


Comprehensive Analysis of Characteristics of Cuproptosis-Related LncRNAs Associated with Prognosis of Lung Adenocarcinoma and Tumor Immune Microenvironment

Abstract
1. Introduction
2. Results
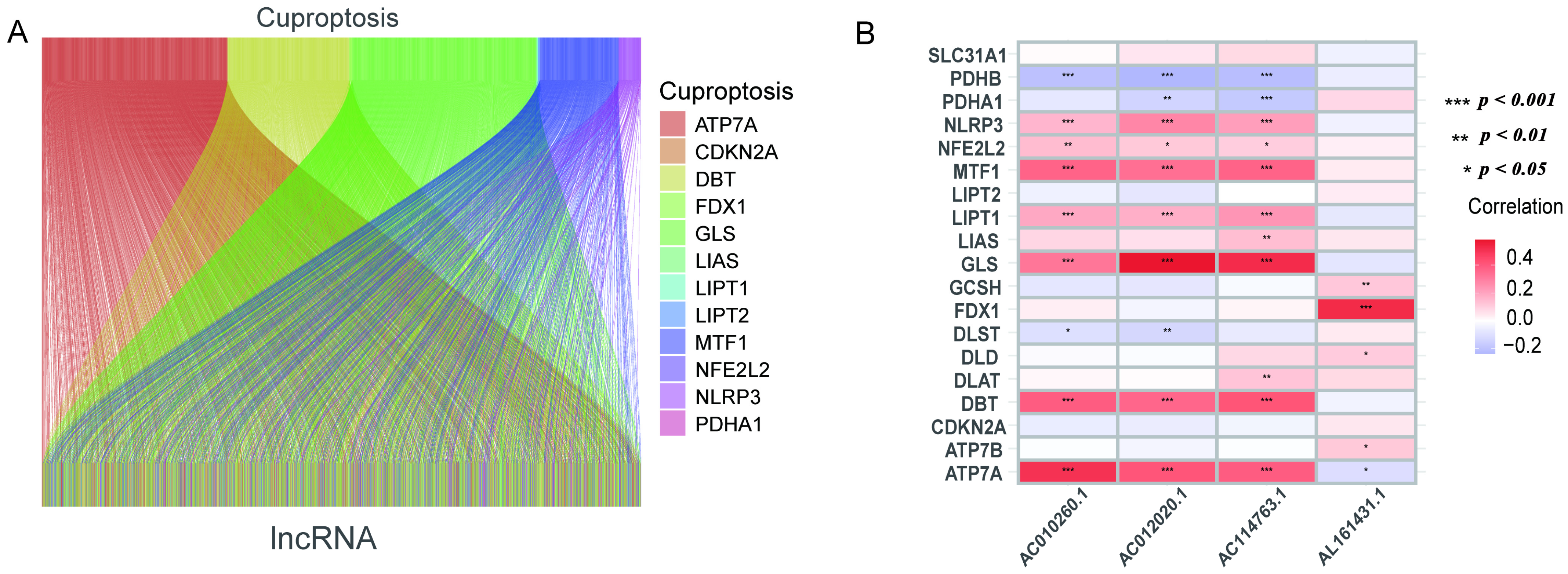
2.1. Data Processing
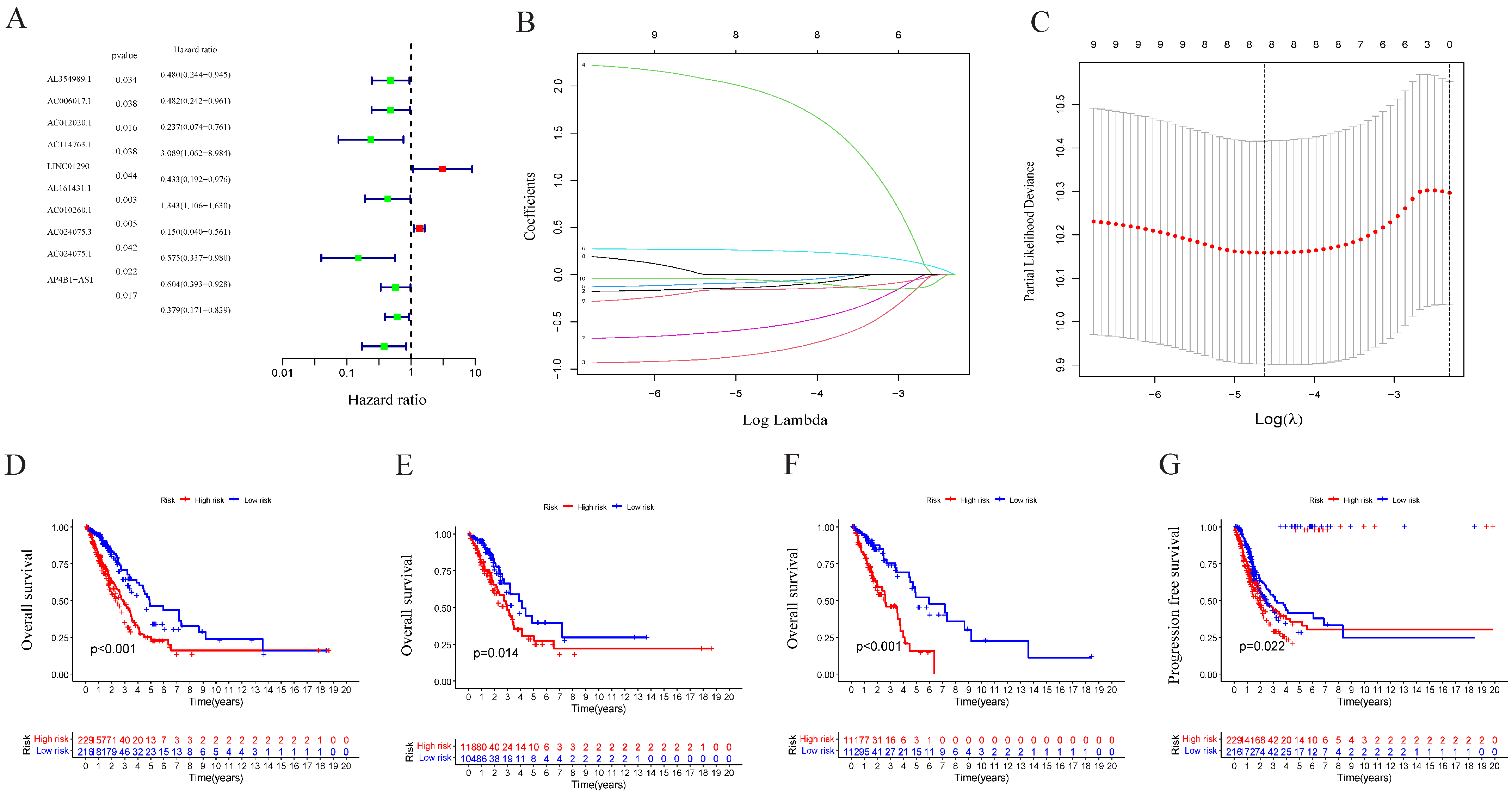
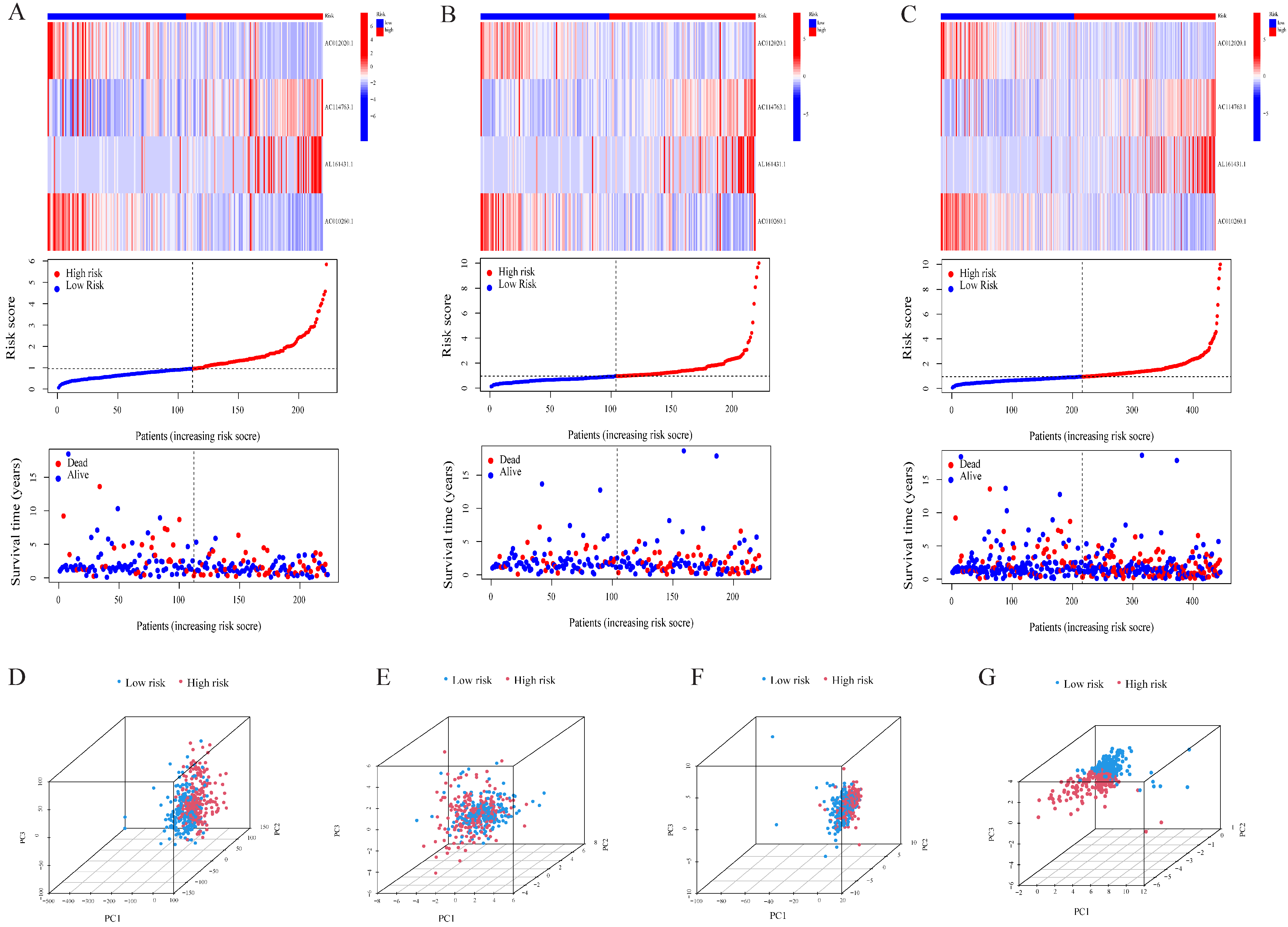
2.2. Construction and Validation of Prognostic Markers of Cuproptosis-Related LncRNA
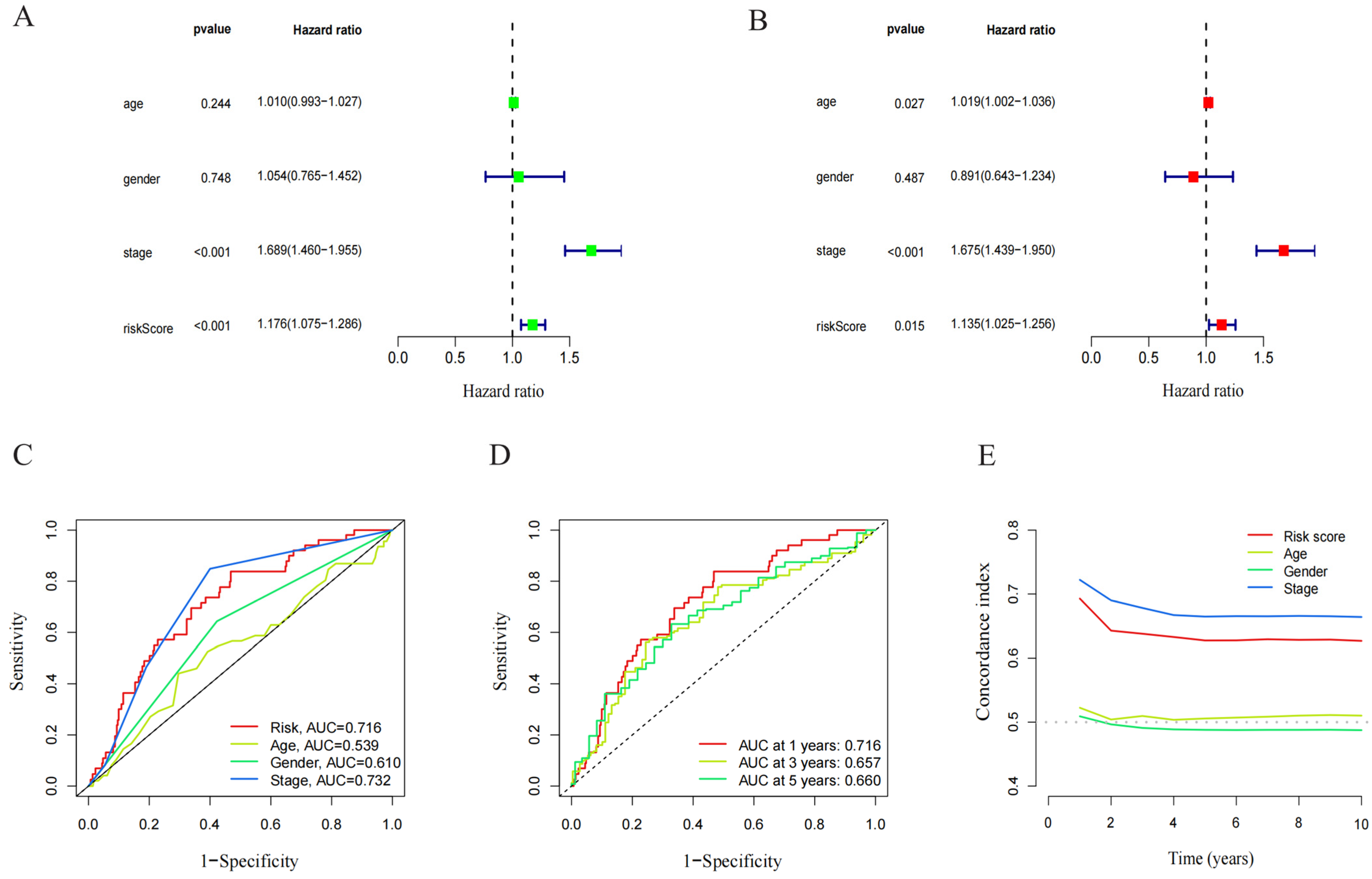
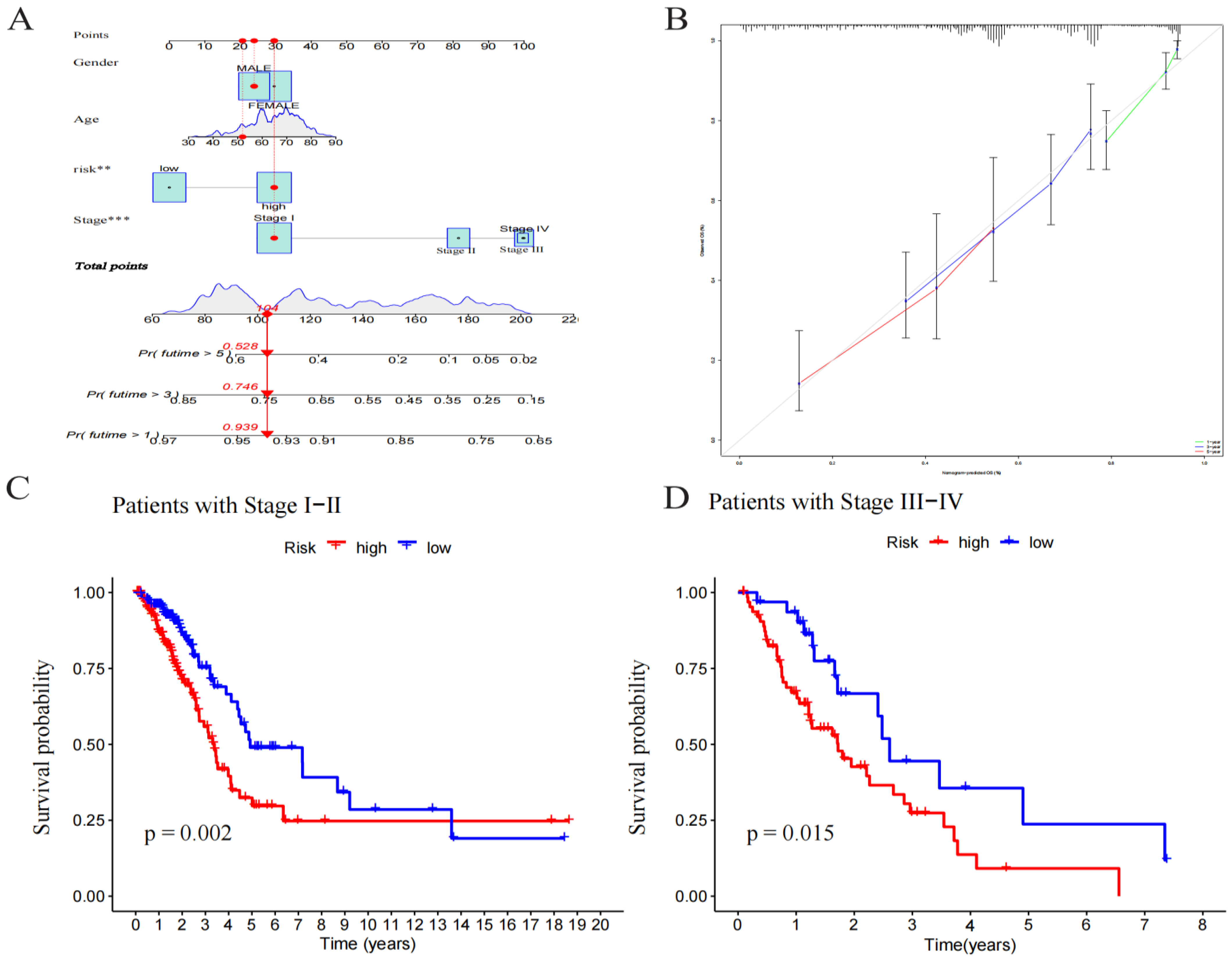
2.3. Independence of Prognostic Markers of Cuproptosis-Related LncRNAs in Predicting Overall Survival
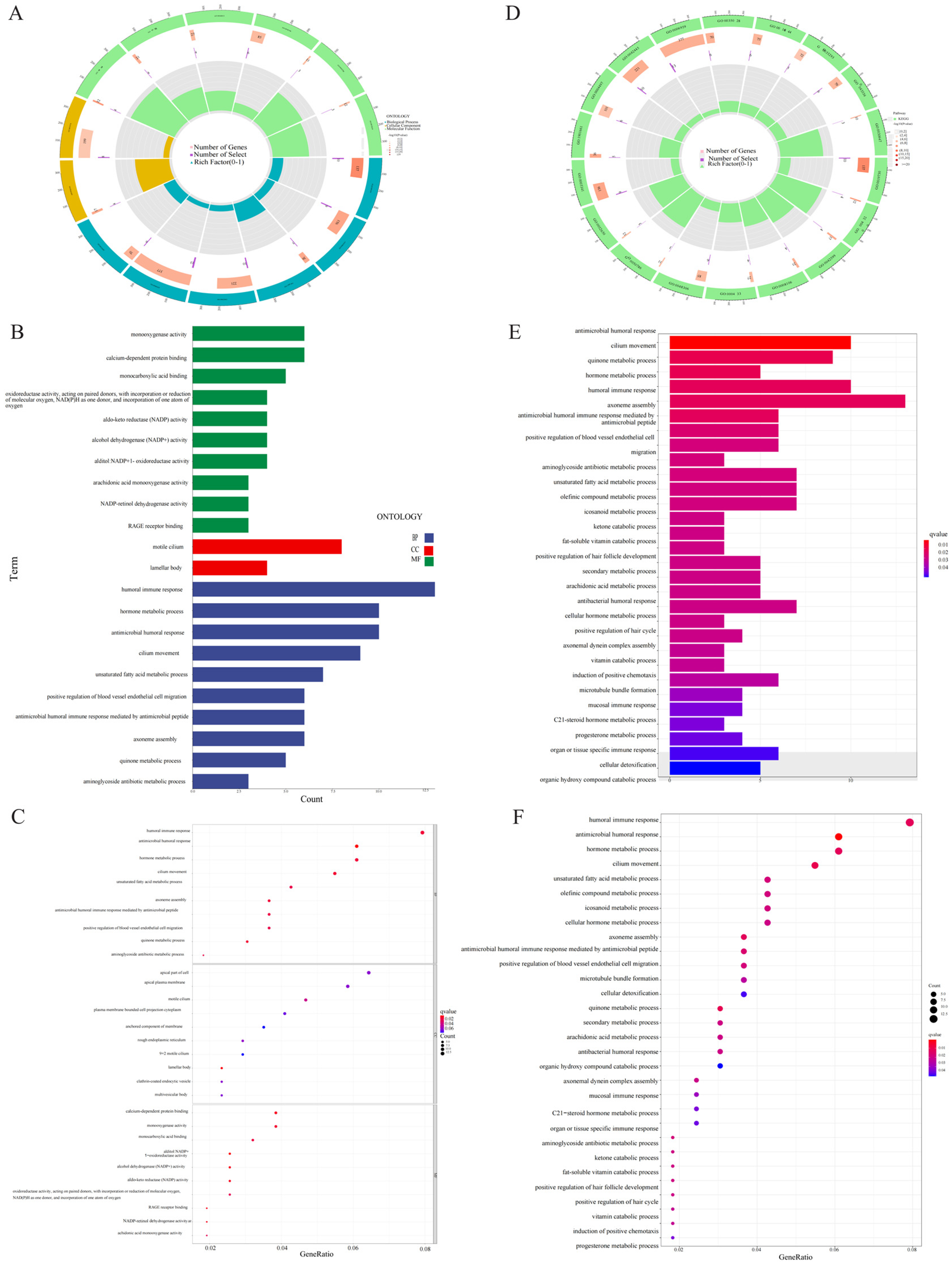
2.4. Pathway and Gene Enrichment Analyses
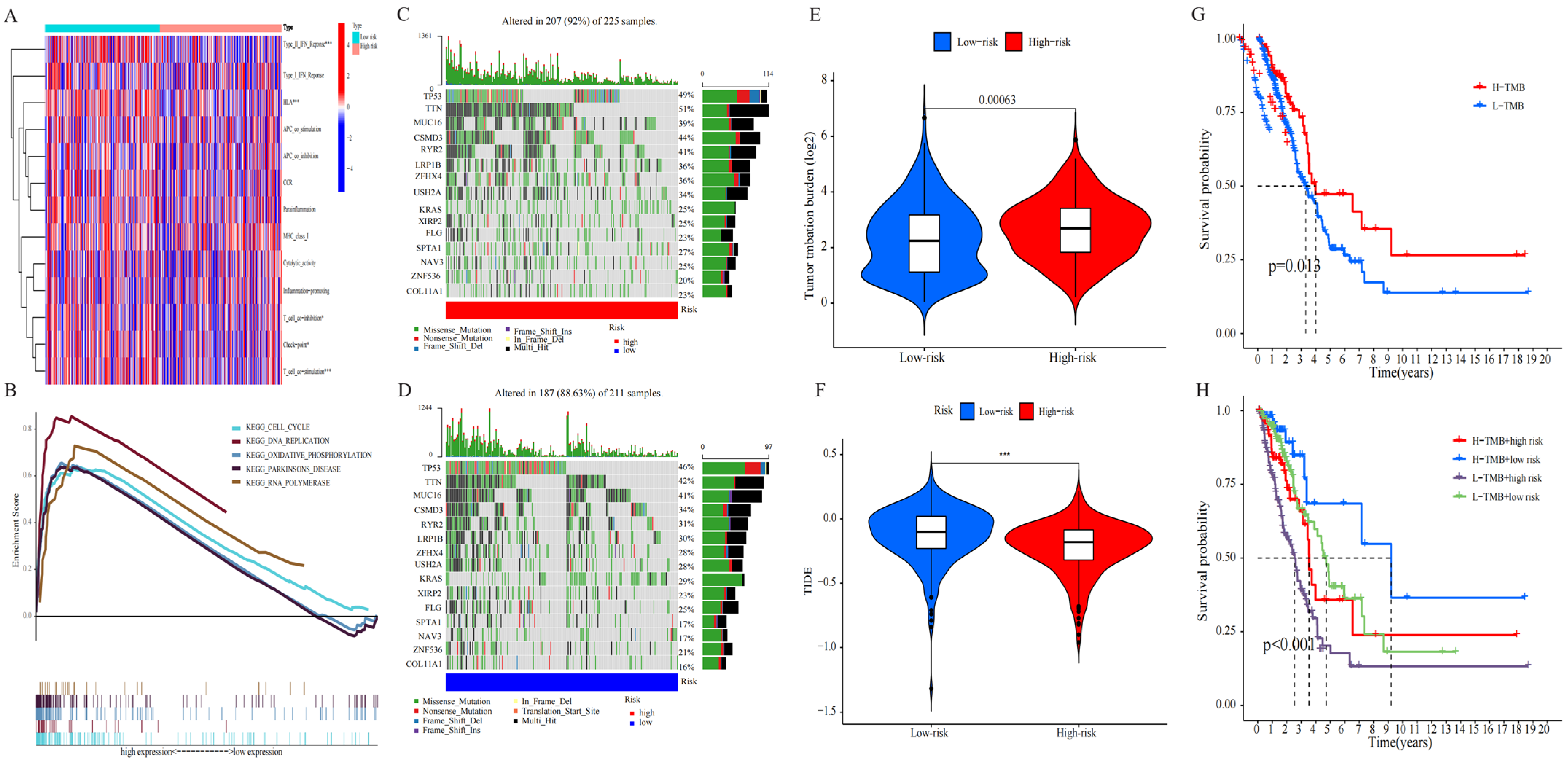
2.5. Estimation of Immune Cell Infiltration and Immunotherapy in Tumors
2.6. Analysis of TMB
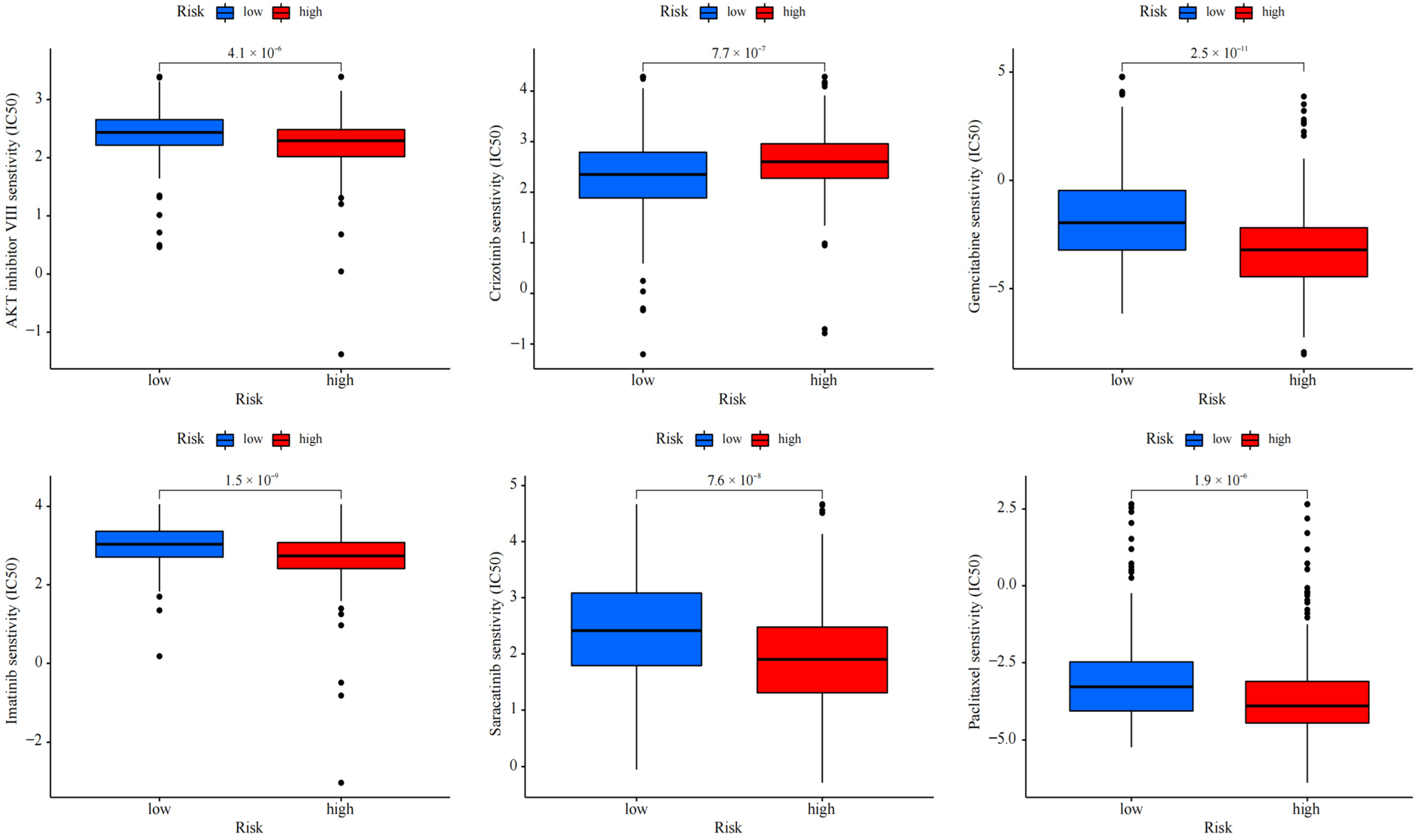
2.7. Drug Sensitivity Analysis
3. Discussion
4. Materials and Methods
4.1. Downloading and Processing of Transcriptome and Mutation Data in Clinic
4.2. Production and Evaluation of LncRNA Associated with Cuproptosis
