
Cytokine Level Changes in Schizophrenia Patients with and without Metabolic Syndrome Treated with Atypical Antipsychotics

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Results and Discussion
2.1. Baseline Characteristics of Study Participants
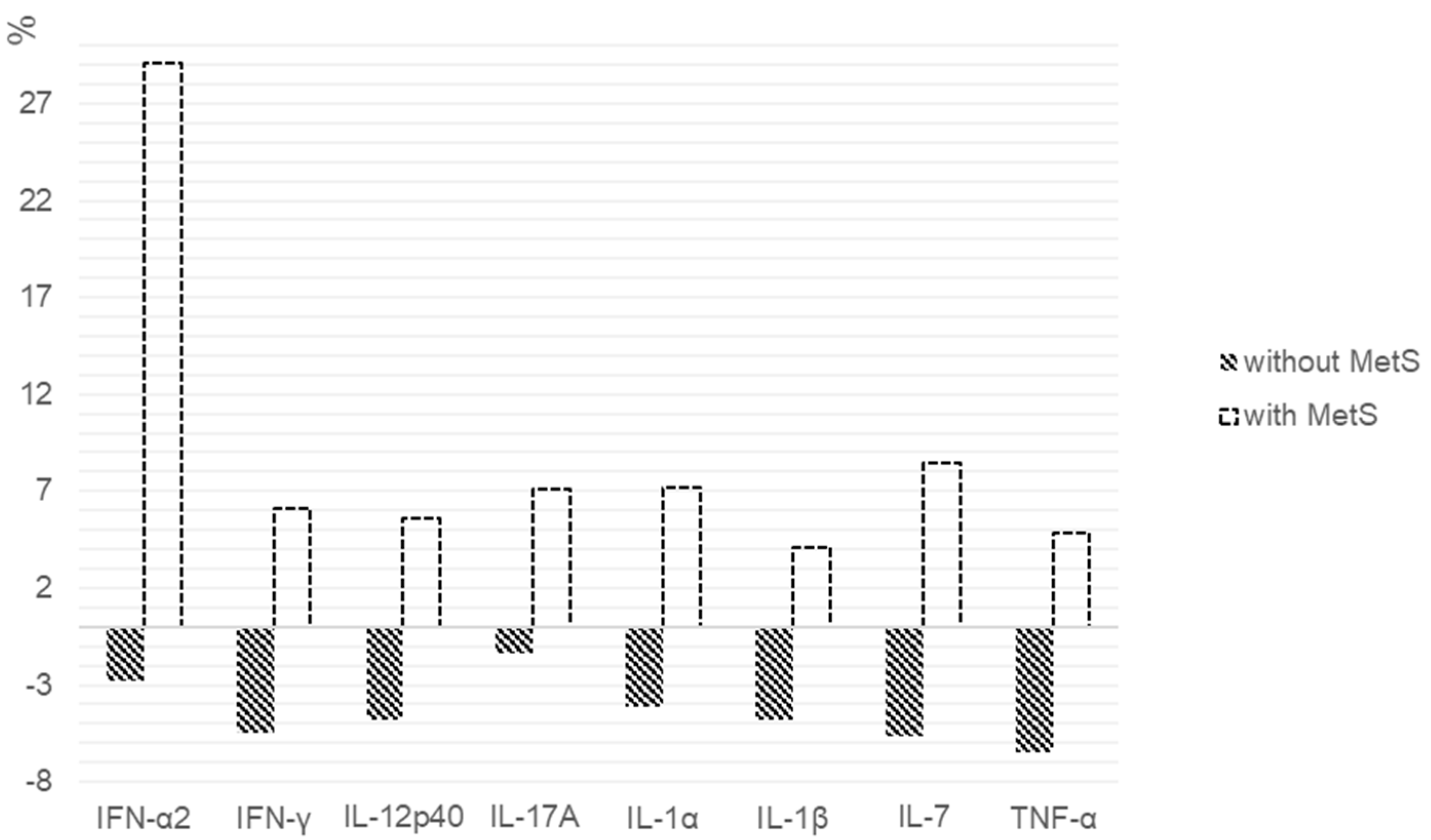
2.2. Cytokine Levels Depending on the Presence of MetS in Patients with Schizophrenia Receiving SGA
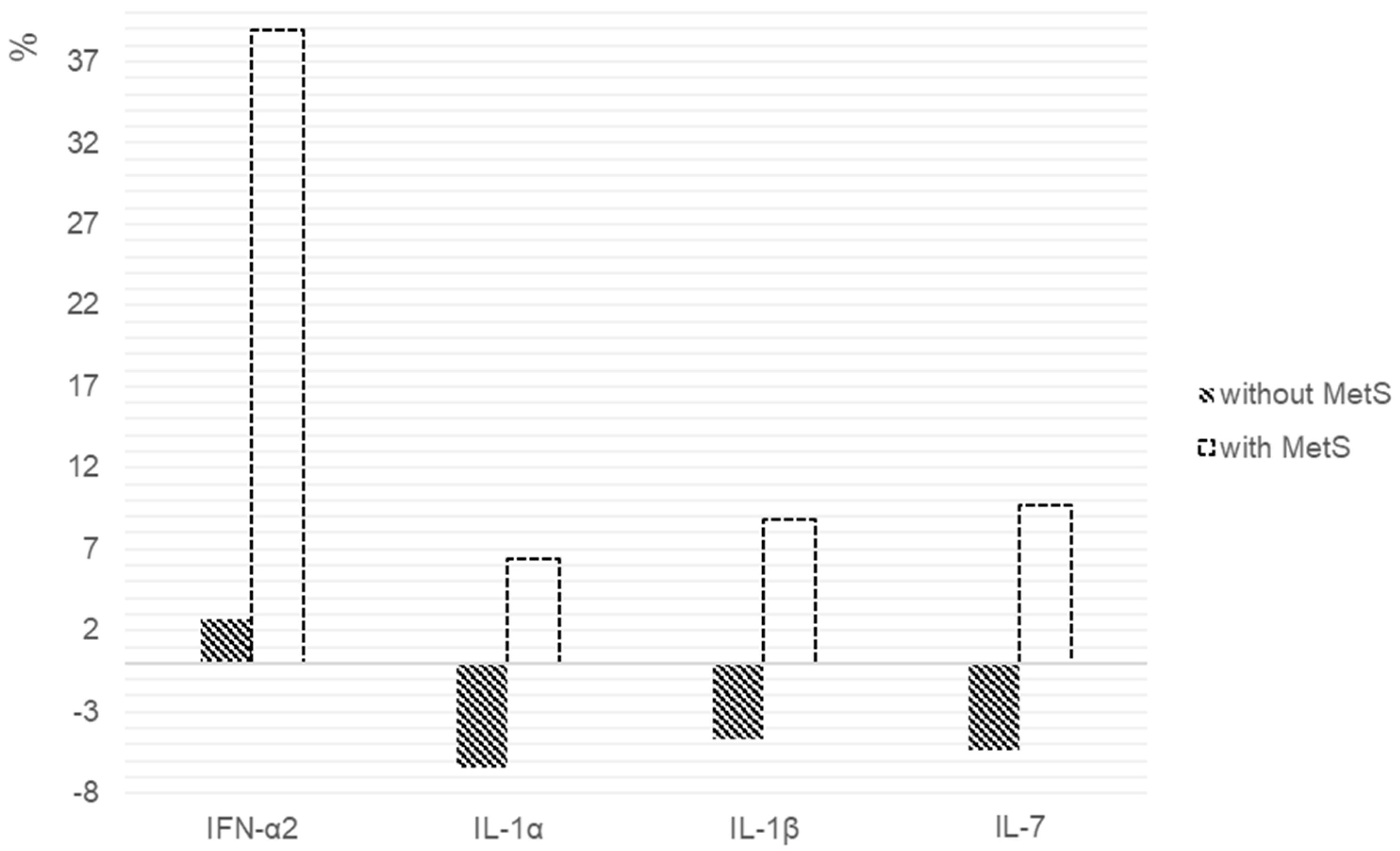
2.3. Cytokine Levels in Patients with Schizophrenia Depending on the Presence of MetS When Receiving Risperidone
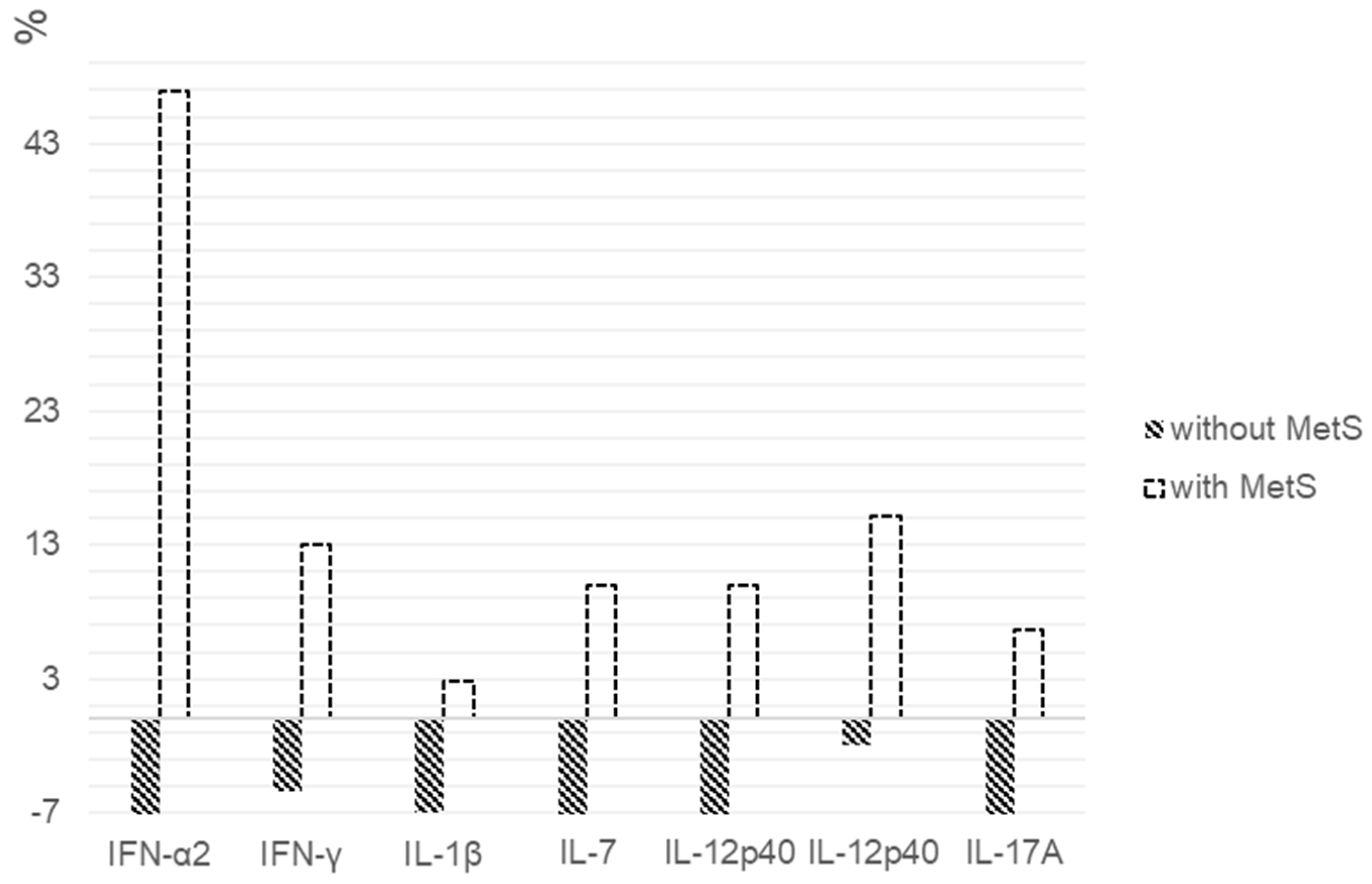
2.4. Cytokine Levels in Patients with Schizophrenia Depending on the Presence of MetS When Receiving Quetiapine or Olanzapine
2.5. Cytokine Levels in Patients with Schizophrenia Depending on the Presence of MetS When Receiving Aripiprazole
3. Materials and Methods
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marques, T.; Ashok, A.; Pillinger, T.; Veronese, M.; Turkheimer, F.; Dazzan, P.; Sommer, I.; Howes, O. Neuroinflammation in schizophrenia: Meta-analysis of in vivo microglial imaging studies. Psychol. Med. 2019, 49, 2186–2196. [Google Scholar] [CrossRef]
- Van Kesteren, C.; Gremmels, H.; De Witte, L.; Hol, E.; Van Gool, A.; Falkai, P.; Kahn, R.; Sommer, I. Immune involvement in the pathogenesis of schizophrenia: A meta-analysis on postmortem brain studies. Transl. Psychiatry 2017, 7, 1075. [Google Scholar] [CrossRef]
- Müller, N. Inflammation in schizophrenia: Pathogenetic aspects and therapeutic considerations. Schizophr. Bull. 2018, 44, 973–982. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, J.; Nutma, E.; van der Valk, P.; Amor, S. Inflammation in CNS neurodegenerative diseases. Immunology 2018, 154, 204–219. [Google Scholar] [CrossRef]
- Upthegrove, R.; Khandaker, G. Cytokines, oxidative stress and cellular markers of inflammation in schizophrenia. Curr. Top. Behav. Neurosci. 2019, 44, 49–66. [Google Scholar] [CrossRef]
- Miller, B.; Buckley, P.; Seabolt, W.; Mellor, A.; Kirkpatrick, B. Meta-analysis of cytokine alterations in schizophrenia: Clinical status and antipsychotic effects. Biol. Psychiatry 2011, 70, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Monji, A.; Mizoguchi, Y.; Hashioka, S.; Horikawa, H.; Seki, Y.; Kasai, M.; Utsumi, H.; Kanba, S. Anti-Inflammatory properties of antipsychotics via microglia modulations: Are antipsychotics a ’fire extinguisher’ in the brain of schizophrenia? Mini Rev. Med. Chem. 2011, 11, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Dinesh, A.; Islam, J.; Khan, J.; Turkheimer, F.; Vernon, A. Effects of Antipsychotic Drugs: Cross Talk Between the Nervous and Innate Immune System. CNS Drugs 2020, 34, 1229–1251. [Google Scholar] [CrossRef] [PubMed]
- Baumeister, D.; Ciufolini, S.; Mondelli, V. Effects of psychotropic drugs on inflammation: Consequence or mediator of therapeutic effects in psychiatric treatment? Psychopharmacology 2016, 233, 1575–1589. [Google Scholar] [CrossRef]
