
Prognostic Value of CXCL12 in Non-Small Cell Lung Cancer Patients Undergoing Tumor Resection

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Results
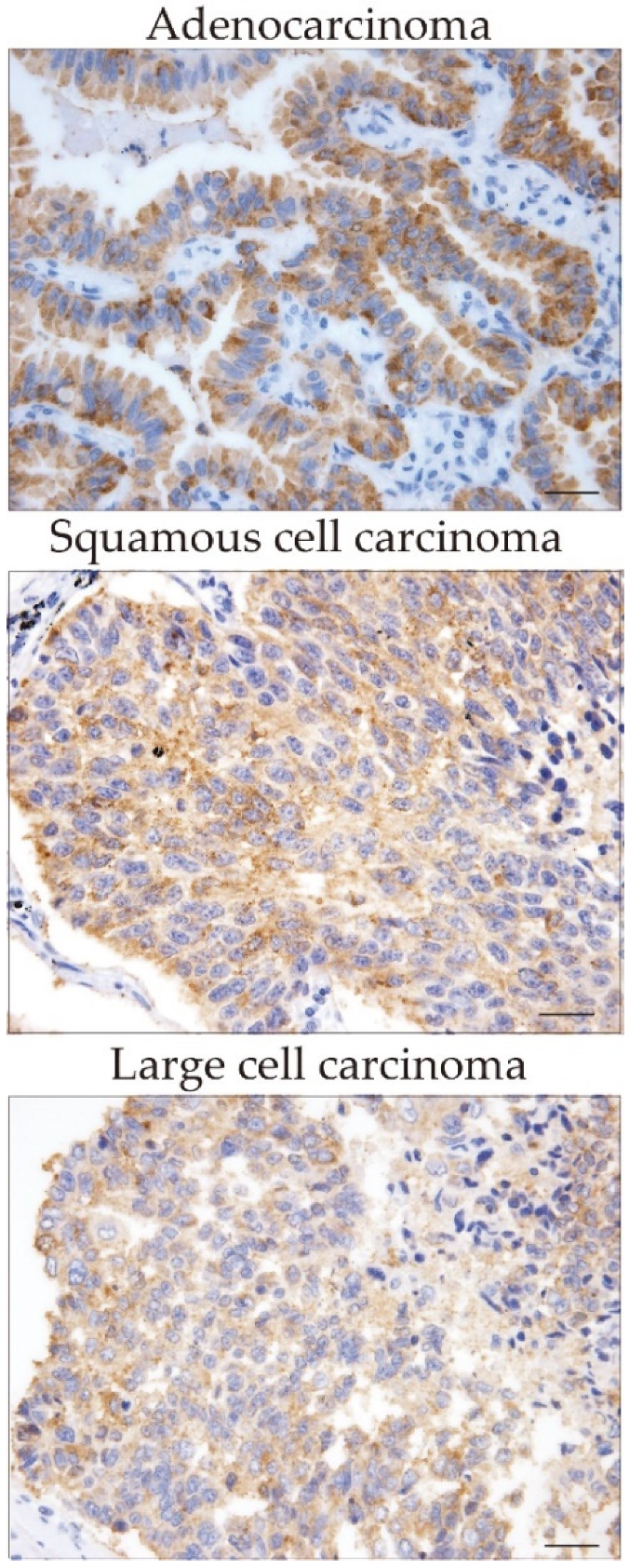
2.1. Expression of CXCL12 in Cancer Cells and Cancer-Associated Fibroblasts
2.2. CXCL-12 Staining Was Not Associated with Clinicopathological Parameters
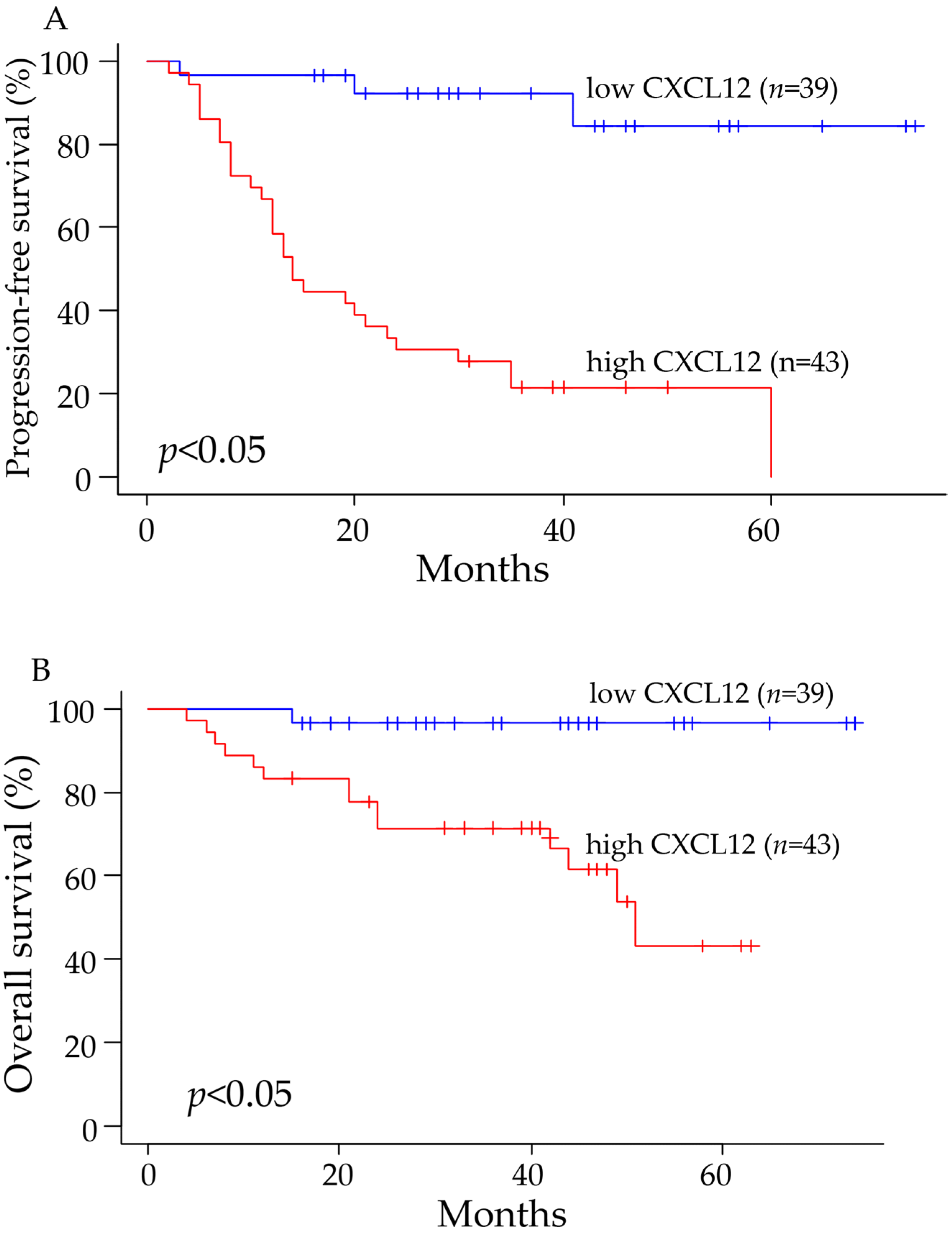
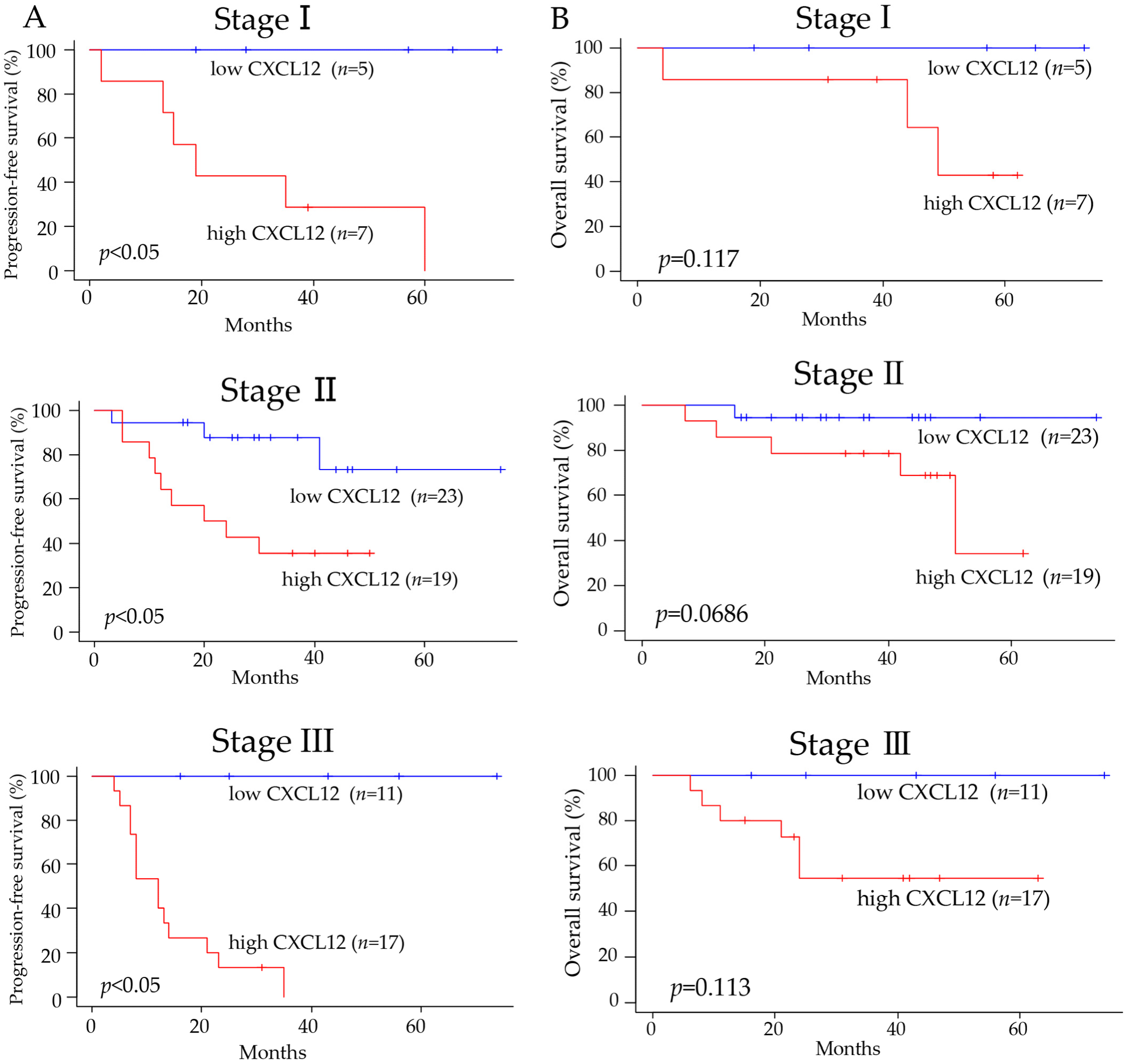
2.3. CXCL12 Expression Was Associated with the Prognosis of Cancer Patients
2.4. Univariate and Multivariate Analyses
2.5. CXCL12 May Be a Biomarker to Indicate Adjuvant Chemotherapy
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Immunohistochemistry
4.3. Scoring of CXCL12 Tumor Expression
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Altorki, N.K.; Markowitz, G.J.; Gao, D.; Port, J.L.; Saxena, A.; Stiles, B.; McGraw, T.; Mittal, V. The lung microenvironment: An important regulator of tumour growth and metastasis. Nat. Rev. Cancer 2019, 19, 9–31. [Google Scholar] [CrossRef] [PubMed]
- Okami, J.; Shintani, Y.; Okumura, M.; Ito, H.; Ohtsuka, T.; Toyooka, S.; Mori, T.; Watanabe, S.I.; Date, H.; Yokoi, K.; et al. Demographics, Safety and Quality, and Prognostic Information in Both the Seventh and Eighth Editions of the TNM Classification in 18,973 Surgical Cases of the Japanese Joint Committee of Lung Cancer Registry Database in 2010. J. Thorac. Oncol. 2019, 14, 212–222. [Google Scholar] [CrossRef]
- Douillard, J.Y.; Tribodet, H.; Aubert, D.; Shepherd, F.A.; Rosell, R.; Ding, K.; Veillard, A.S.; Seymour, L.; Le Chevalier, T.; Spiro, S.; et al. Adjuvant cisplatin and vinorelbine for completely resected non-small cell lung cancer: Subgroup analysis of the Lung Adjuvant Cisplatin Evaluation. J. Thorac. Oncol. 