
Conventional Training Integrated with SteamVR Tracking 2.0: Body Stability and Coordination Training Evaluation on ICAROS Pro

 , , , , , , , ,
, , , , , , , ,  and
and
Abstract
1. Introduction
- A free and open-source software platform for the inclusion of SteamVR Tracking 2.0 into conventional training procedures on analog training devices.
- A platform-connected app for user guidance and feedback during the execution of freely configurable training procedures.
- A thorough evaluation of the training system and investigation of training effects for the use case of body stability and coordination training, with a representative training procedure conceptualized by a sports manager.
- A showcase for further extension of the platform towards VR-based exergaming, teasing directions of future work.
2. Related Work
3. Materials and Methods
3.1. ICAROS Pro
3.2. SteamVR Tracking 2.0
3.3. HTC VIVE Pro 2
3.4. Zephyr BioHarness 3.0
3.5. Empatica EmbracePlus
3.6. Study Populations
3.7. Evaluation Survey
3.8. Signal Processing
4. Design and Implementation
4.1. Main Study of Training System
4.1.1. System Architecture
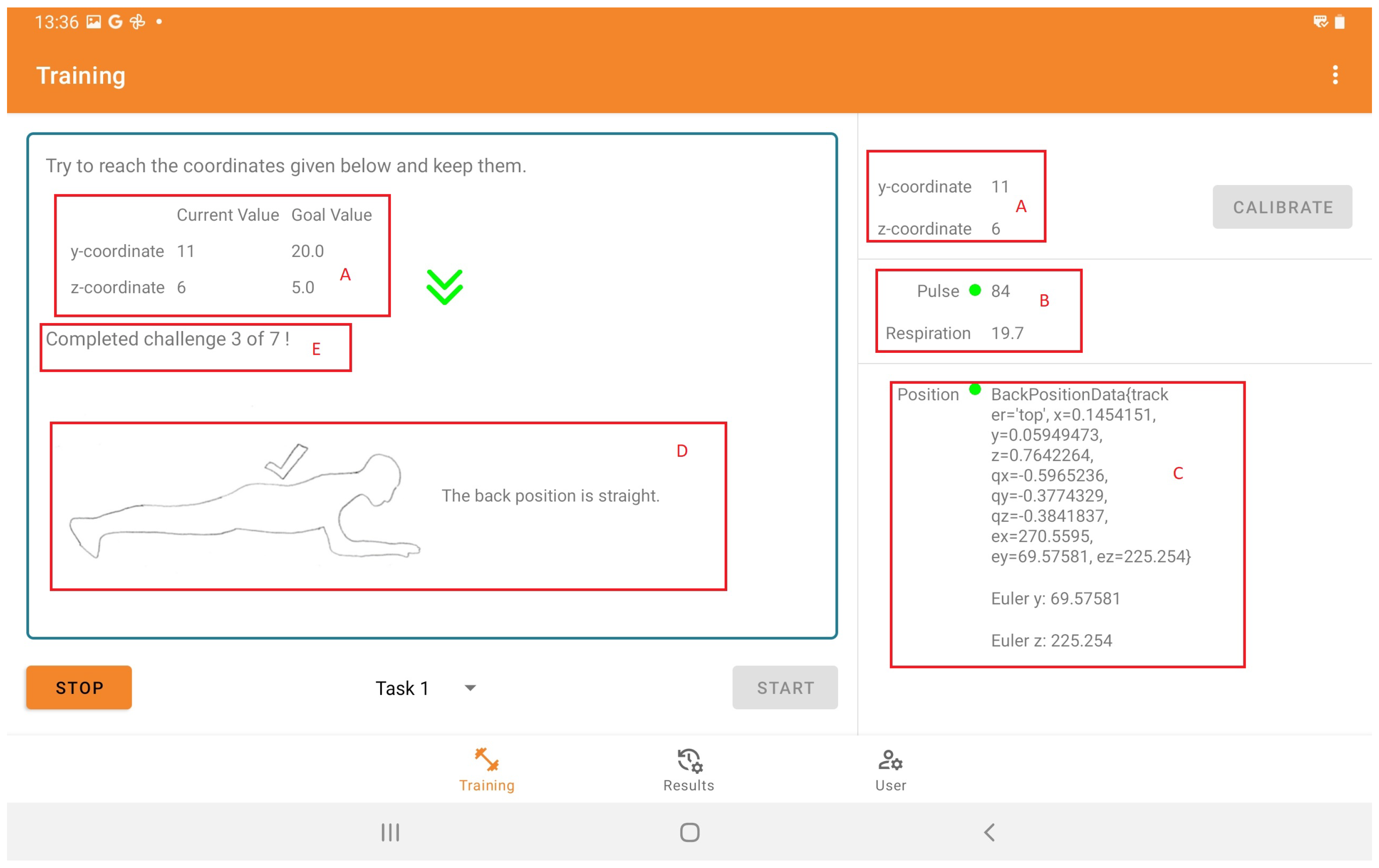
4.1.2. Tablet Application
4.1.3. Training Procedure
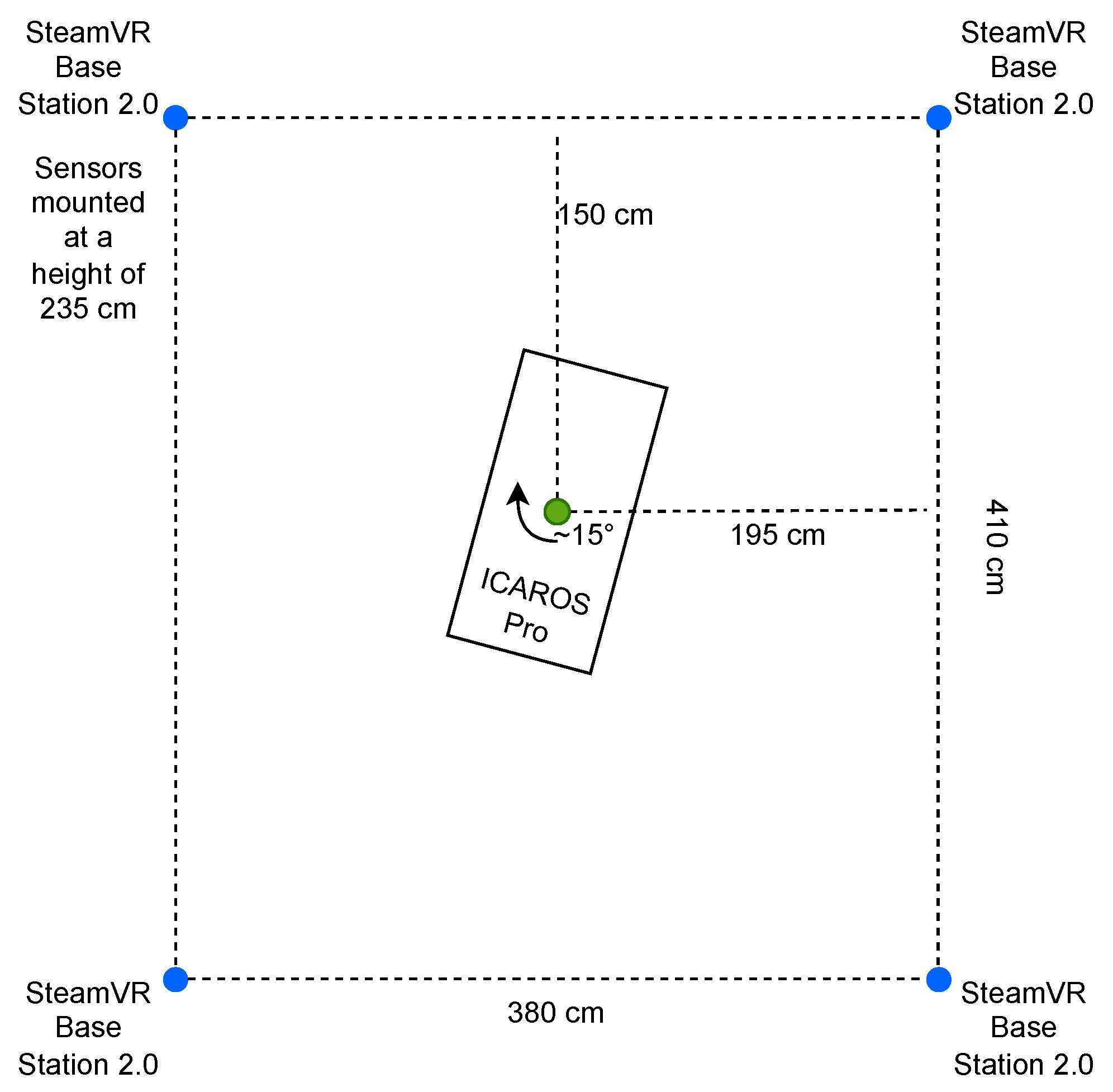
4.1.4. Training Setup
4.2. Secondary Study of VR-Based Exergame
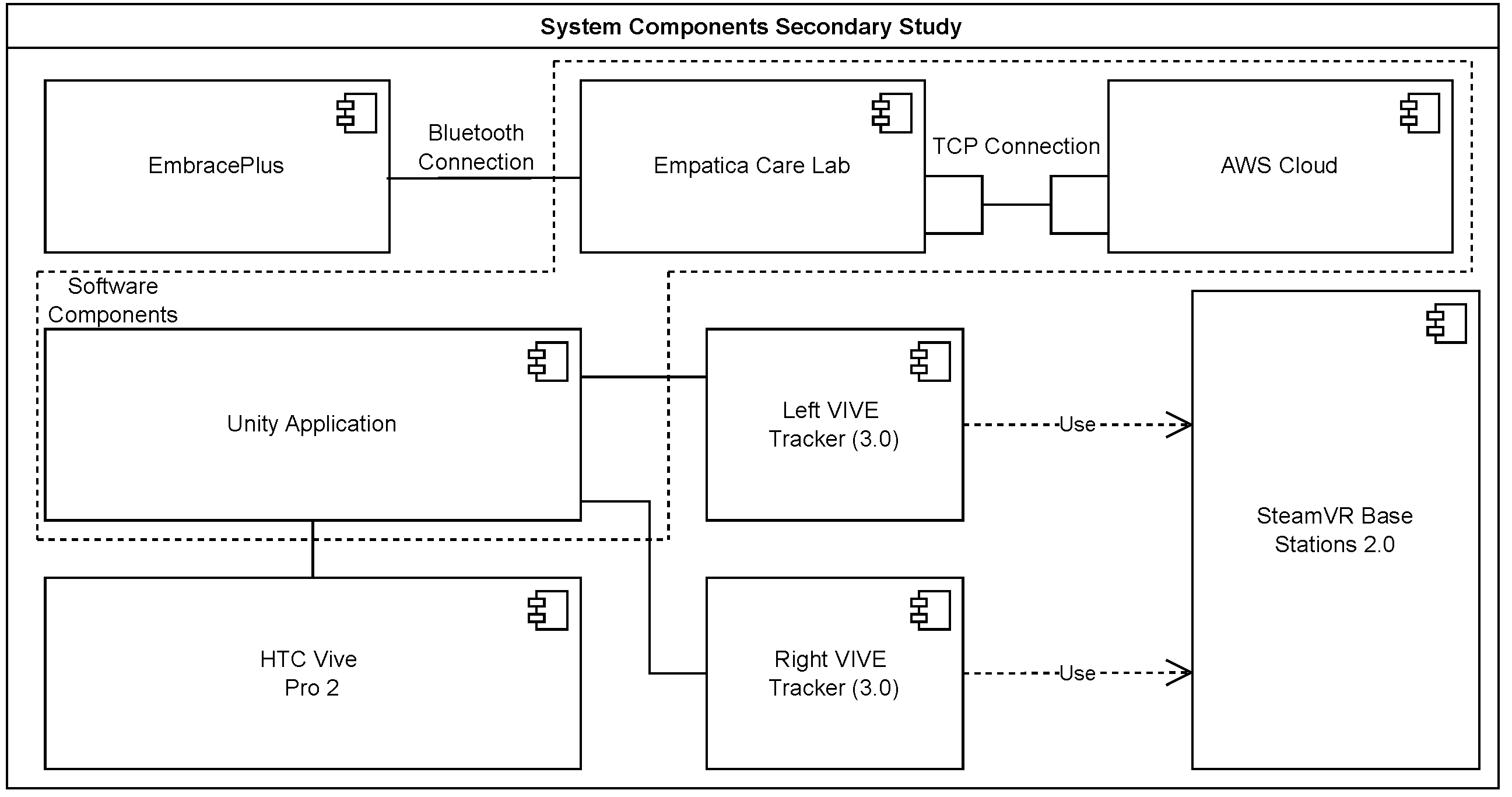
4.2.1. System Architecture
4.2.2. VR Interface
4.2.3. Training Procedure
4.2.4. Training Setup
5. Results
5.1. Main Study of Training System
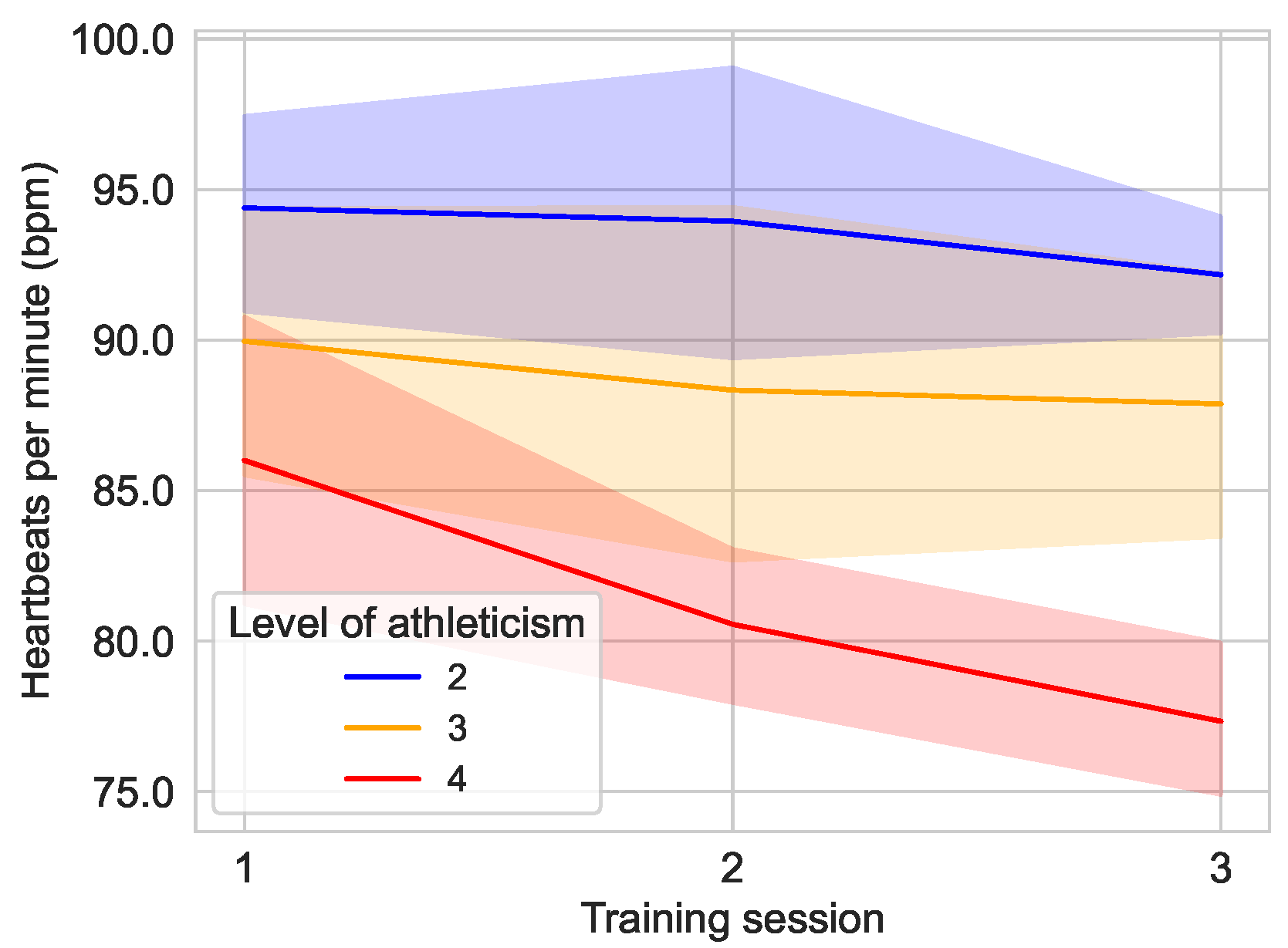
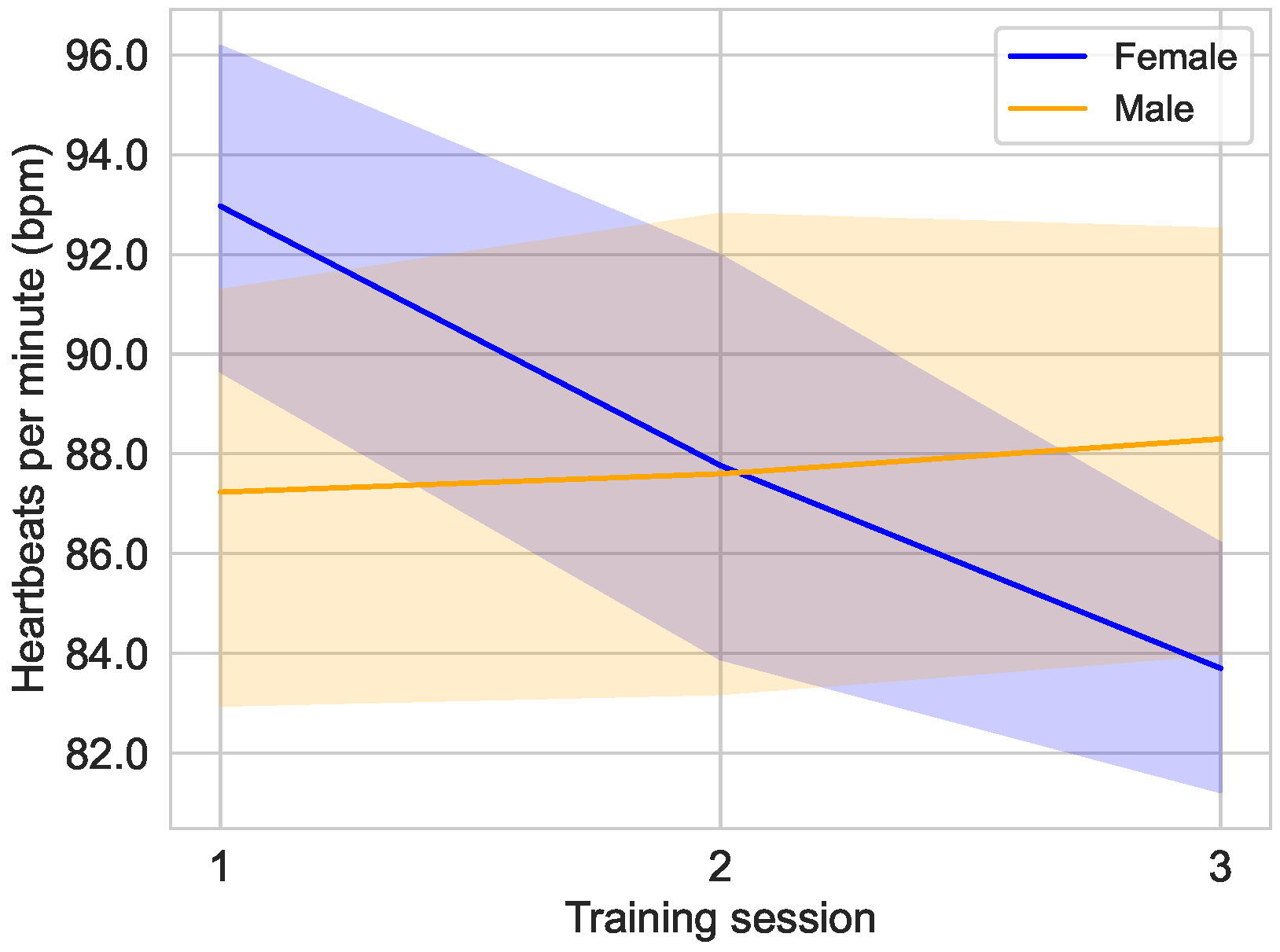
5.1.1. Heart Rate
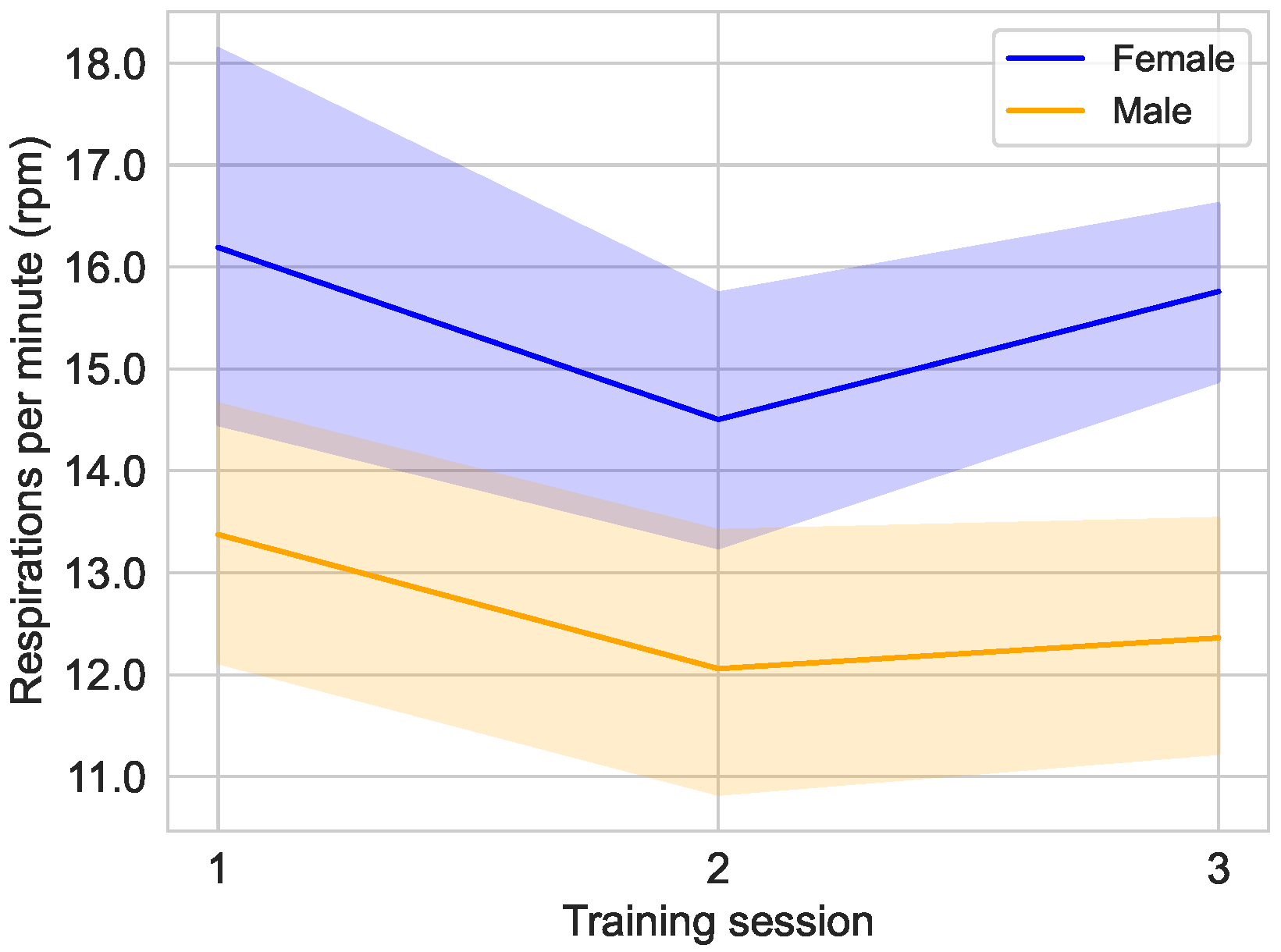
5.1.2. Respiration Rate
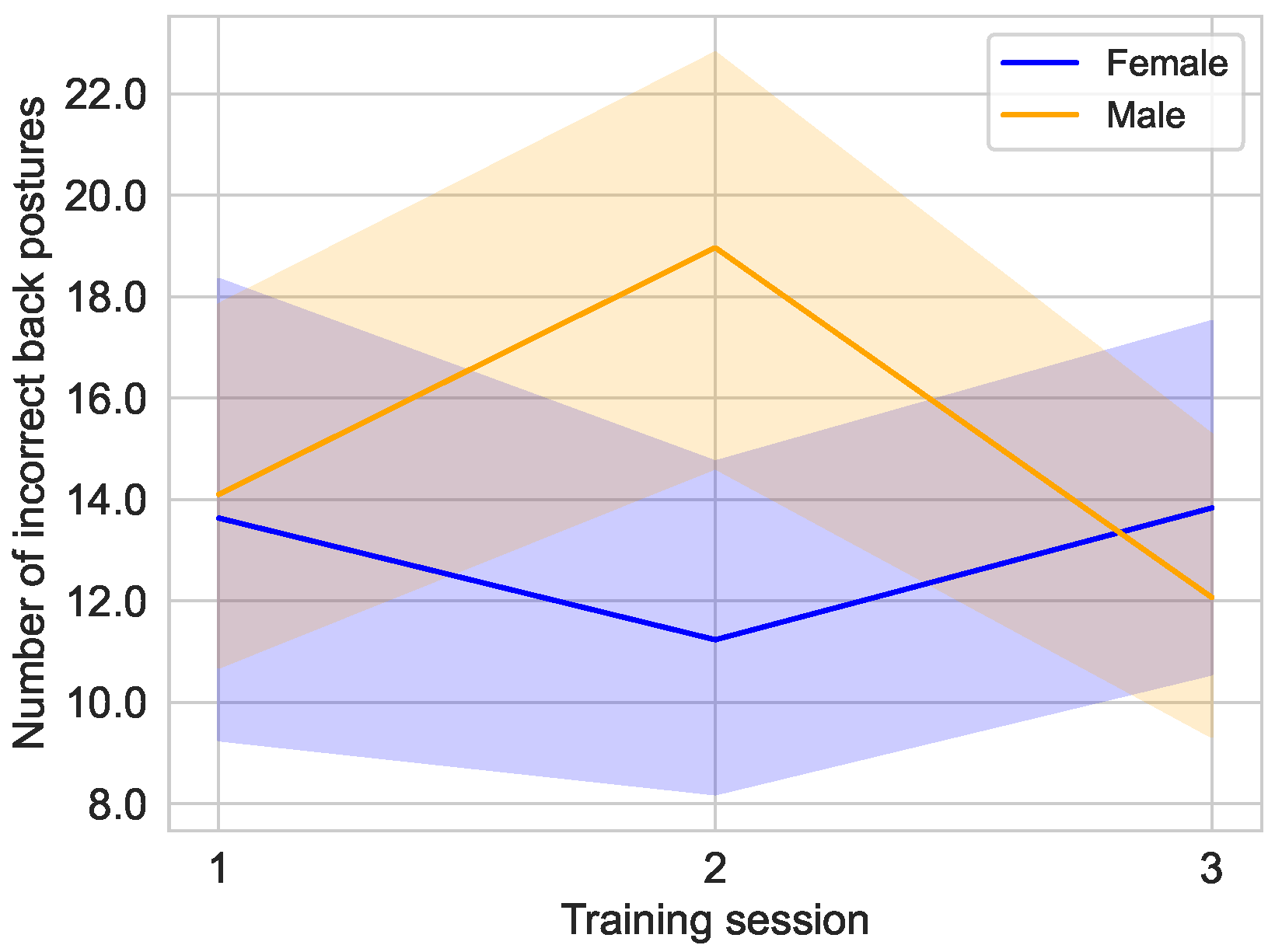
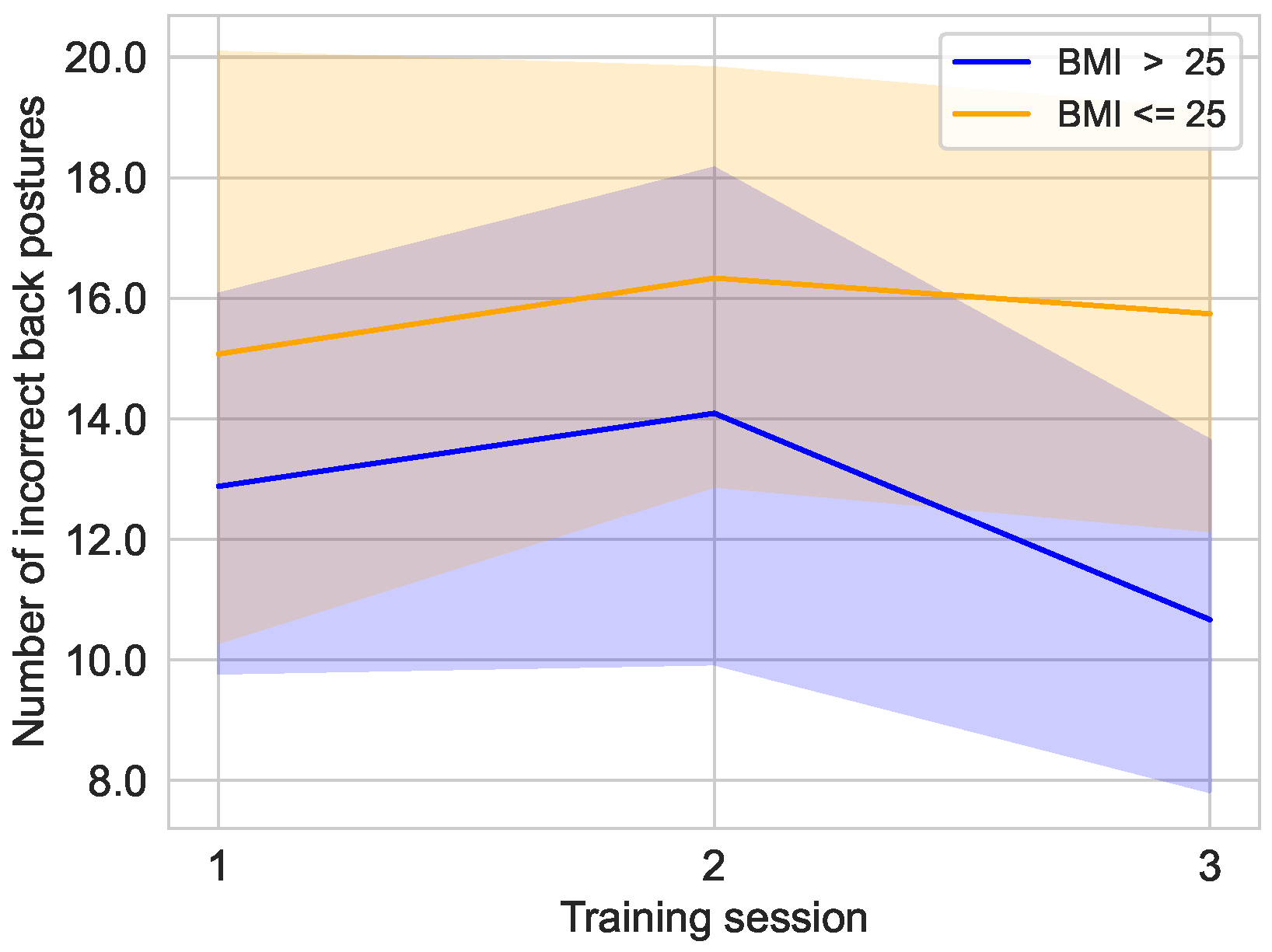
5.1.3. Back Posture
5.2. Secondary Study of VR-Based Exergame
5.2.1. Heart Rate
5.2.2. Game Score
5.2.3. Survey Results
6. Discussion
6.1. Main Study of Training System
6.2. Secondary Study of VR-Based Exergame
6.3. Future Work
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| bpm | Beats per Minute |
| CI | Confidence Interval |
| CSV | Comma Separated Values |
| ECG | Electrocardiography |
| EDA | Electrodermal Activity |
| FDA | U.S. Food and Drug Administration |
| HMD | Head-Mounted Display |
| IR | Infrared |
| MR | Mixed Reality |
| rpm | Respirations per Minute |
| TCP | Transmission Control Protocol |
| VR | Virtual Reality |
References
- Weiss, D.; Rydland, H.T.; Øversveen, E.; Jensen, M.R.; Solhaug, S.; Krokstad, S. Innovative technologies and social inequalities in health: A scoping review of the literature. PLoS ONE 2018, 13, e0195447. [Google Scholar] [CrossRef]
