
Matrix Metalloproteinase-2 Inhibition in Acute Ischemia-Reperfusion Heart Injury—Cardioprotective Properties of Carvedilol

 , , and
, , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
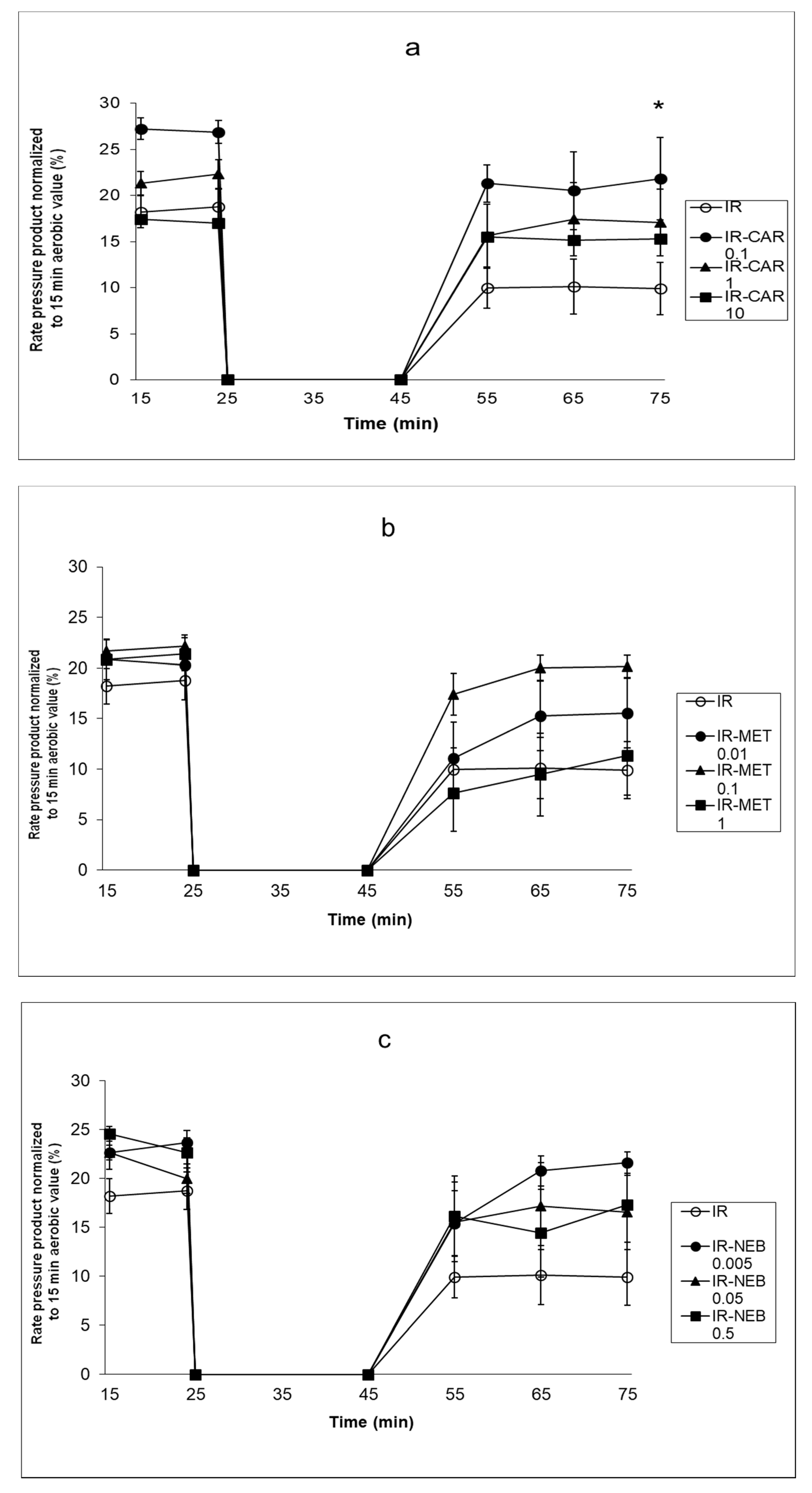
2.1. Carvedilol Protects Hearts from Ischemia-Reperfusion Injury
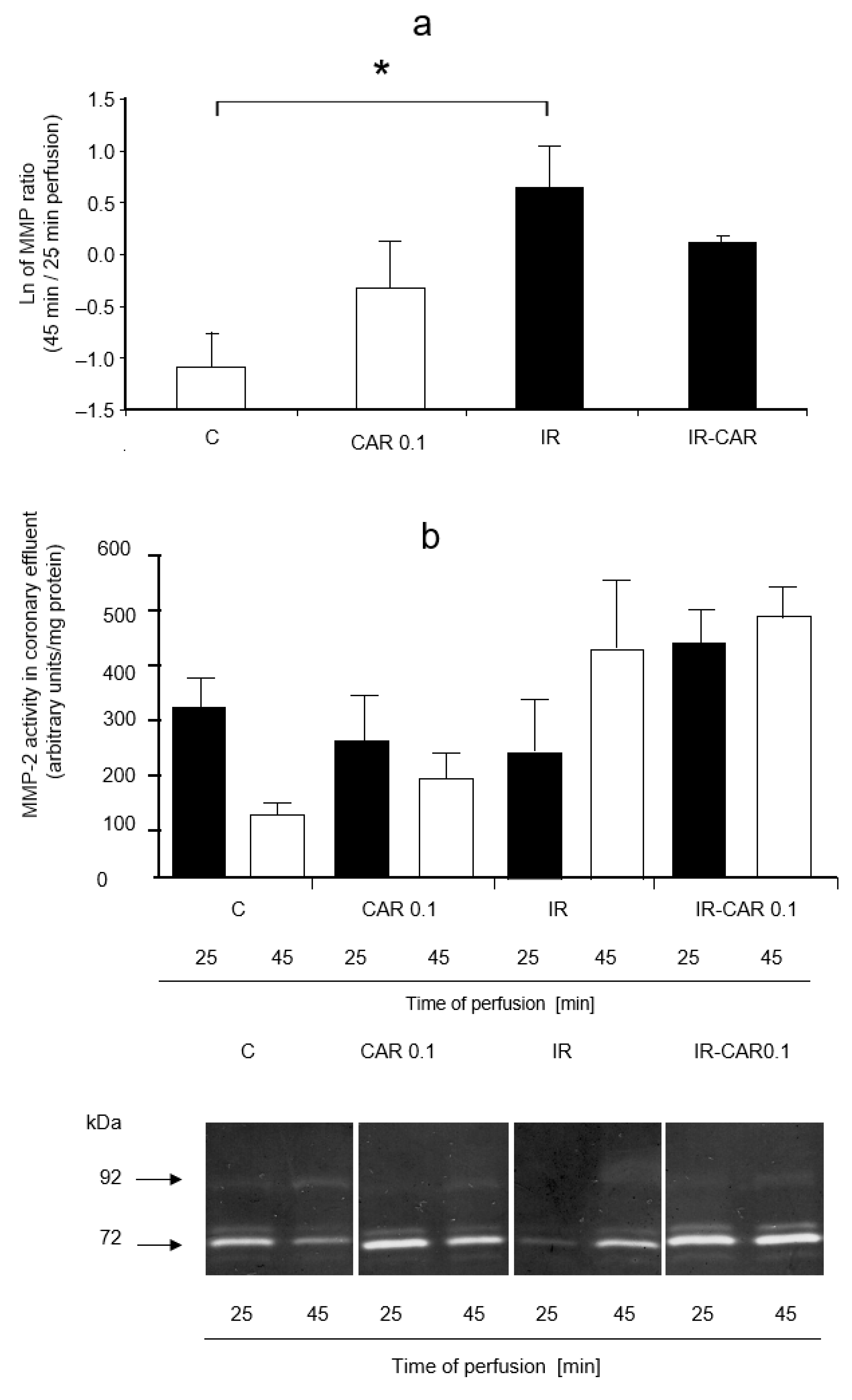
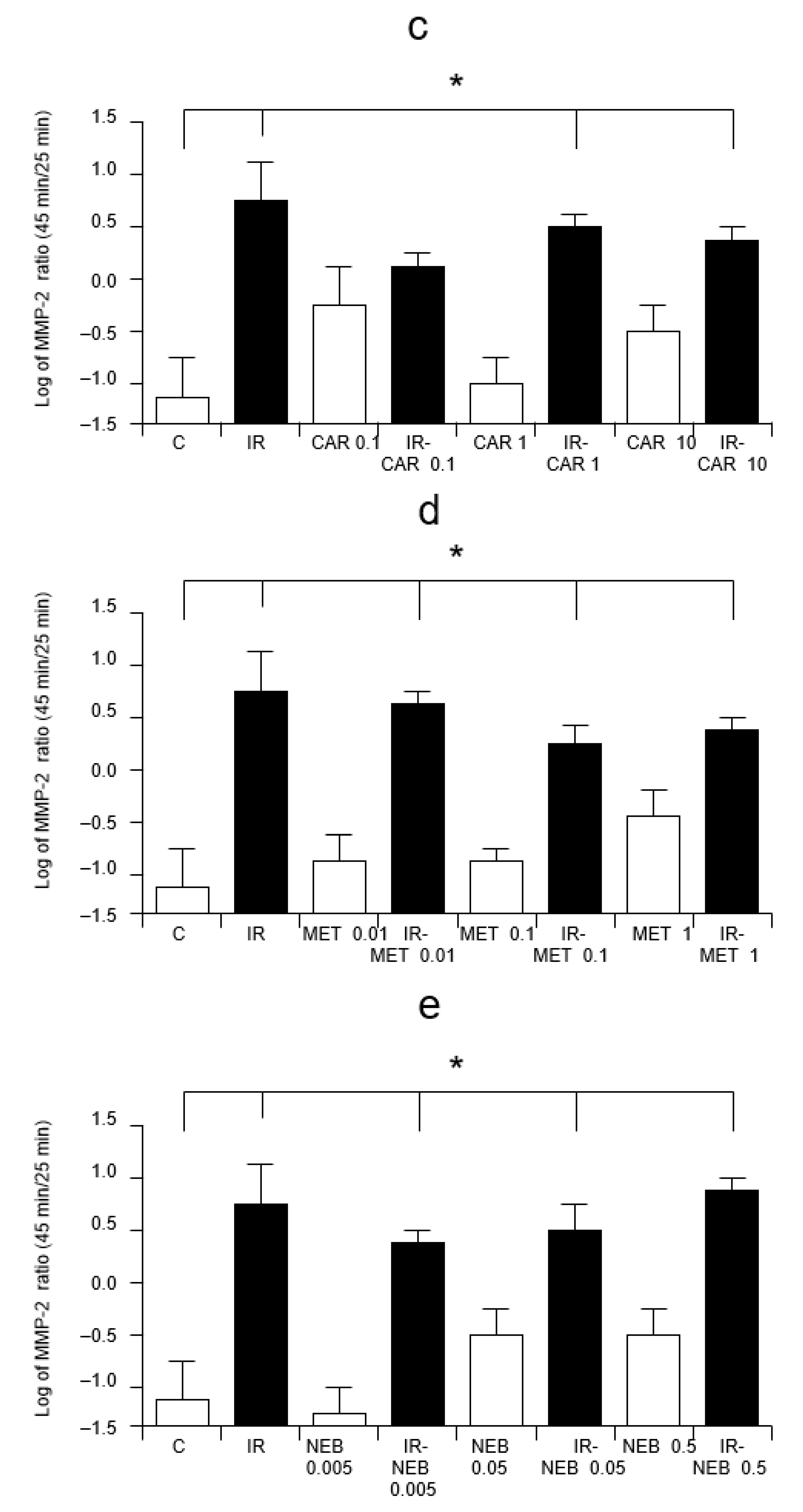
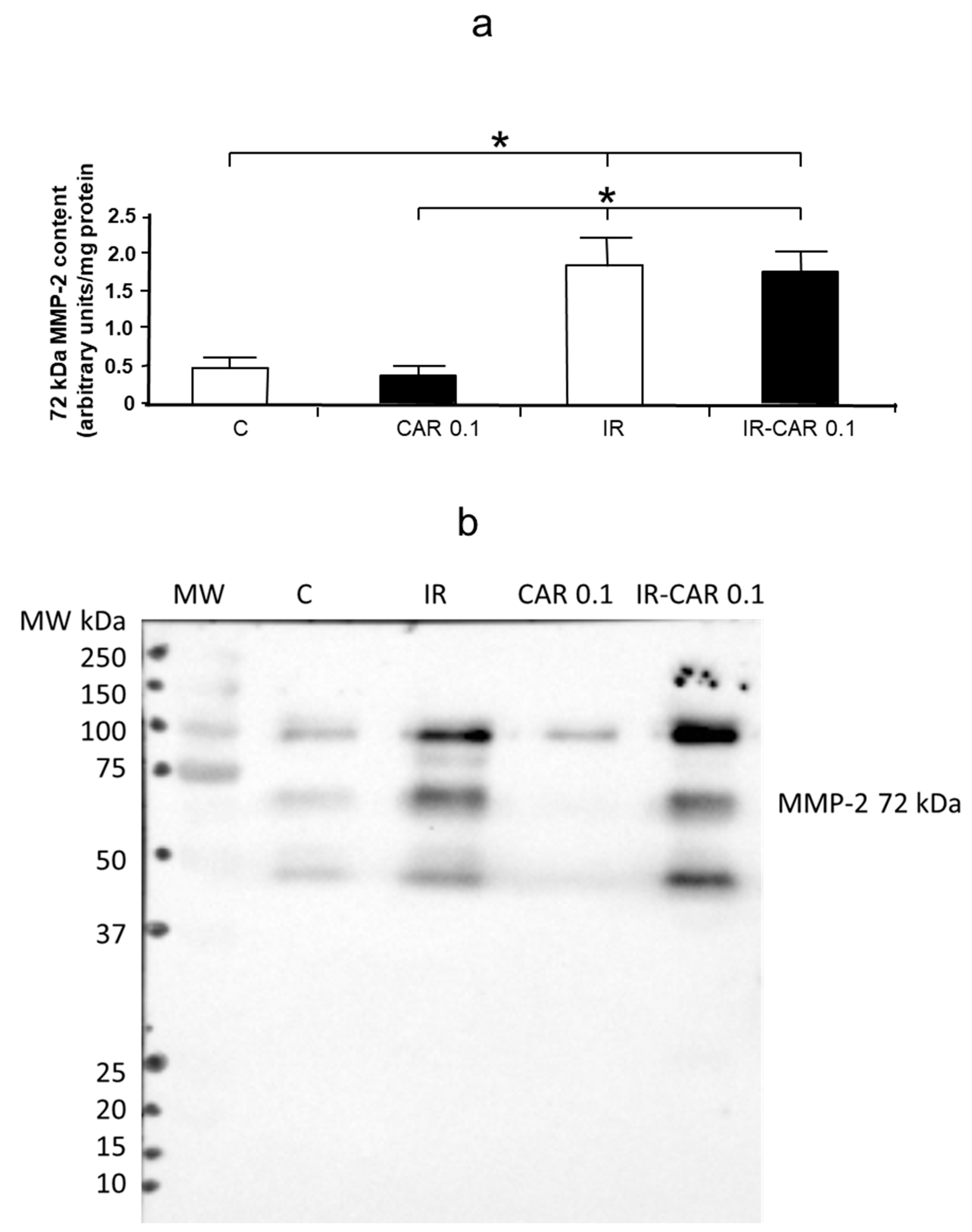
2.2. Carvedilol Influences MMP-2 Activity
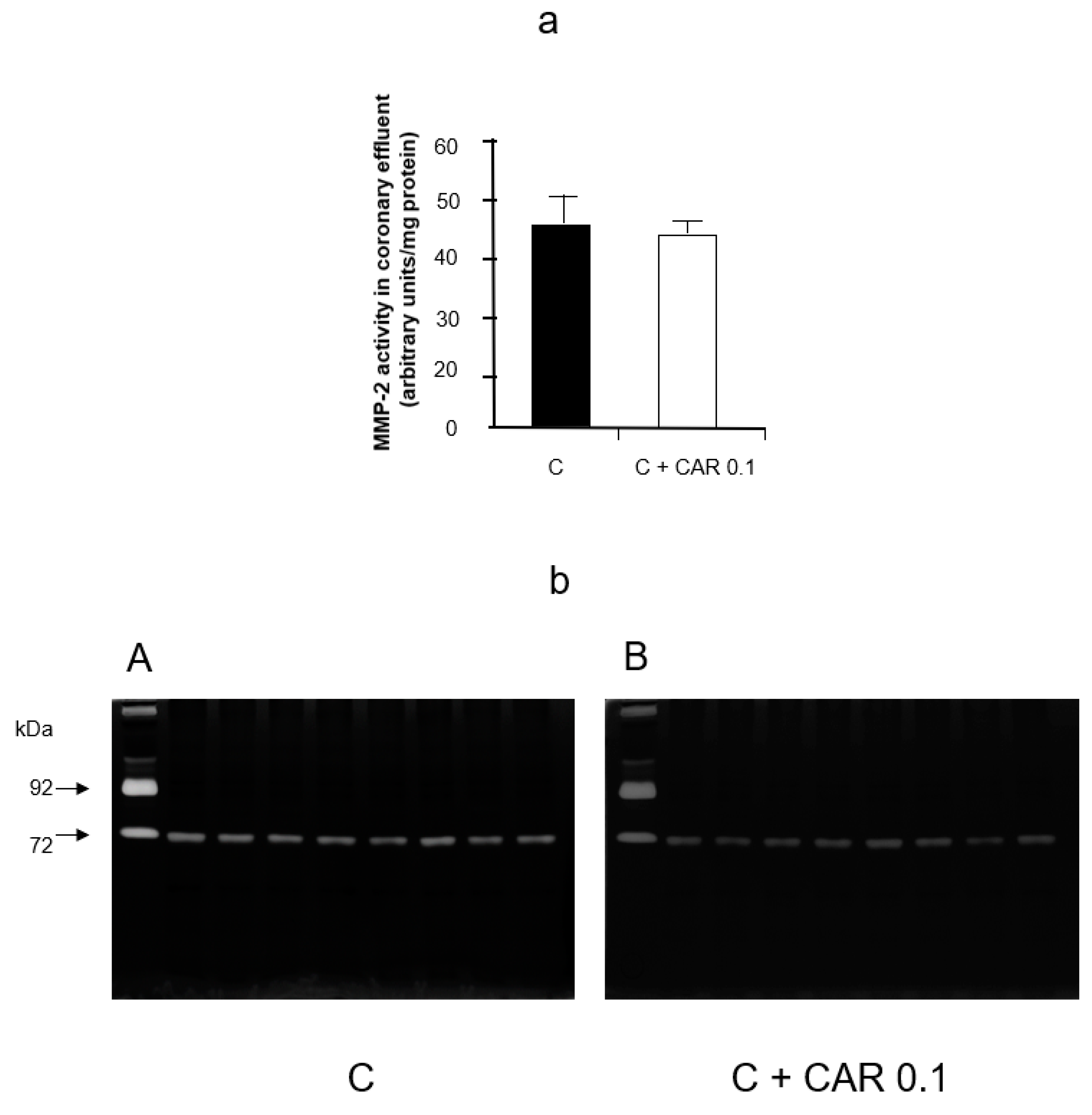
2.3. Carvedilol Has No Effect on MMP-2 Activity In Vitro
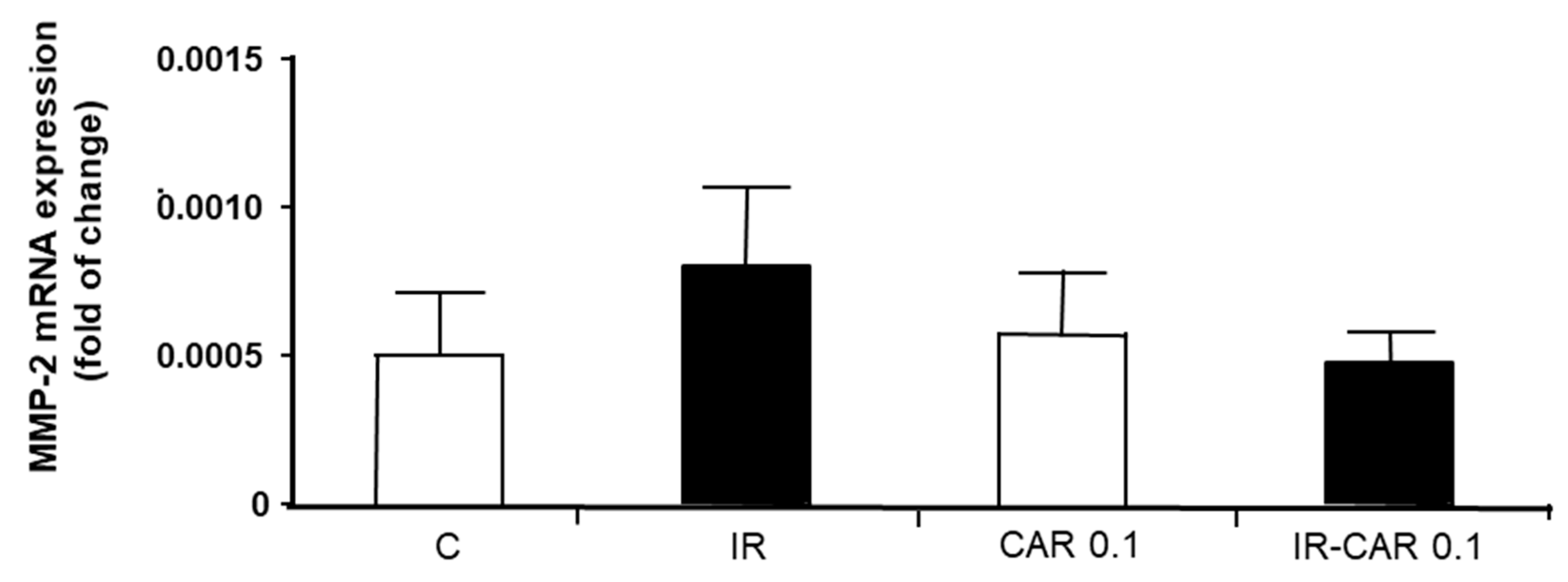
2.4. Carvedilol Does Not Change MMP-2 mRNA Expression in Hearts Subjected to Ischemia-Reperfusion
2.5. Carvedilol Does Not Affect MMP-2 Content in Coronary Effluent
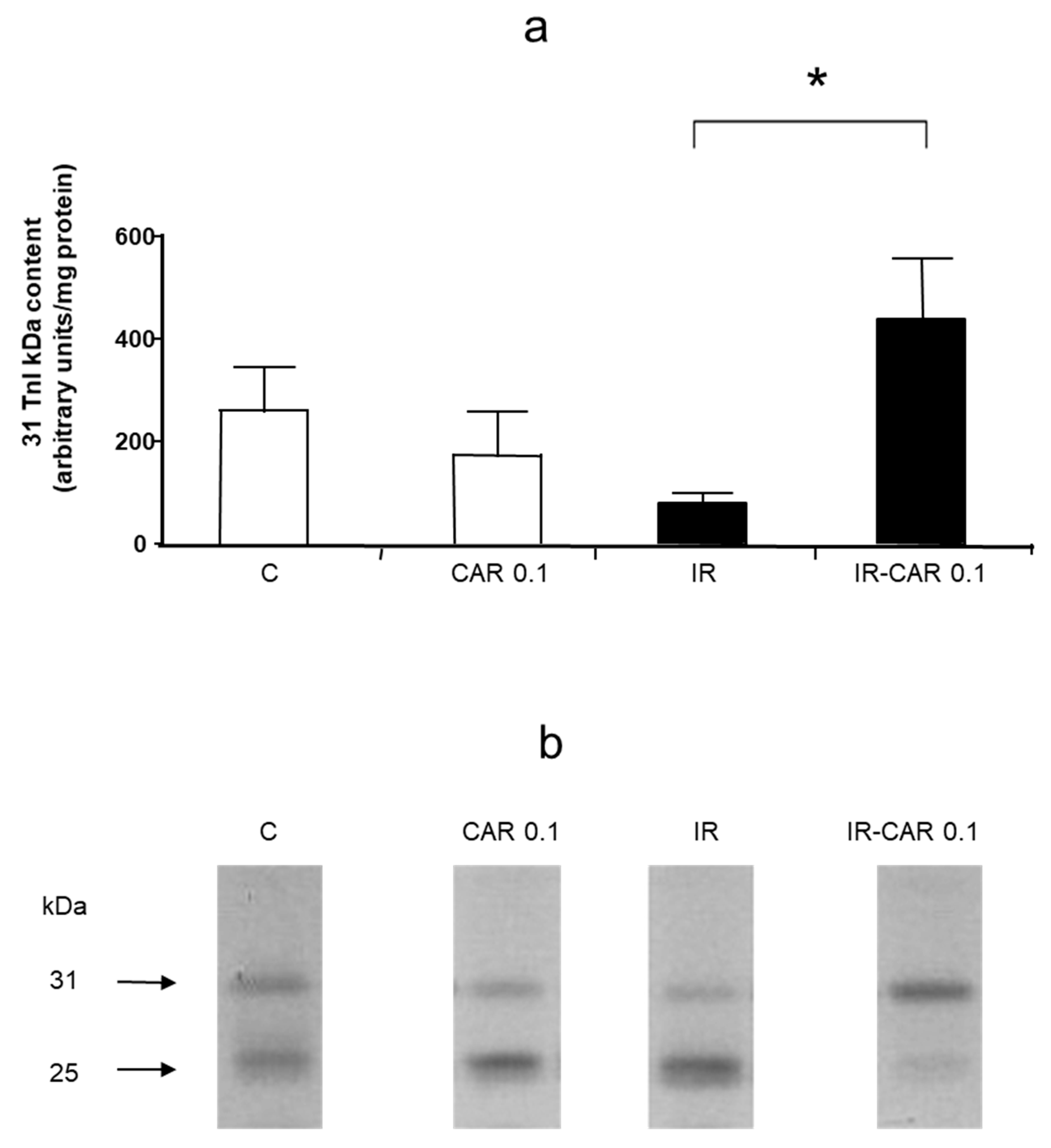
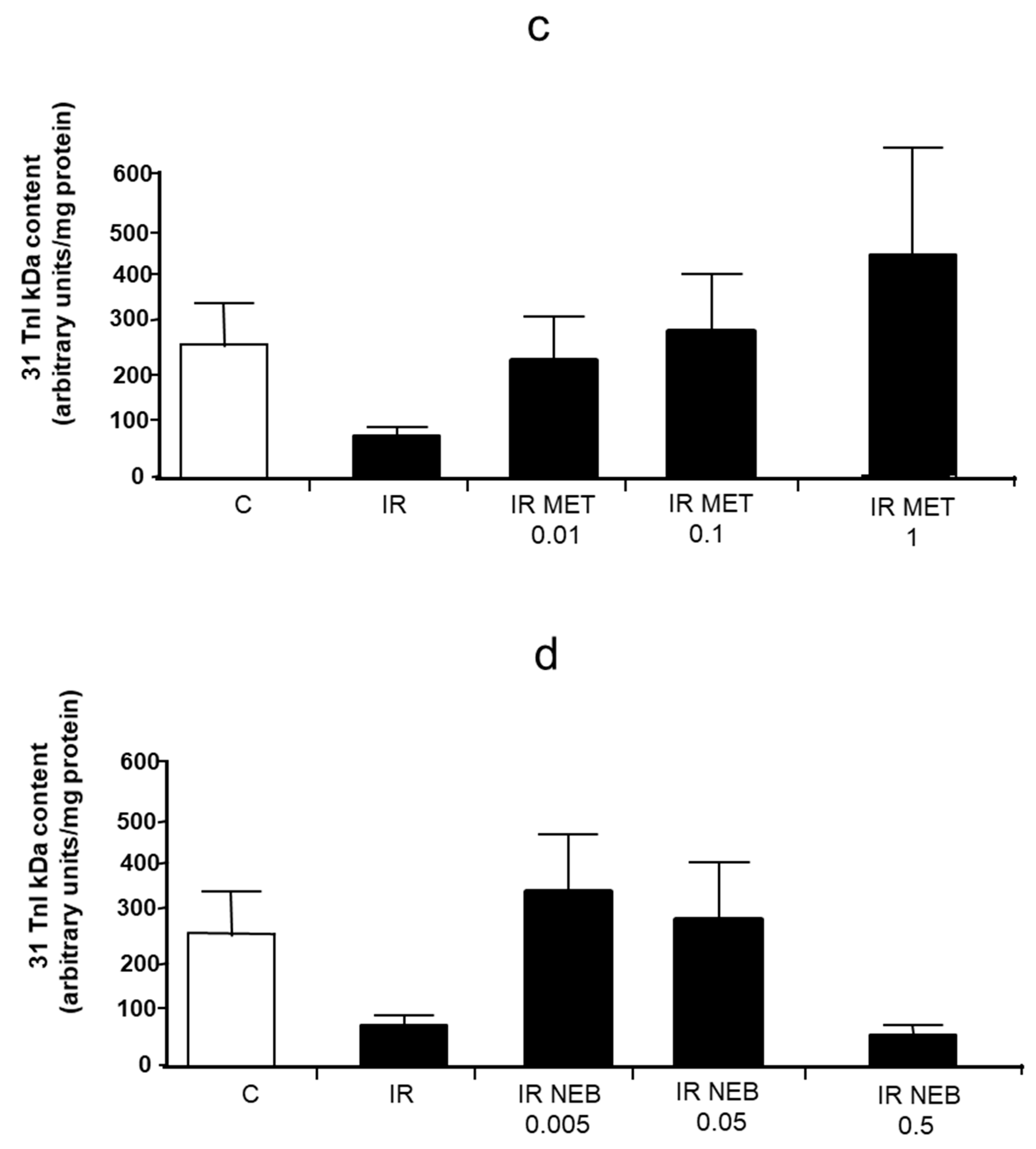
2.6. Carvedilol Abolishes Troponin I Level in Heart Tissue
3. Discussion
4. Materials and Methods
4.1. Animals
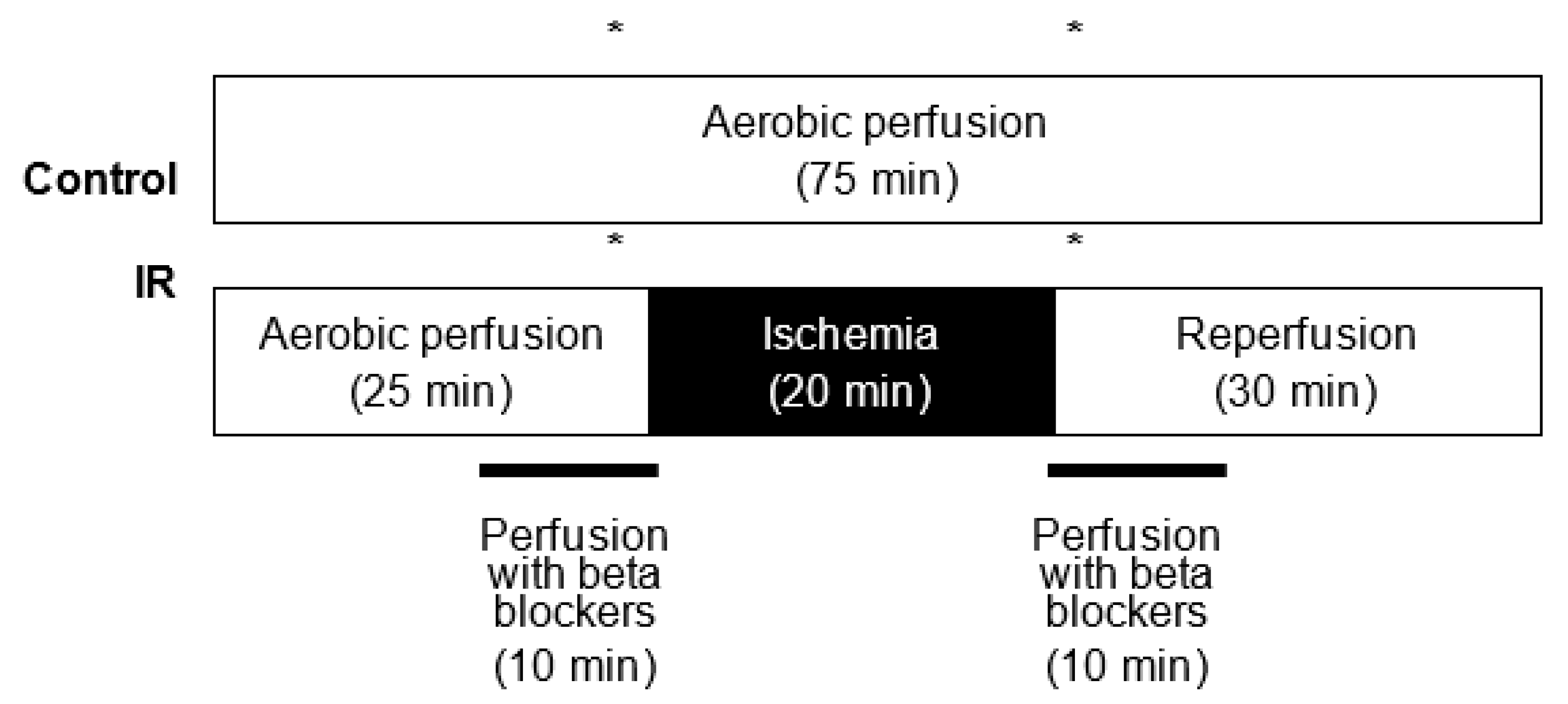
4.2. Heart Perfusion Protocol
4.3. Experimental Groups
4.4. Preparation of Heart Extracts and Concentration of Coronary Effluent
4.5. Measurement of MMP-2 by Gelatin Zymography
4.6. Measurement of Troponin I and MMP-2 by Western Blot
4.7. Expression of MMP-2 Gene in Heart Tissue
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- O’Rourke, S. Antianginal Actions of Beta-Adrenoceptor Antagonists. Am. J. Pharm. Educ. 2007, 71, 95. [Google Scholar] [CrossRef] [Green Version]