2010, 5, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Hamada, C.; Tsuboi, M.; Ohta, M.; Fujimura, S.; Kodama, K.; Imaizumi, M.; Wada, H. Effect of postoperative adjuvant chemotherapy with tegaf ur-uracil on survival in patients with stage IA non-small cell lung cancer: An exploratory analysis from a meta-analysis of six randomized controlled trials. J. Thorac. Oncol. 2009, 4, 1511–1516. [Google Scholar] [CrossRef] [PubMed]
- Uramoto, H.; Tanaka, F. Recurrence after surgery in patients with NSCLC. Transl. Lung Cancer Res. 2014, 3, 242–249. [Google Scholar] [CrossRef]
- Burger, J.A.; Kipps, T.J. CXCR4: A key receptor in the crosstalk between tumor cells and their microenvironment. Blood 2006, 107, 1761–1767. [Google Scholar] [CrossRef] [PubMed]
- Phillips, R.J.; Burdick, M.D.; Lutz, M.; Belperio, J.A.; Keane, M.P.; Strieter, R.M. The stromal derived factor-1/CXCL12-CXC chemokine receptor 4 biological axis in non-small cell lung cancer metastases. Am. J. Respir. Crit. Care Med. 2003, 167, 1676–1686. [Google Scholar] [CrossRef] [PubMed]
- Wagner, P.L.; Hyjek, E.; Vazquez, M.F.; Meherally, D.; Liu, Y.F.; Chadwick, P.A.; Rengifo, T.; Sica, G.L.; Port, J.L.; Lee, P.C.; et al. CXCL12 and CXCR4 in adenocarcinoma of the lung: Association with metastasis and survival. J. Thorac. Cardiovasc. Surg. 2009, 137, 615–621. [Google Scholar] [CrossRef]
- Dewan, M.Z.; Ahmed, S.; Iwasaki, Y.; Ohba, K.; Toi, M.; Yamamoto, N. Stromal cell-derived factor-1 and CXCR4 receptor interaction in tumor growth and metastasis of breast cancer. Biomed. Pharmacother. 2006, 60, 273–276. [Google Scholar] [CrossRef]