4.3. Construction of Prediction Model
4.4. Verification of RS Model
4.5. Establishment and Evaluation of Nomograms
4.6. Exploring the Relationship between Prognosis RS and Clinical Stages
4.7. GO and KEGG Enrichment Analysis
4.8. Determination of Immune Cell Infiltration and Immunotherapy in Tumors
4.9. Drug Sensitivity Evaluation
4.10. Calculation of Tumor Mutational Burden Score
4.11. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsvetkov, P.; Coy, S.; Petrova, B.; Dreishpoon, M.; Verma, A.; Abdusamad, M. Copper Induces Cell Death by Targeting Lipoylated TCA Cycle Proteins. Science 2020, 375, 1254–1261. [Google Scholar] [CrossRef]
- Engreitz, J.M.; Haines, J.E.; Perez, E.M.; Munson, G.; Chen, J.; Kane, M. Local Regulation of Gene Expression by lncRNA Promoters, Transcription and Splicing. Nature 2016, 539, 452–455. [Google Scholar] [CrossRef] [PubMed]
- Bridges, M.C.; Daulagala, A.C.; Kourtidis, A. LNCcation: LncRNA Localization and Function. J. Cell Biol. 2021, 220, e202009045. [Google Scholar] [CrossRef] [PubMed]
- Huarte, M. The Emerging Role of lncRNAs in Cancer. Nat. Med. 2015, 21, 1253–1261. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.J.; Wang, X.; Song, Y.X.; Zhao, J.H.; Sun, J.X.; Shi, J.X. Circulating Noncoding RNAs Have a Promising Future Acting as Novel Biomarkers for Colorectal Cancer. Dis. Markers 2019, 2019, 2587109. [Google Scholar] [CrossRef]
- Gu, Z.R.; Liu, W. The LncRNA AL161431.1 Targets miR-1252-5p and Facilitates Cellular Proliferation and Migration via MAPK Signaling in Endometrial Carcinoma. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 2294–2302. [Google Scholar] [CrossRef]
- Song, J.Y.; Li, X.P.; Qin, X.J.; Zhang, J.D.; Zhao, J.Y.; Wang, R. A fourteen-lncRNA Risk Score System for Prognostic Prediction of Patients with Non-small Cell Lung Cancer. Cancer Biomark. 2020, 29, 493–508. [Google Scholar] [CrossRef]
- Xie, G.; Zhu, Y.; Lin, Z.; Sun, Y.; Gu, G.; Wang, W. HOPMCLDA: Predicting lncRNA-disease Associations Based on High-order Proximity and Matrix Completion. Mol. Omics 2021, 17, 760–768. [Google Scholar] [CrossRef]
