
Cell Membrane Capacitance (Cm) Measured by Bioimpedance Spectroscopy (BIS): A Narrative Review of Its Clinical Relevance and Biomarker Potential
 , , , , and
, , , , and
Abstract
1. Introduction
2. BIS Technology and Methodology
2.1. What Is BIS
2.2. Capacitance and Current
2.3. Impedance and Phase Angle
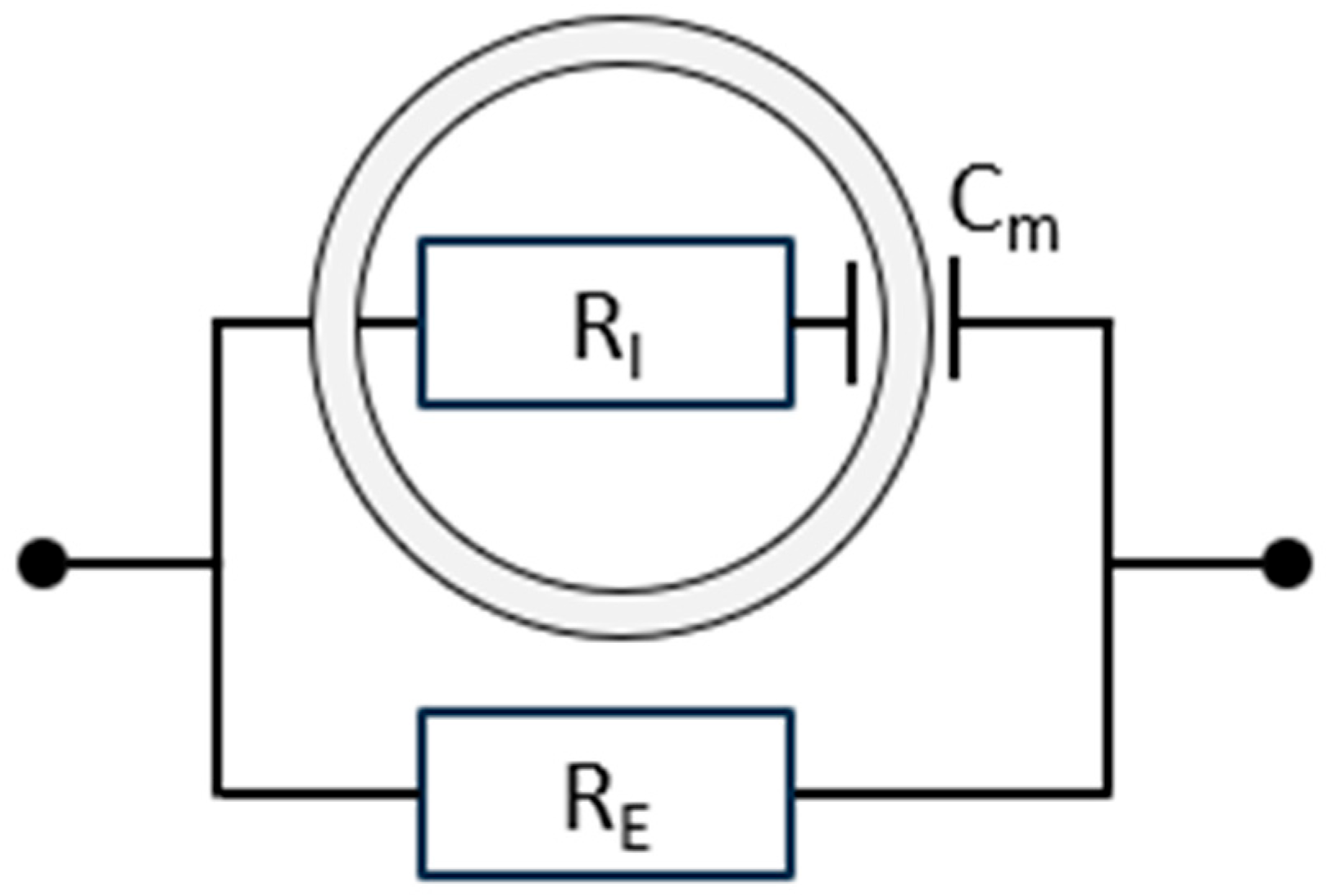
2.4. Electrical Models for Tissue
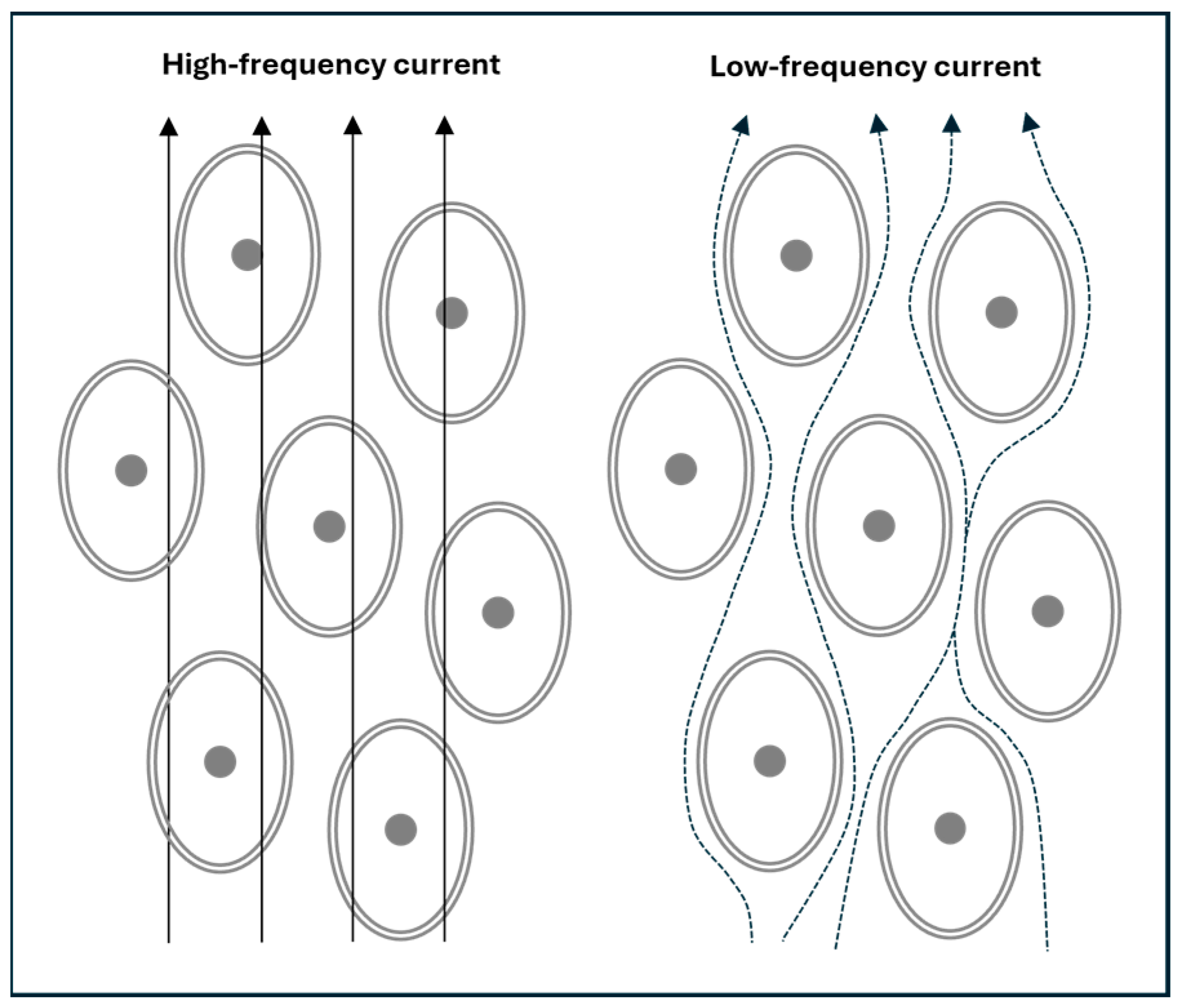
2.5. Frequency Dependence and BIS
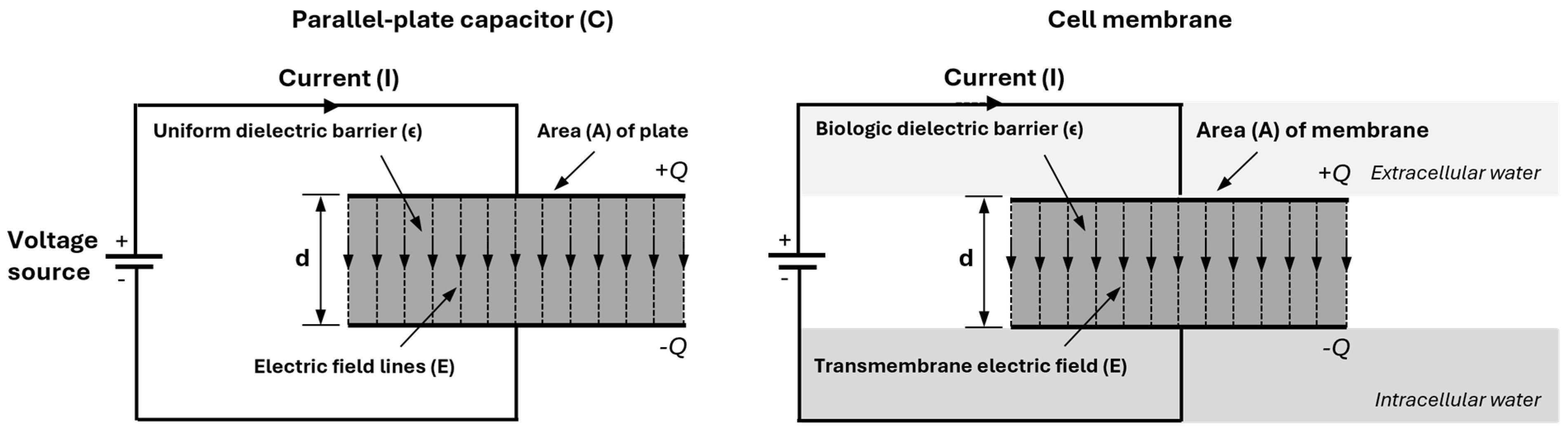
2.6. The Cell Membrane as a Parallel-Plate Capacitor
2.7. The Biophysical Cole Model Used in BIS
- Z(f): The impedance, or total opposition to the flow of AC at a particular frequency (f), is measured in ohms (Ω). Impedance combines both resistive and reactive elements. Through ω (see below), Z(f) varies with frequency, i.e., the impedance is frequency-dependent.
- ω: The angular frequency of the applied alternating current, related to the frequency f by the formula ω = 2πf, which converts frequency to angular frequency in order to standardise formulas for analysing waves and oscillations. As frequency increases, the capacitive effects decrease, affecting the total impedance.
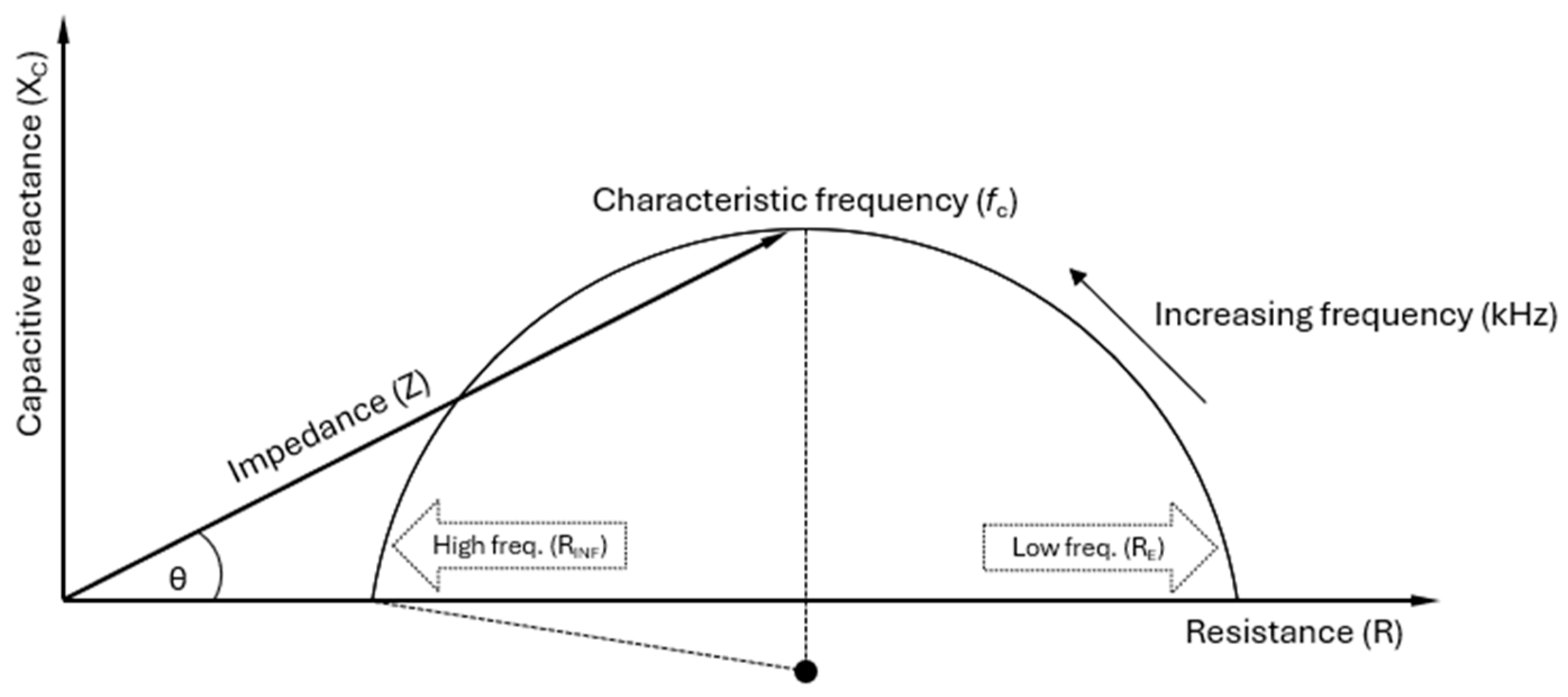