- Zhang, C.; Li, J.; Han, Y.; Jiang, J. A meta-analysis for CXCR4 as a prognostic marker and potential drug target in non-small cell lung cancer. Drug Des. Dev. Ther. 2015, 9, 3267–3278. [Google Scholar] [CrossRef]
- Muller, A.; Homey, B.; Soto, H.; Ge, N.; Catron, D.; Buchanan, M.E.; McClanahan, T.; Murphy, E.; Yuan, W.; Wagner, S.N.; et al. Involvement of chemokine receptors in breast cancer metastasis. Nature 2001, 410, 50–56. [Google Scholar] [CrossRef]
- Economidou, F.; Antoniou, K.M.; Soufla, G.; Lasithiotaki, I.; Karagiannis, K.; Lymbouridou, R.; Proklou, A.; Spandidos, D.A.; Siafakas, N.M. Role of VEGF-stromal cell-derived factor-1alpha/CXCL12 axis in pleural effusion of lung cancer. J. Recept. Signal Transduct. Res. 2010, 30, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Burger, J.A.; Peled, A. CXCR4 antagonists: Targeting the microenvironment in leukemia and other cancers. Leukemia 2009, 23, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Wald, O.; Izhar, U.; Amir, G.; Kirshberg, S.; Shlomai, Z.; Zamir, G.; Peled, A.; Shapira, O.M. Interaction between neoplastic cells and cancer-associated fibroblasts through the CXCL12/CXCR4 axis: Role in non-small cell lung cancer tumor proliferation. J. Thorac. Cardiovasc. Surg. 2011, 141, 1503–1512. [Google Scholar] [CrossRef] [PubMed]
- Burger, J.A.; Stewart, D.J.; Wald, O.; Peled, A. Potential of CXCR4 antagonists for the treatment of metastatic lung cancer. Expert Rev. Anticancer Ther. 2011, 11, 621–630. [Google Scholar] [CrossRef]
- Liang, C.M.; Chen, L.; Hu, H.; Ma, H.Y.; Gao, L.L.; Qin, J.; Zhong, C.P. Chemokines and their receptors play important roles in the development of hepatocellular carcinoma. World J. Hepatol. 2015, 7, 1390–1402. [Google Scholar] [CrossRef]
