
Bacterial Cellulose—Adaptation of a Nature-Identical Material to the Needs of Advanced Chronic Wound Care

 , , , and
, , , and
Abstract
:1. Introduction
2. Results and Discussion
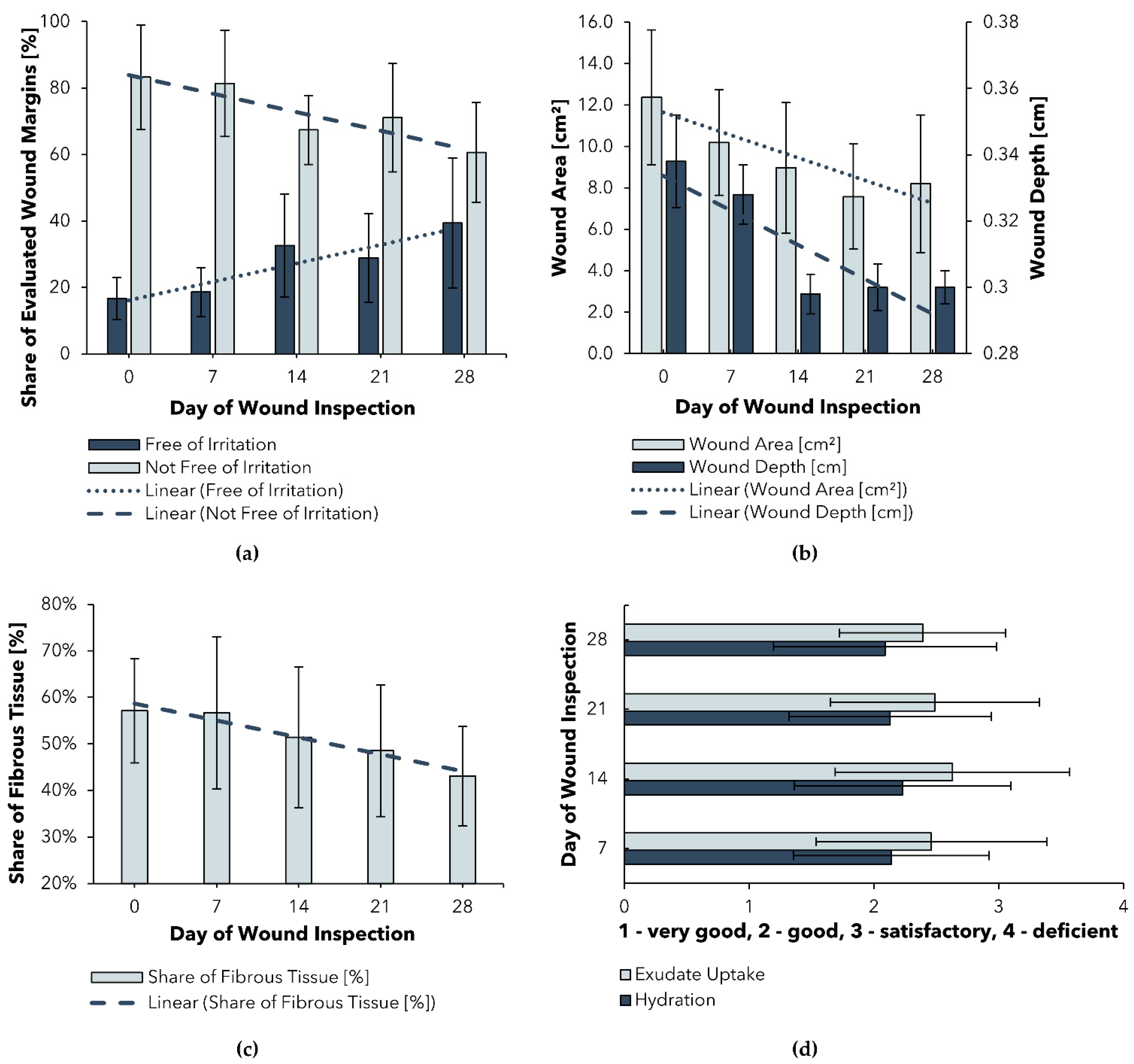
2.1. Post-Market Clinical Follow-Up Study
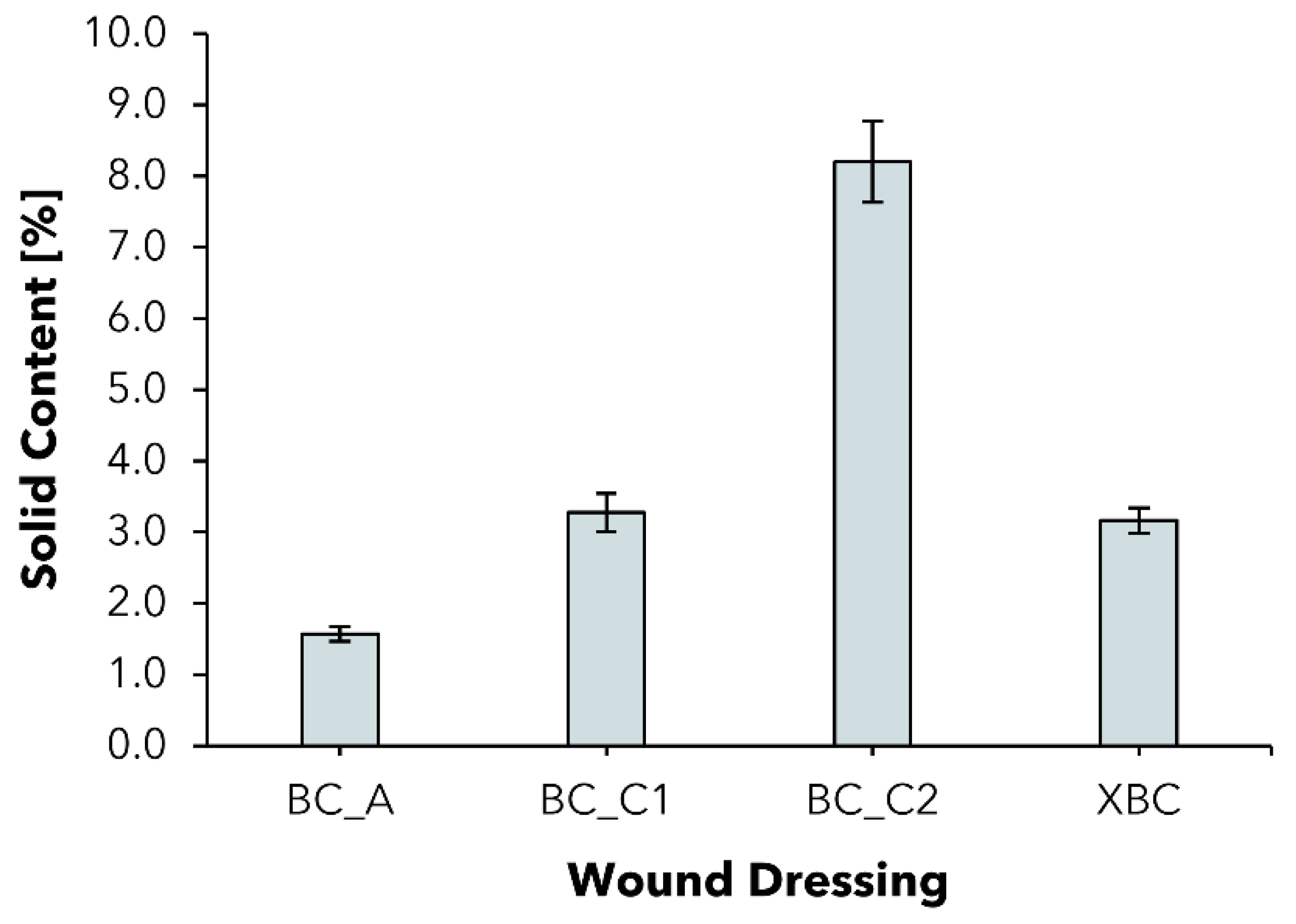
2.2. Solid Content
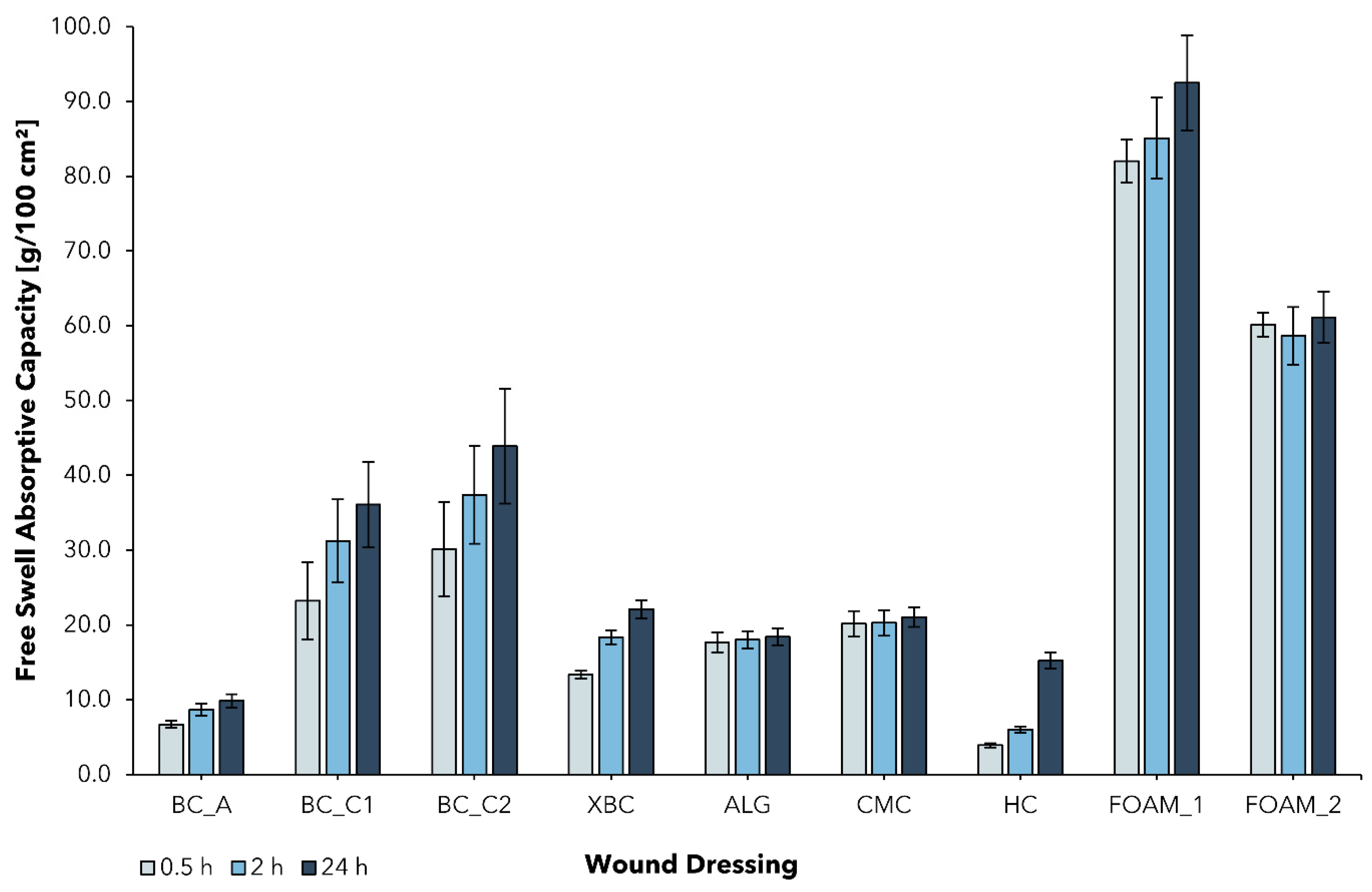
2.3. Free Swell Absorptive Capacity
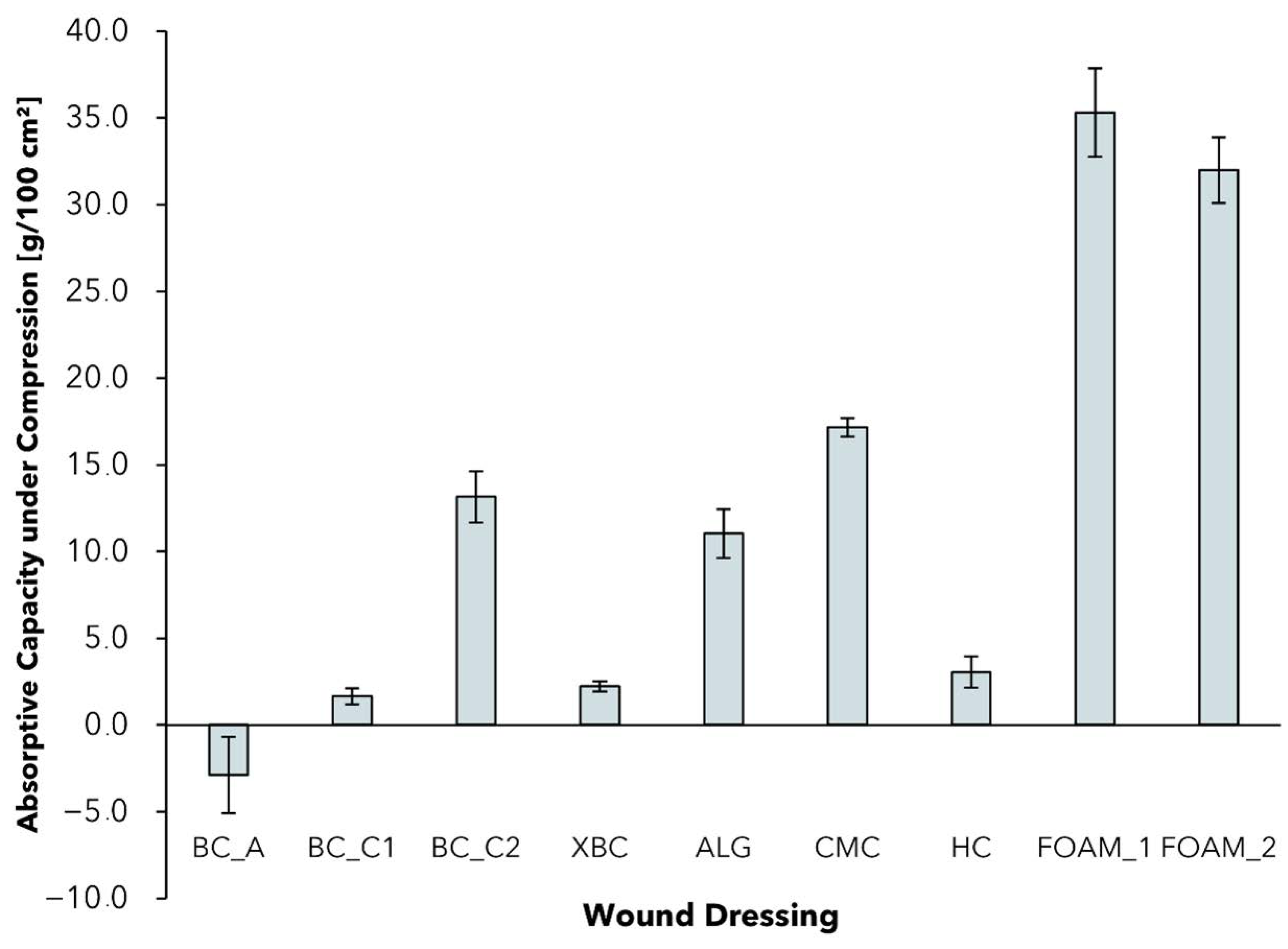
2.4. Absorptive Capacity under Pressure
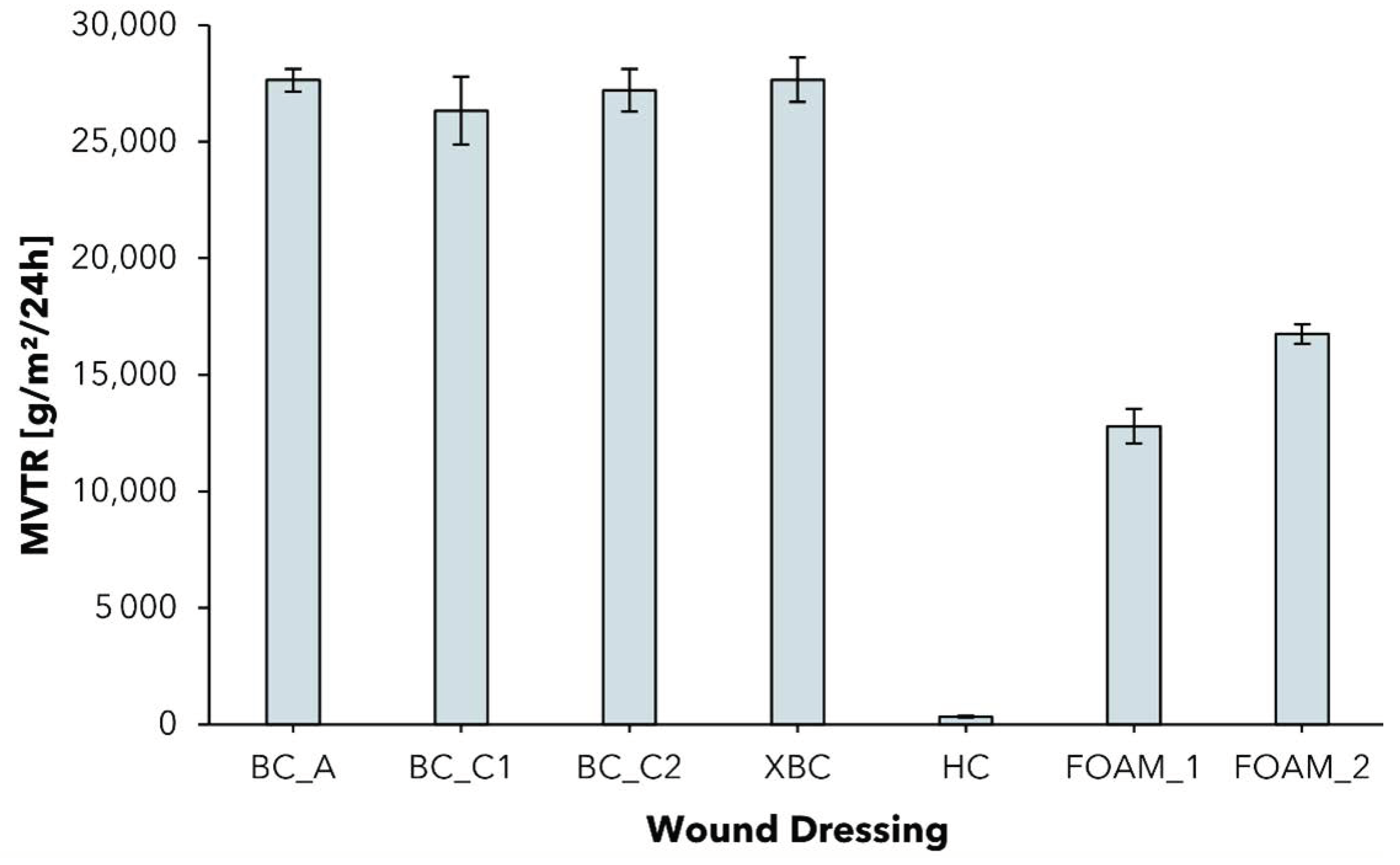
2.5. Moisture Vapor Transmission Rate
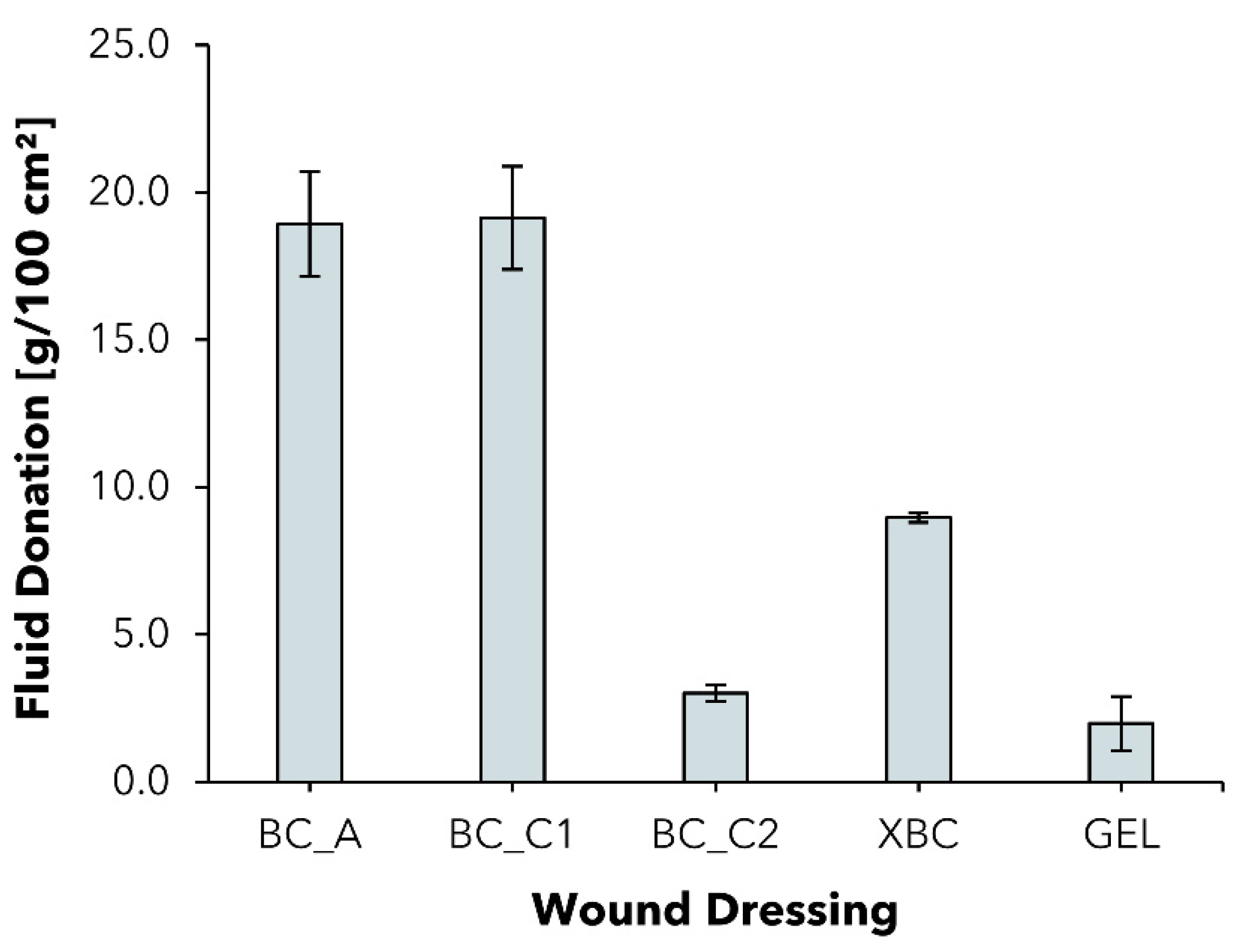
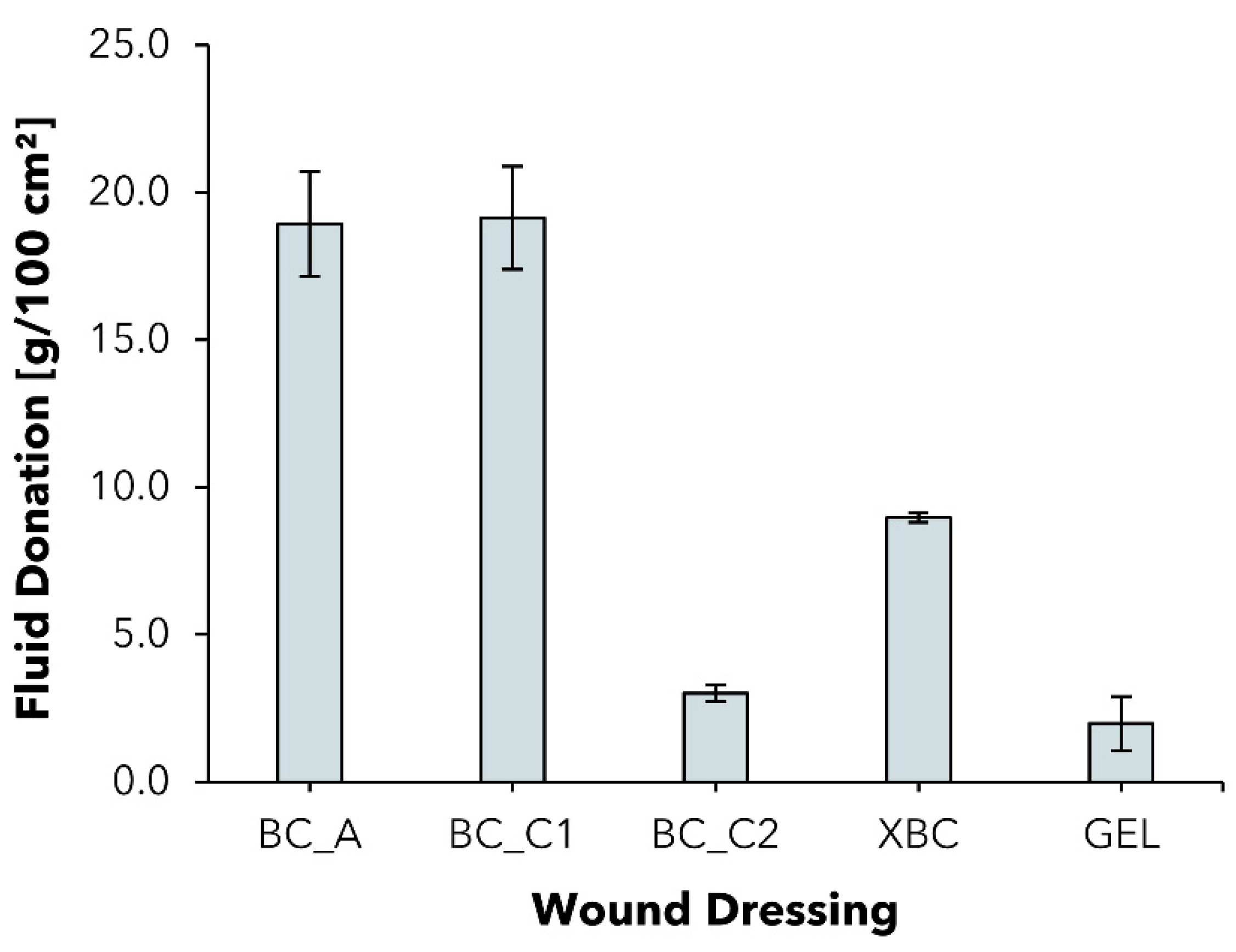
2.6. Fluid Donation
2.7. Overview of Results
3. Materials and Methods
3.1. Post-Market Clinical Follow-Up Study Design
3.2. In Vitro Tests
3.2.1. Materials
3.2.2. Preparation of Native BC
3.2.3. Solid Content
3.2.4. Free Swell Absorptive Capacity
3.2.5. Absorptive Capacity under Pressure
3.2.6. Moisture Vapor Transmission Rate
3.2.7. Fluid Donation
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations & Terms
| AC | Absorptive Capacity |
| ALG | Calcium Alginate dressing Suprasorb® A (Lohmann & Rauscher GmbH & Co. KG, Neuwied, Germany) |
| BC | Bacterial Cellulose |
| BC_A | BC based wound dressing epicitehydro (QRSKIN GmbH, Würzburg, Germany) |
| BC_C1 | Experimental, non-commercial and modified BC-based wound dressing |
| BC_C2 | Experimental, non-commercial, and modified BC Cellulose-based wound dressing |
| CCl | Compression Class |
| CMC | Sodium carboxymethylcellulose dressing Aquacel® Extra™ (ConvaTec Limited, Flintshire, UK) |
| DSMZ | Deutsche Sammlung von Mikroorganismen und Zellkulturen (German Collection of Microorganisms and Cell Cultures) |
| FD | Fluid Donation |
| FOAM_1 | Polyurethan foam dressing ALLEVYN Gentle (Smith & Nephew Medical Ltd., Hull, UK) |
| FOAM_2 | Soft silicone foam dressing Mepilex® (Mölnlycke Health Care AB, Göteborg, Sweden) |
| GEL | Gel dressing Suprasorb® G (Lohmann & Rauscher GmbH & Co. KG, Neuwied, Germany) |
| HC | Hydrocolloid dressing Hydrocoll® (PAUL HARTMANN Limited, Heywood, UK) |
| HET-CAV | Shell-less Hen’s Egg Test on Chick Area Vasculosa |
| HSM | Hestrin–Schramm culture medium |
| K. xylinus | Komagataeibacter xylinus |
| MTT | 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide |
| MVTR | Moisture Vapor Transmission Rate |
| PMCF | Post-Market Clinical Follow-up (Study) |
| SC | Solid Content |
| VLU | Venous Leg Ulcer |
| XBC | BC-based wound dressing Suprasorb® X (Lohmann & Rauscher GmbH & Co. KG, Neuwied, Germany) |
References
- Olsson, M.; Järbrink, K.; Divakar, U.; Bajpai, R.; Upton, Z.; Schmidtchen, A.; Car, J. The Humanistic and Economic Burden of Chronic Wounds: A Systematic Review: The Burden of Chronic Wounds. Wound Repair Regen. 2019, 27, 114–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fife, C.E.; Carter, M.J. Wound Care Outcomes and Associated Cost among Patients Treated in US Outpatient Wound Centers: Data from the US Wound Registry. Wounds Compend. Clin. Res. Pract. 2012, 24, 10–17. [Google Scholar]