- Heitzler, V.N.; Pavlov, M. Therapeutic approach in acute coronary syndrome focusing on oral therapy. Acta Clin. Croat. 2010, 49, 81–87. [Google Scholar]
- Joseph, J.; Velasco, A.; Hage, F.G.; Reyes, E. Guidelines in review: Comparison of ESC and ACC/AHA guidelines for the diagnosis and management of patients with stable coronary artery disease. J. Nucl. Cardiol. 2018, 25, 509–515. [Google Scholar] [CrossRef]
- Schwarz, E.R.; Kersting, P.H.; Reffelmann, T.; Meven, D.A.; Al-Dashti, R.; Skobel, E.C.; Klosterhalfen, B.; Hanrath, P. Cardioprotection by carvedilol: Anti-apoptosis is independent on beta-adrenoceptor blockage in the rat heart. J. Cardiovasc. Pharm. Ther. 2003, 8, 207–215. [Google Scholar] [CrossRef]
- Lu, H.R.; Vandeplassche, G.; Wouters, L.; Borgers, M. Beta-blockade in the ischemic reperfused working rabbit heart: Dissociation of beta-adrenergic blocking and protective effects. Arch. Int. Pharmacodyn. Ther. 1989, 301, 165–181. [Google Scholar]
- Kimura-Kurosawa, S.; Kanaya, N.; Kamada, N.; Hirata, N.; Nakayama, M.; Namiki, A. Cardioprotective effect and mechanism of action of landiolol on the ischemic reperfused heart. J. Anesth. 2007, 21, 480–489. [Google Scholar] [CrossRef]
- Gao, F.; Chen, J.; Lopez, B.L.; Christopher, T.A.; Gu, J.; Lysko, P.; Ruffolo, R.R.; Ohlstein, E.H.; Ma, X.L.; Yue, T.-L. Comparison of bisoprolol and carvedilol cardioprotection in rabit ischemia and reperfusion model. Eur. J. Pharmacol. 2000, 406, 109–116. [Google Scholar] [CrossRef]