- Debnath, M.; Venkatasubramanian, G. Recent advances in psychoneuroimmunology relevant to schizophrenia therapeutics. Curr. Opin. Psychiatry 2013, 26, 433–439. [Google Scholar] [CrossRef]
- Müller, N.; Riedel, M.; Schwarz, M. Psychotropic effects of COX-2 inhibitors--a possible new approach for the treatment of psychiatric disorders. Pharmacopsychiatry 2004, 37, 266–269. [Google Scholar] [CrossRef]
- Hong, J.; Bang, M. Anti-inflammatory Strategies for Schizophrenia: A Review of Evidence for Therapeutic Applications and Drug Repurposing. Clin. Psychopharmacol. Neurosci. 2020, 18, 10–24. [Google Scholar] [CrossRef]
- Na, K.S.; Jung, H.Y.; Kim, Y.K. The role of pro-inflammatory cytokines in the neuroinflammation and neurogenesis of schizophrenia. Prog. Neuropsychopharmacol. Biol. Psychiatry 2014, 48, 277–286. [Google Scholar] [CrossRef]
- Mitchell, A.; Vancampfort, D.; Sweers, K.; van Winkel, R.; Yu, W.; De Hert, M. Prevalence of metabolic syndrome and metabolic abnormalities in schizophrenia and related disorders--a systematic review and meta-analysis. Schizophr. Bull. 2013, 39, 306–318. [Google Scholar] [CrossRef]
- Sugawara, N.; Yasui-Furukori, N.; Sato, Y.; Umeda, T.; Kishida, I.; Yamashita, H.; Saito, M.; Furukori, H.; Nakagami, T.; Hatakeyama, M.; et al. Prevalence of metabolic syndrome among patients with schizophrenia in Japan. Schizophr. Res. 2010, 123, 244–250. [Google Scholar] [CrossRef]
- Lee, J.; Nurjono, M.; Wong, A.; Salim, A. Prevalence of metabolic syndrome among patients with schizophrenia in Singapore. Ann. Acad. Med. Singap. 2012, 41, 457–462. [Google Scholar]
- De Hert, M.; van Winkel, R.; Van Eyck, D.; Hanssens, L.; Wampers, M.; Scheen, A.; Peuskens, J. Prevalence of diabetes, metabolic syndrome and metabolic abnormalities in schizophrenia over the course of the illness: A cross-sectional study. Clin. Pract. Epidemiol. Ment. Health 2006, 2, 14. [Google Scholar] [CrossRef]
- Leonard, B.; Schwarz, M.; Myint, A. The metabolic syndrome in schizophrenia: Is inflammation a contributing cause? J. Psychopharmacol. 2012, 26, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Lasić, D.; Bevanda, M.; Bošnjak, N.; Uglešić, B.; Glavina, T.; Franić, T. Metabolic syndrome and inflammation markers in patients with schizophrenia and recurrent depressive disorder. Psychiatr. Danub. 2014, 6, 214–219. [Google Scholar]
- Kelly, C.W.; McEvoy, J.P.; Miller, B.J. Total and differential white blood cell counts, inflammatory markers, adipokines, and incident metabolic syndrome in phase 1 of the clinical antipsychotic trials of intervention effectiveness study. Schizophr. Res. 2019, 209, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Pandurangi, A.K.; Buckley, P.F. Inflammation, Antipsychotic Drugs, and Evidence for Effectiveness of Anti-inflammatory Agents in Schizophrenia. Curr. Top. Behav. Neurosci. 2020, 44, 227–244. [Google Scholar] [CrossRef]
