

Patient-Centric Design of Topical Dermatological Medicines



Abstract
1. Introduction
2. Vehicles/Bases Used in Topical Dermatological Treatments
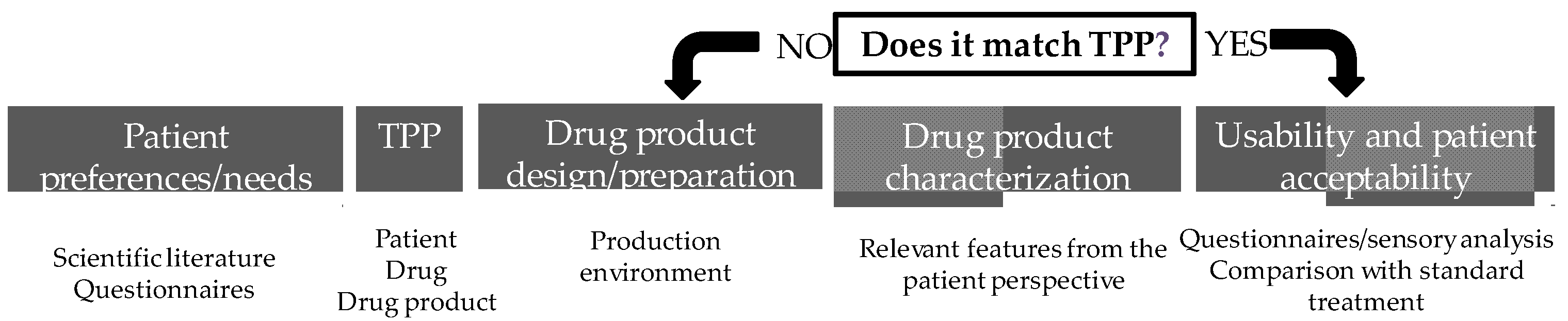
3. Patient-Centric Topical-Medicine Design
3.1. Patient Preferences and Needs Regarding Topical Medicines
