
Retention Effects of Long-Term Balance Training with Vibrotactile Sensory Augmentation in Healthy Older Adults

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
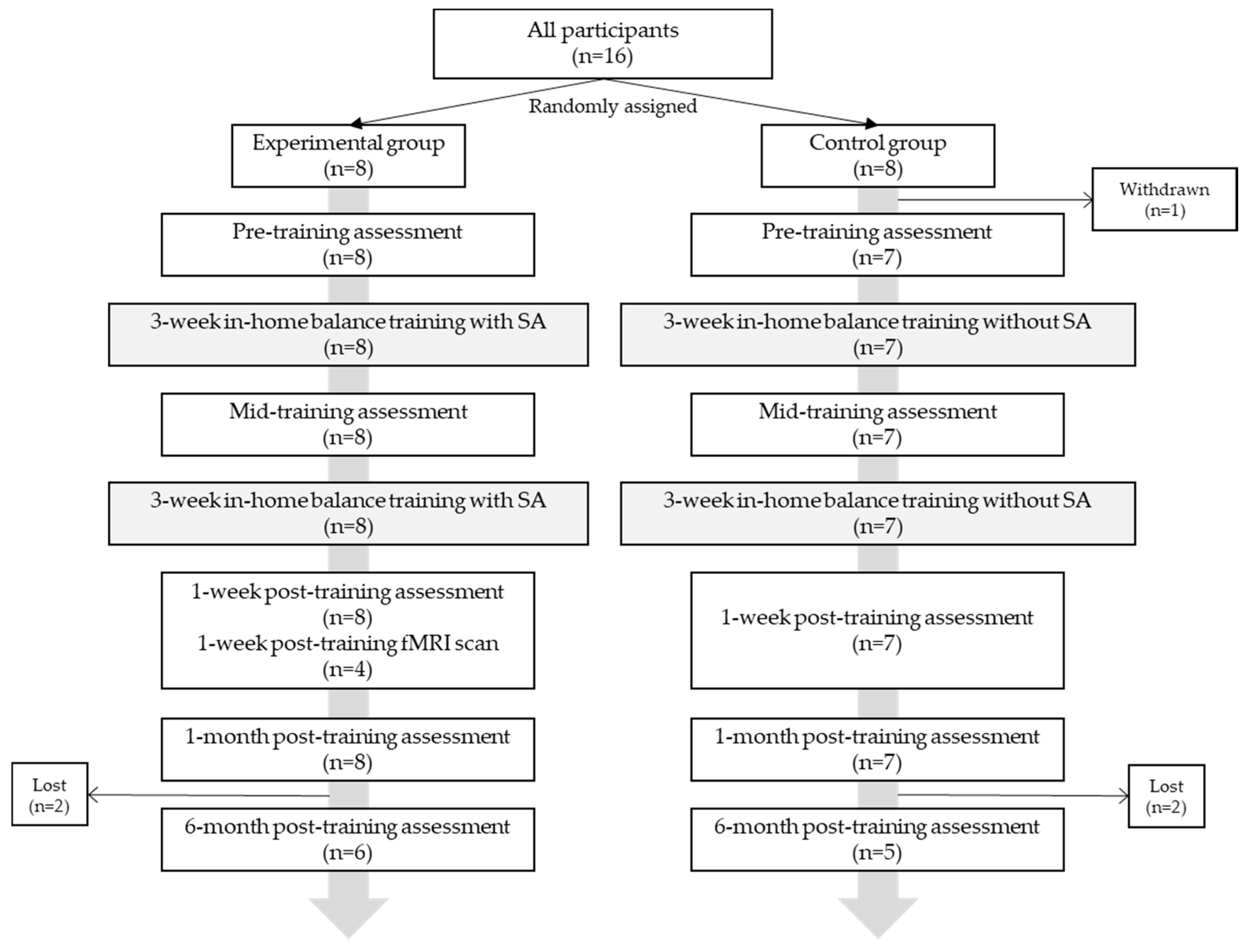
2.1. Participants
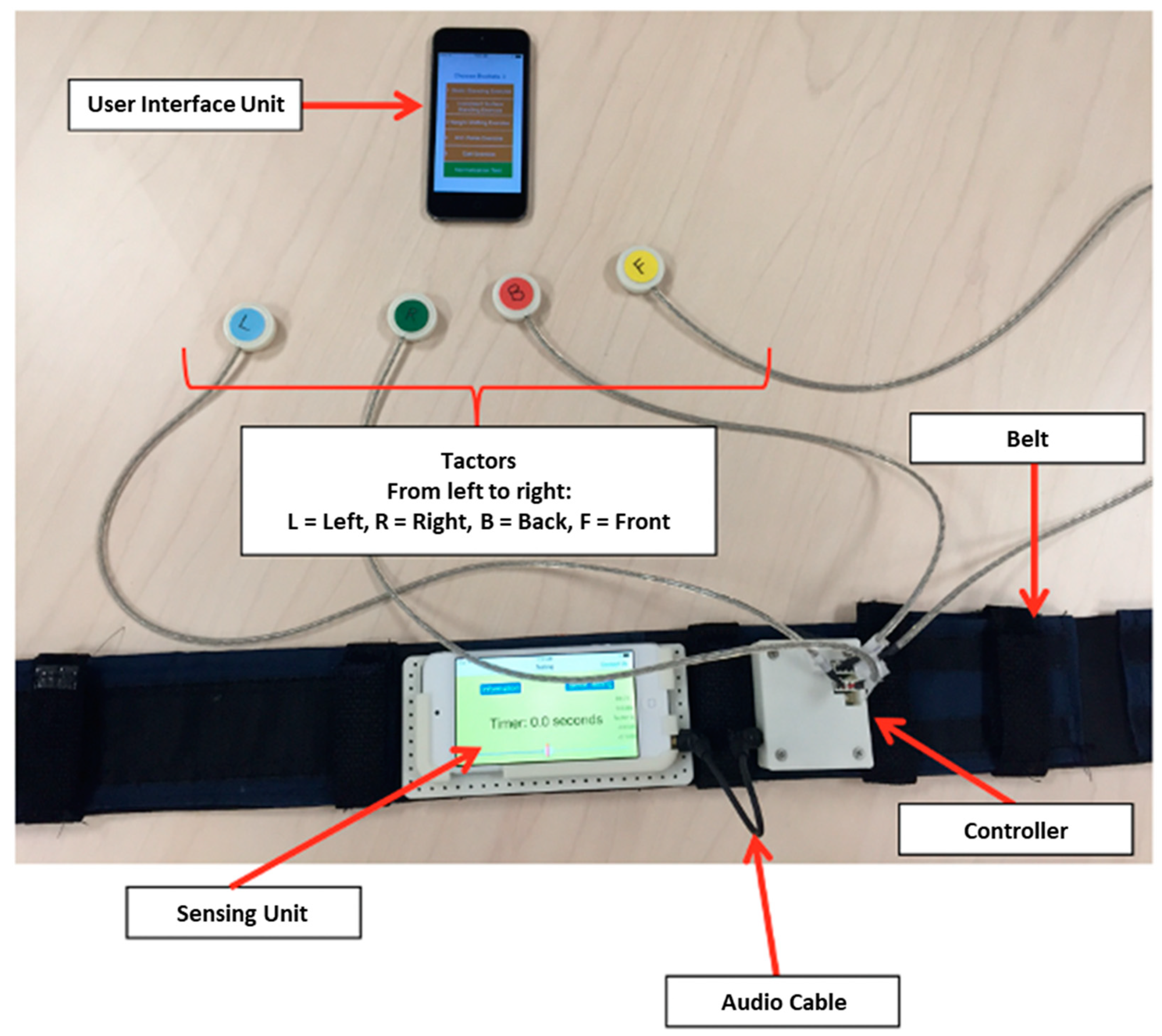
2.2. Protocol
2.3. Analysis
3. Results
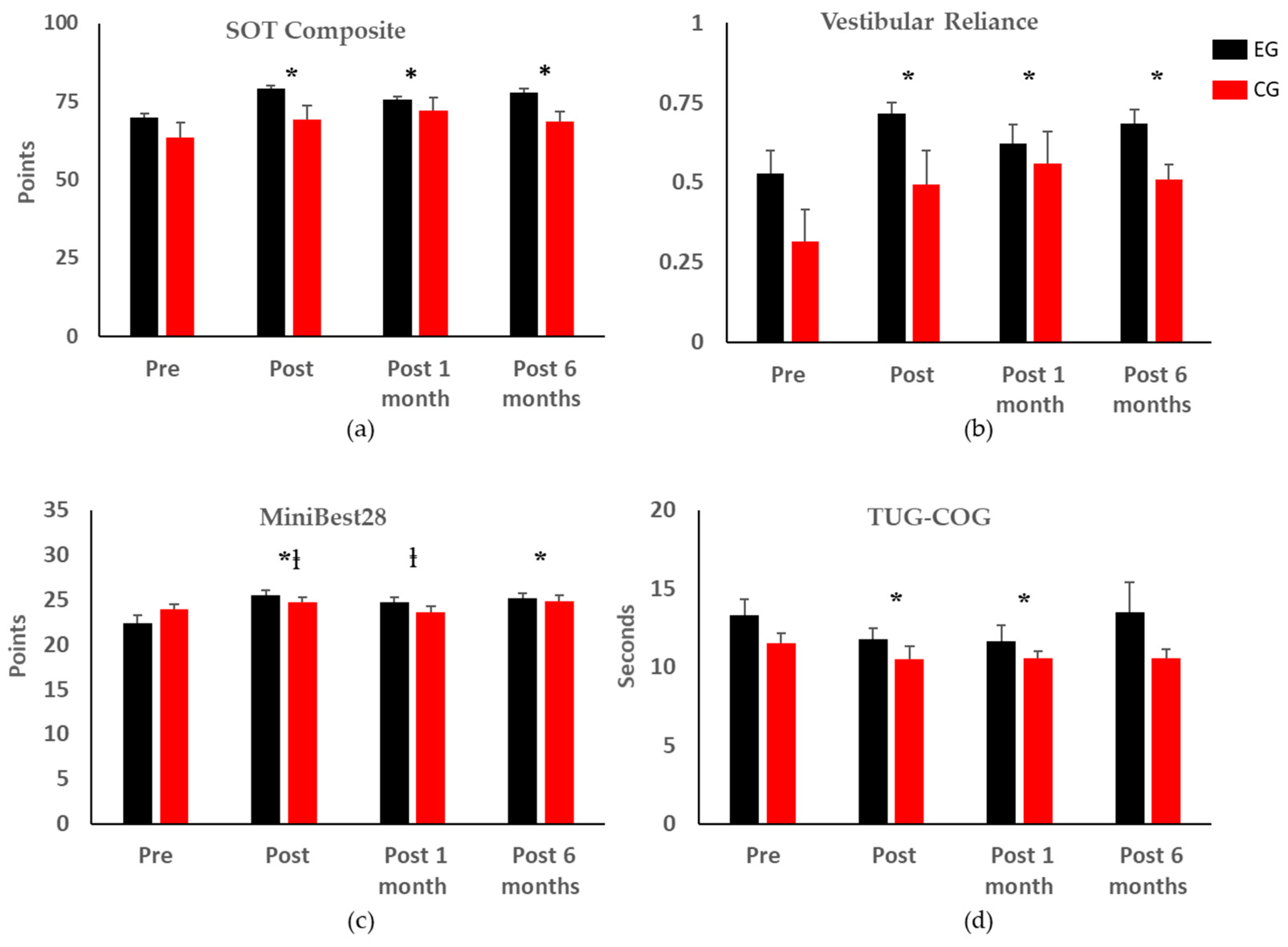
3.1. Clinical Balance Testing Results
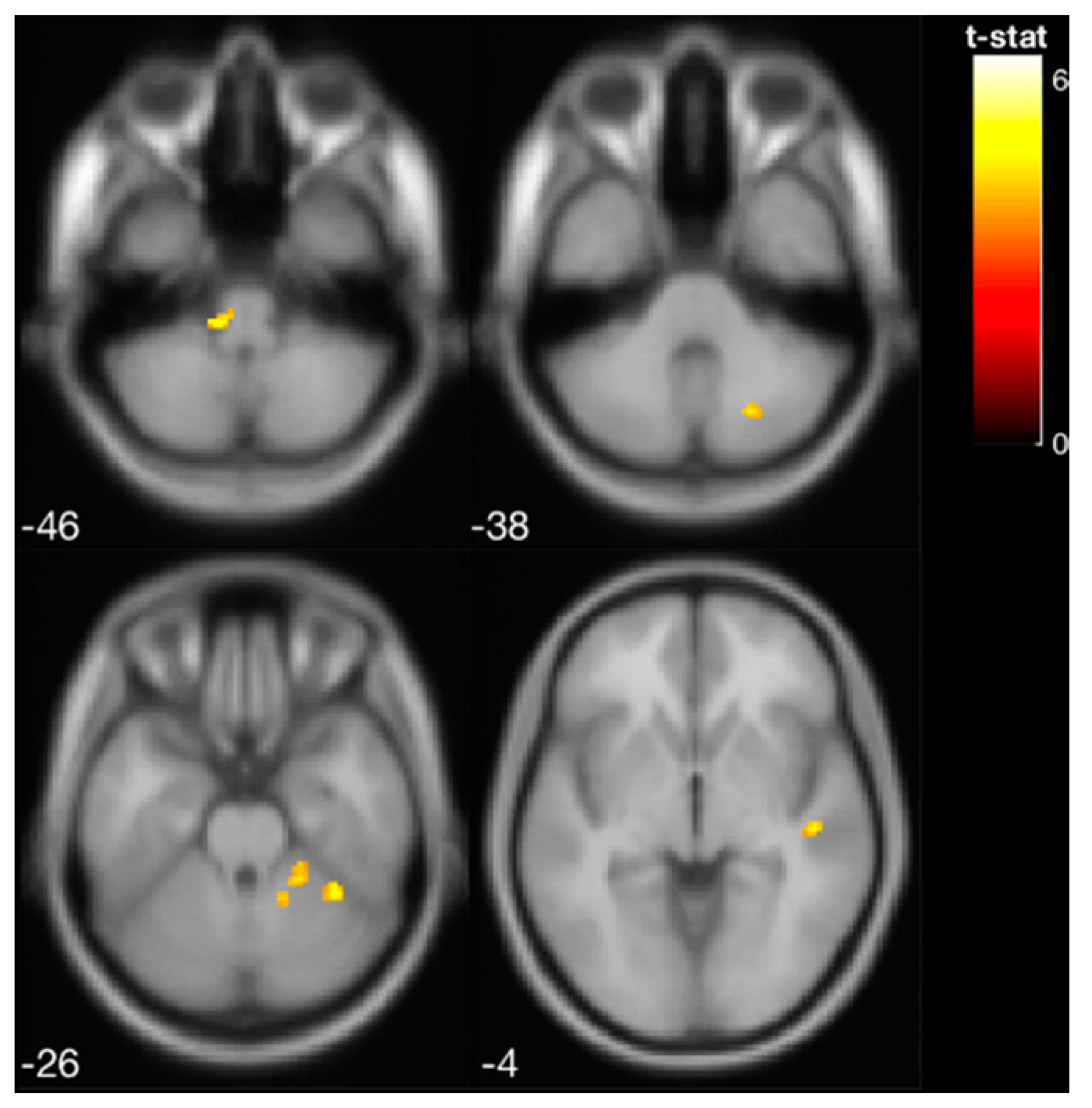
3.2. fMRI Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 16 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Time | |||||||||||||||||
| Gender | M | F | F | F | M | M | M | F | F | F | F | M | F | F | F | ||
| Age | 83 | 83 | 70 | 72 | 70 | 80 | 73 | 70 | 82 | 78 | 74 | 74 | 74 | 73 | 75 | ||
| Group | CG | EG | EG | CG | CG | EG | CG | EG | EG | CG | CG | EG | EG | EG | CG | ||
| SOT | Pre | 71 | 63 | 78 | 49 | 76 | 68 | 60 | 83 | 74 | 83 | 68 | 58 | 50 | 74 | 43 | |
| Post 1wk | 81 | 83 | 76 | 46 | 73 | 86 | 65 | 85 | 79 | 85 | 76 | 60 | 79 | 65 | 67 | ||
| Post 1mo | 83 | 76 | 78 | 49 | 77 | 78 | 65 | 85 | 77 | 85 | 77 | 65 | 73 | 62 | 75 | ||
| Post 6mo | 80 | 77 | - | 56 | 75 | 76 | 69 | 85 | 76 | - | 71 | 61 | 76 | - | - | ||
| MiniBESTest28 | Pre | 21 | 22 | 20 | 25 | 26 | 23 | 24 | 24 | 25 | 23 | 24 | 24 | 19 | 24 | 25 | |
| Post 1wk | 25 | 25 | 27 | 24 | 22 | 23 | 25 | 27 | 26 | 25 | 24 | 27 | 26 | 25 | 26 | ||
| Post 1mo | 21 | 26 | 24 | 23 | 22 | 23 | 27 | 26 | 27 | 22 | 24 | 25 | 24 | 23 | 25 | ||
| Post 6mo | 26 | 24 | - | 23 | 25 | 24 | 27 | 27 | 25 | - | 22 | 26 | 26 | - | - | ||
| MiniBESTest32 | Pre | 24 | 26 | 23 | 28 | 30 | 25 | 26 | 27 | 28 | 26 | 27 | 28 | 21 | 28 | 29 | |
| Post 1wk | 27 | 29 | 31 | 27 | 24 | 26 | 28 | 31 | 29 | 27 | 26 | 31 | 30 | 29 | 30 | ||
| Post 1mo | 25 | 29 | 27 | 26 | 25 | 25 | 31 | 30 | 30 | 26 | 26 | 29 | 27 | 28 | 29 | ||