- Kurosawa, S.; Kanaya, N.; Niiyama, Y.; Nakayama, M.; Fujita, S.; Namiki, A. Landiolol, esmolol and propranolol protect from ischemia/reperfusion injury in isolated guinea pig hearts. Can. J. Anaesth. 2003, 50, 489–494. [Google Scholar] [CrossRef] [Green Version]
- Cargnoni, A.; Ceconi, C.; Bernocchi, P.; Boraso, A.; Parrinello, G.; Curello, S.; Ferrari, R. Reduction of oxidative stress by carvedilol: Role in maintenance of ischaemic myocardium viability. Cardiovasc. Res. 2000, 47, 556–566. [Google Scholar] [CrossRef] [Green Version]
- Feuerstein, G.Z.; Ruffolo, R.R. Carvedilol, a novel vasodilating beta-blocker with the potential for cardiovascular organ protection. Eur. Heart J. 1996, 17 (Suppl. B), 24–29. [Google Scholar] [CrossRef] [Green Version]
- Pauschinger, M.; Rutschow, S.; Chandrasekharan, K.; Westermann, D.; Weitz, A.; Schwimmbeck, L.P.; Zeichhardt, H.; Poller, W.; Noutsias, M.; Li, J.; et al. Carvedilol improves left ventricular function in murine coxsackievirus-induced acute myocarditis association with reduced myocardial interleukin-1beta and MMP-8 expression and a modulated immune response. Eur. J. Heart Fail. 2005, 7, 444–452. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.-C.; Chen, Y.-H.; Leu, H.-B.; Chen, Y.-L.; Lin, F.-Y.; Lin, S.-J.; Chen, J.-W. Carvedilol, a pharmacological antioxidant, inhibits neointimal matrix metalloproteinase-2 and -9 in experimental atherosclerosis. Free. Radic. Biol. Med. 2007, 43, 1508–1522. [Google Scholar] [CrossRef]