- Graves, N.; Phillips, C.J.; Harding, K. A Narrative Review of the Epidemiology and Economics of Chronic Wounds. Br. J. Dermatol. 2021, bjd.20692. [Google Scholar] [CrossRef] [PubMed]
- Shi, C.; Wang, C.; Liu, H.; Li, Q.; Li, R.; Zhang, Y.; Liu, Y.; Shao, Y.; Wang, J. Selection of Appropriate Wound Dressing for Various Wounds. Front. Bioeng. Biotechnol. 2020, 8, 182. [Google Scholar] [CrossRef] [Green Version]
- Seaman, S. Dressing Selection in Chronic Wound Management. J. Am. Podiatr. Med. Assoc. 2002, 92, 24–33. [Google Scholar] [CrossRef]
- Korting, H.; Schöllmann, C.; White, R. Management of Minor Acute Cutaneous Wounds: Importance of Wound Healing in a Moist Environment: Acute Wounds and Healing. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 130–137. [Google Scholar] [CrossRef]
- Lazarus, G.S.; Cooper, D.M.; Knighton, D.R.; Margolis, D.J.; Percoraro, R.E.; Rodeheaver, G.; Robson, M.C. Definitions and Guidelines for Assessment of Wounds and Evaluation of Healing. Wound Repair Regen. 1994, 2, 165–170. [Google Scholar] [CrossRef]
- Dai, C.; Shih, S.; Khachemoune, A. Skin Substitutes for Acute and Chronic Wound Healing: An Updated Review. J. Dermatol. Treat. 2020, 31, 639–648. [Google Scholar] [CrossRef]
- Koehler, J.; Brandl, F.P.; Goepferich, A.M. Hydrogel Wound Dressings for Bioactive Treatment of Acute and Chronic Wounds. Eur. Polym. J. 2018, 100, 1–11. [Google Scholar] [CrossRef]
- Dissemond, J.; Kröger, K.; Initiative Chronische Wunden, e.V. Chronische Wunden: Diagnostik-Therapie-Versorgung; Urban & Fischer Verlag/Elsevier GmbH: München, Germany, 2019. [Google Scholar]
- Zhao, R.; Liang, H.; Clarke, E.; Jackson, C.; Xue, M. Inflammation in Chronic Wounds. Int. J. Mol. Sci. 2016, 17, 2085. [Google Scholar] [CrossRef] [PubMed]
- Smith, F.; Sharp, A. Undertaking a Person-Centred Assessment of Patients with Chronic Wounds. Nurs. Stand. 2019, 34, 77–82. [Google Scholar] [CrossRef] [Green Version]
- Boateng, J. Therapeutic Dressings and Wound Healing Applications. In Advances in Pharmaceutical Technology, 1st ed.; Wiley: Hoboken, NJ, USA, 2020; ISBN 978-1-119-43326-2. [Google Scholar]
- Morton, L.M.; Phillips, T.J. Wound Healing and Treating Wounds. J. Am. Acad. Dermatol. 2016, 74, 589–605. [Google Scholar] [CrossRef] [PubMed]
- Winter, G.D. Formation of the Scab and the Rate of Epithelization of Superficial Wounds in the Skin of the Young Domestic Pig. Nature 1962, 193, 293–294. [Google Scholar] [CrossRef] [PubMed]
- Nuutila, K.; Eriksson, E. Moist Wound Healing with Commonly Available Dressings. Adv. Wound Care 2021, 10, 685–698. [Google Scholar] [CrossRef] [PubMed]