- Carli, M.; Kolachalam, S.; Longoni, B.; Pintaudi, A.; Baldini, M.; Aringhieri, S.; Fasciani, I.; Annibale, P.; Maggio, R.; Scarselli, M. Atypical Antipsychotics and Metabolic Syndrome: From Molecular Mechanisms to Clinical Differences. Pharmaceuticals 2021, 14, 238. [Google Scholar] [CrossRef]
- Sárvári, A.; Veréb, Z.; Uray, I.; Fésüs, L.; Balajthy, Z. Atypical antipsychotics induce both proinflammatory and adipogenic gene expression in human adipocytes in vitro. Biochem. Biophys. Res. Commun. 2014, 450, 1383–1389. [Google Scholar] [CrossRef]
- Stapel, B.; Sieve, I.; Falk, C.S.; Bleich, S.; Hilfiker-Kleiner, D.; Kahl, K.G. Second generation atypical antipsychotics olanzapine and aripiprazole reduce expression and secretion of inflammatory cytokines in human immune cells. J. Psychiatr. Res. 2018, 105, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Yu, L.; Wang, D.; Chen, Y.; Wang, Y.; Wu, Z.; Liu, R.; Ren, J.; Tang, W.; Zhang, C. Association Between SIRT1, Cytokines, and Metabolic Syndrome in Schizophrenia Patients with Olanzapine or Clozapine Monotherapy. Front. Psychiatry 2020, 11, 602121. [Google Scholar] [CrossRef] [PubMed]
- Na, K.S.; Kim, W.H.; Jung, H.Y.; Ryu, S.G.; Min, K.J.; Park, K.C.; Kim, Y.S.; Yoon, J.S.; Ahn, Y.M.; Kim, C.E. Relationship between inflammation and metabolic syndrome following treatment with paliperidone for schizophrenia. Prog. Neuropsychopharmacol. Biol. Psychiatry 2013, 39, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Kornetova, E.G.; Kornetov, A.N.; Mednova, I.A.; Dubrovskaya, V.V.; Boiko, A.S.; Bokhan, N.A.; Loonen, A.J.M.; Ivanova, S.A. Changes in body fat and related biochemical parameters associated with atypical antipsychotic drug treatment in schizophrenia patients with or without metabolic syndrome. Front. Psychiatry 2019, 10, 803. [Google Scholar] [CrossRef]
- Jaberi, N.; Faramarzi, E.; Farahbakhsh, M.; Ostadarahimi, A.; Asghari Jafarabadi, M.; Fakhari, A. Prevalence of metabolic syndrome in schizophrenia patients treated with antipsychotic medications. Casp. J. Intern. Med. 2020, 11, 310–314. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, Q.; Reynolds, G.P.; Yue, W.; Deng, W.; Yan, H.; Tan, L.; Wang, C.; Yang, G.; Lu, T.; et al. Chinese Antipsychotics Pharmacogenomics Consortium. Metabolic Effects of 7 Antipsychotics on Patients with Schizophrenia: A Short-Term, Randomized, Open-Label, Multicenter, Pharmacologic Trial. J. Clin. Psychiatry. 2020, 81, 19m12785. [Google Scholar] [CrossRef]
- Mednova, I.A.; Boiko, A.S.; Kornetova, E.G.; Parshukova, D.A.; Semke, A.V.; Bokhan, N.A.; Loonen, A.J.M.; Ivanova, S.A. Adipocytokines and Metabolic Syndrome in Patients with Schizophrenia. Metabolites 2020, 10, 410. [Google Scholar] [CrossRef]
- Kay, S.R.; Opler, L.A.; Fiszbein, A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef]
- Papanastasiou, E. The prevalence and mechanisms of metabolic syndrome in schizophrenia: A review. Ther. Adv. Psychopharmacol. 2013, 3, 33–51. [Google Scholar] [CrossRef]