3.1.1. Patient- and Disease-Related Needs in Dermatology
3.1.2. Patient Preferences for Topical Medicines
3.2. Target Product Profile (TPP)
3.2.1. Packaging
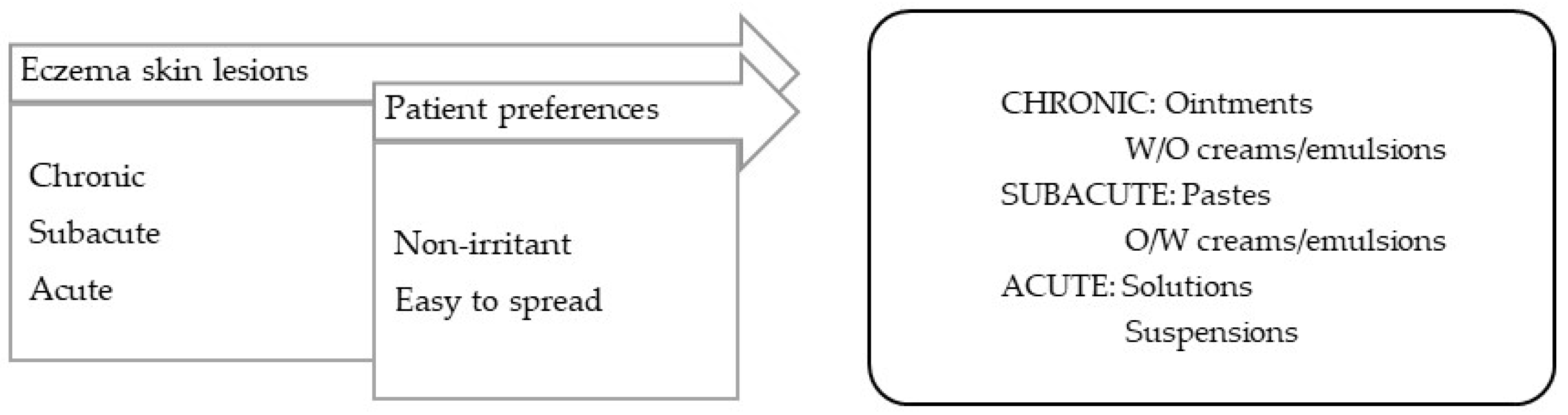
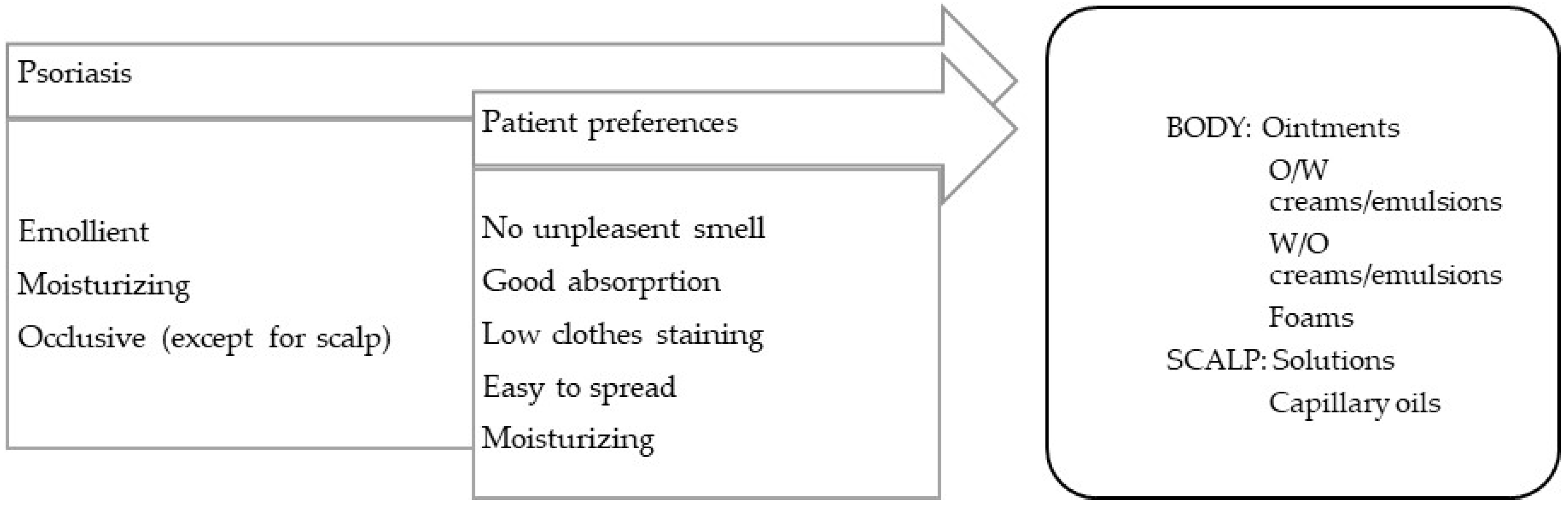
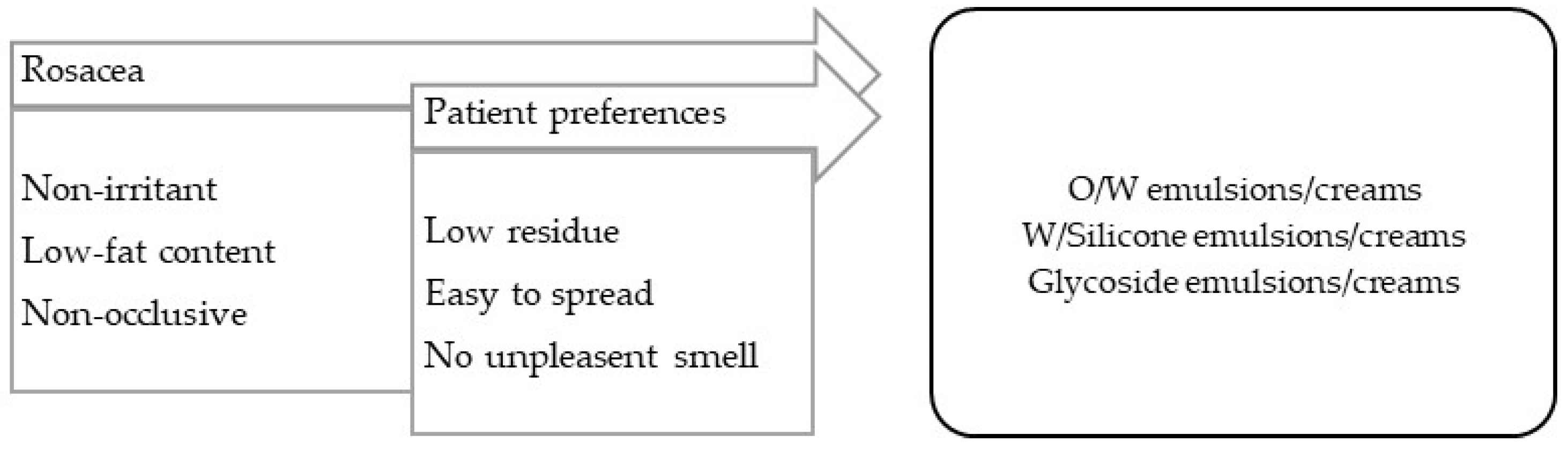
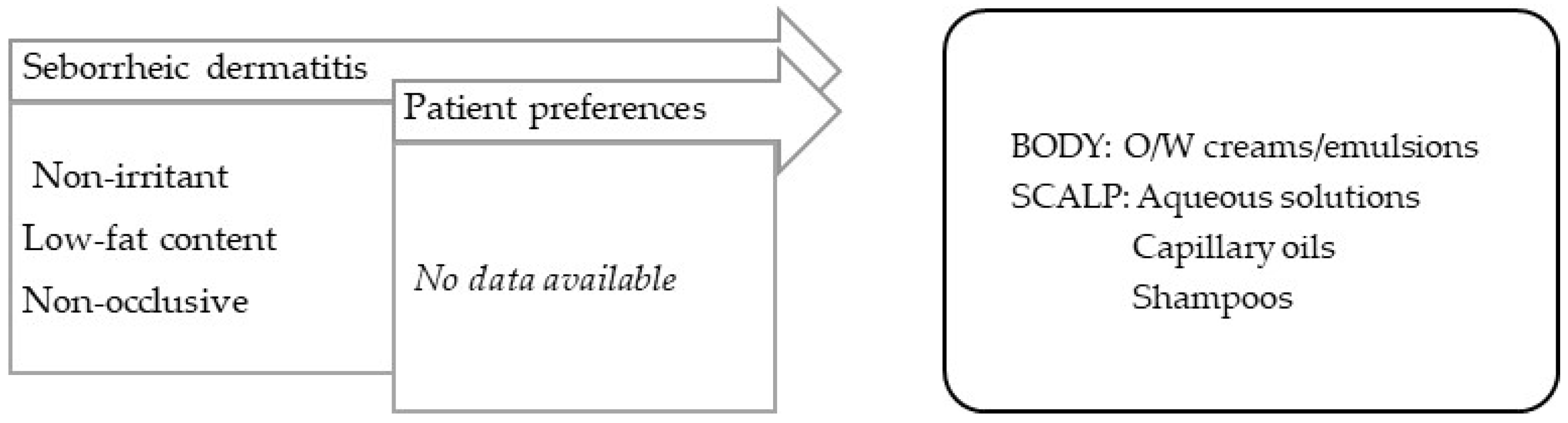