- Benbow, M. Exploring the Concept of Moist Wound Healing and Its Application in Practice. Br. J. Nurs. 2008, 17, S4–S16. [Google Scholar] [CrossRef]
- Constantine, B.E.; Bolton, L.L. A Wound Model for Ischemic Ulcers in the Guinea Pig. Arch. Dermatol. Res. 1986, 278, 429–431. [Google Scholar] [CrossRef]
- Madden, M.R.; Nolan, E.; Finkelstein, J.L.; Yurt, R.W.; Smeland, J.; Goodwin, C.W.; Hefton, J.; Staiano-Coico, L. Comparison of an Occlusive and a Semi-Occlusive Dressing and the Effect of the Wound Exudate upon Keratinocyte Proliferation. J. Trauma 1989, 29, 924–930. [Google Scholar] [CrossRef]
- Katz, M.H.; Alvarez, A.F.; Kirsner, R.S.; Eaglstein, W.H.; Falanga, V. Human Wound Fluid from Acute Wounds Stimulates Fibroblast and Endothelial Cell Growth. J. Am. Acad. Dermatol. 1991, 25, 1054–1058. [Google Scholar] [CrossRef]
- Leipziger, L.S.; Glushko, V.; DiBernardo, B.; Shafaie, F.; Noble, J.; Nichols, J.; Alvarez, O.M. Dermal Wound Repair: Role of Collagen Matrix Implants and Synthetic Polymer Dressings. J. Am. Acad. Dermatol. 1985, 12, 409–419. [Google Scholar] [CrossRef]
- Sharman, D. Moist Wound Healing: A Review of Evidence, Application and Outcome. Diabet. Foot 2003, 6, 5. [Google Scholar]
- Powers, J.G.; Morton, L.M.; Phillips, T.J. Dressings for Chronic Wounds: Dressings. Dermatol. Ther. 2013, 26, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Wiegand, C.; Hipler, U.-C.; Elsner, P.; Tittelbach, J. Clinical Efficacy of Dressings for Treatment of Heavily Exuding Chronic Wounds. Chronic Wound Care Manag. Res. 2015, 2, 101. [Google Scholar] [CrossRef] [Green Version]
- Si, H.; Xing, T.; Ding, Y.; Zhang, H.; Yin, R.; Zhang, W. 3D Bioprinting of the Sustained Drug Release Wound Dressing with Double-Crosslinked Hyaluronic-Acid-Based Hydrogels. Polymers 2019, 11, 1584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, Y.; Zhang, H.; Yang, S.; Xi, Z.; Tang, T.; Yin, R.; Zhang, W. Electrospun PLGA Membrane Incorporated with Andrographolide-Loaded Mesoporous Silica Nanoparticles for Sustained Antibacterial Wound Dressing. Nanomedicine 2018, 13, 2881–2899. [Google Scholar] [CrossRef] [PubMed]
- De Pieri, A.; Byerley, A.M.; Musumeci, C.R.; Salemizadehparizi, F.; Vanderhorst, M.A.; Wuertz-Kozak, K. Electrospinning and 3D Bioprinting for Intervertebral Disc Tissue Engineering. JOR Spine 2020, 3, e1117. [Google Scholar] [CrossRef]
- Vowden, K.; Vowden, P. Wound Dressings: Principles and Practice. Surgery 2014, 32, 462–467. [Google Scholar]
- Dhivya, S.; Padma, V.V.; Santhini, E. Wound Dressings—A Review. BioMedicine 2015, 5, 22. [Google Scholar] [CrossRef]
- Tudoroiu, E.-E.; Dinu-Pîrvu, C.-E.; Albu Kaya, M.G.; Popa, L.; Anuța, V.; Prisada, R.M.; Ghica, M.V. An Overview of Cellulose Derivatives-Based Dressings for Wound-Healing Management. Pharmaceuticals 2021, 14, 1215. [Google Scholar] [CrossRef]