- Zhang, K.; Corsa, C.A.; Ponik, S.M.; Prior, J.L.; Piwnica-Worms, D.; Eliceiri, K.W.; Keely, P.J.; Longmore, G.D. The collagen receptor discoidin domain receptor 2 stabilizes SNAIL1 to facilitate breast cancer metastasis. Nat. Cell Biol. 2013, 15, 677–687. [Google Scholar] [CrossRef]
- Liu, L.; Liu, L.; Yao, H.H.; Zhu, Z.Q.; Ning, Z.L.; Huang, Q. Stromal Myofibroblasts Are Associated with Poor Prognosis in Solid Cancers: A Meta-Analysis of Published Studies. PLoS ONE 2016, 11, e0159947. [Google Scholar] [CrossRef]
- Allred, D.C.; Harvey, J.M.; Berardo, M.; Clark, G.M. Prognostic and predictive factors in breast cancer by immunohistochemical analysis. Mod. Pathol. 1998, 11, 155–168. [Google Scholar]
- Katsura, M.; Shoji, F.; Okamoto, T.; Shimamatsu, S.; Hirai, F.; Toyokawa, G.; Morodomi, Y.; Tagawa, T.; Oda, Y.; Maehara, Y. Correlation between CXCR4/CXCR7/CXCL12 chemokine axis expression and prognosis in lymph-node-positive lung cancer patients. Cancer Sci. 2018, 109, 154–165. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Carcinoma | |||||
|---|---|---|---|---|---|
| Overall | Strong | Weak | p Value | Expression | Expression |
| Numbers | 82 | 43 | 39 | ||
| Mean Age | 71.5 ± 9.0 | 72.8 ± 9.2 | 70.1 ± 8.6 | 0.169 | |
| Gender | |||||
| Female | 26 | 15 | 11 | 0.636 | |
| Male | 56 | 28 | 28 | ||
| Histology | |||||
| Adeno | 64 | 36 | 28 | 0.0461 | |
| Squamous | 11 | 2 | 9 | ||
| Adenosquamous | 2 | 2 | 0 | ||
| Large | 5 | 3 | 2 | ||
| T Score | |||||
| T1 | 19 | 7 | 12 | 0.418 | |
| T2 | 40 | 22 | 18 | ||
| T3 | 19 | 11 | 8 | ||
| T4 | 4 | 3 | 1 | ||
| N Score | |||||
| N0 | 28 | 15 | 13 | 0.922 | |
| N1 | 34 | 17 | 17 | ||
| N2 | 20 | 11 | 9 | ||
| P-Stage | |||||
| I | 12 | 7 | 5 | 0.445 | |
| II | 42 | 19 | 23 | ||