| Post 6mo | 30 | 26 | - | 27 | 29 | 26 | 30 | 30 | 28 | - | 24 | 30 | 30 | - | - | ||
| ABC | Pre | 95 | 92 | 94 | 95 | 95 | 94 | 98 | 86 | 93 | 89 | 92 | 94 | 87 | 98 | 96 | |
| Post 1wk | 92 | 82 | 89 | - | 93 | 87 | 99 | 98 | 97 | 91 | 94 | 83 | 95 | 98 | 93 | ||
| Post 1mo | 89 | 88 | 88 | - | 92 | 81 | 99 | 99 | 96 | 91 | 96 | 93 | 96 | 98 | 96 | ||
| Post 6mo | 93 | 91 | - | 88 | 93 | 86 | 99 | 99 | 98 | - | 91 | 88 | 94 | - | - | ||
| TUG | Pre | 9.9 | 8.4 | 9.3 | 9.3 | 9.3 | 13 | 8.6 | 9.8 | 13.6 | 10.5 | 12.4 | 10.6 | 10.7 | 10.1 | 10.5 | |
| Post 1wk | 9.8 | 9.9 | 10.4 | 8.8 | 9.5 | 12.8 | 9.7 | 8.9 | 11.4 | 12 | 9.3 | 10.3 | 9.6 | 9.7 | 13.2 | ||
| Post 1mo | 9.3 | 10.3 | 9.1 | 8.2 | 9.9 | 12.2 | 8.4 | 7.2 | 13.5 | 10.5 | 10.1 | 13.4 | 8.5 | 8.4 | 13.7 | ||
| Post 6mo | 9.8 | 9.3 | - | 10.1 | 10.2 | 15.5 | 8.7 | 8.1 | 9.6 | - | 11.2 | 10 | 9.1 | - | - | ||
| TUG-COG | Pre | 12.2 | 10 | 11.6 | 8.3 | 8.8 | 16.9 | 8.7 | 10.8 | 14.2 | 12.4 | 14.8 | 14.2 | 16.4 | 13.5 | 13 | |
| Post 1wk | 7.8 | 10.3 | 11.2 | 8.4 | 11.4 | 15 | 8.9 | 9.1 | 12.6 | 11.6 | 10.3 | 11.8 | 12.7 | 11.6 | 13.8 | ||
| Post 1mo | 9.1 | 9.4 | 13.1 | 9.1 | 12 | 15.2 | 10.1 | 7.7 | 13.4 | 11 | 12.5 | 8.7 | 11.9 | 10.4 | 12.2 | ||
| Post 6mo | 8.9 | 10.5 | - | 10.5 | 12 | 19.9 | 9.2 | 8.1 | 11 | - | 11.8 | 10.8 | 18.0 | - | - | ||
| 5TSTS | Pre | 11 | 12 | 10.1 | 7.4 | 9.7 | 14.5 | 8.8 | 12.2 | 17.8 | 13.7 | 17.7 | 8.9 | 14.6 | 9.7 | 16.9 | |
| Post 1wk | 14.6 | 11 | 8.7 | 11 | 11.4 | 12.3 | 8.3 | 6.6 | 15 | 9.9 | 9.5 | 14.7 | 10.6 | 9.4 | 12.9 | ||
| Post 1mo | 10.4 | 11.7 | 9.1 | 7.2 | 10 | 13.5 | 9.3 | 7.1 | 13.3 | 9.3 | 8.9 | 12.8 | 9.6 | 10.7 | 14.6 | ||
| Post 6mo | 14.4 | 10.3 | - | 8.4 | 10.3 | 14.4 | 7.1 | 6.5 | 16.8 | - | 11.1 | 12.7 | 10.6 | - | - | ||