- Klemm, D.; Kramer, F.; Moritz, S.; Lindström, T.; Ankerfors, M.; Gray, D.; Dorris, A. Nanocellulosen: Eine neue Familie naturbasierter Materialien. Angew. Chem. 2011, 123, 5550–5580. [Google Scholar] [CrossRef]
- Klemm, D.; Petzold-Welcke, K.; Kramer, F.; Richter, T.; Raddatz, V.; Fried, W.; Nietzsche, S.; Bellmann, T.; Fischer, D. Biotech Nanocellulose: A Review on Progress in Product Design and Today’s State of Technical and Medical Applications. Carbohydr. Polym. 2021, 254, 117313. [Google Scholar] [CrossRef]
- Kralisch, D.; Hessler, N.; Klemm, D.; Erdmann, R.; Schmidt, W. White Biotechnology for Cellulose Manufacturing—The HoLiR Concept. Biotechnol. Bioeng. 2010, 105, 740–747. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, J.; Gultekinoglu, M.; Edirisinghe, M. Bacterial Cellulose Micro-Nano Fibres for Wound Healing Applications. Biotechnol. Adv. 2020, 41, 107549. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.; Sun, Q.; Han, Z.; Li, J.; Liao, B.; Hu, L.; Huang, J.; Zou, C.; Jia, C.; Huang, J.; et al. Comparison of Bacterial Nanocellulose Produced by Different Strains under Static and Agitated Culture Conditions. Carbohydr. Polym. 2020, 227, 115323. [Google Scholar] [CrossRef] [PubMed]
- Beekmann, U.; Zahel, P.; Karl, B.; Schmölz, L.; Börner, F.; Gerstmeier, J.; Werz, O.; Lorkowski, S.; Wiegand, C.; Fischer, D.; et al. Modified Bacterial Cellulose Dressings to Treat Inflammatory Wounds. Nanomaterials 2020, 10, 2508. [Google Scholar] [CrossRef]
- Beekmann, U.; Schmölz, L.; Lorkowski, S.; Werz, O.; Thamm, J.; Fischer, D.; Kralisch, D. Process Control and Scale-up of Modified Bacterial Cellulose Production for Tailor-Made Anti-Inflammatory Drug Delivery Systems. Carbohydr. Polym. 2020, 236, 116062. [Google Scholar] [CrossRef]
- Wiegand, C.; Moritz, S.; Hessler, N.; Kralisch, D.; Wesarg, F.; Müller, F.A.; Fischer, D.; Hipler, U.-C. Antimicrobial Functionalization of Bacterial Nanocellulose by Loading with Polihexanide and Povidone-Iodine. J. Mater. Sci. Mater. Med. 2015, 26, 245. [Google Scholar] [CrossRef]
- Picheth, G.F.; Pirich, C.L.; Sierakowski, M.R.; Woehl, M.A.; Sakakibara, C.N.; de Souza, C.F.; Martin, A.A.; da Silva, R.; de Freitas, R.A. Bacterial Cellulose in Biomedical Applications: A Review. Int. J. Biol. Macromol. 2017, 104, 97–106. [Google Scholar] [CrossRef]
- Czaja, W.; Krystynowicz, A.; Bielecki, S.; Brownjr, R. Microbial Cellulose—The Natural Power to Heal Wounds. Biomaterials 2006, 27, 145–151. [Google Scholar] [CrossRef]
- Sulaeva, I.; Henniges, U.; Rosenau, T.; Potthast, A. Bacterial Cellulose as a Material for Wound Treatment: Properties and Modifications. A Review. Biotechnol. Adv. 2015, 33, 1547–1571. [Google Scholar] [CrossRef]
- He, W.; Wu, J.; Xu, J.; Mosselhy, D.A.; Zheng, Y.; Yang, S. Bacterial Cellulose: Functional Modification and Wound Healing Applications. Adv. Wound Care 2021, 10, 623–640. [Google Scholar] [CrossRef]