- Skrzypiec-Spring, M.; Haczkiewicz-Leśniak, K.; Sapa, A.; Piasecki, T.; Kwiatkowska, J.; Ceremuga, I.; Woźniak, M.; Biczysko, W.; Kobierzycki, C.; Dziegiel, P.; et al. Carvedilol inhibits matrix metalloproteinase-2 activation in experimental autoimmune myocarditis: Possibilities of cardioprotective application. J. Cardiovasc. Pharmacol. Ther. 2018, 23, 89–97. [Google Scholar] [CrossRef] [Green Version]
- Kamp, O.; Metra, M.; Bugatti, S.; Bettari, L.; Cas, A.D.; Petrini, N.; Cas, L.D. Nebivolol: Haemodynamic effects and clinical significance of combined beta-blockade and nitric oxide release. Drugs 2010, 70, 41–56. [Google Scholar] [CrossRef] [Green Version]
- Ceron, C.S.; Rizzi, E.; Guimarães, D.A.; Martins-Oliveira, A.; Gerlach, R.F.; Tanus-Santos, J.E. Nebivolol attenuates prooxidant and profibrotic mechanisms involving TGF-β and MMPs, and decreases vascular remodeling in renovascular hypertension. Free. Radic. Biol. Med. 2013, 65, 47–56. [Google Scholar] [CrossRef] [Green Version]
- Ersan, S.; Tanrisev, M.; Cavdar, Z.; Celik, A.; Unli, M.; Kocak, A.; Kose, T. Pretreatment with nebivolol attenuates level and expression of matrix metalloproteinases in a rat model of renal ischemia-reperfusion injury. Nephrology 2017, 22, 1023–1029. [Google Scholar] [CrossRef]