- Senbekov, M.; Saliev, T.; Bukeyeva, Z.; Almabayeva, A.; Zhanaliyeva, M.; Aitenova, N.; Toishibekov, Y.; Fakhradiyev, I. The Recent Progress and Applications of Digital Technologies in Healthcare: A Review. Int. J. Telemed. Appl. 2020, 2020, 8830200. [Google Scholar] [CrossRef]
- Osipov, V.S.; Skryl, T.V. Impact of Digital Technologies on the Efficiency of Healthcare Delivery. In IoT in Healthcare and Ambient Assisted Living; Springer: Singapore, 2021; pp. 243–261. [Google Scholar] [CrossRef]
- Dal Mas, F.; Massaro, M.; Rippa, P.; Secundo, G. The challenges of digital transformation in healthcare: An interdisciplinary literature review, framework, and future research agenda. Technovation 2023, 123, 102716. [Google Scholar] [CrossRef]
- Frederix, I.; Hansen, D.; Coninx, K.; Vandervoort, P.; Vandijck, D.; Hens, N.; Van Craenenbroeck, E.; Van Driessche, N.; Dendale, P. Effect of comprehensive cardiac telerehabilitation on one-year cardiovascular rehospitalization rate, medical costs and quality of life: A cost-effectiveness analysis. Eur. J. Prev. Cardiol. 2015, 23, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Hwang, R.; Bruning, J.; Morris, N.R.; Mandrusiak, A.; Russell, T. Home-based telerehabilitation is not inferior to a centre-based program in patients with chronic heart failure: A randomised trial. J. Physiother. 2017, 63, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Pastora-Bernal, J.M.; Martín-Valero, R.; Barón-López, F.J. Cost analysis of telerehabilitation after arthroscopic subacromial decompression. J. Telemed. Telecare 2017, 24, 553–559. [Google Scholar] [CrossRef]
- Fatoye, F.; Gebrye, T.; Fatoye, C.; Mbada, C.E.; Olaoye, M.I.; Odole, A.C.; Dada, O. The Clinical and Cost-Effectiveness of Telerehabilitation for People With Nonspecific Chronic Low Back Pain: Randomized Controlled Trial. JMIR mHealth uHealth 2020, 8, e15375. [Google Scholar] [CrossRef] [PubMed]
- Kouijzer, M.M.T.E.; Kip, H.; Bouman, Y.H.A.; Kelders, S.M. Implementation of virtual reality in healthcare: A scoping review on the implementation process of virtual reality in various healthcare settings. Implement. Sci. Commun. 2023, 4, 67. [Google Scholar] [CrossRef]
- Worlikar, H.; Coleman, S.; Kelly, J.; O’Connor, S.; Murray, A.; McVeigh, T.; Doran, J.; McCabe, I.; O’Keeffe, D. Mixed Reality Platforms in Telehealth Delivery: Scoping Review. JMIR Biomed. Eng. 2023, 8, e42709. [Google Scholar] [CrossRef]
- Su, Z.; Zhang, L.; Lian, X.; Guan, M. Virtual Reality–Based Exercise Rehabilitation in Cancer-Related Dysfunctions: Scoping Review. J. Med. Internet Res. 2024, 26, e49312. [Google Scholar] [CrossRef]