- R0 or RE: The resistance at zero frequency (f = 0), i.e., under direct current (DC) conditions. The cell membranes act as insulators at zero or low frequencies (in practice, typically <5 kHz), allowing current to flow primarily through the ECW. As a result, RE reflects the electrical resistance of the ECW, where the capacitive effect of the cell membrane significantly limits current flow into the intracellular space, leading to higher resistance.
- R∞ or RINF: The resistance at infinite frequency (f = ∞). At very high frequencies, the capacitive reactance of the cell membrane becomes negligible, allowing current to pass through both the ECW and the ICW compartments. This is due to the rapid oscillations that make the cell membranes permeable to the AC. Therefore, RINF reflects the total resistance of the TBW, the combination of the ECW and ICW. Since the current has more pathways to travel, RINF is lower than RE, where the current is restricted to the extracellular space.
- RI: The resistance of the ICW, which is related to R0 = RE and R∞ = RINF by the formula
- j: The imaginary unit in the complex numbers, defined by the property that j2 = −1. It is used in the equation to represent the phase shift introduced by the capacitive element in the system. In the impedance context, j distinguishes between the resistive (real) and reactive (imaginary) components. If the complex impedance Z = R + jX is visualised as a vector in the complex plane, with R on the horizontal axis and X on the vertical axis, the angle between the vector and the horizontal axis represents the phase difference between voltage and current.
- τ (tau): The time constant, representing how quickly tissue responds to an AC signal. It shows how different tissue components, such as cell membranes, accumulate and release electrical energy. The time constant is τ = (RE + RI) ⋅ Cm, where Cm is the cell membrane capacitance. τ indicates the characteristic time over which the system adjusts to changes in the electrical field. Bioimpedance helps determine the speed at which the tissue reacts to the applied alternating current, providing insights into the electrical behaviour of the tissue.
- fc: The characteristic frequency is the point at which the capacitive properties of the cell membrane are most pronounced, meaning the reactance (the imaginary part of the impedance), reaches the peak (or top point) of the semi-circle in the Cole plot. The membrane’s capacitance impedes current flow at this frequency, making it crucial in clinical measurements. The characteristic frequency maximises the membrane’s ability to accumulate and release electrical charge, providing critical insights into membrane functionality in bioimpedance analysis. fc can be mathematically calculated as
- Clinically, fc is essential for understanding how the cell membrane behaves under alternating current. It represents the transition point between low-frequency resistance dominance and high-frequency capacitive dominance, offering insight into the cell membrane’s electrical properties.
- α: A parameter allowing the adjustment of the Cole plot. The value α = 1 corresponds to leaving out α from the formula for Z(f), which places the centre of the semi-circle on the R axis. This is the expected behaviour of the idealised circuit shown in Figure 1. In non-ideal reality, the Cole plot has a centre slightly below the R axis (see Figure 4), reflecting that the body consists of more than one type of tissue and therefore a mixture of relaxation times [8]. This is mathematically modelled with values of α < 1, with α ≈ 0.7 as a typical value.
