
A Novel Bilateral Data Fusion Approach for EMG-Driven Deep Learning in Post-Stroke Paretic Gesture Recognition
 , , ,
, , ,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
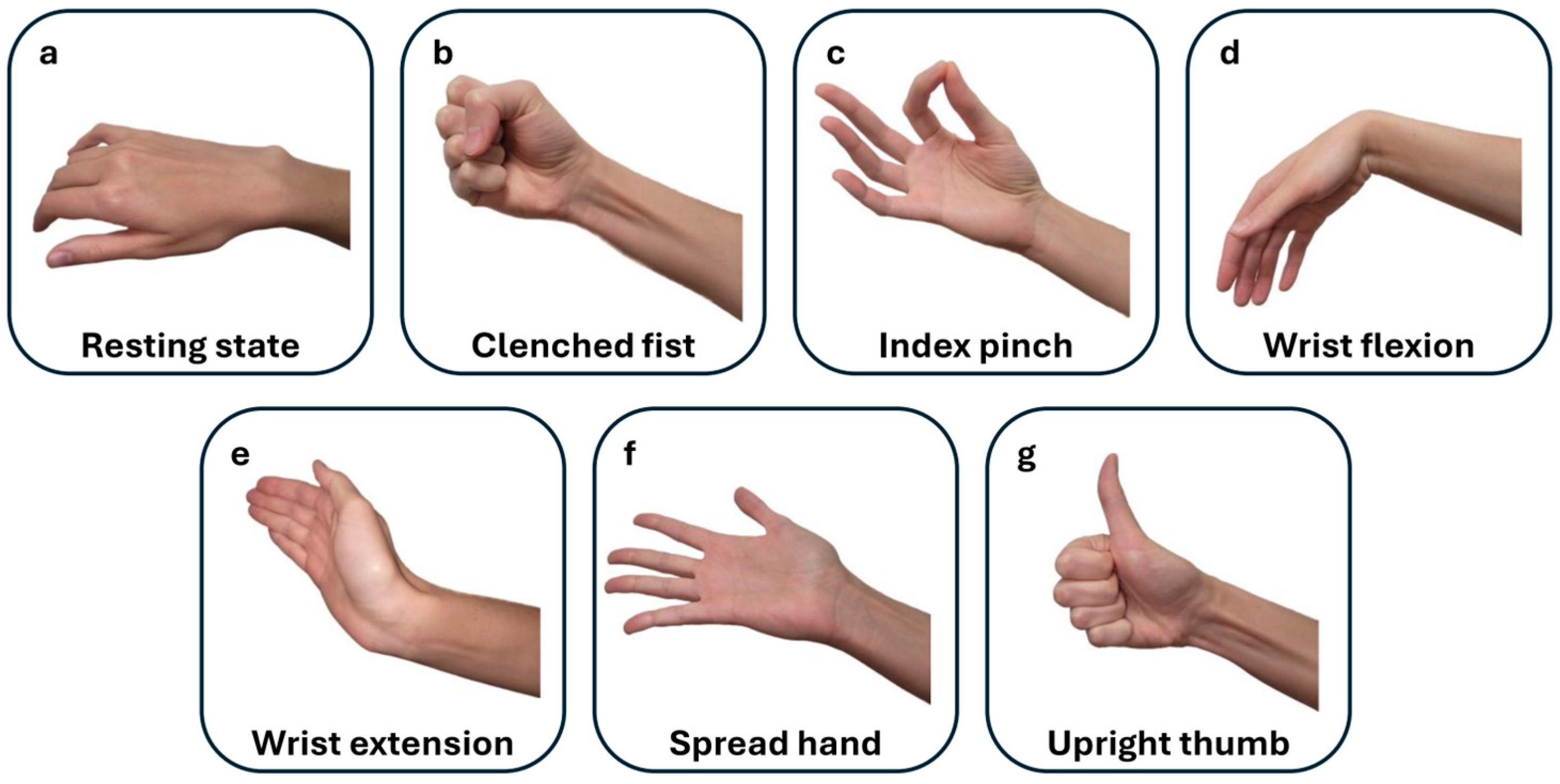
2.1. Data Gathering Outlines
2.2. Deep Neural Network Architecture
2.3. Model Metrics and Evaluation
3. Results
3.1. Post-Stroke Patients
3.2. Observed Network Performance
3.3. AUC-ROC Visualization for Paretic and Fused EMG Classification
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yeung, A.W.K.; Torkamani, A.; Butte, A.J.; Glicksberg, B.S.; Schuller, B.; Rodriguez, B.; Ting, D.S.; Bates, D.; Schaden, E.; Peng, H.; et al. The Promise of Digital Healthcare Technologies. Front. Public Health 2023, 11, 1196596. [Google Scholar] [CrossRef]
- Sumner, J.; Lim, H.W.; Chong, L.S.; Bundele, A.; Mukhopadhyay, A.; Kayambu, G. Artificial Intelligence in Physical Rehabilitation: A Systematic Review. Artif. Intell. Med. 2023, 146, 102693. [Google Scholar] [CrossRef]
- O’Brien, M.K.; Lanotte, F.; Khazanchi, R.; Shin, S.Y.; Lieber, R.L.; Ghaffari, R.; Rogers, J.A.; Jayaraman, A. Early Prediction of Poststroke Rehabilitation Outcomes Using Wearable Sensors. Phys. Ther. 2024, 104, pzad183. [Google Scholar] [CrossRef]
- Sakamoto, D.; Hamaguchi, T.; Nakayama, Y.; Hada, T.; Abo, M. Upper-Limb Functional Recovery in Chronic Stroke Patients after COVID-19-Interrupted Rehabilitation: An Observational Study. J. Clin. Med. 2024, 13, 2212. [Google Scholar] [CrossRef]
- Lang, C.E.; Waddell, K.J.; Barth, J.; Holleran, C.L.; Strube, M.J.; Bland, M.D. Upper Limb Performance in Daily Life Approaches Plateau Around Three to Six Weeks Post-Stroke. Neurorehabilit. Neural Repair 2021, 35, 903–914. [Google Scholar] [CrossRef]
- Yamamoto, H.; Takeda, K.; Koyama, S.; Morishima, K.; Hirakawa, Y.; Motoya, I.; Sakurai, H.; Kanada, Y.; Kawamura, N.; Kawamura, M.; et al. Relationship between Upper Limb Motor Function and Activities of Daily Living after Removing the Influence of Lower Limb Motor Function in Subacute Patients with Stroke: A Cross-Sectional Study. Hong Kong J. Occup. Ther. 2020, 33, 12–17. [Google Scholar] [CrossRef]
- Mubin, O.; Alnajjar, F.; Jishtu, N.; Alsinglawi, B.; Al Mahmud, A. Exoskeletons with Virtual Reality, Augmented Reality, and Gamification for Stroke Patients’ Rehabilitation: Systematic Review. JMIR Rehabil. Assist. Technol. 2019, 6, e12010. [Google Scholar] [CrossRef]