- Hu, Q.; Wang, R.; Ma, H.; Zhang, Z.; Xue, Q. Cuproptosis Predicts the Risk and Clinical Outcomes of Lung Adenocarcinoma. Front. Oncol. 2022, 12, 922332. [Google Scholar] [CrossRef]
- Talotta, R.; Bahrami, S.; Laska, M.J. Sequence Complementarity Between Human Noncoding RNAs and SARS-CoV-2 genes: What Are the Implications for Human Health? Biochim. Biophys. Acta Mol. Basis Dis. 2022, 1868, 166291. [Google Scholar] [CrossRef]
- Zhang, M.; Shi, M.; Zhao, Y. Association Between Serum Copper Levels and Cervical Cancer Risk: A Meta-analysis. Biosci. Rep. 2018, 38, BSR20180161. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Zeng, J.W.; Ma, Q.; Zhang, S.; Tang, J.; Feng, J.F. Serum Copper and Zinc Levels in Breast Cancer: A Meta-analysis. J. Trace Elem. Med. Biol. 2020, 62, 126629. [Google Scholar] [CrossRef] [PubMed]
- Lai, D.; Tan, L.; Zuo, X.; Liu, D.; Jiao, D.; Wan, G. Prognostic Ferroptosis-Related lncRNA Signatures Associated with Immunotherapy and Chemotherapy Responses in Patients With Stomach Cancer. Front. Genet. 2021, 12, 798612. [Google Scholar] [CrossRef]