- Portela, R.; Leal, C.R.; Almeida, P.L.; Sobral, R.G. Bacterial Cellulose: A Versatile Biopolymer for Wound Dressing Applications. Microb. Biotechnol. 2019, 12, 586–610. [Google Scholar] [CrossRef] [PubMed]
- Pang, M.; Huang, Y.; Meng, F.; Zhuang, Y.; Liu, H.; Du, M.; Ma, Q.; Wang, Q.; Chen, Z.; Chen, L.; et al. Application of Bacterial Cellulose in Skin and Bone Tissue Engineering. Eur. Polym. J. 2020, 122, 109365. [Google Scholar] [CrossRef]
- Sanchavanakit, N.; Sangrungraungroj, W.; Kaomongkolgit, R.; Banaprasert, T.; Pavasant, P.; Phisalaphong, M. Growth of Human Keratinocytes and Fibroblasts on Bacterial Cellulose Film. Biotechnol. Prog. 2006, 22, 1194–1199. [Google Scholar] [CrossRef] [PubMed]
- Kwak, M.H.; Kim, J.E.; Go, J.; Koh, E.K.; Song, S.H.; Son, H.J.; Kim, H.S.; Yun, Y.H.; Jung, Y.J.; Hwang, D.Y. Bacterial Cellulose Membrane Produced by Acetobacter Sp. A10 for Burn Wound Dressing Applications. Carbohydr. Polym. 2015, 122, 387–398. [Google Scholar] [CrossRef]
- Li, Y.; Wang, S.; Huang, R.; Huang, Z.; Hu, B.; Zheng, W.; Yang, G.; Jiang, X. Evaluation of the Effect of the Structure of Bacterial Cellulose on Full Thickness Skin Wound Repair on a Microfluidic Chip. Biomacromolecules 2015, 16, 780–789. [Google Scholar] [CrossRef] [PubMed]
- Holzer, J.C.J.; Tiffner, K.; Kainz, S.; Reisenegger, P.; de Mattos, I.B.; Funk, M.; Lemarchand, T.; Laaff, H.; Bal, A.; Birngruber, T.; et al. A Novel Human Ex-Vivo Burn Model and the Local Cooling Effect of a Bacterial Nanocellulose-Based Wound Dressing. Burns 2020, 46, 1924–1932. [Google Scholar] [CrossRef]
- Jones, E.M.; Cochrane, C.A.; Percival, S.L. The Effect of PH on the Extracellular Matrix and Biofilms. Adv. Wound Care 2015, 4, 431–439. [Google Scholar] [CrossRef]
- Pourali, P.; Razavianzadeh, N.; Khojasteh, L.; Yahyaei, B. Assessment of the Cutaneous Wound Healing Efficiency of Acidic, Neutral and Alkaline Bacterial Cellulose Membrane in Rat. J. Mater. Sci. Mater. Med. 2018, 29, 90. [Google Scholar] [CrossRef]
- Hoff, J.; Karl, B.; Gerstmeier, J.; Beekmann, U.; Schmölz, L.; Börner, F.; Kralisch, D.; Bauer, M.; Werz, O.; Fischer, D.; et al. Controlled Release of the α-Tocopherol-Derived Metabolite α-13′-Carboxychromanol from Bacterial Nanocellulose Wound Cover Improves Wound Healing. Nanomaterials 2021, 11, 1939. [Google Scholar] [CrossRef]
- Maurer, K.; Renkert, M.; Duis, M.; Weiss, C.; Wessel, L.M.; Lange, B. Application of Bacterial Nanocellulose-Based Wound Dressings in the Management of Thermal Injuries: Experience in 92 Children. Burns 2021, 48, 608–614. [Google Scholar] [CrossRef]