- Mubin, O.; Alnajjar, F.; Al Mahmud, A.; Jishtu, N.; Alsinglawi, B. Exploring serious games for stroke rehabilitation: A scoping review. Disabil. Rehabil. Assist. Technol. 2020, 17, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Doumas, I.; Everard, G.; Dehem, S.; Lejeune, T. Serious games for upper limb rehabilitation after stroke: A meta-analysis. J. Neuroeng. Rehabil. 2021, 18, 100. [Google Scholar] [CrossRef] [PubMed]
- Vieira, C.; Ferreira da Silva Pais-Vieira, C.; Novais, J.; Perrotta, A. Serious Game Design and Clinical Improvement in Physical Rehabilitation: Systematic Review. JMIR Serious Games 2021, 9, e20066. [Google Scholar] [CrossRef] [PubMed]
- Damaševičius, R.; Maskeliūnas, R.; Blažauskas, T. Serious Games and Gamification in Healthcare: A Meta-Review. Information 2023, 14, 105. [Google Scholar] [CrossRef]
- Meiszl, K.; Potthast, T.; Schulten, T.; Silberbach, M.; Wiswede, D.; Abbassi, P.; Hake, L.; Hussein, V.; de Canaviri, L.K.; Mirraziroudsari, S.D.; et al. App-Guided ICAROS Pro Training via SteamVR Tracking 2.0 and Zephyr BioHarness 3.0. In Proceedings of the 2023 IEEE 12th International Conference on Intelligent Data Acquisition and Advanced Computing Systems: Technology and Applications (IDAACS), Dortmund, Germany, 7–9 September 2023; pp. 430–435. [Google Scholar] [CrossRef]
- Kuhlmann de Canaviri, L.; Meiszl, K.; Hussein, V.; Abbassi, P.; Mirraziroudsari, S.D.; Hake, L.; Potthast, T.; Ratert, F.; Schulten, T.; Silberbach, M.; et al. Static and Dynamic Accuracy and Occlusion Robustness of SteamVR Tracking 2.0 in Multi-Base Station Setups. Sensors 2023, 23, 725. [Google Scholar] [CrossRef]
- Hao, J.; Xie, H.; Harp, K.; Chen, Z.; Siu, K.C. Effects of Virtual Reality Intervention on Neural Plasticity in Stroke Rehabilitation: A Systematic Review. Arch. Phys. Med. Rehabil. 2022, 103, 523–541. [Google Scholar] [CrossRef]
- Chen, J.; Or, C.K.; Chen, T. Effectiveness of Using Virtual Reality–Supported Exercise Therapy for Upper Extremity Motor Rehabilitation in Patients With Stroke: Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Med. Internet Res. 2022, 24, e24111. [Google Scholar] [CrossRef]
- Vassantachart, A.; Yeo, E.; Chau, B. Virtual and Augmented Reality-based Treatments for Phantom Limb Pain: A Systematic Review. Innov. Clin. Neurosci. 2022, 19, 48–57. [Google Scholar]
- Ali, S.G.; Wang, X.; Li, P.; Jung, Y.; Bi, L.; Kim, J.; Chen, Y.; Feng, D.D.; Magnenat Thalmann, N.; Wang, J.; et al. A systematic review: Virtual-reality-based techniques for human exercises and health improvement. Front. Public Health 2023, 11, 1143947. [Google Scholar] [CrossRef]