- Tourjman, V.; Kouassi, É.; Koué, M.È.; Rocchetti, M.; Fortin-Fournier, S.; Fusar-Poli, P.; Potvin, S. Antipsychotics’ effects on blood levels of cytokines in schizophrenia: A meta-analysis. Schizophr. Res. 2013, 151, 43–47. [Google Scholar] [CrossRef]
- De Witte, L.; Tomasik, J.; Schwarz, E.; Guest, P.C.; Rahmoune, H.; Kahn, R.S.; Bahn, S. Cytokine alterations in first-episode schizophrenia patients before and after antipsychotic treatment. Schizophr. Res. 2014, 154, 23–29. [Google Scholar] [CrossRef]
- Noto, C.; Ota, V.K.; Gouvea, E.S.; Rizzo, L.B.; Spindola, L.; Honda, P.H.; Cordeiro, Q.; Belangero, S.I.; Bressan, R.A.; Gadelha, A.; et al. Effects of risperidone on cytokine profile in drug-naive first-episode psychosis. Int. J. Neuropsychopharmacol. 2015, 18. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.L.; Wu, S.; Tsai, T.C.; Wang, L.K.; Tsai, F.M. Regulation of macrophage immune responses by antipsychotic drugs. Immunopharmacol. Immunotoxicol. 2013, 35, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Jaehne, E.J.; Corrigan, F.; Toben, C.; Jawahar, M.; Baune, B. The effect of the antipsychotic drug quetiapine and its metabolite norquetiapine on acute inflammation, memory and anhedonia. Pharmacol. Biochem. Behav. 2015, 135, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Wolf, A.M.; Wolf, D.; Rumpold, H.; Enrich, B.; Tilg, H. Adiponectin induces the anti-inflammatory cytokines IL-10 and IL-1RA in human leukocytes. Biochem. Biophys. Res. Commun. 2004, 323, 630–635. [Google Scholar] [CrossRef]
- Chen, C.Y.; Goh, K.K.; Chen, C.H.; Lu, M.L. The Role of Adiponectin in the Pathogenesis of Metabolic Disturbances in Patients with Schizophrenia. Front. Psychiatry 2020, 11, 605124. [Google Scholar] [CrossRef]
- Song, X.; Fan, X.; Li, X.; Zhang, W.; Gao, J.; Zhao, J.; Harrington, A.; Ziedonis, D.; Lv, L. Changes in pro-inflammatory cytokines and body weight during 6-month risperidone treatment in drug naive, first-episode schizophrenia. Psychopharmacology 2014, 231, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Korn, T.; Bettelli, E.; Oukka, M.; Kuchroo, V. IL-17 and Th17 Cells. Annu. Rev. Immunol. 2009, 27, 485–517. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Zhang, Y.; Fan, W.; Tang, W.; Zhang, C. Interleukin-17 alteration in first-episode psychosis: A meta-analysis. Mol. Neuropsychiatry 2017, 3, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Dimitrov, D.H.; Lee, S.; Yantis, J.; Valdez, C.; Paredes, R.M.; Braida, N.; Velligan, D.; Walss-Bass, C. Differential correlations between inflammatory cytokines and psychopathology in veterans with schizophrenia: Potential role for IL-17 pathway. Schizophr. Res. 2013, 151, 29–35. [Google Scholar] [CrossRef]
- Himmerich, H.; Schönherr, J.; Fulda, S.; Sheldrick, A.J.; Bauer, K.; Sack, U. Impact of antipsychotics on cytokine production in-vitro. J. Psychiatr. Res. 2011, 45, 1358–1365. [Google Scholar] [CrossRef] [PubMed]