3. Physiology and Cm
3.1. Factors Influencing Cm and Its Interpretation
3.2. Cm in Disease Monitoring
3.3. Cm and Other BIS Parameters
3.4. Limitations and Future Perspectives
4. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AC | Alternating current |
| BIA | Bioelectrical impedance analysis |
| BIS | Bioimpedance spectroscopy |
| Cm | Cell membrane capacitance |
| CPE | Constant phase element |
| ICW | Intracellular water |
| MF-BIA | Multi-frequency bioelectrical impedance analysis |
| PhA | Phase angle |
| RE | Resistance of the extracellular water |
| RI | Resistance of the intracellular water |
| RINF (R∞) | Resistance at infinite frequency (f = ∞) |
| R0 (RE) | Resistance at zero frequency (f = 0) |
| SF-BIA | Single-frequency bioelectrical impedance analysis |
| TBW | Total body water |
| XC | Capacitive reactance |
References
- Hall, J.E.; Hall, M.E. Guyton and Hall Textbook of Medical Physiology, 14th ed.; Elsevier: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Grimnes, S.; Martinsen, Ø.G. Bioimpedance and Bioelectricity, Basics. In Bioimpedance and Bioelectricity Basics, 2nd ed.; Grimnes, S., Martinsen, Ø.G., Eds.; Academic Press: New York, NY, USA, 2008; pp. 1–6. [Google Scholar]
- Chrysafides, S.M.; Bordes, S.J.; Sharma, S. Physiology, Resting Potential. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2025. Available online: http://www.ncbi.nlm.nih.gov/books/NBK538338/ (accessed on 11 April 2025).
- Kuroshima, T.; Kawaguchi, S.; Okada, M. Current Perspectives of Mitochondria in Sepsis-Induced Cardiomyopathy. Int. J. Mol. Sci. 2024, 25, 4710. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.-C.; Pirlich, M. Bioelectrical impedance analysis—Part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef] [PubMed]
- Lukaski, H.C. Evolution of bioimpedance: A circuitous journey from estimation of physiological function to assessment of body composition and a return to clinical research. Eur. J. Clin. Nutr. 2013, 67 (Suppl. S1), S2–S9. [Google Scholar] [CrossRef] [PubMed]
- Mulasi, U.; Kuchnia, A.J.; Cole, A.J.; Earthman, C.P. Bioimpedance at the Bedside Current Applications, Limitations, and Opportunities. Nutr. Clin. Pract. 2015, 30, 180–193. [Google Scholar] [CrossRef]
- Matthie, J.R. Bioimpedance measurements of human body composition: Critical analysis and outlook. Expert Rev. Med. Devices 2008, 5, 239–261. [Google Scholar] [CrossRef]
- Hill, C.L.; Stephens, G.J. An Introduction to Patch Clamp Recording. In Patch Clamp Electrophysiology: Methods and Protocols; Dallas, M., Bell, D., Eds.; Methods in Molecular Biology; Springer: New York, NY, USA, 2021; pp. 1–19. [Google Scholar]
- Wang, S.; Zhang, J.; Gharbi, O.; Vivier, V.; Gao, M.; Orazem, M.E. Electrochemical impedance spectroscopy. Nat. Rev. Methods Primers 2021, 1, 41. [Google Scholar] [CrossRef]
- Gandhi, C.S.; Olcese, R. The voltage-clamp fluorometry technique. Methods Mol. Biol. 2008, 491, 213–231. [Google Scholar]
- Berecki, G.; Verkerk, A.O.; van Ginneken, A.C.G.; Wilders, R. Dynamic clamp as a tool to study the functional effects of individual membrane currents. Methods Mol. Biol. 2014, 1183, 309–326. [Google Scholar]
- Guan, B.; Chen, X.; Zhang, H. Two-electrode voltage clamp. Methods Mol. Biol. 2013, 998, 79–89. [Google Scholar]
- Ward, L.C. Bioelectrical impedance analysis for body composition assessment: Reflections on accuracy, clinical utility, and standardisation. Eur. J. Clin. Nutr. 2019, 73, 194–199. [Google Scholar] [CrossRef]