- Yasmin, W.; Strynadka, K.D.; Schulz, R. Generation of peroxynitrite contributes to ischemia-reperfusion injury in isolated rat hearts. Cardiovasc. Res. 1997, 33, 422–432. [Google Scholar] [CrossRef] [Green Version]
- Viappiani, S.; Nicolescu, A.C.; Holt, A.; Sawicki, G.; Crawford, B.D.; León, H.; van Mulligen, T.; Schulz, R. Activation and modulation of 72kDa matrix metalloproteinase-2 by peroxynitrite and glutathione. Biochem. Pharmacol. 2009, 77, 826–834. [Google Scholar] [CrossRef]
- Wang, W.; Schulze, C.J.; Suarez-Pinzon, W.L.; Dyck, J.R.B.; Sawicki, G.; Schulz, R. Intracellular action of matrix metalloproteinase-2 accounts for acute myocardial ischemia and reperfusion injury. Circulation 2002, 106, 1543–1549. [Google Scholar] [CrossRef] [Green Version]
- Ali, M.A.M.; Fan, X.; Schulz, R. Cardiac sarcomeric proteins: Novel intracellular targets of matrix metalloproteinase-2 in heart disease. Trends Cardiovasc. Med. 2011, 21, 112–118. [Google Scholar] [CrossRef]
- Sariahmetoglu, M.; Skrzypiec-Spring, M.; Youssef, N.; Jacob-Ferreira, A.L.B.; Sawicka, J.; Holmes, C.; Sawicki, G.; Schulz, R. Phosphorylation status of matrix metalloproteinase-2 in myocardial ischemia-reperfusion injury. Heart 2012, 98, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Lalu, M.M.; Pasini, E.; Schulze, C.J.; Ferrari-Vivaldi, M.; Ferrari-Vivaldi, G.; Bachetti, T.; Schulz, R. Ischaemia-reperfusion injury activates matrix metalloproteinases in the human heart. Eur. Heart J. 2005, 26, 27–35. [Google Scholar] [CrossRef]