- Sobiś, J.; Rykaczewska-Czerwińska, M.; Świętochowska, E.; Gorczyca, P. Therapeutic effect of aripiprazole in chronic schizophrenia is accompanied by anti-inflammatory activity. Pharmacol. Rep. 2015, 67, 353–359. [Google Scholar] [CrossRef]
- Yogaratnam, J.; Biswas, N.; Vadivel, R.; Jacob, R. Metabolic complications of schizophrenia and antipsychotic medications-an updated review. East Asian Arch. Psychiatry 2013, 23, 21–28. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Indicators | Patients with MetS (n = 38) | Patients without MetS (n = 63) | p-Value |
|---|---|---|---|
| Age, Me (Q1; Q3) years | 35 (30; 47) | 30 (25; 36) | 0.002 * |
| Gender (Male, n (%)/Female, n (%)) | 23 (60.5%)/15 (39.5%) | 32 (50.8%)/31 (49.2%) | 0.341 |
| Schizophrenia onset age, Me [Q1; Q3] years | 22 (19;27) | 23.5 (19;29) | 0.717 |
| Duration of disease, Me [Q1; Q3] years | 16 (5; 22) | 6 (3; 11) | <0.001 * |
| PANSS positive symptoms score | 19 (16; 23) | 19 (14; 22) | 0.405 |
| PANSS negative symptoms score | 25.5 (20; 30) | 25 (21; 28) | 0.629 |
| PANSS general psychopathology symptoms score | 51.5 (41; 54) | 52 (43; 56) | 0.735 |
| PANSS total score | 100.5 (85; 108) | 96 (86; 104) | 0.469 |
| Antipsychotic therapy duration, years | 5.5 (2; 16) | 3 (0.2; 5) | 0.002 * |
| Total antipsychotic dose, CPZeq | 389.95 (200; 600) | 360 (233; 609.75) | 0.934 |
| Smoking | 23 (60.5%) | 37 (58.7%) | 0.237 |
| Indicators | Patients with MetS (n = 38) | Patients without MetS (n = 63) | ||||
|---|---|---|---|---|---|---|
| Before | After | p-Value | Before | After | p-Value | |
| IFN-α2 | 18.07 (10.78; 26.01) | 23.54 (14.82; 33.96) | 0.010 * | 18.59 (14.22; 28.18) | 21.26 (15.38; 28.90) | 0.975 |
| IFN-γ | 10.06 (8.33; 12.04) | 11.13 (9.17; 13.80) | 0.119 | 10.85 (8.93; 13.67) | 10.12 (9.14; 11.76) | 0.011 * |
| IL-1RA | 43.68 (38.13; 58.71) | 48.79 (38.25; 64.82) | 0.713 | 48.99 (38.38; 80.99) | 47.14 (38.13; 73.21) | 0.291 |
| IL-1α | 53.51 (47.66; 60.34) | 55.74 (52.36; 63.92) | 0.024 * | 56.95 (50.02; 65.88) | 54.67 (46.51; 63.73) | 0.112 |
| IL-1β | 2.48 (1.99; 2.90) | 2.64 (2.17; 3.10) | 0.090 | 2.49 (1.88; 3.02) | 2.33 (1.70; 2.74) | 0.035 * |
| IL-2 | 4.74 (4.26; 5.12) | 4.97 (4.42; 5.82) | 0.063 | 5.15 (4.42; 6.11) | 5.29 (4.62; 5.92) | 0.986 |
| IL-3 | 3.32 (2.90; 3.68) | 3.32 (3.07; 3.73) | 0.447 | 3.28 (2.81; 4.00) | 3.52 (2.94; 4.02) | 0.517 |
| IL-4 | 75.27 (69.78; 87.86) | 80.11 (71.35; 101.36) | 0.245 | 79.28 (70.03; 97.11) | 83.80 (70.40; 93.69) | 0.866 |
| IL-5 | 2.08 (1.39; 2.47) | 1.98 (1.48; 2.66) | 0.361 | 2.11 (1.57; 2.59) | 1.98 (1.72; 2.58) | 0.464 |
| IL-6 | 6.13 (4.53; 8.18) | 5.44 (4.48; 6.95) | 0.274 | 5.94 (4.40; 9.61) | 5.16 (3.81; 7.39) | 0.043 * |
| IL-7 | 10.45 (8.98; 11.75) | 10.67 (9.62; 12.71) | 0.017 * | 10.24 (8.87; 12.19) | 9.65 (8.49; 11.96) | 0.118 |