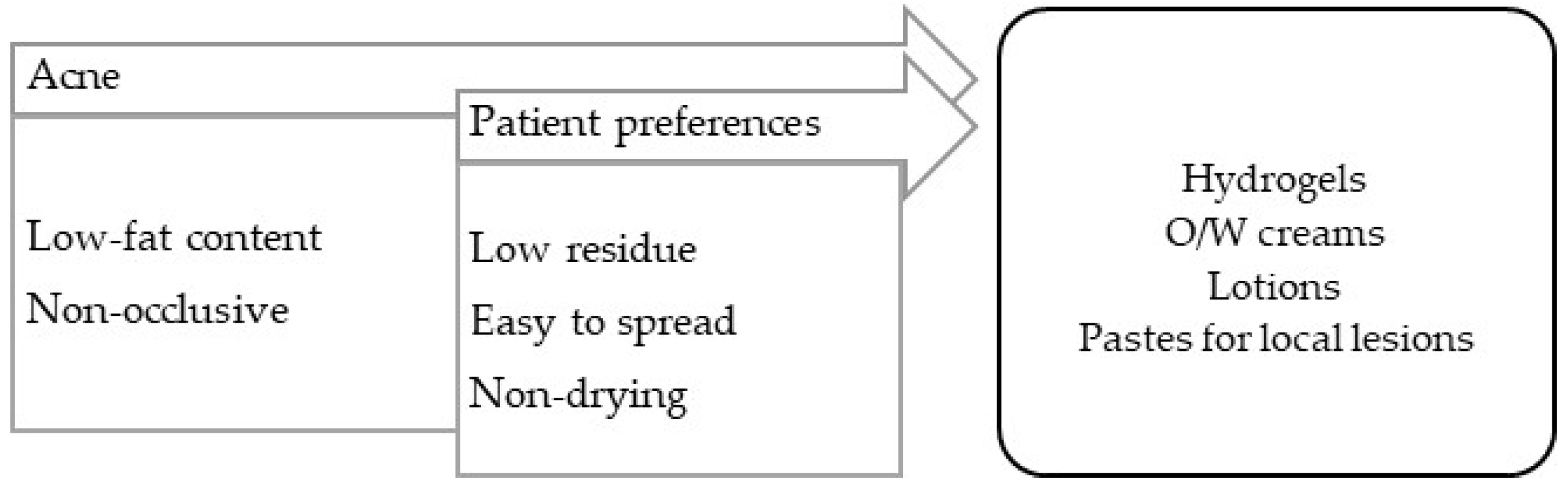
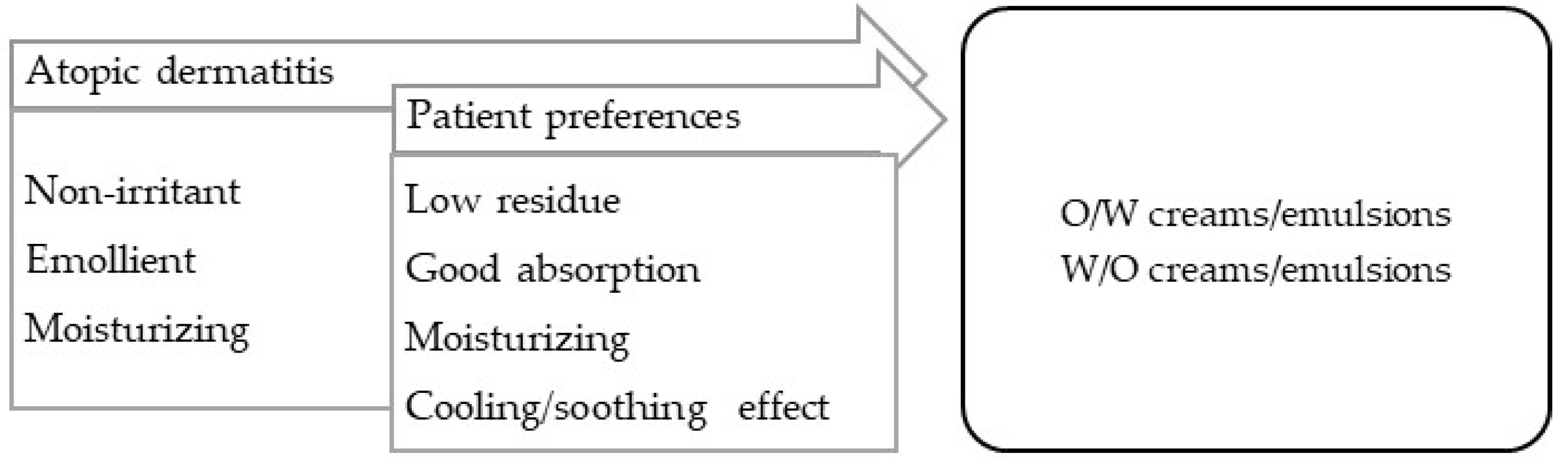
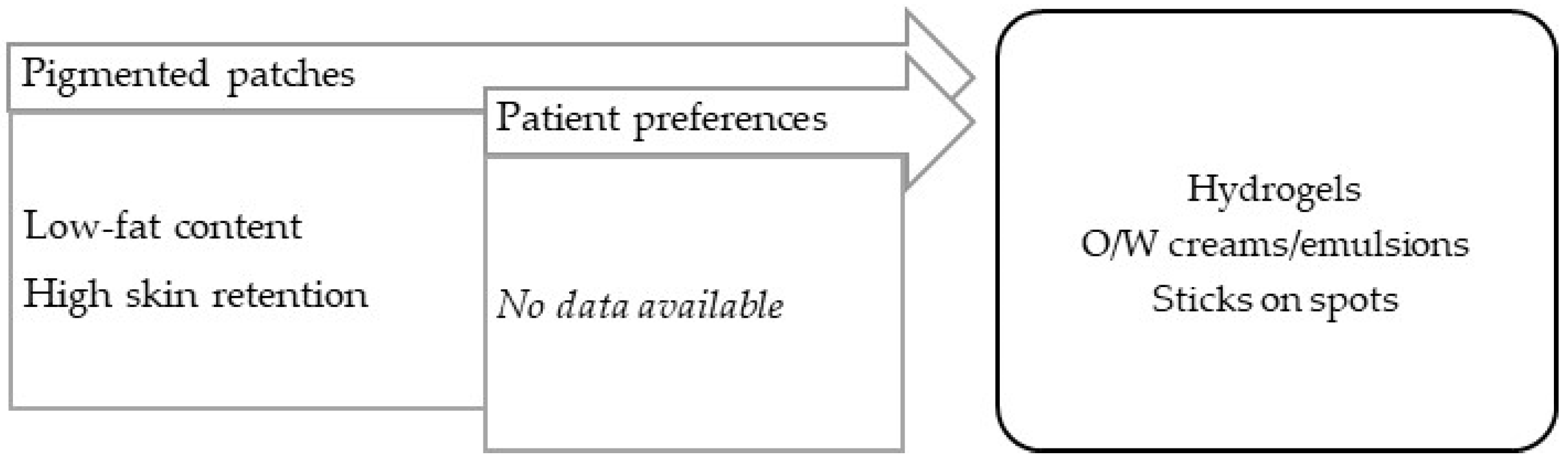
3.2.2. Target Product Profile for Selected Skin Disorders
- Scaly and xerotic disorders.
- 2.
- Long-term inflammatory disorders.
- 3.
- Seborrheic disorders.
- 4.
- Pruritic disorders.
- 5.