- Ward, L.C.; Thompson, B.; Gaitatzis, K.; Koelmeyer, L.A. Comparison of Volume Measurements and Bioimpedance Spectroscopy Using A Stand-on Device for Assessment of Unilateral Breast Cancer-Related Lymphedema. Eur. J. Breast Health 2024, 20, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Sobieszek, G.; Mlak, R.; Powrózek, T.; Mazurek, M.; Skwarek-Dziekanowska, A.; Terlecki, P.; Małecka-Massalska, T. Polymorphism of the ITGAM gene (rs7193943) and bioelectric impedance analysis as potential predictors of cachexia in chronic heart failure. Sci. Rep. 2021, 11, 20145. [Google Scholar] [CrossRef] [PubMed]
- Foster, K.R.; Lukaski, H.C. Whole-body impedance--what does it measure? Am. J. Clin. Nutr. 1996, 64 (Suppl. S3), 388S–396S. [Google Scholar] [CrossRef] [PubMed]
- Golowasch, J.; Thomas, G.; Taylor, A.L.; Patel, A.; Pineda, A.; Khalil, C.; Nadim, F. Membrane capacitance measurements revisited: Dependence of capacitance value on measurement method in nonisopotential neurons. J. Neurophysiol. 2009, 102, 2161–2175. [Google Scholar] [CrossRef]
- Ray, S.; Kassan, A.; Busija, A.R.; Rangamani, P.; Patel, H.H. The plasma membrane as a capacitor for energy and metabolism. Am. J. Physiol. Physiol. 2016, 310, C181–C192. [Google Scholar] [CrossRef]
- Cole, K.S. Permeability and Impermeability of Cell Membranes for Ions. Cold Spring Harb. Symp. Quant. Biol. 1940, 8, 110–122. [Google Scholar] [CrossRef]
- Cole, K.S.; Cole, R.H. Dispersion and Absorption in Dielectrics, I. Alternating Current Characteristics. J. Chem. Phys. 2004, 9, 341–351. [Google Scholar] [CrossRef]
- Naranjo-Hernández, D.; Reina-Tosina, J.; Min, M. Fundamentals, Recent Advances, and Future Challenges in Bioimpedance Devices for Healthcare Applications. J. Sens. 2019, 2019, 9210258. [Google Scholar] [CrossRef]
- Ward, L.C.; Brantlov, S. Bioimpedance basics and phase angle fundamentals. Rev. Endocr. Metab. Disord. 2023, 24, 381–391. [Google Scholar] [CrossRef]
- Grimnes, S.; Martinsen, Ø.G. Chapter 9—Data and Models. In Bioimpedance and Bioelectricity Basics, 3rd ed.; Grimnes, S., Martinsen, Ø.G., Eds.; Academic Press: Oxford, UK, 2015; p. 370. Available online: https://www.sciencedirect.com/science/article/pii/B978012411470800009X (accessed on 7 July 2025).
- Doole, F.T.; Kumarage, T.; Ashkar, R.; Brown, M.F. Cholesterol Stiffening of Lipid Membranes. J. Membr. Biol. 2022, 255, 385–405. [Google Scholar] [CrossRef]
- Małecka-Massalska, T.; Mlak, R.; Smoleń, A.; Brzozowska, A.; Surtel, W.; Morshed, K. Capacitance of Membrane As a Prognostic Indicator of Survival in Head and Neck Cancer. PLoS ONE 2016, 11, e0165809. [Google Scholar] [CrossRef]
- Garr Barry, V.; Peterson, C.M.; Gower, B.A. Membrane Capacitance from a Bioimpedance Approach: Associations with Insulin Resistance in Relatively Healthy Adults. Obesity 2020, 28, 2184–2191. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Hirata, K.; Iida, N.; Kanda, A.; Shoji, M.; Yoshida, T.; Myachi, M.; Akagi, R. Membrane capacitance and characteristic frequency are associated with contractile properties of skeletal muscle. Med. Eng. Phys. 2022, 106, 103832. [Google Scholar] [CrossRef]
- Cornish, B.H.; Lingwood, B.E.; Ward, L.C. Can bioimpedance spectroscopy (BIS) tell us about the form of lymphoedema? In Proceedings of the 13th International Conference on Electrical Bioimpedance and the 8th Conference on Electrical Impedance Tomography, Graz, Austria, 29 August–2 September 2017; Scharfetter, H., Merwa, R., Eds.; IFMBE Proceedings. Springer: Berlin/Heidelberg, Germany, 2007; pp. 795–798. [Google Scholar]
- Yashiro, M.; Kotera, H. Association of bioimpedance-derived 50-kHz phase angle as marker of body composition with electrical parameters regarding the Cole-Cole model. Ther. Apher. Dial. 2021, 25, 166–178. [Google Scholar] [CrossRef] [PubMed]
- Sobieszek, G.; Powrózek, T.; Mazurek, M.; Skwarek-Dziekanowska, A.; Małecka-Massalska, T. Electrical and Hormonal Biomarkers in Cachectic Elderly Women with Chronic Heart Failure. J. Clin. Med. 2020, 9, 1021. [Google Scholar] [CrossRef] [PubMed]