| FSST | Pre | 13 | 10.4 | 10.2 | 11 | 8.3 | 10.7 | 8.5 | 6.5 | 13 | 10.7 | 11.7 | 10.9 | 8.3 | 11.3 | 10.8 | |
| Post 1wk | 14.4 | 10.2 | 10.2 | 9.9 | 8.9 | 11 | 8.1 | 6.2 | 11.8 | 9.8 | 9.7 | 12.5 | 7.8 | 11.8 | 12.3 | ||
| Post 1mo | 12.7 | 10.6 | 10.1 | 10.6 | 9.5 | 10.7 | 9 | 5.6 | 12.6 | 8.5 | 9.2 | 11.2 | 8.2 | 8.4 | 10.8 | ||
| Post 6mo | 11.2 | 10.3 | - | 12.1 | 10.1 | 11.7 | 9.1 | 5.8 | 11.5 | - | 10.2 | 10 | 7.8 | - | - | ||
| FRT | Pre | 9.2 | 10.7 | 15.8 | 14.2 | 12.8 | 9.8 | 14.8 | 13.7 | 15.7 | 11.8 | 12.7 | 12 | 13.8 | 15.5 | 12 | |
| Post 1wk | 12 | 11.3 | 13.5 | 14.3 | 14.8 | 10.7 | 13.5 | 10.3 | 14.8 | 13.3 | 14.7 | 7.8 | 13.5 | 13.7 | 12 | ||
| Post 1mo | 11.8 | 9.3 | 13.3 | 13.5 | 10.8 | 14.5 | 13.3 | 13 | 12.8 | 12.5 | 10 | 10.7 | 16 | 15.5 | 12.2 | ||
| Post 6mo | 10.2 | 13.2 | - | 11.8 | 12 | 10.7 | 11.7 | 12.3 | 12.2 | - | 11.2 | 7.7 | 12.8 | - | - | ||
| fMRI Scan | Yes | Yes | Yes | Yes | Yes | ||||||||||||
References
- Florence, C.S.; Bergen, G.; Atherly, A.; Burns, E.; Stevens, J.; Drake, C. Medical costs of fatal and nonfatal falls in older adults. J. Am. Geriatr. Soc. 2018, 66, 693–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.M.; Lamb, S.E. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2012, 2012, CD007146. [Google Scholar]
- Moncada, L.V.V.; Mire, L.G. Preventing Falls in Older Persons. Am. Fam. Physician 2017, 96, 240–247. [Google Scholar] [PubMed]
- Panel on Prevention of Falls in Older Persons, American Geriatrics Society and British Geriatrics Society. Summary of the updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J. Am. Geriatr. Soc. 2011, 59, 148–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youssef, E.F.; Shanb, A.A. Supervised Versus Home Exercise Training Programs on Functional Balance in Older