- Pigmentation disorders.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ana Teixeira, M.T.; Almeida, V.; Almeida, I.F. Adherence to Topical Treatment in Psoriasis. In Adherence to Medical Plans for Active and Healthy Ageing; Costa, E., Giardini, A., Monaco, A., Eds.; Nova Science Publishers, Incorporated: New York, NY, USA, 2017. [Google Scholar]
- Augustin, M.; Holland, B.; Dartsch, D.; Langenbruch, A.; Radtke, M.A. Adherence in the treatment of psoriasis: A systematic review. Dermatology 2011, 222, 363–374. [Google Scholar] [CrossRef]
- Miyachi, Y.; Hayashi, N.; Furukawa, F.; Akamatsu, H.; Matsunaga, K.; Watanabe, S.; Kawashima, M. Acne management in Japan: Study of patient adherence. Dermatology 2011, 223, 174–181. [Google Scholar] [CrossRef]
- Snyder, A.; Farhangian, M.; Feldman, S.R. A review of patient adherence to topical therapies for treatment of atopic dermatitis. Cutis 2015, 96, 397–401. [Google Scholar]
- Teixeira, A.; Oliveira, C.; Teixeira, M.; Rita Gaio, A.; Lobo, J.M.S.; de Almeida, I.F.M.; Almeida, V. Development and Validation of a Novel Questionnaire for Adherence with Topical Treatments in Psoriasis (QATOP). Am. J. Clin. Dermatol. 2017, 18, 571–581. [Google Scholar] [CrossRef]
- Tveit, K.S.; Duvetorp, A.; Østergaard, M.; Skov, L.; Danielsen, K.; Iversen, L.; Seifert, O. Treatment use and satisfaction among patients with psoriasis and psoriatic arthritis: Results from the NORdic PAtient survey of Psoriasis and Psoriatic arthritis (NORPAPP). J. Eur. Acad. Dermatol. Venereol. 2019, 33, 340–354. [Google Scholar] [CrossRef]
- Schaarschmidt, M.L.; Umar, N.; Schmieder, A.; Terris, D.D.; Goebeler, M.; Goerdt, S.; Peitsch, W.K. Patient preferences for psoriasis treatments: Impact of treatment experience. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 187–198. [Google Scholar] [CrossRef]
- Fouéré, S.; Adjadj, L.; Pawin, H. How patients experience psoriasis: Results from a European survey. J. Eur. Acad. Dermatol. Venereol. 2005, 19 (Suppl. S3), 2–6. [Google Scholar] [CrossRef]
- Brown, K.K.; Rehmus, W.E.; Kimball, A.B. Determining the relative importance of patient motivations for nonadherence to topical corticosteroid therapy in psoriasis. J. Am. Acad. Dermatol. 2006, 55, 607–613. [Google Scholar] [CrossRef]
- Teixeira, A.; Teixeira, M.; Almeida, V.; Gaio, R.; Torres, T.; Magina, S.; Cunha, C.; Sousa Lobo, J.M.; Almeida, I.F. Does the Vehicle Matter? Real-World Evidence on Adherence to Topical Treatment in Psoriasis. Pharmaceutics 2021, 13, 1539. [Google Scholar] [CrossRef]
- Puig, L.; Carrascosa, J.M.; Belinchón, I.; Fernández-Redondo, V.; Carretero, G.; Ruiz-Carrascosa, J.C.; Careaga, J.M.; de la Cueva, P.; Gárate, M.T.; Ribera, M. Adherence and Patient Satisfaction With Topical Treatment in Psoriasis, and the Use, and Organoleptic Properties of Such Treatments: A Delphi Study With an Expert Panel and Members of the Psoriasis Group of the Spanish Academy of Dermatology and Venereology. Actas Dermo-Sifiliográficas 2013, 104, 488–496. [Google Scholar] [CrossRef]
- Iversen, L.; Jakobsen, H.B. Patient Preferences for Topical Psoriasis Treatments are Diverse and Difficult to Predict. Dermatol. Ther. 2016, 6, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Council of Europe. European Pharmacopoeia, 10th Edition 2020; Directorate for the Quality of Medicines and HealthCare of the Council of Europe (EDQM): Strasbourg, France, 2019. [Google Scholar]
- Teixeira, A.; Vasconcelos, V.; Teixeira, M.; Almeida, V.; Azevedo, R.; Torres, T.; Sousa Lobo, J.M.; Costa, P.C.; Almeida, I.F. Mechanical Properties of Topical Anti-Psoriatic Medicines: Implications for Patient Satisfaction with Treatment. AAPS PharmSciTech 2019, 20, 36. [Google Scholar] [CrossRef] [PubMed]
- Encyclopedia of Pharmaceutical Technology, 3rd ed.; Swarbrick, J., Ed.; CRC Press: Boca Raton, FL, USA, 2007. [Google Scholar]
- Taylor, K.M.G.; Aulton, M.E. Aulton’s Pharmaceutics: The Design and Manufacture of Medicines, 6th ed.; Taylor, K.M.G., Aulton, M.E., Eds.; Elsevier: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Lukic, M.; Pantelic, I.; Savic, S. An Overview of Novel Surfactants for Formulation of Cosmetics with Certain Emphasis on Acidic Active Substances. Tenside Surfactants Deterg. 2016, 53, 7–19. [Google Scholar] [CrossRef]
- Pal, A.; Mondal, M.H.; Adhikari, A.; Bhattarai, A.; Saha, B. Scientific information about sugar-based emulsifiers: A comprehensive review. RSC Adv. 2021, 11, 33004–33016. [Google Scholar] [CrossRef]
- Ajazuddin; Alexander, A.; Khichariya, A.; Gupta, S.; Patel, R.J.; Giri, T.K.; Tripathi, D.K. Recent expansions in an emergent novel drug delivery technology: Emulgel. J. Control. Release 2013, 171, 122–132. [Google Scholar] [CrossRef]
- Somasundaran, P.; Mehta, S.C.; Purohit, P. Silicone emulsions. Adv. Colloid Interface Sci. 2006, 128–130, 103–109. [Google Scholar] [CrossRef]
- Mancuso, A.; Tarsitano, M.; Udongo, B.P.; Cristiano, M.C.; Torella, D.; Paolino, D.; Fresta, M. A comparison between silicone-free and silicone-based emulsions: Technological features and in vivo evaluation. Int. J. Cosmet. Sci. 2022, 44, 514–529. [Google Scholar] [CrossRef]
- Ohsedo, Y. N-Alkylhydantoins as New Organogelators and Their Ability to Create Thixotropic Mixed Molecular Organogels. Gels 2022, 8, 638. [Google Scholar] [CrossRef]
- Ambreen, Z.; Faran, S.A.; Daniel, A.; Khalid, S.H.; Khan, I.U.; Asif, M.; Rehman, A.; Mehmood, H.Q.; Asghar, S. Physicochemical, rheological and antifungal evaluation of miconazole nitrate organogels for topical delivery. Pak. J. Pharm. Sci. 2022, 35, 1215–1221. [Google Scholar]
- Jun Yang, S.; Yoon, K.S. Preparation and Evaluation of Pluronic Lecithin Organogels in Cosmetics. J. Cosmet. Sci. 2021, 72, 325–346. [Google Scholar]
- Kircik, L.H. Vehicles Always Matter. J. Drugs Dermatol. 2019, 18, s99. [Google Scholar] [PubMed]
- Hoc, D.; Haznar-Garbacz, D. Foams as unique drug delivery systems. Eur. J. Pharm. Biopharm. 2021, 167, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Daniels, R.; Knie, U. Galenics of dermal products--vehicles, properties and drug release. J. Dtsch. Dermatol. Ges. 2007, 5, 367–383. [Google Scholar] [CrossRef] [PubMed]
- Weiss, S.C. Conventional topical delivery systems. Dermatol. Ther. 2011, 24, 471–476. [Google Scholar] [CrossRef]
- Rosen, J.; Landriscina, A.; Friedman, A.J. Principles and approaches for optimizing therapy with unique topical vehicles. J. Drugs Dermatol. 2014, 13, 1431–1435. [Google Scholar]
- Mayba, J.N.; Gooderham, M.J. A Guide to Topical Vehicle Formulations. J. Cutan. Med. Surg. 2018, 22, 207–212. [Google Scholar] [CrossRef]
- Barnes, T.M.; Mijaljica, D.; Townley, J.P.; Spada, F.; Harrison, I.P. Vehicles for Drug Delivery and Cosmetic Moisturizers: Review and Comparison. Pharmaceutics 2021, 13, 2012. [Google Scholar] [CrossRef]
- EMA. Reflection Paper on the Use of Extrapolation in the Development of Medicines for Paediatrics (EMA/189724/2018). Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/adopted-reflection-paper-use-extrapolation-development-medicines-paediatrics-revision-1_en.pdf (accessed on 20 February 2023).