- Espuela-Ortiz, A.; Herrera-Luis, E.; Lorenzo-Diaz, F.; Hu, D.; Eng, C.; Villar, J. Role of Sex on the Genetic Susceptibility to Childhood Asthma in Latinos and African Americans. J. Pers. Med. 2021, 11, 1140. [Google Scholar] [CrossRef]
- Ju, Q.; Zhao, Y.J.; Ma, S.; Li, X.M.; Zhang, H.; Zhang, S.Q. Genome-wide Analysis of Prognostic-related LncRNAs, miRNAs and mRNAs Forming a Competing Endogenous RNA Network in Lung Squamous Cell Carcinoma. J. Cancer Res. Clin. Oncol. 2020, 146, 1711–1723. [Google Scholar] [CrossRef]
- Shao, J.; Zhang, B.; Kuai, L.; Li, Q. Integrated Analysis of Hypoxia-associated lncRNA Signature to Predict Prognosis and Immune Microenvironment of Lung Adenocarcinoma Patients. Bioengineered 2021, 12, 6186–6200. [Google Scholar] [CrossRef]
- Zhao, J.; Lin, X.; Zhuang, J.; He, F. Relationships of N6-Methyladenosine-Related Long Non-Coding RNAs With Tumor Immune Microenvironment and Clinical Prognosis in Lung Adenocarcinoma. Front. Genet. 2021, 12, 714697. [Google Scholar] [CrossRef]
- Zou, X.; He, R.; Zhang, Z.; Yan, Y. Apoptosis-Related Signature Predicts Prognosis and Immune Microenvironment Infiltration in Lung Adenocarcinoma. Front. Genet. 2022, 13, 818403. [Google Scholar] [CrossRef]