- Sobieszek, G.; Mlak, R.; Skwarek-Dziekanowska, A.; Jurzak-Myśliwy, A.; Homa-Mlak, I.; Małecka-Massalska, T. Electrical Changes in Polish Patients with Chronic Heart Failure: Preliminary Observations. Medicina 2019, 55, 484. [Google Scholar] [CrossRef]
- Brantlov, S.; Jødal, L.; Frydensbjerg Andersen, R.; Lange, A.; Rittig, S.; Ward, L.C. Bioimpedance Resistance Indices and Cell Membrane Capacitance Used to Assess Disease Status and Cell Membrane Integrity in Children with Nephrotic Syndrome. Sci. World J. 2019, 2019, 4274856. [Google Scholar] [CrossRef]
- Popiołek, J.; Teter, M.; Kozak, G.; Powrózek, T.; Mlak, R.; Karakuła-Juchnowicz, H.; Małecka-Massalska, T. Anthropometrical and Bioelectrical Impedance Analysis Parameters in Anorexia Nervosa Patients’ Nutritional Status Assessment. Medicina 2019, 55, 671. [Google Scholar] [CrossRef]
- Cox-Reijven, P.L.M.; van Kreel, B.; Soeters, P.B. Bioelectrical impedance measurements in patients with gastrointestinal disease: Validation of the spectrum approach and a comparison of different methods for screening for nutritional depletion. Am. J. Clin. Nutr. 2003, 78, 1111–1119. [Google Scholar] [CrossRef]
- Norman, K.; Stobäus, N.; Pirlich, M.; Bosy-Westphal, A. Bioelectrical phase angle and impedance vector analysis–clinical relevance and applicability of impedance parameters. Clin. Nutr. 2012, 31, 854–861. [Google Scholar] [CrossRef]
- Martins, P.C.; Junior, C.A.S.A.; Silva, A.M.; Silva, D.A.S. Phase angle and body composition: A scoping review. Clin. Nutr. ESPEN 2023, 56, 237–250. [Google Scholar] [CrossRef] [PubMed]
- Brantlov, S.; Jødal, L.; Lange, A.; Rittig, S.; Ward, L.C. Standardisation of bioelectrical impedance analysis for the estimation of body composition in healthy paediatric populations: A systematic review. J. Med. Eng. Technol. 2017, 41, 460–479. [Google Scholar] [CrossRef] [PubMed]
- Brantlov, S.; Ward, L.C.; Jødal, L.; Rittig, S.; Lange, A. Critical factors and their impact on bioelectrical impedance analysis in children: A review. J. Med. Eng. Technol. 2017, 41, 22–35. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Manuel Gómez, J.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.-C.; Pirlich, M.; et al. Bioelectrical impedance analysis-part II: Utilization in clinical practice. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef]
- Mehra, A.; Starkoff, B.E.; Nickerson, B.S. The evolution of bioimpedance analysis: From traditional methods to wearable technology. Nutrition 2025, 129, 112601. [Google Scholar] [CrossRef]
- Hou, J.; Nesaragi, N.; Tronstad, C. Electrical bioimpedance in the era of artificial intelligence. J. Electr. Bioimpedance 2024, 15, 1–3. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Technique | Invasiveness | Resolution | Clinical Use | Limitations |
|---|---|---|---|---|
| Bioimpedance spectroscopy (BIS) | Non-invasive | Whole body/ segmental | Routine use | Requires calibration, affected by hydration, temperature, and body position |
| Patch-clamp | Invasive | Single-cell level | Research (electrophysiology) | Requires isolated cells and skilled operators, unsuitable for in vivo use |
| Electrical impedance spectroscopy (EIS) | Semi-invasive | Tissue-specific | Research/ experimental | Limited clinical use; sensitive to electrode setup and boundary conditions |
| Voltage clamp fluorometry | Invasive | Single-cell level | Research (electrophysiology) | Combines electrical and optical methods; used only in advanced research |
| Dynamic clamp | Invasive | Single-cell level | Research (electrophysiology) | Technically complex; not applicable to clinical settings |
| Two-electrode voltage clamp | Invasive | Single-cell level | Research (electrophysiology) | Useful for large cells, such as oocytes, but not for routine or clinical use |