- Sengupta, N.; Rao, A.S.; Yan, B.; Palaniswami, M. A Survey of Wearable Sensors and Machine Learning Algorithms for Automated Stroke Rehabilitation. IEEE Access 2024, 12, 36026–36054. [Google Scholar] [CrossRef]
- Xiong, D.; Zhang, D.; Zhao, X.; Zhao, Y. Deep Learning for EMG-Based Human-Machine Interaction: A Review. IEEE/CAA J. Autom. Sin. 2021, 8, 512–533. [Google Scholar] [CrossRef]
- Bao, T.; Lu, Z.; Zhou, P. Deep Learning-Based Post-Stroke Myoelectric Gesture Recognition: From Feature Construction to Network Design. IEEE Trans. Neural Syst. Rehabil. Eng. 2025, 33, 191–200. [Google Scholar] [CrossRef]
- Nasri, N.; Orts-Escolano, S.; Cazorla, M. An sEMG-Controlled 3D Game for Rehabilitation Therapies: Real-Time Time Hand Gesture Recognition Using Deep Learning Techniques. Sensors 2020, 20, 6451. [Google Scholar] [CrossRef]
- Jochumsen, M.; Niazi, I.K.; Zia ur Rehman, M.; Amjad, I.; Shafique, M.; Gilani, S.O.; Waris, A. Decoding Attempted Hand Movements in Stroke Patients Using Surface Electromyography. Sensors 2020, 20, 6763. [Google Scholar] [CrossRef]
- Anastasiev, A.; Kadone, H.; Marushima, A.; Watanabe, H.; Zaboronok, A.; Watanabe, S.; Matsumura, A.; Suzuki, K.; Matsumaru, Y.; Ishikawa, E. Supervised Myoelectrical Hand Gesture Recognition in Post-Acute Stroke Patients with Upper Limb Paresis on Affected and Non-Affected Sides. Sensors 2022, 22, 8733. [Google Scholar] [CrossRef]
- Anastasiev, A.; Kadone, H.; Marushima, A.; Watanabe, H.; Zaboronok, A.; Watanabe, S.; Matsumura, A.; Suzuki, K.; Matsumaru, Y.; Ishikawa, E. Empirical Myoelectric Feature Extraction and Pattern Recognition in Hemiplegic Distal Movement Decoding. Bioengineering 2023, 10, 866. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Van De Ven, S.S.; Liu, L.; Wouda, F.J.; Wang, H.; Shull, P.B. Activities of Daily Living-Based Rehabilitation System for Arm and Hand Motor Function Retraining After Stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2022, 30, 621–631. [Google Scholar] [CrossRef]
- Guo, K.; Orban, M.; Lu, J.; Al-Quraishi, M.S.; Yang, H.; Elsamanty, M. Empowering Hand Rehabilitation with AI-Powered Gesture Recognition: A Study of an sEMG-Based System. Bioengineering 2023, 10, 557. [Google Scholar] [CrossRef]
- Burns, A.; Adeli, H.; Buford, J.A. Upper Limb Movement Classification via Electromyographic Signals and an Enhanced Probabilistic Network. J. Med. Syst. 2020, 44, 176. [Google Scholar] [CrossRef]
- Atzori, M.; Cognolato, M.; Müller, H. Deep Learning with Convolutional Neural Networks Applied to Electromyography Data: A Resource for the Classification of Movements for Prosthetic Hands. Front. Neurorobot. 2016, 10, 9. [Google Scholar] [CrossRef]