- Tortora, C.; Di Crosta, A.; La Malva, P.; Prete, G.; Ceccato, I.; Mammarella, N.; Di Domenico, A.; Palumbo, R. Virtual reality and cognitive rehabilitation for older adults with mild cognitive impairment: A systematic review. Ageing Res. Rev. 2024, 93, 102146. [Google Scholar] [CrossRef]
- Dębska, M.; Polechoński, J.; Mynarski, A.; Polechoński, P. Enjoyment and Intensity of Physical Activity in Immersive Virtual Reality Performed on Innovative Training Devices in Compliance with Recommendations for Health. Int. J. Environ. Res. Public Health 2019, 16, 3673. [Google Scholar] [CrossRef] [PubMed]
- Feodoroff, B.; Konstantinidis, I.; Froböse, I. Effects of Full Body Exergaming in Virtual Reality on Cardiovascular and Muscular Parameters: Cross-Sectional Experiment. JMIR Serious Games 2019, 7, e12324. [Google Scholar] [CrossRef] [PubMed]
- Treskunov, A.; Gerhardt, E.; Nowottnik, D.; Fischer, B.; Gerhardt, L.; Säger, M.; Geiger, C. ICAROSmuIti—A VR Test Environment for the Development of Multimodal and Multi-User Interaction Concepts. In Proceedings of the Mensch und Computer 2019, MuC’19, Hamburg, Germany, 8–11 September 2019; ACM: New York, NY, USA, 2019; pp. 909–911. [Google Scholar] [CrossRef]
- Strassmann, C.; Arntz, A.; Eimler, S.C. Under The (Plastic) Sea—Sensitizing People Toward Ecological Behavior Using Virtual Reality Controlled by Users’ Physical Activity. In Proceedings of the 2020 IEEE International Conference on Artificial Intelligence and Virtual Reality (AIVR), Utrecht, The Netherlands, 14–18 December 2020; pp. 166–173. [Google Scholar] [CrossRef]
- Howard, M.C. A meta-analysis and systematic literature review of virtual reality rehabilitation programs. Comput. Hum. Behav. 2017, 70, 317–327. [Google Scholar] [CrossRef]
- Tieri, G.; Morone, G.; Paolucci, S.; Iosa, M. Virtual reality in cognitive and motor rehabilitation: Facts, fiction and fallacies. Expert Rev. Med. Devices 2018, 15, 107–117. [Google Scholar] [CrossRef]
- Villada Castillo, J.F.; Montoya Vega, M.F.; Muñoz Cardona, J.E.; Lopez, D.; Quiñones, L.; Henao Gallo, O.A.; Lopez, J.F. Design of Virtual Reality Exergames for Upper Limb Stroke Rehabilitation Following Iterative Design Methods: Usability Study. JMIR Serious Games 2024, 12, e48900. [Google Scholar] [CrossRef]
- Davis, J.C.; Killen, L.G.; Green, J.M.; Waldman, H.S.; Renfroe, L.G. Exergaming for physical activity: A systematic review. J. Am. Coll. Health J. ACH 2024, 72, 2090–2098. [Google Scholar] [CrossRef]