| IL-8 | 14.25 (9.21; 19.97) | 12.55 (8.98; 28.01) | 0.258 | 12.35 (8.70; 20.70) | 11.54 (8.61; 17.71) | 0.271 |
| IL-9 | 3.73 (2.86; 4.10) | 3.84 (2.72; 4.39) | 0.845 | 3.52 (2.61; 4.36) | 3.42 (2.25; 4.10) | 0.279 |
| IL-10 | 9.11 (7.52; 11.95) | 8.92 (7.08; 10.40) | 0.572 | 7.99 (6.41; 10.81) | 7.75 (6.24; 9.83) | 0.335 |
| IL-12p40 | 44.52 (38.30; 52.44) | 44.85 (39.66; 53.38) | 0.182 | 42.75 (34.27; 51.76) | 40.18 (28.34; 51.72) | 0.011 * |
| IL-12p70 | 6.78 (6.09; 9.82) | 7.28 (6.57; 8.74) | 0.072 | 7.26 (6.05; 8.66) | 6.99 (6.14; 8.59) | 0.352 |
| IL-13 | 13.75 (12.18; 16.55) | 13.42 (12.18; 18.23) | 0.334 | 13.52 (11.45; 16.10) | 12.97 (10.42; 16.83) | 0.994 |
| IL-15 | 6.90 (5.69; 8.53) | 7.04 (5.65; 8.21) | 0.839 | 6.26 (5.12; 8.23) | 6.17 (4.93; 7.62) | 0.183 |
| IL-17A | 4.39 (3.74; 5.24) | 4.66 (4.14; 5.62) | 0.150 | 4.47 (3.75; 5.34) | 4.39 (3.47; 5.24) | 0.031 * |
| TNF-α | 20.75 (15.26; 26.26) | 22.34 (16.15; 26.59) | 0.342 | 18.22 (11.62; 25.48) | 16.33 (12.10; 20.52) | 0.012 * |
| TNF-β | 6.78 (5.51; 8.83) | 6.67 (5.59; 9.05) | 0.604 | 6.49 (2.89; 11.92) | 6.49 (2.50; 9.36) | 0.199 |
| Indicators | Patients with MetS (n = 14) | Patients without MetS (n = 29) | ||||
|---|---|---|---|---|---|---|
| Before | After | p-Value | Before | After | p-Value | |
| IFN-α2 | 17.95 (8.29; 23.98) | 23.49 (12.39; 35.17) | 0.008 * | 17.53 (13.36; 27.83) | 20.11 (15.62; 27.22) | 0.633 |
| IFN-γ | 10.53 (8.78; 12.05) | 11.31 (9.00; 13.59) | 0.433 | 10.77 (8.90; 13.67) | 10.51 (9.52; 11.71) | 0.191 |
| IL-1RA | 43.86 (39.07; 57.35) | 43.68 (39.07; 59.90) | 0.859 | 46.65 (39.09; 78.24) | 45.48 (38.25; 69.43) | 0.641 |
| IL-1α | 54.08 (49.43; 58.69) | 58.85 (50.02; 70.66) | 0.084 | 56.95 (50.58; 65.88) | 54.67 (45.85; 62.57) | 0.111 |
| IL-1β | 2.68 (2.28; 2.87) | 2.79 (2.44; 3.28) | 0.041 * | 2.49 (1.98; 3.23) | 2.33 (1.83; 2.91) | 0.225 |
| IL-2 | 4.85 (4.37; 5.12) | 5.34 (4.61; 5.78) | 0.346 | 4.91 (4.38; 5.50) | 5.19 (4.49; 5.80) | 0.905 |
| IL-3 | 3.32 (2.94; 3.73) | 3.45 (3.07; 3.83) | 0.289 | 3.07 (2.77; 3.86) | 3.52 (3.07; 3.79) | 0.319 |
| IL-4 | 75.27 (72.14; 83.85) | 85.97 (68.19; 107.62) | 0.152 | 81.48 (69.68; 96.15) | 83.85 (69.70; 134.07) | 0.733 |
| IL-5 | 1.78 (1.34; 2.46) | 1.81 (1.42; 2.62) | 0.600 | 2.09 (1.57; 2.81) | 1.96 (1.51; 2.79) | 0.464 |
| IL-6 | 6.67 (4.67; 8.18) | 5.44 (4.48; 7.35) | 0.363 | 6.67 (4.46; 9.55) | 5.56 (3.99; 8.28) | 0.202 |
| IL-7 | 10.84 (9.62; 11.75) | 11.18 (10.05; 13.80) | 0.046 * | 10.18 (9.18; 11.67) | 9.69 (8.90; 12.14) | 0.948 |
| IL-8 | 14.87 (11.71; 20.69) | 13.97 (10.89; 21.83) | 0.807 | 12.04 (8.77; 18.99) | 13.03 (9.41; 17.36) | 0.456 |
| IL-9 | 3.78 (3.23; 4.13) | 4.06 (3.24; 4.51) | 0.706 | 3.57 (2.33; 4.93) | 3.57 (2.71; 5.25) | 0.673 |
| IL-10 | 9.00 (7.08; 12.63) | 8.84 (7.29; 11.42) | 0.889 | 8.00 (7.08; 10.84) | 8.00 (6.60; 1.01) | 0.568 |
| IL-12p40 | 45.73 (41.05; 52.31) | 46.50 (40.18; 53.74) | 0.397 | 44.52 (36.01; 62.32) | 42.10 (32.29; 59.95) | 0.315 |