Subjects. Malays. J. Med. Sci. 2016, 23, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Kao, C.L.; Chen, L.K.; Chern, C.M.; Hsu, L.C.; Chen, C.C.; Hwang, S.J. Rehabilitation outcome in home-based versus supervised exercise programs for chronically dizzy patients. Arch. Gerontol. Geriatr. 2010, 51, 264–267. [Google Scholar] [CrossRef]
- Laufer, Y.; Dar, G.; Kodesh, E. Does a Wii-based exercise program enhance balance control of independently functioning older adults? A systematic review. Clin. Interv. Aging 2014, 9, 1803–1813. [Google Scholar] [CrossRef] [Green Version]
- de Vries, A.W.; Faber, G.; Jonkers, I.; Van Dieen, J.H.; Verschueren, S.M.P. Virtual reality balance training for elderly: Similar skiing games elicit different challenges in balance training. Gait Posture 2018, 59, 111–116. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.B.; Horslen, B.C.; Davis, J.R.; Allum, J.H.J.; Carpenter, M.G. Benefits of multi-session balance and gait training with multi-modal biofeedback in healthy older adults. Gait Posture 2016, 47, 10–17. [Google Scholar] [CrossRef]
- Schwenk, M.; Grewal, G.S.; Holloway, D.; Muchna, A.; Garland, L.; Najafi, B. Interactive Sensor-Based Balance Training in Older Cancer Patients with Chemotherapy-Induced Peripheral Neuropathy: A Randomized Controlled Trial. Gerontology 2016, 62, 553–563. [Google Scholar] [CrossRef]
- Sienko, K.H.; Balkwill, M.D.; Oddsson, L.I.E.; Wall, C. Effects of multi-directional vibrotactile feedback on vestibular-deficient postural performance during continuous multi-directional support surface perturbations. J. Vestib. Res. 2008, 18, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Basta, D.; Rossi-Izquierdo, M.; Soto-Varela, A.; Greters, M.E.; Bittar, R.S.; Steinhagen-Thiessen, E.; Eckardt, R.; Harada, T.; Goto, F.; Ogawa, K.; et al. Efficacy of a vibrotactile neurofeedback training in stance and gait conditions for the treatment of balance deficits: A double-blind, placebo-controlled multicenter study. Otol. Neurotol. 