- Niehorster, D.C.; Li, L.; Lappe, M. The Accuracy and Precision of Position and Orientation Tracking in the HTC Vive Virtual Reality System for Scientific Research. i-Perception 2017, 8, 204166951770820. [Google Scholar] [CrossRef]
- Luckett, E.; Key, T.; Newsome, N.; Jones, J.A. Metrics for the Evaluation of Tracking Systems for Virtual Environments. In Proceedings of the 26th IEEE Conference on Virtual Reality and 3D User Interfaces, Osaka, Japan, 23–27 March 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 1711–1716. [Google Scholar] [CrossRef]
- Bauer, P.; Lienhart, W.; Jost, S. Accuracy Investigation of the Pose Determination of a VR System. Sensors 2021, 21, 1622. [Google Scholar] [CrossRef]
- Holzwarth, V.; Gisler, J.; Hirt, C.; Kunz, A. Comparing the Accuracy and Precision of SteamVR Tracking 2.0 and Oculus Quest 2 in a Room Scale Setup. In Proceedings of the 2021 the 5th International Conference on Virtual and Augmented Reality Simulations, ICVARS 2021, Melbourne, Australia, 20–22 March 2021; ACM: New York, NY, USA, 2021. [Google Scholar] [CrossRef]
- Wang, Y.W.; Chen, C.H.; Lin, Y.C. Balance Rehabilitation System for Parkinson’s Disease Patients based on Augmented Reality. In Proceedings of the 2020 IEEE Eurasia Conference on IOT, Communication and Engineering (ECICE), Yunlin, Taiwan, 23–25 October 2020; pp. 191–194. [Google Scholar] [CrossRef]
- Chen, L.Y.; Chang, L.Y.; Deng, Y.C.; Hsieh, B.C. The Rehabilitation and Assessment in Virtual Reality Game for the patient with Cognitive impairment. In Proceedings of the 2020 International Symposium on Computer, Consumer and Control (IS3C), Taichung City, Taiwan, 13–16 November 2020; pp. 387–390. [Google Scholar] [CrossRef]
- Wen, H.; Zhang, Z.; Lv, C.; Wang, Y.; Hu, Y. Construction of Psychological Training System for College Students Based on Virtual Reality Technology. In Proceedings of the 2022 8th International Conference on Virtual Reality (ICVR), Nanjing, China, 26–28 May 2022; pp. 175–179. [Google Scholar] [CrossRef]
- Lima, G.A.C.d.; Lamounier Junior, E.A.; Melo, B.G.R.V.d.; Soares, A.B.; Silva, A.C.; Cardoso, A. A Markerless Augmented Reality Application for Training Upper Limb Amputees. In Proceedings of the Anais Estendidos do XXIV Simpósio de Realidade Virtual e Aumentada (SVR Estendido 2022). Sociedade Brasileira de Computação, 2022, SVR Estendido 2022, Natal, Brazil, 24–27 October 2022; pp. 28–29. [Google Scholar] [CrossRef]
- Gouveia, É.R.; Campos, P.; França, C.S.; Rodrigues, L.M.; Martins, F.; França, C.; Gonçalves, F.; Teixeira, F.; Ihle, A.; Gouveia, B.R. Virtual Reality Gaming in Rehabilitation after Musculoskeletal Injury—User Experience Pilot Study. Appl. Sci. 2023, 13, 2523. [Google Scholar] [CrossRef]