- Vijayvargiya, A.; Khimraj; Kumar, R.; Dey, N. Voting-Based 1D CNN Model for Human Lower Limb Activity Recognition Using sEMG Signal. Phys. Eng. Sci. Med. 2021, 44, 1297–1309. [Google Scholar] [CrossRef]
- Wang, L.; Fu, J.; Chen, H.; Zheng, B. Hand Gesture Recognition Using Smooth Wavelet Packet Transformation and Hybrid CNN Based on Surface EMG and Accelerometer Signal. Biomed. Signal Process. Control 2023, 86, 105141. [Google Scholar] [CrossRef]
- Toro-Ossaba, A.; Jaramillo-Tigreros, J.; Tejada, J.C.; Peña, A.; López-González, A.; Castanho, R.A. LSTM Recurrent Neural Network for Hand Gesture Recognition Using EMG Signals. Appl. Sci. 2022, 12, 9700. [Google Scholar] [CrossRef]
- López, L.I.B.; Ferri, F.M.; Zea, J.; Caraguay, Á.L.V.; Benalcázar, M.E. CNN-LSTM and Post-Processing for EMG-Based Hand Gesture Recognition. Intell. Syst. Appl. 2024, 22, 200352. [Google Scholar] [CrossRef]
- Bao, T.; Zaidi, S.A.R.; Xie, S.; Yang, P.; Zhang, Z.Q. A CNN-LSTM Hybrid Model for Wrist Kinematics Estimation Using Surface Electromyography. IEEE Trans. Instrum. Meas. 2020, 70, 1–9. [Google Scholar] [CrossRef]
- Li, H.; Guo, S.; Bu, D.; Wang, H.; Kawanishi, M. Subject-Independent Estimation of Continuous Movements Using CNN-LSTM for a Home-Based Upper Limb Rehabilitation System. IEEE Robot. Autom. Lett. 2023, 8, 6403–6410. [Google Scholar] [CrossRef]
- Karnam, N.K.; Dubey, S.R.; Turlapaty, A.C.; Gokaraju, B. EMGHandNet: A Hybrid CNN and Bi-LSTM Architecture for Hand Activity Classification Using Surface EMG Signals. Biocybern. Biomed. Eng. 2022, 42, 325–340. [Google Scholar] [CrossRef]
- Zea, J.A.; Santillán, L.G.M.; López, L.I.B.; Caraguay, Á.L.V.; Benalcázar, M.E. Effects on Hand Gesture Recognition Accuracy after Severe Cranial Trauma. In Proceedings of the 2023 IEEE Seventh Ecuador Technical Chapters Meeting (ECTM), Ambato, Ecuador, 10–13 October 2023; pp. 1–5. [Google Scholar] [CrossRef]
- Olsen, C.D.; Hamrick, W.C.; Lewis, S.R.; Iverson, M.M.; George, J.A. Wrist EMG Improves Gesture Classification for Stroke Patients. In Proceedings of the 2023 International Conference on Rehabilitation Robotics (ICORR), Singapore, 24–28 September 2023; pp. 1–6. [Google Scholar] [CrossRef]
- Sobinov, A.R.; Bensmaia, S.J. The Neural Mechanisms of Manual Dexterity. Nat. Rev. Neurosci. 2021, 22, 741–757. [Google Scholar] [CrossRef]
- Bae, J.H.; Kang, S.H.; Seo, K.M.; Kim, D.K.; Shin, H.I.; Shin, H.E. Relationship Between Grip and Pinch Strength and Activities of Daily Living in Stroke Patients. Ann. Rehabil. Med. 2015, 39, 752–762. [Google Scholar] [CrossRef]