- Li, Y. Copper Homeostasis: Emerging Target for Cancer Treatment. IUBMB Life 2020, 72, 1900–1908. [Google Scholar] [CrossRef]
- Nagai, M.; Vo, N.H.; Shin Ogawa, L.; Chimmanamada, D.; Inoue, T.; Chu, J. The Oncology Drug Elesclomol Selectively Transports Copper to the Mitochondria to Induce Oxidative Stress in Cancer Cells. Free Radic. Biol. Med. 2012, 52, 2142–2150. [Google Scholar] [CrossRef]
- Rowland, E.A.; Snowden, C.K.; Cristea, I.M. Protein Lipoylation: An Evolutionarily Conserved Metabolic Regulator of Health and Disease. Curr. Opin. Chem. Biol. 2018, 42, 76–85. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total | Validation Set | Training Set | p-Value |
|---|---|---|---|---|
| Age | ||||
| ≤65 | 217 (48.76%) | 105 (47.3%) | 112 (50.22%) | 0.6011 |
| >65 | 228 (51.24%) | 117 (52.7%) | 111 (49.78%) | |
| gender | ||||
| FEMALE | 244 (54.83%) | 121 (54.5%) | 123 (55.16%) | 0.9657 |
| MALE | 201 (45.17%) | 101 (45.5%) | 100 (44.84%) | |
| stage | ||||