- Jamieson, A.R.; Singh, I.; Nguyen, D.V.; Waghmare, K.C.; Singh, B.G.C.; Gu, Y.; Wijesundara, M.B.J. Integrating an Assistive Soft Robotic Glove with an Immersive Virtual Reality Hand Rehabilitation Game. In Proceedings of the 2023 IEEE 11th International Conference on Serious Games and Applications for Health (SeGAH), Athens, Greece, 28–30 August 2023; pp. 1–8. [Google Scholar] [CrossRef]
- Bosch-Barceló, P.; Climent-Sanz, C.; Martínez-Navarro, O.; Masbernat-Almenara, M.; Pakarinen, A.; Ghosh, P.K.; Fernández-Lago, H. A treadmill training program in a gamified virtual reality environment combined with transcranial direct current stimulation in Parkinson’s Disease: Study protocol for a randomized controlled trial. PLoS ONE 2024, 19, e0307304. [Google Scholar] [CrossRef]
- De Fazio, R.; Mastronardi, V.M.; De Vittorio, M.; Visconti, P. Wearable Sensors and Smart Devices to Monitor Rehabilitation Parameters and Sports Performance: An Overview. Sensors 2023, 23, 1856. [Google Scholar] [CrossRef]
- Al-Ayyad, M.; Owida, H.A.; De Fazio, R.; Al-Naami, B.; Visconti, P. Electromyography Monitoring Systems in Rehabilitation: A Review of Clinical Applications, Wearable Devices and Signal Acquisition Methodologies. Electronics 2023, 12, 1520. [Google Scholar] [CrossRef]
- Hintz, C.; Presley, D.M.; Butler, C.R. Heat stroke burden and validity of wearable-derived core temperature estimation during elite military training. Physician Sportsmed. 2023, 52, 154–159. [Google Scholar] [CrossRef]
- Romagnoli, S.; Sbrollini, A.; Nocera, A.; Morettini, M.; Gambi, E.; Bondi, D.; Pietrangelo, T.; Verratti, V.; Burattini, L. Sport DB 2.0: A New Database of Data Acquired by Wearable and Portable Devices While Practicing Sport. In Proceedings of the 2023 Computing in Cardiology Conference (CinC), Computing in Cardiology, CinC2023, Atlanta, GA, USA, 1–4 October 2023. [Google Scholar] [CrossRef]
- Sbrollini, A.; Marcantoni, I.; Lunghi, T.; Morettini, M.; Burattini, L. Cardiorespiratory DB: Collection of cardiorespiratory data acquired during normal breathing, deep breathing and breath holding. Data Brief 2024, 54, 110406. [Google Scholar] [CrossRef] [PubMed]
- Citarelli, F. Metrological Characterization of a Wearable Device and a Machine Learning Algorithm for Assessment Of Sport Activities Performances. Master’s Thesis, Università Politecnica delle Marche, Ancona, Italy, 2022. Available online: https://hdl.handle.net/20.500.12075/16688 (accessed on 21 February 2025).