- Schambra, H.M.; Xu, J.; Branscheidt, M.; Lindquist, M.; Uddin, J.; Steiner, L.; Hertler, B.; Kim, N.; Berard, J.; Harran, M.D.; et al. Differential Poststroke Motor Recovery in an Arm Versus Hand Muscle in the Absence of Motor Evoked Potentials. Neurorehabil. Neural Repair 2019, 33, 568–580. [Google Scholar] [CrossRef]
- Xu, J.; Haith, A.M.; Krakauer, J.W. Motor control of the hand before and after stroke. In Clinical Systems Neuroscience, 1st ed.; Iriki, J., Yuasa, S., Eds.; Springer: Tokyo, Japan, 2015; pp. 271–289. [Google Scholar] [CrossRef]
- Silva, C.C.; Silva, A.; Sousa, A.; Pinheiro, A.R.; Bourlinova, C.; Silva, A.; Salazar, A.; Borges, C.; Crasto, C.; Correia, M.V.; et al. Co-activation of upper limb muscles during reaching in post-stroke subjects: An analysis of the contralesional and ipsilesional limbs. J. Electromyogr. Kinesiol. 2014, 24, 731–738. [Google Scholar] [CrossRef]
- Sheng, W.; Li, S.; Zhao, J.; Wang, Y.; Luo, Z.; Lo, W.L.A.; Ding, M.; Wang, C.; Li, L. Upper limbs muscle co-contraction changes correlated with the impairment of the corticospinal tract in stroke survivors: Preliminary evidence from electromyography and motor-evoked potential. Front. Neurosci. 2022, 16, 886909. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Trial | Patient No. | Age | Sex | Stroke Type | Onset (Days) | FMA-UE | Paretic Extremity |
|---|---|---|---|---|---|---|---|
| R02-204 (input data for datasets A and B) | S001 | 80 | M | CI | 11 | 58 | R |
| S002 | 32 | F | CI | 11 | 50 | R | |
| S003 | 71 | M | ICH | 13 | 64 | R | |
| S004 | 52 | F | CI | 8 | 63 | L | |
| S005 | 82 | M | CI | 9 | 27 | L | |
| S006 | 81 | M | ICH | 5 | 16 | R | |
| S007 | 77 | M | CI | 9 | 60 | R | |
| S008 | 79 | F | ICH | 7 | 28 | R | |
| S009 | 65 | M | ICH | 5 | 55 | R | |
| S010 | 67 | F | ICH | 12 | 37 | L | |
| S011 | 66 | M | CI | 13 | 15 | L | |
| S011 | 66 | M | CI | 13 | 15 | L | |
| S012 | 64 | F | ICH | 33 | 35 | L | |
| S013 | 63 | M | CI | 13 | 59 | R | |
| S014 | 50 | M | CI | 19 | 22 | R | |
| S015 | 72 | F | CI | 16 | 52 | R | |
| S016 | 57 | M | ICH | 12 | 42 | L | |
| S017 | 57 | M | ICH | 18 | 8 | L | |
| S018 | 64 | M | CI | 9 | 60 | R | |
| S019 | 74 | F | CI | 12 | 9 | L | |
| R04-041 (measurements from session A were allocated to dataset A, and measurements from session B were allocated to dataset B) | S020-A | 75 | M | CI | 24 | 10 | L |
| S020-B | 45 | 10 | |||||