2011, 32, 1492–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brugnera, C.; Bittar, R.S.M.; Greters, M.E.; Basta, D. Effects of vibrotactile vestibular substitution on vestibular rehabilitation—preliminary study. Braz. J. Otorhinolaryngol. 2015, 81, 616–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sienko, K.H.; Seidler, R.D.; Carender, W.J.; Goodworth, A.D.; Whitney, S.L.; Peterka, R.J. Potential Mechanisms of Sensory Augmentation Systems on Human Balance Control. Front. Neurol. 2018, 9, 944. [Google Scholar] [CrossRef]
- Kingma, H.; Felipe, L.; Cecile, M.; Peter, G.; Nils, G.; Angelica, G.; Fornos, P.; Demkin, V.; Berg, R. Van De Vibrotactile feedback improves balance and mobility in patients with severe bilateral vestibular loss. J. Neurol. 2019, 266, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Shull, P.B.; Jirattigalachote, W.; Hunt, M.A.; Cutkosky, M.R.; Delp, S.L. Quantified self and human movement: A review on the clinical impact of wearable sensing and feedback for gait analysis and intervention. Gait Posture 2014, 40, 11–19. [Google Scholar] [CrossRef]
- Yen, C.; Lin, K.; Hu, M.; Wu, R.; Lu, T.; Lin, C. Effects of Virtual Reality—Augmented Balance Training on Sensory Organization and Attentional Demand for Postural Control in People With Parkinson Disease: A Randomized Controlled Trial. Phys. Ther. 2011, 91, 862–874. [Google Scholar] [CrossRef] [Green Version]
- Rossi-Izquierdo, M.; Ernst, A.; Soto-Varela, A.; Santos-Pérez, S.; Faraldo-García, A.; Sesar-Ignacio, A.; Basta, D. Vibrotactile neurofeedback balance training in patients with Parkinson’s disease: Reducing the number of falls. Gait Posture 2013, 37, 195–200. [Google Scholar] [CrossRef]