- EMA. Guideline on Pharmaceutical Development of Medicines for Paediatric Use (EMA/CHMP/QWP/805880/2012 Rev.2). Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-pharmaceutical-development-medicines-paediatric-use_en.pdf (accessed on 20 February 2023).
- EMA. Reflection paper on the pharmaceutical development of medicines for use in the older population (EMA/CHMP/QWP/292439/2017). Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/reflection-paper-pharmaceutical-development-medicines-use-older-population-first-version_en.pdf (accessed on 20 February 2023).
- FDA. Patient-Focused Drug Development: Methods to Identify What Is Important to Patients. Available online: https://www.fda.gov/media/131230/download (accessed on 20 February 2023).
- Perfetto, E.M.; Burke, L.; Oehrlein, E.M.; Epstein, R.S. Patient-Focused Drug Development: A New Direction for Collaboration. Med. Care 2015, 53, 9–17. [Google Scholar] [CrossRef]
- Chalasani, M.; Vaidya, P.; Mullin, T. Enhancing the incorporation of the patient’s voice in drug development and evaluation. Res. Involv. Engagem. 2018, 4, 10. [Google Scholar] [CrossRef]
- Zvonareva, O.; Craveț, C.; Richards, D.P. Practices of patient engagement in drug development: A systematic scoping review. Res. Involv. Engagem. 2022, 8, 29. [Google Scholar] [CrossRef]
- ICH. Proposed ICH guideline work to advance patient focused drug development. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-reflection-paper-proposed-ich-guideline-work-advance-patient-focused-drug-development_en.pdf (accessed on 20 February 2023).
- Stegemann, S.; Ternik, R.L.; Onder, G.; Khan, M.A.; van Riet-Nales, D.A. Defining Patient Centric Pharmaceutical Drug Product Design. AAPS J. 2016, 18, 1047–1055. [Google Scholar] [CrossRef] [PubMed]
- Timpe, C.; Stegemann, S.; Barrett, A.; Mujumdar, S. Challenges and opportunities to include patient-centric product design in industrial medicines development to improve therapeutic goals. Br. J. Clin. Pharmacol. 2020, 86, 2020–2027. [Google Scholar] [CrossRef] [PubMed]
- Algorri, M.; Cauchon, N.S.; Christian, T.; O’Connell, C.; Vaidya, P. Patient-Centric Product Development: A Summary of Select Regulatory CMC and Device Considerations. J. Pharm. Sci. 2023, 112, 922–936. [Google Scholar] [CrossRef] [PubMed]
- Ogbonna, J.D.N.; Cunha, E.; Attama, A.A.; Ofokansi, K.C.; Ferreira, H.; Pinto, S.; Gomes, J.; Marx, Í.M.G.; Peres, A.M.; Lobo, J.M.S.; et al. Overcoming Challenges in Pediatric Formulation with a Patient-Centric Design Approach: A Proof-of-Concept Study on the Design of an Oral Solution of a Bitter Drug. Pharmaceuticals 2022, 15, 1331. [Google Scholar] [CrossRef] [PubMed]
- Shariff, Z.; Kirby, D.; Missaghi, S.; Rajabi-Siahboomi, A.; Maidment, I. Patient-Centric Medicine Design: Key Characteristics of Oral Solid Dosage Forms that Improve Adherence and Acceptance in Older People. Pharmaceutics 2020, 12, 905. [Google Scholar] [CrossRef]
- Drumond, N. Future Perspectives for Patient-Centric Pharmaceutical Drug Product Design with Regard to Solid Oral Dosage Forms. J. Pharm. Innov. 2020, 15, 318–324. [Google Scholar] [CrossRef]
- Oliveira, R.S.; da Silva, D.F.; Mota, S.; Garrido, J.; Garrido, E.M.; Lobo, J.M.S.; Almeida, I.F. Design of an Emulgel for Psoriasis Focused on Patient Preferences. Appl. Sci. 2022, 12, 3260. [Google Scholar] [CrossRef]
- Cook, N.S.; Cave, J.; Holtorf, A.P. Patient Preference Studies During Early Drug Development: Aligning Stakeholders to Ensure Development Plans Meet Patient Needs. Front. Med. 2019, 6, 82. [Google Scholar] [CrossRef]
- Stegemann, S.; Sheehan, L.; Rossi, A.; Barrett, A.; Paudel, A.; Crean, A.; Ruiz, F.; Bresciani, M.; Liu, F.; Shariff, Z.; et al. Rational and practical considerations to guide a target product profile for patient-centric drug product development with measurable patient outcomes—A proposed roadmap. Eur. J. Pharm. Biopharm. 2022, 177, 81–88. [Google Scholar] [CrossRef]
- Surber, C.; Smith, E.W. The mystical effects of dermatological vehicles. Dermatology 2005, 210, 157–168. [Google Scholar] [CrossRef]
- Danby, S.G.; Draelos, Z.D.; Gold, L.F.S.; Cha, A.; Vlahos, B.; Aikman, L.; Sanders, P.; Wu-Linhares, D.; Cork, M.J. Vehicles for atopic dermatitis therapies: More than just a placebo. J. Dermatol. Treat. 2022, 33, 685–698. [Google Scholar] [CrossRef]
- Crowther, J.M.; Sieg, A.; Blenkiron, P.; Marcott, C.; Matts, P.J.; Kaczvinsky, J.R.; Rawlings, A.V. Measuring the effects of topical moisturizers on changes in stratum corneum thickness, water gradients and hydration in vivo. Br. J. Dermatol. 2008, 159, 567–577. [Google Scholar] [CrossRef]
- Spada, F.; Barnes, T.M.; Greive, K.A. Skin hydration is significantly increased by a cream formulated to mimic the skin’s own natural moisturizing systems. Clin. Cosmet. Investig. Dermatol. 2018, 11, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Danby, S.G.; Andrew, P.V.; Taylor, R.N.; Kay, L.J.; Chittock, J.; Pinnock, A.; Ulhaq, I.; Fasth, A.; Carlander, K.; Holm, T.; et al. Different types of emollient cream exhibit diverse physiological effects on the skin barrier in adults with atopic dermatitis. Clin Exp. Dermatol. 2022, 47, 1154–1164. [Google Scholar] [CrossRef] [PubMed]