| III | 28 | 17 | 11 | ||
| Adjuvant Chemotherapy | |||||
| Treated | 35 | 19 | 16 | 0.947 | |
| Untreated | 47 | 24 | 23 | ||
| Lymphatic Vessel Invasion | |||||
| Positive | 72 | 38 | 34 | 0.869 | |
| Negative | 10 | 5 | 5 | ||
| Blood Vessel | |||||
| Invasion | |||||
| Positive | 66 | 36 | 30 | 0.437 | |
| Negative | 16 | 7 | 9 |
| Progression-Free Survival | ||||||
|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||||
| Factor | n | Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | |
| CXCL12 | Low | 39 | Ref | Ref | ||
| High | 43 | 7.05 (3.09–16.08) | 0.0000034 | 9.99 (4.02–24.84) | 0.00000073 | |
| Gender | Male | 56 | Ref | Ref | ||
| Female | 26 | 0.79 (0.41–1.52) | 0.48 | 0.65 (0.31–1.38) | 0.27 | |
| Age (years) | <75 | 50 | Ref | Ref | ||
| ≥75 | 32 | 1.60 (0.86–2.98) | 0.14 | 0.87 (0.37–2.03) | 0.74 | |
| Pathological Stage | I or II | 54 | Ref | Ref | ||
| III | 28 | 1.66 (0.89–3.1) | 0.11 | 1.88 (0.97–3.66) | 0.061 | |
| Histology | Non-Squamous | 71 | Ref | Ref | ||
| Squamous | 11 | 0.64 (0.23–1.81) | 0.4 | 1.16 (0.38–3.52) | 0.8 | |
| Adjuvant Chemotherapy | Untreated | 47 | Ref | Ref | ||
| Treated | 35 | 0.62 (0.33–1.16) | 0.14 | 0.44 (0.17–1.10) | 0.079 | |
| Overall Survival | ||||||
| Univariate Analysis | Multivariate Analysis | |||||
| Factor | n | Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | |
| CXCL12 | Low | 39 | Ref | Ref | ||
| High | 43 | 3.78 (1.4–10.19) | 0.0087 | 6.88 (2.17–21.85) | 0.0011 | |
| Gender | Male | 56 | Ref | Ref | ||
| Female | 26 | 0.07 (0.01–0.56) | 0.011 | 0.07 (0.01–0.57) | 0.013 | |
| Age (years) | <75 | 50 | Ref | Ref | ||
| ≥75 | 32 | 2.02 (0.89–4.6) | 0.092 | 0.75 (0.25–2.19) | 0.6 | |
| Pathological Stage | I or II | 54 | Ref | Ref | ||