- Cosoli, G.; Antognoli, L.; Panni, L.; Scalise, L. The Indirect Estimation of Breathing Rate through Wearables: Experimental Study and Uncertainty Analysis through Monte Carlo Simulation. In Proceedings of the 2023 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Jeju, Republic of Korea, 14–16 June 2023. [Google Scholar] [CrossRef]
- Panni, L.; Cosoli, G.; Antognoli, L.; Scalise, L. Measurement of respiratory rate with cardiac belt: Metrological characterization. Meas. Sens. 2024, 34, 101244. [Google Scholar] [CrossRef]
- Ray, I.; Liaqat, D.; Gabel, M.; de Lara, E. Skin tone, Confidence, and Data Quality of Heart Rate Sensing in WearOS Smartwatches. In Proceedings of the 2021 IEEE International Conference on Pervasive Computing and Communications Workshops and other Affiliated Events (PerCom Workshops), Kassel, Germany, 22–26 March 2021; pp. 213–219. [Google Scholar] [CrossRef]
- Gashi, S.; Min, C.; Montanari, A.; Santini, S.; Kawsar, F. A multidevice and multimodal dataset for human energy expenditure estimation using wearable devices. Sci. Data 2022, 9, 537. [Google Scholar] [CrossRef]
- Cosoli, G.; Antognoli, L.; Scalise, L. Wearable Electrocardiography for Physical Activity Monitoring: Definition of Validation Protocol and Automatic Classification. Biosensors 2023, 13, 154. [Google Scholar] [CrossRef]
- Cosoli, G.; Antognoli, L.; Panni, L.; Scalise, L. Indirect Estimation of Breathing Rate Using Wearable Devices. IEEE Trans. Instrum. Meas. 2024, 73, 4004708. [Google Scholar] [CrossRef]
- Denyer, H.; Ramos-Quiroga, J.A.; Folarin, A.; Ramos, C.; Nemeth, P.; Bilbow, A.; Woodward, E.; Whitwell, S.; Müller-Sedgwick, U.; Larsson, H.; et al. ADHD Remote Technology study of cardiometabolic risk factors and medication adherence (ART-CARMA): A multi-centre prospective cohort study protocol. BMC Psychiatry 2022, 22, 813. [Google Scholar] [CrossRef]
- Stojchevska, M.; de Brouwer, M.; Courteaux, M.; Steenwinckel, B.; van Hoecke, S.; Ongenae, F. Unlocking the potential of smartphone and ambient sensors for ADL detection. Sci. Rep. 2024, 14, 5392. [Google Scholar] [CrossRef]
- Badawi, A.; Elmoghazy, S.; Choudhury, S.; Elgazzar, S.; Elgazzar, K.; Burhan, A. A Novel Multimodal System to Predict Agitation in People with Dementia Within Clinical Settings: A Proof of Concept. arXiv 2024, arXiv:2411.08882. [Google Scholar] [CrossRef]
- Empatica. EmbracePlus|The World’s Most Advanced Smartwatch for Continuous Health Monitoring. 25 November 2024. Available online: https://www.empatica.com/embraceplus/ (accessed on 21 February 2025).
- Gerboni, G.; Comunale, G.; Chen, W.; Lever Taylor, J.; Migliorini, M.; Picard, R.; Cruz, M.; Regalia, G. Prospective clinical validation of the Empatica EmbracePlus wristband as a reflective pulse oximeter. Front. Digit. Health 2023, 5, 1258915. [Google Scholar] [CrossRef] [PubMed]
- Mologne, M.S.; Yamamoto, T.; Viggiano, M.; Blatney, A.E.; Lechner, R.J.; Nguyen, T.H.; Doyle, A.; Farrales, J.P.; Neufeld, E.V.; Dolezal, B.A. Field-based fitness measures improve via an immersive virtual reality exergaming platform: A randomized controlled trial. Front. Virtual Real. 2024, 5, 1290711. [Google Scholar] [CrossRef]
- Lu, Y.; Ota, K.; Dong, M. An Empirical Study of VR Head-Mounted Displays Based on VR Games Reviews. Games Res. Pract. 2024, 2, 1–20. [Google Scholar] [CrossRef]
- Du, Q.; Song, Z.; Jiang, H.; Wei, X.; Weng, D.; Fan, M. LightSword: A Customized Virtual Reality Exergame for Long-Term Cognitive Inhibition Training in Older Adults. In Proceedings of the CHI Conference on Human Factors in Computing Systems, Honolulu, HI, USA, 11–16 May 2024; ACM: New York, NY, USA, 2024; pp. 1–17. [Google Scholar] [CrossRef]
- Olberding, H.; Vetter, M. Analysis of Cartographic Symbols as Visual Support in Interactive VR Geovisualizations. Proc. ICA 2023, 5, 1–6. [Google Scholar] [CrossRef]
- Polat, M.D.; Izzetoglu, K.; Aksoy, M.E.; Kitapcioglu, D.; Usseli, T.; Yoner, S.I. Cognitive Load Quantified via Functional Near Infrared Spectroscopy During Immersive Training with VR Based Basic Life Support Learning Modules in Hostile Environment. In Proceedings of the Augmented Cognition; Schmorrow, D.D., Fidopiastis, C.M., Eds.; Springer: Cham, switzerland, 2023; pp. 359–372. [Google Scholar]
- ICAROS GmbH. ICAROS Tablet Holder Universal. Technical Report, ICAROS GmbH, Martinsried, Germany. 2022. Available online: https://www.icaros.com/fileadmin/user_upload/ICAROS_Tablet_Holder_Universal_-_Installation__Home__Pro__Health_.pdf (accessed on 22 February 2025).
