholar] [CrossRef]
- Vinh-Hung, V.; Gorobets, O.; Natchagande, G.; Sargos, P.; Yin, M.; Nguyen, N.P.; Verschraegen, C.; Folefac, E. Low-Dose Enzalutamide in Metastatic Prostate Cancer-Longevity Over Conventional Survival Analysis. Clin. Genitourin. Cancer 2022, 20, e473–e484. [Google Scholar] [CrossRef]
- Hori, A.; Sahashi, H.; Sano, S.; Matsumiya, E.; Ariga, M.; Asano, A.; Soda, M.; Goto, C.; Mizui, T.; Komeda, H.; et al. Efficacy and Safety of Enzalutamide in a Real-World Cohort of Japanese Patients with Castration-resistant Prostate Cancer. Anticancer. Res. 2020, 40, 7101–7108. [Google Scholar] [CrossRef]
- Terada, N.; Akamatsu, S.; Okada, Y.; Negoro, H.; Kobayashi, T.; Yamasaki, T.; Matsui, Y.; Inoue, T.; Kamba, T.; Ogawa, O. Factors predicting efficacy and adverse effects of enzalutamide in Japanese patients with castration-resistant prostate cancer: Results of retrospective multi-institutional study. Int. J. Clin. Oncol. 2016, 21, 1155–1161. [Google Scholar] [CrossRef]
- Shelan, M.; Achard, V.; Appiagyei, F.; Mose, L.; Zilli, T.; Fankhauser, C.D.; Zamboglou, C.; Mohamad, O.; Aebersold, D.M.; Cathomas, R. Role of enzalutamide in primary and recurrent non-metastatic hormone sensitive prostate cancer: A systematic review of prospective clinical trials. Prostate Cancer Prostatic Dis. 2024, 27, 422–431. [Google Scholar] [CrossRef]
- Iguchi, T.; Kato, M.; Hirayama, Y.; Yamasaki, T.; Yasuda, S.; Morita, N.; Chikazawa, I.; Fukushima, W.; Tamada, S.; Miyazawa, K. A study of the association between enzalutamide blood concentrations and adverse events in patients with castration-resistant prostate cancer. J. Clin. Oncol. 2024, 42 (Suppl. 4), 102. [Google Scholar] [CrossRef]
- Szmulewitz, R.Z.; Peer, C.J.; Ibraheem, A.; Martinez, E.; Kozloff, M.F.; Carthon, B.; Harvey, R.D.; Fishkin, P.; Yong, W.P.; Chiong, E.; et al. Prospective International Randomized Phase II Study of Low-Dose Abiraterone With Food Versus Standard Dose Abiraterone In Castration-Resistant Prostate Cancer. J. Clin. Oncol. 2018, 36, 1389–1395. [Google Scholar] [CrossRef]
- Do, T.A.; Tran, P.M.; Vu, T.H.; Tran, H.K.; Nguyen, H.Q.; Nguyen, L.D.; Nguyen, H.T.; Van Nguyen, C. Real-world Efficacy and Safety of Low-Dose Abiraterone With Food and Standard-Dose Abiraterone in De Novo Metastatic Hormone-Sensitive Prostate Cancer: A Retrospective Analysis. Clin. Genitourin. Cancer 2024, 22, 102191. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belabaci, Z.; Mose, L.; El-Taji, O.; Otmani, Z.; Hannouneh, Z.A.; Mohamad, I.; Zilli, T.; Mohamad, O.; Pervez, N.; Arafat, W.; et al. Safety and Efficacy of Reduced Dose of Enzalutamide in Patients with Castration-Resistant Prostate Cancer: A Systematic Review. Pharmaceuticals 2025, 18, 732. https://doi.org/10.3390/ph18050732
Belabaci Z, Mose L, El-Taji O, Otmani Z, Hannouneh ZA, Mohamad I, Zilli T, Mohamad O, Pervez N, Arafat W, et al. Safety and Efficacy of Reduced Dose of Enzalutamide in Patients with Castration-Resistant Prostate Cancer: A Systematic Review. Pharmaceuticals. 2025; 18(5):732. https://doi.org/10.3390/ph18050732
Chicago/Turabian StyleBelabaci, Zineddine, Lucas Mose, Omar El-Taji, Zina Otmani, Zein Alabdin Hannouneh, Issa Mohamad, Thomas Zilli, Osama Mohamad, Nadeem Pervez, Waleed Arafat, and et al. 2025. "Safety and Efficacy of Reduced Dose of Enzalutamide in Patients with Castration-Resistant Prostate Cancer: A Systematic Review" Pharmaceuticals 18, no. 5: 732. https://doi.org/10.3390/ph18050732
APA StyleBelabaci, Z., Mose, L., El-Taji, O., Otmani, Z., Hannouneh, Z. A., Mohamad, I., Zilli, T., Mohamad, O., Pervez, N., Arafat, W., Vogl, U., & Shelan, M. (2025). Safety and Efficacy of Reduced Dose of Enzalutamide in Patients with Castration-Resistant Prostate Cancer: A Systematic Review. Pharmaceuticals, 18(5), 732. https://doi.org/10.3390/ph18050732