| IL-12p70 | 6.83 (6.66; 7.39) | 7.47 (6.84; 8.45) | 0.221 | 7.26 (6.23; 8.76) | 7.08 (6.21; 8.59) | 0.737 |
| IL-13 | 12.97 (11.78; 14.32) | 12.70 (11.98; 14.13) | 0.944 | 13.75 (11.53; 17.90) | 13.75 (10.60; 21.16) | 0.341 |
| IL-15 | 7.81 (6.93; 9.43) | 7.80 (5.76; 8.79) | 0.209 | 6.35 (5.39; 8.50) | 6.70 (5.02; 7.95) | 0.548 |
| IL-17A | 4.61 (3.95; 5.24) | 5.30 (4.31; 6.81) | 0.221 | 4.61 (3.75; 5.55) | 4.50 (3.87; 5.39) | 0.755 |
| TNF-α | 20.75 (18.67; 26.76) | 22.79 (20.71; 26.48) | 0.347 | 18.33 (12.84; 25.36) | 17.46 (12.87; 20.17) | 0.111 |
| TNF-β | 6.90 (6.13; 7.70) | 6.93 (5.74; 8.52) | 0.279 | 7.46 (3.44; 19.90) | 6.78 (2.34; 18.72) | 0.336 |
| Indicators | Patients with MetS (n = 13) | Patients without MetS (n = 23) | ||||
|---|---|---|---|---|---|---|
| Before | After | p-Value | Before | After | p-Value | |
| IFN-α2 | 17.50 (8.78; 27.07) | 23.59 (13.54; 36.84) | 0.050 * | 18.87 (15.78; 27.67) | 20.88 (15.38; 28.89) | 0.438 |
| IFN-γ | 9.23 (8.33; 11.98) | 11.76 (8.45; 14.32) | 0.944 | 11.31 (9.01; 13.14) | 10.11 (9.11; 10.99) | 0.086 |
| IL-1RA | 47.24 (35.25; 68.65) | 52.42 (43.67; 75.81) | 0.940 | 48.99 (38.13; 86.43) | 52.20 (38.13; 75.37) | 0.651 |
| IL-1α | 49.69 (43.25; 63.39) | 55.43 (53.38; 63.77) | 0.057 | 56.95 (46.15; 71.46) | 54.67 (50.12; 74.52) | 0.461 |
| IL-1β | 2.34 (2.06; 2.99) | 2.56 (2.29; 2.93) | 0.907 | 2.64 (1.85; 2.98) | 2.17 (1.52; 2.64) | 0.139 |
| IL-2 | 4.42 (4.23; 4.99) | 4.67 (4.30; 5.65) | 0.153 | 5.16 (4.67; 6.11) | 5.29 (4.62; 6.11) | 0.564 |
| IL-3 | 3.22 (2.55; 3.43) | 3.07 (2.81; 3.69) | 0.750 | 3.32 (2.81; 4.05) | 3.25 (2.81; 4.08) | 0.457 |
| IL-4 | 78.37 (69.57; 120.05) | 80.70 (76.83; 111.72) | 0.509 | 75.10 (65.15; 100.79) | 79.52 (65.74; 89.87) | 0.637 |
| IL-5 | 1.98 (1.34; 3.23) | 2.07 (1.40; 2.62) | 0.991 | 1.98 (1.43; 2.53) | 1.87 (1.73; 2.49) | 0.619 |
| IL-6 | 5.75 (4.38; 10.25) | 5.86 (4.45; 7.12) | 0.054 | 5.47 (4.15; 10.24) | 4.89 (3.39; 7.03) | 0.041 * |
| IL-7 | 10.33 (7.69; 12.92) | 10.67 (9.62; 12.06) | 0.551 | 10.33 (7.69; 12.93) | 9.57 (7.74; 11.41) | 0.632 |
| IL-8 | 14.75 (9.04; 18.32) | 13.63 (10.40; 16.99) | 0.100 | 11.76 (7.56; 22.41) | 10.72 (7.34; 17.61) | 0.291 |
| IL-9 | 3.73 (2.63; 3.97) | 3.44 (2.54; 3.90) | 0.236 | 3.80 (2.33; 4.61) | 2.94 (2.11; 3.84) | 0.386 |
| IL-10 | 9.07 (7.78; 11.34) | 9.24 (7.24; 9.91) | 0.216 | 7.89 (6.15; 11.19) | 7.39 (6.05; 8.87) | 0.169 |
| IL-12p40 | 42.10 (39.05; 48.45) | 44.23 (42.62; 46.19) | 0.654 | 40.66 (33.10; 53.31) | 39.46 (26.89; 46.83) | 0.050 * |
| IL-12p70 | 6.71 (5.69; 7.13) | 7.24 (6.43; 9.19) | 0.417 | 6.85 (5.96; 8.89) | 7.28 (6.14; 8.59) | 0.765 |
| IL-13 | 14.52 (11.61; 17.91) | 16.00 (12.93; 21.11) | 0.567 | 13.52 (10.64; 15.27) | 12.97 (10.56; 16.01) | 0.411 |
| IL-15 | 6.47 (5.25; 7.31) | 6.70 (5.56; 7.65) | 0.687 | 6.17 (4.84; 7.39) | 5.91 (4.97; 7.49) | 0.540 |
| IL-17A | 4.18 (3.51; 5.24) | 4.59 (4.18; 5.15) | 0.581 | 4.43 (3.73; 6.32) | 3.97 (3.21; 5.24) | 0.172 |