- American College of Sports Medicin. ACSM’s Health-Related Physical Fitness Assessment Manual; Lippincott & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Bao, T.; Klatt, B.N.; Carender, W.J.; Kinnaird, C.; Alsubaie, S. Effects of long-term vestibular rehabilitation therapy with vibrotactile sensory augmentation for people with unilateral vestibular disorders—A randomized preliminary study. J. Vestib. Res. 2019, 29, 323–334. [Google Scholar] [CrossRef] [Green Version]
- Bao, T.; Carender, W.J.; Kinnaird, C.; Barone, V.J.; Peethambaran, G.; Whitney, S.L.; Kabeto, M.; Seidler, R.D.; Sienko, K.H. Effects of long-term balance training with vibrotactile sensory augmentation among community-dwelling healthy older adults. J. Neuroeng. Rehabil. 2018, 15, 5. [Google Scholar] [CrossRef] [Green Version]
- Sienko, K.H.; Whitney, S.L.; Carender, W.J.; Wall III, C. The role of sensory augmentation for people with vestibular deficits: Real-time balance aid and/or rehabilitation device? J. Vestib. Res. 2017, 27, 63–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schumann, F.; Keyser, J.; Goeke, C.; Ko, S.U.; Krause, C.; Wache, S.; Lytochkin, A.; Ebert, M.; Brunsch, V.; Wahn, B.; et al. Learning New Sensorimotor Contingencies: Effects of Long-Term Use of Sensory Augmentation on the Brain and Conscious Perception. PLoS ONE 2016, 11, e0166647. [Google Scholar]
- Clendaniel, R.A. Outcome measures for assessment of treatment of the dizzy and balance disorder patient. Otolaryngol. Clin. N. Am. 2000, 33, 519–533. [Google Scholar] [CrossRef]
- Rehabilitation Measures Database. Available online: https://www.sralab.org/statistical-terms-use (accessed on 9 October 2017).