- Jaggi, A.S.; Singh, M.; Sharna, A.; Singh, D.; Singh, N. Cardioprotective effects of mast cell modulators in ischemia-reperfusion-induced injury in rats. Methods Find Exp. Clin. Pharmacol. 2007, 29, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Skobel, E.; Dannemann, O.; Reffelmann, T.; Böhm, V.; Weber, C.; Hanrath, P.; Uretsky, B.F.; Schwarz, E.R. Carvedilol protects myocardial cytoskeleton during hypoxia in the rat heart. J. Appl. Res. 2005, 5, 378–386. [Google Scholar]
- Jones, S.P.; Bolli, R. The ubiquitous role of nitric oxide in cardioprotection. J. Mol. Cell. Cardiol. 2006, 40, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.M.; MacCarthy, P.A. Paracrine and autocrine effects of nitric oxide on myocardial function. Pharmacol. Ther. 2000, 86, 49–86. [Google Scholar] [CrossRef]
- Dawn, B.; Bolli, R. Role of nitric oxide in myocardial preconditioning. Ann. N. Y. Acad. Sci. 2002, 962, 18–41. [Google Scholar] [CrossRef] [PubMed]
- Mori, E.; Haramaki, N.; Ikeda, H.; Imaizumi, T. Intra-coronary administration of L-arginine aggravates myocardial stunning through production of peroxynitrite in dogs. Cardiovasc. Res. 1998, 40, 113–123. [Google Scholar] [CrossRef]