| TNF-α | 19.14 (14.61; 25.91) | 22.06 (14.77; 28.79) | 0.798 | 16.09 (10.49; 25.48) | 16.15 (11.24; 20.52) | 0.161 |
| TNF-β | 8.29 (6.00; 13.81) | 6.98 (6.12; 18.92) | 0.569 | 6.24 (2.89; 13.51) | 5.88 (2.50; 8.90) | 0.280 |
| Indicators | Patients without MetS (n = 11) | ||
|---|---|---|---|
| Before | After | p-Value | |
| IFN-α2 | 17.60 (12.85; 34.04) | 22.87 (11.38; 27.33) | 0.131 |
| IFN-γ | 9.85 (8.03; 14.19) | 9.33 (8.33; 12.58) | 0.082 |
| IL-1α | 55.31 (40.39; 62.64) | 54.18 (44.46; 55.67) | 0.721 |
| IL-1β | 2.26 (1.98; 2.57) | 2.01 (1.39; 2.50) | 0.333 |
| IL-2 | 5.40 (3.93; 6.65) | 5.49 (4.67; 6.11) | 0.929 |
| IL-3 | 3.34 (2.81; 4.22) | 3.58 (2.83; 4.05) | 0.721 |
| IL-4 | 85.19 (70.40; 108.60) | 78.46 (72.14; 101.36) | 0.477 |
| IL-5 | 2.41 (2.23; 2.56) | 2.18 (1.70; 3.00) | 0.594 |
| IL-6 | 4.83 (3.59; 8.25) | 5.16 (3.80; 7.39) | 0.965 |
| IL-7 | 9.88 (8.02; 12.19) | 9.50 (8.49; 12.19) | 0.610 |
| IL-8 | 16.58 (7.85; 30.76) | 10.03 (7.70; 17.83) | 0.859 |
| IL-9 | 3.04 (2.76; 4.01) | 2.89 (2.11; 4.10) | 0.575 |
| IL-10 | 8.00 (5.84; 10.72) | 7.83 (5.14; 10.35) | 0.131 |
| IL-12p40 | 40.18 (32.22; 48.98) | 38.33 (27.89; 47.52) | 0.477 |
| IL-12p70 | 7.13 (5.53; 9.69) | 6.50 (6.06; 7.38) | 0.197 |
| IL-13 | 13.58 (11.33; 17.54) | 12.18 (9.84; 15.52) | 0.285 |
| IL-15 | 5.98 (5.38; 7.49) | 5.42 (4.84; 7.75) | 0.185 |
| IL-17A | 4.45 (3.58; 5.03) | 4.16 (3.26; 5.15) | 0.153 |
| TNF-α | 19.13 (9.73; 30.40) | 13.89 (10.67; 23.87) | 0.333 |
| TNF-β | 5.02 (2.69; 6.97) | 5.51 (2.36; 7.41) | 0.859 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boiko, A.S.; Mednova, I.A.; Kornetova, E.G.; Gerasimova, V.I.; Kornetov, A.N.; Loonen, A.J.M.; Bokhan, N.A.; Ivanova, S.A. Cytokine Level Changes in Schizophrenia Patients with and without Metabolic Syndrome Treated with Atypical Antipsychotics. Pharmaceuticals 2021, 14, 446. https://doi.org/10.3390/ph14050446
Boiko AS, Mednova IA, Kornetova EG, Gerasimova VI, Kornetov AN, Loonen AJM, Bokhan NA, Ivanova SA. Cytokine Level Changes in Schizophrenia Patients with and without Metabolic Syndrome Treated with Atypical Antipsychotics. Pharmaceuticals. 2021; 14(5):446. https://doi.org/10.3390/ph14050446
Chicago/Turabian StyleBoiko, Anastasiia S., Irina A. Mednova, Elena G. Kornetova, Valeria I. Gerasimova, Alexander N. Kornetov, Anton J. M. Loonen, Nikolay A. Bokhan, and Svetlana A. Ivanova. 2021. "Cytokine Level Changes in Schizophrenia Patients with and without Metabolic Syndrome Treated with Atypical Antipsychotics" Pharmaceuticals 14, no. 5: 446. https://doi.org/10.3390/ph14050446
APA StyleBoiko, A. S., Mednova, I. A., Kornetova, E. G., Gerasimova, V. I., Kornetov, A. N., Loonen, A. J. M., Bokhan, N. A., & Ivanova, S. A. (2021). Cytokine Level Changes in Schizophrenia Patients with and without Metabolic Syndrome Treated with Atypical Antipsychotics. Pharmaceuticals, 14(5), 446. https://doi.org/10.3390/ph14050446