| S021-A | 74 | M | ICH | 26 | 10 | L | |
| S021-B | 34 | 13 | |||||
| S022-A | 57 | M | ICH | 25 | 15 | R | |
| S022-B | 34 | 24 | |||||
| S023-A | 70 | M | ICH | 23 | 55 | L | |
| S023-B | 31 | 56 | |||||
| S024-A | 80 | M | CI | 34 | 47 | L | |
| S024-B | 47 | 54 | |||||
| S025-A | 51 | M | ICH | 31 | 16 | L | |
| S025-B | 50 | 17 |
| Model | EMG Type | SENS ± SD (%) | p-Value | SP ± SD (%) | p-Value | ACC ± SD (%) | p-Value | F1 ± SD (%) | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| 2G-A | Paretic | 66.69 ± 16.53 | 0.2444 | 66.69 ± 16.53 | 0.2444 | 85.66 ± 14.65 | 0.118 | 64.05 ± 18.90 | 0.1008 |
| Fusion | 64.31 ± 11.90 | 64.31 ± 11.90 | 82.90 ± 9.64 | 60.44 ± 11.07 | |||||
| 3G-A | Paretic | 49.00 ± 10.08 | 2.6326 × 10−12 **** | 76.15 ± 6.57 | 6.478 × 10−10 **** | 73.01 ± 9.20 | 1.1939 × 10−5 **** | 45.46 ± 13.55 | 1.5866 × 10−10 **** |
| Fusion | 59.54 ± 9.90 | 81.82 ± 6.07 | 78.42 ± 7.76 | 57.92 ± 12.55 | |||||
| 4G-A | Paretic | 47.36 ± 9.99 | 0.277 | 84.34 ± 4.21 | 0.4839 | 78.37 ± 6.20 | 0.6892 | 45.74 ± 11.77 | 0.0637 |
| Paretic | 48.78 ± 8.40 | 84.71 ± 3.08 | 78.68 ± 4.60 | 48.57 ± 9.63 | |||||
| 5G-A | Paretic | 42.91 ± 10.46 | 2.3245 × 10−4 **** | 87.12 ± 3.10 | 0.0483 * | 79.93 ± 5.15 | 0.0287 * | 39.28 ± 10.07 | 1.4523 × 10−8 **** |
| Fusion | 47.57 ± 6.69 | 87.86 ± 2.05 | 81.28 ± 3.30 | 46.71 ± 7.52 | |||||
| 6G-A | Paretic | 37.77 ± 8.64 | 1.2787 × 10−5 **** | 88.18 ± 2.12 | 0.0054 ** | 80.64 ± 3.75 | 0.0083 ** | 33.17 ± 8.84 | 6.543 × 10−12 **** |
| Fusion | 43.24 ± 8.62 | 89.00 ± 1.99 | 81.99 ± 3.37 | 42.68 ± 9.55 | |||||
| 7G-A | Paretic | 33.99 ± 8.00 | 0.0592 | 89.50 ± 1.59 | 0.5087 | 82.27 ± 2.86 | 0.5768 | 30.34 ± 7.69 | 2.3736 × 10−5 **** |
| Fusion | 35.99 ± 6.90 | 89.64 ± 1.25 | 82.47 ± 2.26 | 35.11 ± 7.88 | |||||
| 6G-NR-A | Paretic | 40.14 ± 8.85 | 0.4942 | 88.04 ± 1.78 | 0.4910 | 80.09 ± 2.95 | 0.5113 | 36.42 ± 7.99 | 0.0023 ** |
| Fusion | 40.96 ± 8.13 | 88.21 ± 1.63 | 80.36 ± 2.72 | 40.02 ± 8.51 |
| Model | EMG Type | SENS ± SD (%) | p-Value | SP ± SD (%) | p-Value | ACC ± SD (%) | p-Value | F1 ± SD (%) | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| 2G-B | Paretic | 57.09 ± 10.35 | 0.0012 ** | 57.09 ± 10.35 | 0.0012 ** | 88.36 ± 12.07 | 0.0448 * | 57.72 ± 14.39 | 0.156 |
| Fusion | 62.00 ± 10.79 | 62.00 ± 10.79 | 84.75 ± 13.17 | 60.51 ± 13.33 | |||||
| 3G-B | Paretic | 52.58 ± 11.38 | 1.3226 × 10−10 **** | 79.10 ± 7.79 | 1.3900 × 10−12 **** | 77.95 ± 8.30 | 7.5559 × 10−12 **** | 52.45 ± 13.79 | 3.1825 × 10−6 **** |