| Stage I | 238 (53.48%) | 125 (56.31%) | 113 (50.67%) | 0.3349 |
| Stage II | 102 (22.92%) | 51 (22.97%) | 51 (22.87%) | |
| Stage III | 73 (16.4%) | 35 (15.77%) | 38 (17.04%) | |
| Stage IV | 24 (5.39%) | 8 (3.6%) | 16 (7.17%) | |
| unknown | 8 (1.8%) | 3 (1.35%) | 5 (2.24%) | |
| T stage | ||||
| T1 | 152 (34.16%) | 80 (36.04%) | 72 (32.29%) | 0.8565 |
| T2 | 235 (52.81%) | 115 (51.8%) | 120 (53.81%) | |
| T3 | 37 (8.31%) | 17 (7.66%) | 20 (8.97%) | |
| T4 | 18 (4.04%) | 9 (4.05%) | 9 (4.04%) | |
| unknown | 3 (0.67%) | 1 (0.45%) | 2 (0.9%) | |
| M stage | ||||
| M0 | 296 (66.52%) | 155 (69.82%) | 141 (63.23%) | 0.0703 |
| M1 | 23 (5.17%) | 7 (3.15%) | 16 (7.17%) | |
| unknown | 126 (28.31%) | 60 (27.03%) | 66 (29.6%) | |
| N stage | ||||
| N0 | 286 (64.27%) | 145 (65.32%) | 141 (63.23%) | 0.9773 |
| N1 | 83 (18.65%) | 42 (18.92%) | 41 (18.39%) | |
| N2 | 63 (14.16%) | 30 (13.51%) | 33 (14.8%) | |
| N3 | 2 (0.45%) | 1 (0.45%) | 1 (0.45%) | |