- Resch, A.; Staud, C.; Radtke, C. Nanocellulose-based Wound Dressing for Conservative Wound Management in Children with Second-degree Burns. Int. Wound J. 2021, 18, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Schiefer, J.L.; Aretz, G.F.; Fuchs, P.C.; Bagheri, M.; Funk, M.; Schulz, A.; Daniels, M. Comparison of Wound Healing and Patient Comfort in Partial-thickness Burn Wounds Treated with SUPRATHEL and Epicte hydro Wound Dressings. Int. Wound J. 2021, 19, 782–790. [Google Scholar] [CrossRef] [PubMed]
- Cattelaens, J.; Turco, L.; Berclaz, L.M.; Huelsse, B.; Hitzl, W.; Vollkommer, T.; Bodenschatz, K.J. The Impact of a Nanocellulose-Based Wound Dressing in the Management of Thermal Injuries in Children: Results of a Retrospective Evaluation. Life 2020, 10, 212. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, O.M.; Patel, M.; Booker, J.; Markowitz, L. Effectiveness of a Biocellulose Wound Dressing for the Treatment of Chronic Venous Leg Ulcers: Results of a Single Center Randomized Study Involving 24 Patients. Wounds Compend. Clin. Res. Pract. 2004, 16, 224–233. [Google Scholar]
- Vowden, K.; Vowden, P. Understanding Exudate Management and the Role of Exudate in the Healing Process. Br. J. Community Nurs. 2003, 8, S4–S13. [Google Scholar] [CrossRef]
- Bishop, S.M.; Walker, M.; Rogers, A.A.; Chen, W.Y.J. Importance of Moisture Balance at the Wound-Dressing Interface. J. Wound Care 2003, 12, 125–128. [Google Scholar] [CrossRef]
- Kim, Y.; Doh, S.J.; Lee, G.D.; Kim, C.; Im, J.N. Composite Nonwovens Based on Carboxymethyl Cellulose for Wound Dressing Materials. Fibers Polym. 2019, 20, 2048–2056. [Google Scholar] [CrossRef]
- Thomas, S. Technical Report: An ‘In-Vitro’ Comparison of the Physical Characteristics of Hydrocolloids, Hydrogels, Foams, and Alginate/CMC Fibrous Dressings; Surgical Materials Testing Laboratory: Bridgend, UK, 2005. [Google Scholar]
- Lee, S.M.; Park, I.K.; Kim, Y.S.; Kim, H.J.; Moon, H.; Mueller, S.; Jeong, Y.-I. Physical, Morphological, and Wound Healing Properties of a Polyurethane Foam-Film Dressing. Biomater. Res. 2016, 20, 15. [Google Scholar] [CrossRef] [Green Version]
- Körber, A.; Weindorf, M.; Dissemond, J. Exudate capacity of modern wound dressings during compression therapy for chronic venous leg ulcers. Hautarzt 2008, 59, 904–911. [Google Scholar] [CrossRef]
- Dissemond, J.; Assenheimer, B.; Bültemann, A.; Gerber, V.; Gretener, S.; Kohler-von Siebenthal, E.; Koller, S.; Kröger, K.; Kurz, P.; Läuchli, S.; et al. Compression Therapy in Patients with Venous Leg Ulcers. JDDG J. Ger. Soc. Dermatol. 2016, 14, 1073–1089. [Google Scholar] [CrossRef]
- Lurie, F.; Bittar, S.; Kasper, G. Optimal Compression Therapy and Wound Care for Venous Ulcers. Surg. Clin. N. Am. 2018, 98, 349–360. [Google Scholar] [CrossRef] [PubMed]
- Linnitt, N.; Jones, J. Indications for Deciding Compression in the Treatment of Chronic Oedema. Br. J. Community Nurs. 2012, 17, S11–S15. [Google Scholar] [CrossRef]
- Walker, M.; Lam, S.; Pritchard, D.; Cochrane, C.A. Biophysical Properties of a Hydrofiber® Cover Dressing. Wounds UK 2010, 6, 9. [Google Scholar]