- Zhang, Y.; Bissing, J.W.; Xu, L.; Ryan, A.J.; Martin, S.M.; Miller, F.J.; Kregel, K.C.; Buettner, G.; Kerber, R.E. Nitric oxide synthase inhibitors decrease coronary sinus-free radical concentration and ameliorate myocardial stunning in an ischemia-reperfusion model. J. Am. Coll. Cardiol. 2001, 38, 546–554. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Davies, L.R.; Martin, S.M.; Coddington, W.J.; Miller, F.J.; Buettner, G.R.; Kerber, R.E. The nitric oxide donor S-nitroso-N-acetylpenicillamine (SNAP) increases free radical generation and degrades left ventricular function after myocardial ischemia–reperfusion. Resuscitation 2003, 59, 345–352. [Google Scholar] [CrossRef]
- Bergman, M.R.; Teerlink, J.R.; Mahimkar, R.; Li, L.; Zhu, B.-Q.; Nguyen, A.; Dahi, S.; Karliner, J.S.; Lobertt, D.H. Cardiac transgenic matrix metalloproteinase-2 expression independently induces marked ventricular remodeling and systolic dysfunction. Am. J. Physiol. Heart Circ. Physiol. 2007, 292, 1847–1860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Shitany, N.A.; Tolba, O.A.; El-Shanshory, M.R.; El-Hawary, E.E. Protective effect of carvedilol on adriamycin-induced left ventricular dysfunction in children with acute lymphoblastic leukemia. J. Card. Fail. 2012, 18, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Cheung, P.-Y.; Sawicki, G.; Woźniak, M.; Wang, W.; Radomski, M.W.; Schulz, R. Matrix metalloproteinase-2 contributes to ischemia-reperfusion injury in the heart. Circulation 2000, 101, 1833–1839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skrzypiec-Spring, M.; Urbaniak, J.; Sapa-Wojciechowska, A.; Pietkiewicz, J.; Orda, A.; Karolko, B.; Danielewicz, R.; Bil-Lula, I.; Woźniak, M.; Schulz, R.; et