| III | 28 | 1.18 (0.5–2.78) | 0.71 | 1.23 (0.49–3.04) | 0.66 | |
| Histology | Non-Squamous | 71 | Ref | Ref | ||
| Squamous | 11 | 1.45 (0.49–4.27) | 0.5 | 2.57 (0.77–8.56) | 0.12 | |
| Adjuvant Chemotherapy | Untreated | 47 | Ref | Ref | ||
| Treated | 35 | 0.40 (0.16–1) | 0.051 | 0.43 (0.12–1.47) | 0.18 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kogue, Y.; Kobayashi, H.; Nakamura, Y.; Takano, T.; Furuta, C.; Kawano, O.; Yasuma, T.; Nishimura, T.; D’Alessandro-Gabazza, C.N.; Fujimoto, H.; et al. Prognostic Value of CXCL12 in Non-Small Cell Lung Cancer Patients Undergoing Tumor Resection. Pharmaceuticals 2023, 16, 255. https://doi.org/10.3390/ph16020255
Kogue Y, Kobayashi H, Nakamura Y, Takano T, Furuta C, Kawano O, Yasuma T, Nishimura T, D’Alessandro-Gabazza CN, Fujimoto H, et al. Prognostic Value of CXCL12 in Non-Small Cell Lung Cancer Patients Undergoing Tumor Resection. Pharmaceuticals. 2023; 16(2):255. https://doi.org/10.3390/ph16020255
Chicago/Turabian StyleKogue, Yurie, Hiroyasu Kobayashi, Yutaka Nakamura, Takatsugu Takano, Chihiro Furuta, Osamu Kawano, Taro Yasuma, Tadashi Nishimura, Corina N. D’Alessandro-Gabazza, Hajime Fujimoto, and et al. 2023. "Prognostic Value of CXCL12 in Non-Small Cell Lung Cancer Patients Undergoing Tumor Resection" Pharmaceuticals 16, no. 2: 255. https://doi.org/10.3390/ph16020255
APA StyleKogue, Y., Kobayashi, H., Nakamura, Y., Takano, T., Furuta, C., Kawano, O., Yasuma, T., Nishimura, T., D’Alessandro-Gabazza, C. N., Fujimoto, H., Gabazza, E. C., Kobayashi, T., & Fukai, I. (2023). Prognostic Value of CXCL12 in Non-Small Cell Lung Cancer Patients Undergoing Tumor Resection. Pharmaceuticals, 16(2), 255. https://doi.org/10.3390/ph16020255