- Bao, T.; Kinnaird, C.; Carender, W.J.; Sienko, K.H. Effects of sensory augmentation activation thresholds on balance performance in people with vestibular disorders. In Proceedings of the ISPGR—The International Society of Posture and Gait Research World Congress, Edinburgh, UK, 30 June–4 July 2019. [Google Scholar]
- Lee, B.-C.; Kim, J.; Chen, S.; Sienko, K.H. Cell phone based balance trainer. J. Neuroeng. Rehabil. 2012, 9, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klatt, B.N.; Carender, W.J.; Lin, C.C.; Alsubaie, S.F.; Kinnaird, C.R.; Sienko, K.H.; Whitney, S.L. A Conceptual Framework for the Progression of Balance Exercises in Persons with Balance and Vestibular Disorders. Phys. Med. Rehabil. Int. 2015, 2, 1044. [Google Scholar]
- Noohi, F.; Kinnaird, C.; DeDios, Y.; Kofman, I.S.; Wood, S.; Bloomberg, J.; Mulavara, A.; Seidler, R. Functional Brain Activation in Response to a Clinical Vestibular Test Correlates with Balance. Front. Syst. Neurosci. 2017, 11, 11. [Google Scholar] [CrossRef] [Green Version]
- Hupfeld, K.E.; McGregor, H.R.; Koppelmans, V.; Beltran, N.E.; Kofman, I.S.; De Dios, Y.E.; Riascos, R.F.; Reuter-Lorenz, P.A.; Wood, S.J.; Bloomberg, J.J.; et al. Brain and Behavioral Evidence for Reweighting of Vestibular Inputs with Long-Duration Spaceflight. Cereb. Cortex 2022, 32, 755–769. [Google Scholar] [CrossRef]
- Friston, K.J.; Holmes, A.P.; Worsley, K.J.; Poline, J.-P.; Frith, C.D.; Frackowiak, R.S.J. Statistical parametric maps in functional imaging: A general linear approach. Hum. Brain Mapp. 1994, 2, 189–210. [Google Scholar] [CrossRef]
- Glover, G.H.; Li, T.; Ress, D. Image-Based Method for Retrospective Correction of Physiological Motion Effects in fMRI: RETROICOR. Magn. Reson. Med. 2000, 44, 162–167. [Google Scholar] [CrossRef]
- Friston, K.J.; Ashburner, J.; Frith, C.D.; Poline, J.; Heather, J.D.; Frackowiak, R.S.J. Spatial Registration and Normalization of Images. Hum. Brain Mapp. 1995, 3, 165–189. [Google Scholar] [CrossRef]
- Diedrichsen, J.; Balsters, J.H.; Flavell, J.; Cussans, E.; Ramnani, N. A probabilistic MR atlas of the human cerebellum. Neuroimage 2009, 46, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Diedrichsen, J.; Maderwald, S.; Küper, M.; Thürling, M.; Rabe, K.; Gizewski, E.R. NeuroImage Imaging the deep cerebellar nuclei: A probabilistic atlas and normalization procedure. Neuroimage 2011, 54, 1786–1794. [Google Scholar] [CrossRef]
- Diedrichsen, J.; Zotow, E. Surface-Based Display of Volume-Averaged Cerebellar Imaging Data. PLoS ONE 2015, 10, e0133402. [Google Scholar] [CrossRef]
- Tzourio-Mazoyer, N.; Landeau, B.; Papathanassiou, D.; Crivello, F.; Etard, O.; Delcroix, N.; Mazoyer, B.; Joliot, M. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 2002, 15, 273–289. [Google Scholar] [CrossRef] [PubMed]
- Kirsch, V.; Keeser, D.; Hergenroeder, T.; Erat, O.; Brandt, T.; Dieterich, M. Structural and functional connectivity mapping of the vestibular circuitry from human brainstem to cortex. Brain Struct. Funct. 2016, 221, 1291–1308. [Google Scholar] [CrossRef] [PubMed]
- Wrisley, D.M.; Stephens, M.J.; Mosley, S.; Wojnowski, A.; Duffy, J.; Burkard, R. Learning Effects of Repetitive Administrations of the Sensory Organization Test in Healthy Young Adults. Arch. Phys. Med. Rehabil. 2007, 88, 1049–1054. [Google Scholar] [CrossRef]
- Goldberg, A.; Chavis, M.; Watkins, J.; Wilson, T. The five-times-sit-to-stand test: Validity, reliability and detectable change in older females. Aging Clin. Exp. Res. 2012, 24, 339–344. [Google Scholar] [CrossRef]
- Miller, W.L.; Maffei, V.; Bosco, G.; Iosa, M.; Zago, M.; Macaluso, E.; Lacquaniti, F. Vestibular nuclei and cerebellum put visual gravitational motion in context. J. Neurophysiol. 2008, 99, 1969–1982. [Google Scholar] [CrossRef] [Green Version]
- Peterka, R.J. Sensorimotor Integration in Human Postural Control. J. Neurophysiol. 2002, 88, 1097–1118. [Google Scholar] [CrossRef] [Green Version]
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing 2006, 35, 7–11. [Google Scholar] [CrossRef] [Green Version]
- King, L.; Horak, F.B. The role of the vestibular system in postural control. In Vestibular Rehabilitation, 4th ed.; FA Davis: Philadelphia, PA, USA, 2014; pp. 29–48. [Google Scholar]