| unknown | 11 (2.47%) | 4 (1.8%) | 7 (3.14%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, F.; Wen, X.; Wu, J.; Feng, M.; Feng, S. Comprehensive Analysis of Characteristics of Cuproptosis-Related LncRNAs Associated with Prognosis of Lung Adenocarcinoma and Tumor Immune Microenvironment. Pharmaceuticals 2024, 17, 1244. https://doi.org/10.3390/ph17091244
Chen F, Wen X, Wu J, Feng M, Feng S. Comprehensive Analysis of Characteristics of Cuproptosis-Related LncRNAs Associated with Prognosis of Lung Adenocarcinoma and Tumor Immune Microenvironment. Pharmaceuticals. 2024; 17(9):1244. https://doi.org/10.3390/ph17091244
Chicago/Turabian StyleChen, Feihong, Xin Wen, Jiani Wu, Min Feng, and Shicheng Feng. 2024. "Comprehensive Analysis of Characteristics of Cuproptosis-Related LncRNAs Associated with Prognosis of Lung Adenocarcinoma and Tumor Immune Microenvironment" Pharmaceuticals 17, no. 9: 1244. https://doi.org/10.3390/ph17091244
APA StyleChen, F., Wen, X., Wu, J., Feng, M., & Feng, S. (2024). Comprehensive Analysis of Characteristics of Cuproptosis-Related LncRNAs Associated with Prognosis of Lung Adenocarcinoma and Tumor Immune Microenvironment. Pharmaceuticals, 17(9), 1244. https://doi.org/10.3390/ph17091244