- Lodén, M. Effect of moisturizers on epidermal barrier function. Clin. Dermatol. 2012, 30, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Draelos, Z.D. New treatments for restoring impaired epidermal barrier permeability: Skin barrier repair creams. Clin. Dermatol. 2012, 30, 345–348. [Google Scholar] [CrossRef] [PubMed]
- Murasawa, Y.; Furuta, K.; Noda, Y.; Nakamura, H.; Fujii, S.; Isogai, Z. Ointment vehicles regulate the wound-healing process by modifying the hyaluronan-rich matrix. Wound Repair Regen. 2018, 26, 437–445. [Google Scholar] [CrossRef] [PubMed]
- van Zuuren, E.J.; Fedorowicz, Z.; Christensen, R.; Lavrijsen, A.; Arents, B.W.M. Emollients and moisturisers for eczema. Cochrane Database Syst. Rev. 2017, 2, Cd012119. [Google Scholar] [CrossRef]
- Spigariolo, C.B.; Ferrucci, S.M. Efficacy and tolerability of a repairing moisturizing cream containing amino-inositole and urea 10% in adults with chronic eczematous dermatitis of the hands. Ital. J. Dermatol. Venerol. 2023, 158, 42–48. [Google Scholar] [CrossRef]
- Fakhouri, T.; Yentzer, B.A.; Feldman, S.R. Advancement in benzoyl peroxide-based acne treatment: Methods to increase both efficacy and tolerability. J. Drugs Dermatol. 2009, 8, 657–661. [Google Scholar]
- Hoffman, L.K.; Bhatia, N.; Zeichner, J.; Kircik, L.H. Topical Vehicle Formulations in the Treatment of Acne. J. Drugs Dermatol. 2018, 17, s6–s10. [Google Scholar] [PubMed]
- Menditto, E.; Orlando, V.; De Rosa, G.; Minghetti, P.; Musazzi, U.M.; Cahir, C.; Kurczewska-Michalak, M.; Kardas, P.; Costa, E.; Sousa Lobo, J.M.; et al. Patient Centric Pharmaceutical Drug Product Design-The Impact on Medication Adherence. Pharmaceutics 2020, 12, 44. [Google Scholar] [CrossRef] [PubMed]
- Draelos, Z.; Tanghetti, E.; Guenin, E. Vehicle Formulation Impacts Tolerability and Patient Preference: Comparison of Tretinoin Branded Lotion and Generic Cream. J. Drugs Dermatol. 2022, 21, 875–880. [Google Scholar] [CrossRef]
- Tan, X.; Feldman, S.R.; Chang, J.; Balkrishnan, R. Topical drug delivery systems in dermatology: A review of patient adherence issues. Expert Opin. Drug Deliv. 2012, 9, 1263–1271. [Google Scholar] [CrossRef]
- Patel, N.U.; D’Ambra, V.; Feldman, S.R. Increasing Adherence with Topical Agents for Atopic Dermatitis. Am. J. Clin. Dermatol. 2017, 18, 323–332. [Google Scholar] [CrossRef]
- Umar, N.; Yamamoto, S.; Loerbroks, A.; Terris, D. Elicitation and use of patients’ preferences in the treatment of psoriasis: A systematic review. Acta Derm. Venereol. 2012, 92, 341–346. [Google Scholar] [CrossRef]
- de Wijs, L.E.M.; van Egmond, S.; Devillers, A.C.A.; Nijsten, T.; Hijnen, D.; Lugtenberg, M. Needs and preferences of patients regarding atopic dermatitis care in the era of new therapeutic options: A qualitative study. Arch. Dermatol. Res. 2023, 315, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Svendsen, M.T.; Feldman, S.R.; Tiedemann, S.N.; Sørensen, A.S.S.; Rivas, C.M.R.; Andersen, K.E. Psoriasis patient preferences for topical drugs: A systematic review. J. Dermatol. Treat. 2021, 32, 478–483. [Google Scholar] [CrossRef]
- Park, E.-K.; Song, K.-W. Rheological evaluation of petroleum jelly as a base material in ointment and cream formulations: Steady shear flow behavior. Arch. Pharmacal Res. 2010, 33, 141–150. [Google Scholar] [CrossRef]
- Eastman, W.J.; Malahias, S.; Delconte, J.; DiBenedetti, D. Assessing attributes of topical vehicles for the treatment of acne, atopic dermatitis, and plaque psoriasis. Cutis 2014, 94, 46–53. [Google Scholar]
- Figenshau, K.; Kimmis, B.D.; Reicherter, P. Variations in preference for topical vehicles among demographic groups. Cutis 2020, 106, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Fisher, E.J.; Adams, B.B. African American and Caucasian patients’ vehicle preference for the scalp. J. Am. Acad. Dermatol. 2008, 58, S46–S47. [Google Scholar] [CrossRef] [PubMed]
- Kircik, L.H.; Green, L.; Guenin, E.; Khalid, W.; Alexander, B. Dermal sensitization, safety, tolerability, and patient preference of tazarotene 0.045% lotion from five clinical trials. J. Dermatolog. Treat. 2022, 33, 2241–2249. [Google Scholar] [CrossRef] [PubMed]
- Kellett, N.; West, F.; Finlay, A.Y. Conjoint analysis: A novel, rigorous tool for determining patient preferences for topical antibiotic treatment for acne. A randomised controlled trial. Br. J. Dermatol. 2006, 154, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Kunkiel, K.; Natkańska, A.; Nędzi, M.; Zawadzka-Krajewska, A.; Feleszko, W. Patients’ preferences of leave-on emollients: A survey on patients with atopic dermatitis. J. Dermatol. Treat. 2022, 33, 1143–1145. [Google Scholar] [CrossRef]
- Ervin, C.; Crawford, R.; Evans, E.; Feldman, S.R.; Zeichner, J.; Zielinski, M.A.; Cappelleri, J.C.; DiBonaventura, M.; Takiya, L.; Myers, D.E. Patient and caregiver preferences on treatment attributes for atopic dermatitis. J. Dermatol. Treat. 2022, 33, 2225–2233. [Google Scholar] [CrossRef] [PubMed]
- Kosse, R.C.; Bouvy, M.L.; Daanen, M.; de Vries, T.W.; Koster, E.S. Adolescents’ Perspectives on Atopic Dermatitis Treatment-Experiences, Preferences, and Beliefs. JAMA Dermatol. 2018, 154, 824–827. [Google Scholar] [CrossRef]
- Maleki-Yazdi, K.A.; Heen, A.F.; Zhao, I.X.; Guyatt, G.H.; Suzumura, E.A.; Makhdami, N.; Chen, L.; Winders, T.; Wheeler, K.E.; Wang, J.; et al. Values and Preferences of Patients and Caregivers Regarding Treatment of Atopic Dermatitis (Eczema): A Systematic Review. JAMA Dermatol. 2023, 159, 320–330. [Google Scholar] [CrossRef]