| Author | Disease | Cm |
|---|---|---|
| Małecka-Massalska et al. [26] | Head and neck cancer | Cm was significantly higher in well-nourished patients compared to malnourished ones. |
| Barry et al. [27] | Healthy premenopausal women | Cm showed considerable inter-individual variability but high intra-individual precision. |
| Yamada et al. [28] | Healthy individuals (skeletal muscle function) | Cm positively correlated with muscle strength and contractile properties; higher Cm was associated with greater torque production. |
| Cornish et al. [29] | Lymphedema | Cm was higher in affected limbs compared to controls; values varied by limb and dominance. |
| Yashiro & Kotera, 2021 [30] | Haemodialysis | Cm was lower after dialysis. |
| Sobieszek et al. [31] | Chronic heart failure with cachexia | Cm was lower in advanced disease stages and negatively correlated with inflammatory markers. |
| Sobieszek et al. [32] | Chronic heart failure | Cm was lower in advanced stages in men (significant) and in women (non-significant); negatively correlated with C-reactive protein in men. |
| Brantlov et al. [33] | Nephrotic syndrome | Cm was lowest during active disease, higher in remission, and intermediate in healthy controls. |
| Popiołek et al. [34] | Anorexia nervosa | Higher Cm was found in younger patients, with improvement during refeeding. |
| Cox-Reijven et al. [35] | Gastrointestinal disease | Cm decreased with increasing severity of weight loss. |
| Parameter | Formula | Definition | Function and Use | Features | Limitations |
|---|---|---|---|---|---|
| Cm (nF) | Cell membrane capacitance. | Reflects membrane health, structural integrity, function, and total membrane area; useful for detecting changes in membrane properties | Makes impedance measurement frequency-dependent | Measurement requires BIS device (cannot be measured with SF-BIA or MF-BIA) | |
| PhA (degrees) | Phase shift between voltage and current. | Indicates cell mass, hydration, and membrane health; helpful for assessing overall tissue and fluid status | Most often reported at 50 kHz fixed frequency; it combines resistive and reactive impedance | Single-frequency (50 kHz) measurement gives limited information | |
| XC (Ω) | Reactance is imaginary part of complex impedance Z | Indicates capacitive properties of cell membrane | Most often reported for fixed frequency of 50 kHz | Single-frequency (50 kHz) measurement gives limited information |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brantlov, S.; Ward, L.C.; Isidor, S.; Hvas, C.L.; Rud, C.L.; Jødal, L. Cell Membrane Capacitance (Cm) Measured by Bioimpedance Spectroscopy (BIS): A Narrative Review of Its Clinical Relevance and Biomarker Potential. Sensors 2025, 25, 4362. https://doi.org/10.3390/s25144362
Brantlov S, Ward LC, Isidor S, Hvas CL, Rud CL, Jødal L. Cell Membrane Capacitance (Cm) Measured by Bioimpedance Spectroscopy (BIS): A Narrative Review of Its Clinical Relevance and Biomarker Potential. Sensors. 2025; 25(14):4362. https://doi.org/10.3390/s25144362
Chicago/Turabian StyleBrantlov, Steven, Leigh C. Ward, Søren Isidor, Christian Lodberg Hvas, Charlotte Lock Rud, and Lars Jødal. 2025. "Cell Membrane Capacitance (Cm) Measured by Bioimpedance Spectroscopy (BIS): A Narrative Review of Its Clinical Relevance and Biomarker Potential" Sensors 25, no. 14: 4362. https://doi.org/10.3390/s25144362
APA StyleBrantlov, S., Ward, L. C., Isidor, S., Hvas, C. L., Rud, C. L., & Jødal, L. (2025). Cell Membrane Capacitance (Cm) Measured by Bioimpedance Spectroscopy (BIS): A Narrative Review of Its Clinical Relevance and Biomarker Potential. Sensors, 25(14), 4362. https://doi.org/10.3390/s25144362