| Fusion | 63.54 ± 11.48 | 86.58 ± 6.07 | 85.69 ± 6.63 | 65.39 ± 13.17 | |||||
| 4G-B | Paretic | 43.81 ± 9.40 | 2.9325 × 10−5 **** | 83.43 ± 3.91 | 0.0156 * | 77.2 ± 5.82 | 0.031 * | 42.36 ± 11.05 | 3.1825 × 10−6 **** |
| Paretic | 48.91 ± 7.34 | 84.63 ± 2.97 | 78.78 ± 4.31 | 49.10 ± 8.69 | |||||
| 5G-B | Paretic | 45.08 ± 10.59 | 0.0119 * | 87.44 ± 3.02 | 0.0241 * | 80.84 ± 4.81 | 0.0287 * | 43.23 ± 11.22 | 2.5175 × 10−4 **** |
| Fusion | 48.51 ± 8.37 | 88.30 ± 2.26 | 82.15 ± 3.56 | 48.70 ± 9.48 | |||||
| 6G-B | Paretic | 40.40 ± 11.09 | 0.0128 * | 88.54 ± 2.28 | 0.0043 ** | 81.50 ± 3.71 | 0.0043 ** | 39.27 ± 11.69 | 0.0011 ** |
| Fusion | 44.03 ± 9.23 | 89.42 ± 1.98 | 82.93 ± 3.25 | 44.38 ± 10.04 | |||||
| 7G-B | Paretic | 32.86 ± 9.22 | 4.9629 × 10−5 **** | 89.09 ± 1.66 | 1.3337 × 10−4 **** | 81.69 ± 2.83 | 1.611 × 10−4 **** | 31.69 ± 9.94 | 3.8858 × 10−6 **** |
| Fusion | 38.08 ± 8.57 | 89.97 ± 1.52 | 83.17 ± 2.60 | 38.23 ± 2.60 | |||||
| 6G- NR-B | Paretic | 38.37 ± 9.74 | 0.0171 * | 87.70 ± 1.94 | 0.021 * | 79.49 ± 3.23 | 0.0199 * | 36.64 ± 9.52 | 0.0016 ** |
| Fusion | 41.15 ± 6.23 | 88.24 ± 1.25 | 80.4 ± 2.08 | 40.47 ± 6.43 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anastasiev, A.; Kadone, H.; Marushima, A.; Watanabe, H.; Zaboronok, A.; Watanabe, S.; Matsumura, A.; Suzuki, K.; Matsumaru, Y.; Nishiyama, H.; et al. A Novel Bilateral Data Fusion Approach for EMG-Driven Deep Learning in Post-Stroke Paretic Gesture Recognition. Sensors 2025, 25, 3664. https://doi.org/10.3390/s25123664
Anastasiev A, Kadone H, Marushima A, Watanabe H, Zaboronok A, Watanabe S, Matsumura A, Suzuki K, Matsumaru Y, Nishiyama H, et al. A Novel Bilateral Data Fusion Approach for EMG-Driven Deep Learning in Post-Stroke Paretic Gesture Recognition. Sensors. 2025; 25(12):3664. https://doi.org/10.3390/s25123664
Chicago/Turabian StyleAnastasiev, Alexey, Hideki Kadone, Aiki Marushima, Hiroki Watanabe, Alexander Zaboronok, Shinya Watanabe, Akira Matsumura, Kenji Suzuki, Yuji Matsumaru, Hiroyuki Nishiyama, and et al. 2025. "A Novel Bilateral Data Fusion Approach for EMG-Driven Deep Learning in Post-Stroke Paretic Gesture Recognition" Sensors 25, no. 12: 3664. https://doi.org/10.3390/s25123664
APA StyleAnastasiev, A., Kadone, H., Marushima, A., Watanabe, H., Zaboronok, A., Watanabe, S., Matsumura, A., Suzuki, K., Matsumaru, Y., Nishiyama, H., & Ishikawa, E. (2025). A Novel Bilateral Data Fusion Approach for EMG-Driven Deep Learning in Post-Stroke Paretic Gesture Recognition. Sensors, 25(12), 3664. https://doi.org/10.3390/s25123664