- Contento, M.; Cline, A.; Russo, M. Steroid Phobia: A Review of Prevalence, Risk Factors, and Interventions. Am. J. Clin. Dermatol. 2021, 22, 837–851. [Google Scholar] [CrossRef]
- Williamson, T.; Cameron, J.; McLeod, K.; Turner, B.; Quillen, A.; LaRose, A. Patient Concerns and Treatment Satisfaction in Patients Treated with Azelaic Acid Foam for Rosacea. SKIN J. Cutan. Med. 2018, 2, S36. [Google Scholar] [CrossRef]
- Williamson, T.; Cheng, W.Y.; McCormick, N.; Vekeman, F. Patient Preferences and Therapeutic Satisfaction with Topical Agents for Rosacea: A Survey-Based Study. Am. Health Drug Benefits 2018, 11, 97–106. [Google Scholar] [PubMed]
- Damiani, G.; Bragazzi, N.L.; Karimkhani Aksut, C.; Wu, D.; Alicandro, G.; McGonagle, D.; Guo, C.; Dellavalle, R.; Grada, A.; Wong, P.; et al. The Global, Regional, and National Burden of Psoriasis: Results and Insights From the Global Burden of Disease 2019 Study. Front. Med. 2021, 8, 743180. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, L.; Huang, K.; Harrison, J.; Clark, A.; Feldman, S. Calcipotriene 0.005%-Betamethasone Dipropionate 0.064% Ointment Versus Topical Suspension in the Treatment of Plaque Psoriasis: A Randomized Pilot Study of Patient Preference. Cutis 2014, 94, 304–309. [Google Scholar] [PubMed]
- Housman, T.S.; Mellen, B.G.; Rapp, S.R.; Fleischer, A.B., Jr.; Feldman, S.R. Patients with psoriasis prefer solution and foam vehicles: A quantitative assessment of vehicle preference. Cutis 2002, 70, 327–332. [Google Scholar] [PubMed]
- Hill, D.; Farhangian, M.E.; Feldman, S.R. Increasing adherence to topical therapy in psoriasis through use of solution medication. Dermatol. Online J. 2016, 22, 16. [Google Scholar] [CrossRef]
- Adam, D.N.; Abdulla, S.J.; Fleming, P.; Gooderham, M.J.; Ashkenas, J.; McCracken, C.B. Transition of Topical Therapy Formulation in Psoriasis: Insights from a Canadian Practice Reflective. Skin Therapy Lett. 2022, 27, 6–11. [Google Scholar]
- Chung, M.; Yeroushalmi, S.; Hakimi, M.; Bartholomew, E.; Liao, W.; Bhutani, T. A critical review of halobetasol propionate foam (0.05%) as a treatment option for adolescent plaque psoriasis. Expert Rev. Clin. Immunol. 2022, 18, 997–1003. [Google Scholar] [CrossRef]
- Bhatia, N.; Stein Gold, L.; Kircik, L.H.; Schreiber, R. Two Multicenter, Randomized, Double-Blind, Parallel Group Comparison Studies of a Novel Foam Formulation of Halobetasol Propionate, 0.05% vs Its Vehicle in Adult Subjects With Plaque Psoriasis. J Drugs Dermatol. 2019, 18, 790–796. [Google Scholar]
- Aschoff, R.; Bewley, A.; Dattola, A.; De Simone, C.; Lahfa, M.; Llamas-Velasco, M.; Martorell, A.; Pavlovic, M.; Sticherling, M. Beyond-Mild Psoriasis: A Consensus Statement on Calcipotriol and Betamethasone Dipropionate Foam for the Topical Treatment of Adult Patients. Dermatol. Ther. 2021, 11, 1791–1804. [Google Scholar] [CrossRef]
- Dattola, A.; Silvestri, M.; Bennardo, L.; Passante, M.; Rizzuto, F.; Dastoli, S.; Patruno, C.; Bianchi, L.; Nisticò, S.P. A novel vehicle for the treatment of psoriasis. Dermatol. Ther. 2020, 33, e13185. [Google Scholar] [CrossRef]
- Pinter, A.; Green, L.J.; Selmer, J.; Praestegaard, M.; Gold, L.S.; Augustin, M. A pooled analysis of randomized, controlled, phase 3 trials investigating the efficacy and safety of a novel, fixed dose calcipotriene and betamethasone dipropionate cream for the topical treatment of plaque psoriasis. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Vasconcelos, V.; Teixeira, A.; Almeida, V.; Teixeira, M.; Ramos, S.; Torres, T.; Sousa Lobo, J.M.; Almeida, I.F. Patient preferences for attributes of topical anti-psoriatic medicines. J. Dermatol. Treat. 2019, 30, 659–663. [Google Scholar] [CrossRef] [PubMed]
- Weiss, S.; Wyres, M.; Brundage, T. A novel foam vehicle is consistently preferred by patients for dermatologic conditions. J. Am. Acad. Dermatol. 2011, 64, AB50. [Google Scholar] [CrossRef]
- Gutknecht, M.; Schaarschmidt, M.L.; Herrlein, O.; Augustin, M. A systematic review on methods used to evaluate patient preferences in psoriasis treatments. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1454–1464. [Google Scholar] [CrossRef] [PubMed]
- Nair, P.A.; Vora, R.V.; Jivani, N.B.; Gandhi, S.S. A study of clinical profile and quality of life in patients with scabies. Int. J. Res. Dermatol. 2021, 7, 508–512. [Google Scholar] [CrossRef]
- Garg, B.J.; Saraswat, A.; Bhatia, A.; Katare, O.P. Topical treatment in vitiligo and the potential uses of new drug delivery systems. Indian J. Dermatol. Venereol. Leprol. 2010, 76, 231–238. [Google Scholar] [CrossRef]
- Felix, K.; Unrue, E.; Inyang, M.; Cardwell, L.A.; Oussedik, E.; Richardson, I.; Feldman, S.R. Patients preferences for different corticosteroid vehicles are highly variable. J. Dermatol. Treat. 2020, 31, 147–151. [Google Scholar] [CrossRef]
- Carvalho, M.; Almeida, I.F. The Role of Pharmaceutical Compounding in Promoting Medication Adherence. Pharmaceuticals 2022, 15, 1091. [Google Scholar] [CrossRef]
- Savary, J.; Ortonne, J.P.; Aractingi, S. The right dose in the right place: An overview of current prescription, instruction and application modalities for topical psoriasis treatments. J. Eur. Acad. Dermatol. Venereol. 2005, 19 (Suppl. S3), 14–17. [Google Scholar] [CrossRef]