al. Matrix Metalloproteinase-2 Inhibition in Acute Ischemia-Reperfusion Heart Injury—Cardioprotective Properties of Carvedilol. Pharmaceuticals 2021, 14, 1276. https://doi.org/10.3390/ph14121276
Skrzypiec-Spring M, Urbaniak J, Sapa-Wojciechowska A, Pietkiewicz J, Orda A, Karolko B, Danielewicz R, Bil-Lula I, Woźniak M, Schulz R, et al. Matrix Metalloproteinase-2 Inhibition in Acute Ischemia-Reperfusion Heart Injury—Cardioprotective Properties of Carvedilol. Pharmaceuticals. 2021; 14(12):1276. https://doi.org/10.3390/ph14121276
Chicago/Turabian StyleSkrzypiec-Spring, Monika, Joanna Urbaniak, Agnieszka Sapa-Wojciechowska, Jadwiga Pietkiewicz, Alina Orda, Bożena Karolko, Regina Danielewicz, Iwona Bil-Lula, Mieczysław Woźniak, Richard Schulz, and et al. 2021. "Matrix Metalloproteinase-2 Inhibition in Acute Ischemia-Reperfusion Heart Injury—Cardioprotective Properties of Carvedilol" Pharmaceuticals 14, no. 12: 1276. https://doi.org/10.3390/ph14121276
APA StyleSkrzypiec-Spring, M., Urbaniak, J., Sapa-Wojciechowska, A., Pietkiewicz, J., Orda, A., Karolko, B., Danielewicz, R., Bil-Lula, I., Woźniak, M., Schulz, R., & Szeląg, A. (2021). Matrix Metalloproteinase-2 Inhibition in Acute Ischemia-Reperfusion Heart Injury—Cardioprotective Properties of Carvedilol. Pharmaceuticals, 14(12), 1276. https://doi.org/10.3390/ph14121276