- Wu, P.; Nelson, E.A.; Reid, W.H.; Ruckley, C.V.; Gaylor, J.D.S. Water Vapour Transmission Rates in Burns and Chronic Leg Ulcers: Influence of Wound Dressings and Comparison with in Vitro Evaluation. Biomaterials 1996, 17, 1373–1377. [Google Scholar] [CrossRef]
- Browning, P.; White, R.J.; Rowell, T. Comparative Evaluation of the Functional Properties of Superabsorbent Dressings and Their Effect on Exudate Management. J. Wound Care 2016, 25, 452–462. [Google Scholar] [CrossRef] [Green Version]
- Zehrer, C.L.; Holm, D.; Solfest, S.E.; Walters, S.-A. A Comparison of the in Vitro Moisture Vapour Transmission Rate and in Vivo Fluid-Handling Capacity of Six Adhesive Foam Dressings to a Newly Reformulated Adhesive Foam Dressing: Comparison of Fluid-Handling Capacity of Adhesive Foam Dressings. Int. Wound J. 2014, 11, 681–690. [Google Scholar] [CrossRef]
- Thomas, S. A Review of the Physical, Biological and Clinical Properties of a Bacterial Cellulose Wound. J. Wound Care 2008, 17, 349–352. [Google Scholar] [CrossRef]
- Rajendran, S. Advanced Textiles for Wound Care, 2nd ed.; Woodhead Publishing: Duxford, UK, 2019; ISBN 978-0-08-102192-7. [Google Scholar]
- Wu, P.; Fisher, A.; Foo, P.P.; Queen, D.; Gaylor, J.D.S. In Vitro Assessment of Water Vapour Transmission of Synthetic Wound Dressings. Biomaterials 1995, 16, 5. [Google Scholar] [CrossRef]
- Queen, D.; Gaylor, J.D.S.; Evans, J.H.; Courtney, J.M.; Reid, W.H. The Preclinical Evaluation of the Water Vapour Transmission Rate through Burn Wound Dressings. Biomaterials 1987, 8, 367–371. [Google Scholar] [CrossRef]
- Xu, R.; Xia, H.; He, W.; Li, Z.; Zhao, J.; Liu, B.; Wang, Y.; Lei, Q.; Kong, Y.; Bai, Y.; et al. Controlled Water Vapor Transmission Rate Promotes Wound-Healing via Wound Re-Epithelialization and Contraction Enhancement. Sci. Rep. 2016, 6, 24596. [Google Scholar] [CrossRef] [Green Version]
- White, R.; Cutting, K.F. Modern Exudate Management: A Review of Wound Treatments. Available online: http://www.worldwidewounds.com/2006/september/White/Modern-Exudate-Mgt (accessed on 11 October 2021).
- Lohmann & Rauscher GmbH & Co. KG Product Information “Suprasorb G”. Available online: https://www.lohmann-rauscher.com/en/products/wound-care/modern-wound-care/suprasorb-g-gel-dressing/ (accessed on 8 November 2021).
- Hestrin, S.; Schramm, M. Synthesis of Cellulose by Acetobacter Xylinum. II. Preparation of Freeze-Dried Cells Capable of Polymerizing Glucose to Cellulose. Biochem. J. 1954, 58, 345–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CEN/TC 205 Draft PrEN 13726:2021; Test Methods for Wound Dressings—Aspects of Absorbency and Moisture Vapour Transmission, Waterproofness and Conformability. Beuth: Brussels, Belgium, 2021.
- CEN/TC 205 EN 13726-1:2002; EN 13726-2:2002; Test Methods for Primary Wound Dressings. Beuth: Brussels, Belgium, 2002.