- Buxton, P.K.; Morris-Jones, R. ABC of Dermatology, 5th ed.; Paul, K., Buxton, R.M.-J., Eds.; BMJ Books: London, UK, 2013. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vehicle | Composition | Characteristics | Examples |
|---|---|---|---|
| Solutions | Solute (or solutes) dissolved in a liquid solvent such as water, alcohol, glycols, or oil | Clear and transparent | Urea aqueous solution |
| Suspensions | Insoluble powders dispersed in a liquid phase | Translucent or opaque; with time, the suspended solids tend to settle | Aqueous zinc suspension |
| Emulsions | Homogeneous two-phase liquid systems of water, liquid oils, and emulsifying agents | Opaque and homogeneous | Lanette lotion |
| Base | Composition | Characteristics | Examples |
|---|---|---|---|
| Hydrophobic | Solid and liquid paraffin, petrolatum, waxes, triglycerides, vegetable oils, silicone oils | Emollients, occlusive, greasy, and difficult to remove; high retention on the skin; form an occlusive layer that prevents water loss; rapid delivery of hydrophilic drugs; very low water absorption (<5%) | Coal-tar-paraffin ointment |
| Absorption | Water-absorbent components: lanolin; lanolin alcohols; cholesterol; bees wax; emulsifying agents | Emollient, occlusive, and greasy, albeit less than hydrophobic bases; make emulsions by adding water; | Hydrophilic ointment (USP) or Cetylic ointment (PPh) |
| Water-in-oil (W/O) cream | Water, hydrocarbons, waxes, polyethylene glycols, and emulsifying agents | Water-in-oil two-phase system; occlusive properties; when applied to the skin, they leave an oily film on the surface of the skin | Cold cream (USP) Cooling ointment (FNA) |
| Oil-in-water (O/W) cream | Water, hydrocarbons, waxes, polyethylene glycols, and emulsifying agents | Oil-in-water two-phase system; non-occlusive; non-greasy; moisturizing and emollient effect | Lanette cream (BP) |
| Anhydrous hydrophilic | PEGs of different molecular weights | Non-occlusive, non-oily, and easily removable; exudate miscibility but hyperosmotic miscible; low water absorption | Macrogol ointment |
| Hydrogels | Organic macromolecules or polymers dispersed in water: natural (xanthan gum, alginate); semi-synthetics (cellulose derivatives); synthetics (carbomer) | Transparent aqueous formulations with no grease; easy to apply and remove; refreshing properties; little moisturizing or emollient effect; may contain alcohol, so they are likely to cause irritation and have drying ability; the aqueous medium is susceptible to degradation | Carbomer gel Carboxymethylcellulose gel |
| Oleogels | Organic macromolecules or polymers dispersed in a lipophilic oil | Moisturizing or emollient effect; leave an oily film on the surface of the skin | 12-hydroxystearic acid Oleogel |
| Pastes | Insoluble drug in an ointment or a hydrophilic base | High content of insoluble powders; protective effect; drying effect; varied consistency and solubility | Zinc-oxide paste Darier paste |
| Foams | Nonpolar hydrocarbons as propellants; Solvents include water, oils, ethanol, acetone, hexadecyl alcohol, glycol ethers, and polyglycols | Pressurized solutions or fluid emulsions mixed with a propellent; no need to spread the product and quick-drying; low skin residue low hydration or occlusive effect | Coal-tar foam (Scytera®) |
| Palmoplantar | Glabrous | Hairy | Facial or Intertrigital | |
|---|---|---|---|---|
| Very dry | Hydrophobic ointments | Hydrophobic ointments | Oil solutions | W/O emulsions |
| Absorption ointments | Absorption ointments | W/O emulsions | O/W emulsions | |
| W/O emulsions | W/S emulsions | |||
| Dry | Hydrophobic ointments | Absorption ointments | Oil solutions | W/O emulsions |
| Absorption ointments | W/O emulsions | O/W emulsions | O/W emulsions | |
| W/O emulsions | O/W emulsions | W/S emulsions | ||
| Subacute | Hydrophobic ointments | W/O emulsions | Oil solutions | W/O emulsions |
| W/O emulsions | O/W emulsions | Shampoos | O/W emulsions | |
| O/W emulsions | Hydrophobic pastes | W/S emulsions | ||
| Wet | W/O emulsions | O/W emulsions | O/W emulsions | O/W emulsions |
| O/W emulsions | Hydrogels | Hydrogels | ||
| Aqueous solutions | Hydrophilic pastes | |||
| Exudative | Hydrogels | Hydrogels | Hydrogels | Hydrogels |
| Aqueous solutions | Aqueous solutions | Aqueous solutions | Aqueous solutions | |
| Hydrophilic pastes | Hydrophilic pastes | Hydrophilic pastes |
| Dry Skin | Oily Skin | Combination Skin | Sensitive Skin |
|---|---|---|---|
| W/O cream | O/W cream (<30% F.C.) | O/W cream (<30% F.C.) | O/W cream (>50% F.C.) |
| O/W cream (>50% F.C.) | W/S cream | W/S cream | Oils |
| Emulgel Hydrogel | Glycoside cream | Glycoside cream Emulgel |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliveira, R.; Almeida, I.F. Patient-Centric Design of Topical Dermatological Medicines. Pharmaceuticals 2023, 16, 617. https://doi.org/10.3390/ph16040617
Oliveira R, Almeida IF. Patient-Centric Design of Topical Dermatological Medicines. Pharmaceuticals. 2023; 16(4):617. https://doi.org/10.3390/ph16040617
Chicago/Turabian StyleOliveira, Rita, and Isabel F. Almeida. 2023. "Patient-Centric Design of Topical Dermatological Medicines" Pharmaceuticals 16, no. 4: 617. https://doi.org/10.3390/ph16040617
APA StyleOliveira, R., & Almeida, I. F. (2023). Patient-Centric Design of Topical Dermatological Medicines. Pharmaceuticals, 16(4), 617. https://doi.org/10.3390/ph16040617