- Sbrollini, A.; Bondi, D.; Romagnoli, S.; Morettini, M.; Marcantoni, I.; Pietrangelo, T.; Verratti, V.; Burattini, L. Segmented-Beat Modulation Method-Based Procedure for Extraction of Electrocardiogram-Derived Respiration from Data Acquired by Wearable Sensors During High-Altitude Activity. In Proceedings of the 2022 Computing in Cardiology Conference (CinC). Computing in Cardiology, CinC2022, Tampere, Finland, 4–7 September 2022. [Google Scholar] [CrossRef]
- Brooke, J. SUS: A ’Quick and Dirty’ Usability Scale. In Usability Evaluation In Industry; CRC Press: Boca Raton, FL, USA, 1996; pp. 207–212. [Google Scholar] [CrossRef]
- Laugwitz, B.; Held, T.; Schrepp, M. Construction and Evaluation of a User Experience Questionnaire. In HCI and Usability for Education and Work; Springer: Berlin/Heidelberg, Germany, 2008; pp. 63–76. [Google Scholar] [CrossRef]
- Schubert, T.; Friedmann, F.; Regenbrecht, H. The Experience of Presence: Factor Analytic Insights. Presence Teleoperators Virtual Environ. 2001, 10, 266–281. [Google Scholar] [CrossRef]
- Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal, M.G. Simulator Sickness Questionnaire: An Enhanced Method for Quantifying Simulator Sickness. Int. J. Aviat. Psychol. 1993, 3, 203–220. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sport. Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Berkman, M.İ.; ÇATAK, G. I-group presence questionnaire: Psychometrically revised English version. Mugla J. Sci. Technol. 2021, 7, 1–10. [Google Scholar] [CrossRef]
- Williams, N. The Borg Rating of Perceived Exertion (RPE) scale. Occup. Med. 2017, 67, 404–405. [Google Scholar] [CrossRef]
- Phan, M.H.; Keebler, J.R.; Chaparro, B.S. The Development and Validation of the Game User Experience Satisfaction Scale (GUESS). Hum. Factors 2016, 58, 1217–1247. [Google Scholar] [CrossRef] [PubMed]
- Sweetser, P.; Wyeth, P. GameFlow. Comput. Entertain. 2005, 3, 3. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Manifestation | ||
|---|---|---|---|
| Sex | M () | F () | All () |
| Mean ± standard deviation | |||
| Age (years) | |||
| Height (m) | |||
| Weight (kg) | |||
| BMI | |||
| Self-assigned fitness | |||
| Feature | Manifestation | ||
|---|---|---|---|
| Sex | M () | F () | All () |
| Mean ± standard deviation | |||
| Age (years) | |||
| Height (m) | |||
| Weight (kg) | |||
| BMI | |||
| Self-assigned fitness | |||
| 2-4 Prior VR experience | () | () | () |
| Key | Question | Type | Scope | Ref. |
|---|---|---|---|---|
| Usability | How do you rate the VR system usability? | Likert | 1–5 (Low–High) | [66] |
| Immersion | How do you rate the exergame immersion? | Likert | 1–5 (Low–High) | [71] |
| Adversities | Did you experience adverse effects (e.g., dizziness, nausea)? | Binary | Yes/No (+ optional free text) | [69] |
| Effectiveness | How do you rate the exergame effectiveness for building muscle? | Likert | 1–5 (Low–High) | – |
| Muscles | Which muscle groups were strained most? | Multiple | Arms, Legs, Back, Abdomen, Chest | – |
| Exhaustion | How do you rate the physical exhaustion during the game compared to traditional training? | Likert | 1–5 (Low–High) | [70,72] |
| Fun | How would you rate the fun factor of the game? | Likert | 1–5 (Low–High) | [73] |
| Motivation | How motivating do you find the game mechanics for continuous training? | Likert | 1–5 (Low–High) | – |
| Balancing | How balanced is the game in terms of challenges and rewards? | Likert | 1–5 (Poor–Good) | [74] |
| Graphics | How would you rate the game graphics quality? | Likert | 1–5 (Poor–Good) | – |
| Bugs | Were there any technical problems or bugs? | Binary | Yes/No (+ optional free text) | – |
| Satisfaction | How satisfied are you with the exergame? | Likert | 1–5 (Low–High) | – |
| Recommendation | Would you recommend the game to others? | Binary | Yes/No (+ optional free text) | – |
| Enjoyment | Did you enjoy any particular aspects? | Free text | – | – |
| Improvement | What could be improved for a better training experience? | Free text | – | – |
| Feedback | Do you have any comments or suggestions? | Free text | – | – |
| Setting | Pose Goals with Holding Time | ||||||
|---|---|---|---|---|---|---|---|
| Goal | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| X/Roll axis (°) | 0 | ||||||
| Y/Pitch axis (°) | |||||||
| Time (s) | 10 | 7 | 7 | 7 | 7 | 7 | 7 |
| Training Session | Task | Pose Goals | ||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 1 | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| 2 | 1 | 5 | 4 | 7 | 6 | 3 | 2 | |
| 3 | 1 | 6 | 7 | 2 | 3 | 4 | 5 | |
| 2 | 3 | 1 | 6 | 7 | 2 | 3 | 4 | 5 |
| 2 | 1 | 5 | 4 | 7 | 6 | 3 | 2 | |
| 1 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
| 3 | 2 | 1 | 5 | 4 | 7 | 6 | 3 | 2 |
| 1 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
| 3 | 1 | 6 | 7 | 2 | 3 | 4 | 5 | |
| Training Session | Mean ± Standard Deviation | Minimum | Maximum |
|---|---|---|---|
| 1 | |||
| 2 | |||
| 3 |
| Training Session | Mean ± Standard Deviation | Minimum | Maximum |
|---|---|---|---|
| 1 | |||
| 2 | |||
| 3 |
| Training Session | Mean ± Standard Deviation | Minimum | Maximum |
|---|---|---|---|
| 1 | |||
| 2 | |||
| 3 |
| Training Session | Mean ± Standard Deviation | Median | 95% CI |
|---|---|---|---|
| 1 | [] | ||
| 2 a | [] | ||
| 3 | [] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meiszl, K.; Ratert, F.; Schulten, T.; Wiswede, D.; Kuhlmann de Canaviri, L.; Potthast, T.; Silberbach, M.; Hake, L.; Warnecke, Y.; Schiprowski, W.; et al. Conventional Training Integrated with SteamVR Tracking 2.0: Body Stability and Coordination Training Evaluation on ICAROS Pro. Sensors 2025, 25, 2840. https://doi.org/10.3390/s25092840
Meiszl K, Ratert F, Schulten T, Wiswede D, Kuhlmann de Canaviri L, Potthast T, Silberbach M, Hake L, Warnecke Y, Schiprowski W, et al. Conventional Training Integrated with SteamVR Tracking 2.0: Body Stability and Coordination Training Evaluation on ICAROS Pro. Sensors. 2025; 25(9):2840. https://doi.org/10.3390/s25092840
Chicago/Turabian StyleMeiszl, Katharina, Fabian Ratert, Tessa Schulten, Daniel Wiswede, Lara Kuhlmann de Canaviri, Tobias Potthast, Marc Silberbach, Laurin Hake, Yannik Warnecke, Witold Schiprowski, and et al. 2025. "Conventional Training Integrated with SteamVR Tracking 2.0: Body Stability and Coordination Training Evaluation on ICAROS Pro" Sensors 25, no. 9: 2840. https://doi.org/10.3390/s25092840
APA StyleMeiszl, K., Ratert, F., Schulten, T., Wiswede, D., Kuhlmann de Canaviri, L., Potthast, T., Silberbach, M., Hake, L., Warnecke, Y., Schiprowski, W., Merschhemke, M., Friedrich, C. M., & Brüngel, R. (2025). Conventional Training Integrated with SteamVR Tracking 2.0: Body Stability and Coordination Training Evaluation on ICAROS Pro. Sensors, 25(9), 2840. https://doi.org/10.3390/s25092840