- Jonkman, J.E.N.; Cathcart, J.A.; Xu, F.; Bartolini, M.E.; Amon, J.E.; Stevens, K.M.; Colarusso, P. An Introduction to the Wound Healing Assay Using Live-Cell Microscopy. Cell Adhes. Migr. 2014, 8, 440–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portal, O.; Clark, W.A.; Levinson, D.J. Microbial Cellulose Wound Dressing in the Treatment of Nonhealing Lower Extremity Ulcers. Wounds Compend. Clin. Res. Pract. 2009, 2, 1–3. [Google Scholar]
- Solway, D.R.; Clark, W.A.; Levinson, D.J. A Parallel Open-Label Trial to Evaluate Microbial Cellulose Wound Dressing in the Treatment of Diabetic Foot Ulcers. Int. Wound J. 2011, 8, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Dini, V.; Romanelli, M.; Andriessen, A.; Barbanera, S.; Bertone, M.S.; Brilli, C.; Abel, M. Improvement of Periulcer Skin Condition in Venous Leg Ulcer Patients: Prospective, Randomized, Controlled, Single-Blinded Clinical Trial Comparing a Biosynthetic Cellulose Dressing with a Foam Dressing. Adv. Ski. Wound Care 2013, 26, 8. [Google Scholar] [CrossRef]
- Cavalcanti, L.M.; Pinto, F.C.M.; Oliveira, G.M.D.; Lima, S.V.C.; Aguiar, J.L.D.A.; Lins, E.M. Efficacy of Bacterial Cellulose Membrane for the Treatment of Lower Limbs Chronic Varicose Ulcers: A Randomized and Controlled Trial. Rev. Colégio Bras. Cir. 2017, 44, 72–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colenci, R.; Miot, H.A.; Marques, M.E.A.; Schmitt, J.V.; Basmaji, P.; Jacinto, J. dos S.; Abbade, L.P.F. Cellulose Biomembrane versus Collagenase Dressing for the Treatment of Chronic Venous Ulcers: A Randomized, Controlled Clinical Trial. Eur. J. Dermatol. 2019, 29, 387–395. [Google Scholar] [CrossRef]
- Maia, A.L.; Lins, E.M.; Aguiar, J.L.A.; Pinto, F.C.M.; Rocha, F.A.; Batista, L.L.; Fernandes, W.R. de M.A. Curativo Com Filme e Gel de Biopolímero de Celulose Bacteriana No Tratamento de Feridas Isquêmicas Após Revascularização de Membros Inferiores. Rev. Colégio Bras. Cir. 2019, 46, e20192260. [Google Scholar] [CrossRef] [Green Version]
- Piatkowski, A.; Drummer, N.; Andriessen, A.; Ulrich, D.; Pallua, N. Randomized Controlled Single Center Study Comparing a Polyhexanide Containing Bio-Cellulose Dressing with Silver Sulfadiazine Cream in Partial-Thickness Dermal Burns. Burns 2011, 37, 800–804. [Google Scholar] [CrossRef]
- Aboelnaga, A.; Elmasry, M.; Adly, O.A.; Elbadawy, M.A.; Abbas, A.H.; Abdelrahman, I.; Salah, O.; Steinvall, I. Microbial Cellulose Dressing Compared with Silver Sulphadiazine for the Treatment of Partial Thickness Burns: A Prospective, Randomised, Clinical Trial. Burns 2018, 44, 1982–1988. [Google Scholar] [CrossRef]
- delli Santi, G.; Borgognone, A. The Use of Epiprotect®, an Advanced Wound Dressing, to Heal Paediatric Patients with Burns: A Pilot Study. Burns Open 2019, 3, 103–107. [Google Scholar] [CrossRef]
- Karlsson, M.; Olofsson, P.; Steinvall, I.; Sjöberg, F.; Thorfinn, J.; Elmasry, M. Three Years’ Experience of a Novel Biosynthetic Cellulose Dressing in Burns. Adv. Wound Care 2019, 8, 71–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanks, L.A.; Cronshaw, A.; Alexander, K.S.; Davies, J.A.; O’Boyle, C.P. Evaluation of EpiProtect® Microbial Cellulose Burns Dressings in Young Children. Scars Burns Heal. 2020, 6, 205951312094050. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Wound Dressing | Solid Content | Free Swell Absorptive Capacity (0.5 h; 2 h; 24 h) | Absorptive Capacity under Pressure | MVTR In Contact With Vapor | MVTR in Contact with Liquid | Fluid Donation to Gelatin |
|---|---|---|---|---|---|---|
| Unit | % | g/100 cm2 | g/100 cm2 | g/m2/24 h | g/m2/24 h | g/100 cm2 |
| ALG | - | 17.6 ± 1.3 | 11.0 ± 1.4 | 6135 ± 78 | - | - |
| 18.0 ± 1.1 | ||||||
| 18.4 ± 1.1 | ||||||
| CMC | - | 20.1 ± 1.7 | 17.2 ± 0.5 | 6844 ± 282 | - | - |
| 20.3 ± 1.7 | ||||||
| 21.0 ± 1.3 | ||||||
| HC | - | 3.9 ± 0.3 | 3.0 ± 0.9 | 98 ± 5 | 330 ± 42 | - |
| 6.0 ± 0.4 | ||||||
| 15.2 ± 1.1 | ||||||
| FOAM_1 | - | 82.0 ± 2.9 | 35.3 ± 2.5 | 3510 ± 225 | 12,790 ± 747 | - |
| 85.1 ± 5.4 | ||||||
| 92.5 ± 6.4 | ||||||
| FOAM_2 | - | 60.1 ± 1.6 | 32.0 ± 1.9 | 2808 ± 103 | 16,750 ± 419 | - |
| 58.6 ± 3.9 | ||||||
| 61.1 ± 3.4 | ||||||
| XBC | 3.16 ± 0.18 | 13.3 ± 0.5 | 2.2 ± 0.3 | 3458 ± 198 | 27,663 ± 959 | 9.0 ± 0.2 |
| 18.4 ± 0.9 | ||||||
| 22.1 ± 1.2 | ||||||
| BC_A | 1.57 ± 0.10 | 6.7 ± 0.5 | −2.9 ± 2.2 | 4039 ± 230 | 27,648 ± 488 | 18.9 ± 1.8 |
| 8.7 ± 0.8 | ||||||
| 9.9 ± 0.9 | ||||||
| BC_C1 | 3.27 ± 0.27 | 23.2 ± 5.1 | 1.7 ± 0.5 | 2697 ± 118 | 26,334 ± 1465 | 19.1 ± 1.7 |
| 31.2 ± 5.6 | ||||||
| 36.1 ± 5.7 | ||||||
| BC_C2 | 8.20 ± 0.57 | 30.1 ± 6.3 | 13.1 ± 1.5 | 2908 ± 95 | 27,212 ± 913 | 3.0 ± 0.3 |
| 37.4 ± 6.5 | ||||||
| 43.9 ± 7.7 | ||||||
| GEL | - | - | - | - | - | 2.0 ± 0.9 |
| Male | Female | ||
| Sex | 22 | 22 | |
| Mean | Median | SD | |
| Patient Age [years] | 66.9 | 71 | 15.94 |
| Wound Age [weeks] | 66.56 | 13 | 120.04 |
| Yes | Not specified | ||
| Diagnosis of underlying disease | 42 | 2 | |
| Treatment of underlying disease | 29 | 15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zahel, P.; Beekmann, U.; Eberlein, T.; Schmitz, M.; Werz, O.; Kralisch, D. Bacterial Cellulose—Adaptation of a Nature-Identical Material to the Needs of Advanced Chronic Wound Care. Pharmaceuticals 2022, 15, 683. https://doi.org/10.3390/ph15060683
Zahel P, Beekmann U, Eberlein T, Schmitz M, Werz O, Kralisch D. Bacterial Cellulose—Adaptation of a Nature-Identical Material to the Needs of Advanced Chronic Wound Care. Pharmaceuticals. 2022; 15(6):683. https://doi.org/10.3390/ph15060683
Chicago/Turabian StyleZahel, Paul, Uwe Beekmann, Thomas Eberlein, Michael Schmitz, Oliver Werz, and Dana Kralisch. 2022. "Bacterial Cellulose—Adaptation of a Nature-Identical Material to the Needs of Advanced Chronic Wound Care" Pharmaceuticals 15, no. 6: 683. https://doi.org/10.3390/ph15060683
APA StyleZahel, P., Beekmann, U., Eberlein, T., Schmitz, M., Werz, O., & Kralisch, D. (2022). Bacterial Cellulose—Adaptation of a Nature-Identical Material to the Needs of Advanced Chronic Wound Care. Pharmaceuticals, 15(6), 683. https://doi.org/10.3390/ph15060683