- Wildenberg, J.C.; Tyler, M.E.; Danilov, Y.P.; Kaczmarek, K.A.; Meyerand, M.E. High-resolution fMRI detects neuromodulation of individual brainstem nuclei by electrical tongue stimulation in balance-impaired individuals. Neuroimage 2011, 56, 2129–2137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wildenberg, J.C.; Tyler, M.E.; Danilov, Y.P.; Kaczmarek, K.A.; Meyerand, M.E. Sustained cortical and subcortical neuromodulation induced by electrical tongue stimulation. Brain Imaging Behav. 2010, 4, 199–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wildenberg, J.C.; Tyler, M.E.; Danilov, Y.P.; Kaczmarek, K.A.; Meyerand, M.E. Electrical tongue stimulation normalizes activity within the motion-sensitive brain network in balance-impaired subjects as revealed by group independent component analysis. Brain Connect. 2011, 1, 255–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cullen, K.E.; Brooks, J.X. Neural correlates of sensory prediction errors in monkeys: Evidence for internal models of voluntary self-motion in the cerebellum. Cerebellum 2015, 14, 31–34. [Google Scholar] [CrossRef] [Green Version]
- Dieterich, M.; Bauermann, T.; Best, C.; Stoeter, P.; Schlindwein, P. Evidence for cortical visual substitution of chronic bilateral vestibular failure (an fMRI study). Brain 2007, 130, 2108–2116. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Hu, X.; Zhang, Y.; Pan, Q.; Zhan, Q.; Tan, G.; Wang, K. Effect of Vestibular Rehabilitation on Spontaneous Brain Activity in Patients With Vestibular Migraine: A Resting-State Functional Magnetic Resonance Imaging Study. Front. Hum. Neurosci. 2020, 14, 227. [Google Scholar] [CrossRef]
- Wiesmeier, I.K.; Dalin, D.; Wehrle, A.; Granacher, U.; Muehlbauer, T.; Dietterle, J.; Weiller, C.; Gollhofer, A.; Maurer, C. Balance training enhances vestibular function and reduces overactive proprioceptive feedback in elderly. Front. Aging Neurosci. 2017, 9, 273. [Google Scholar] [CrossRef]
- Lesinski, M.; Hortobagyi, T.; Muehlbauer, T.; Gollhofer, A.; Granacher, U. Effects of Balance Training on Balance Performance in Healthy Older Adults: A Systematic Review and Meta-analysis. Sports Med. 2015, 45, 1721–1738. [Google Scholar] [CrossRef] [Green Version]
- Reinthal, A. Getting the Dosage Right in Balance Exercise Prescription: The Intensity Problem. J. Nov. Physiother. 2017, 7, e147. [Google Scholar] [CrossRef] [Green Version]
| Region Label | Extent | t-Value | MNI Coordinates | |||
|---|---|---|---|---|---|---|
| x | y | z | ||||
| Pre-training | Parietal Operculum Cortex | 72 | 9.983 | −46 | −36 | 22 |
| Post-training | Cerebellar lobules I–IV | 34 | 8.141 | 20 | −44 | −26 |
| Brainstem | 102 | 7.528 | 0 | −22 | −16 | |
| Middle Frontal Gyrus | 14 | 6.453 | 48 | 6 | 46 | |
| Middle Temporal Gyrus, temporooccipital part | 22 | 6.331 | −58 | −48 | −10 | |
| Middle Frontal Gyrus | 18 | 6.147 | −34 | 6 | 32 | |
| Inferior Frontal Gyrus, pars opercularis | 10 | 5.918 | −40 | 14 | 22 | |
| Post-training > Pre-training | Cerebellar lobules V–VI | 40 | 6.408 | 36 | −48 | −28 |
| Cerebellar lobules I–IV | 74 | 6.055 | 18 | −44 | −24 | |
| Vestibular Nucleus in Brainstem | 56 | 5.920 | −12 | −32 | −42 | |
| Superior Temporal Gyrus, posterior division | 30 | 4.761 | 48 | −22 | −4 | |
| Cerebellar lobule VIIB | 28 | 4.695 | 22 | −70 | −38 | |
| Cerebellar Crus I | 22 | 4.289 | −36 | −54 | −34 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bao, T.; Noohi, F.; Kinnaird, C.; Carender, W.J.; Barone, V.J.; Peethambaran, G.; Whitney, S.L.; Seidler, R.D.; Sienko, K.H. Retention Effects of Long-Term Balance Training with Vibrotactile Sensory Augmentation in Healthy Older Adults. Sensors 2022, 22, 3014. https://doi.org/10.3390/s22083014
Bao T, Noohi F, Kinnaird C, Carender WJ, Barone VJ, Peethambaran G, Whitney SL, Seidler RD, Sienko KH. Retention Effects of Long-Term Balance Training with Vibrotactile Sensory Augmentation in Healthy Older Adults. Sensors. 2022; 22(8):3014. https://doi.org/10.3390/s22083014
Chicago/Turabian StyleBao, Tian, Fatemeh Noohi, Catherine Kinnaird, Wendy J. Carender, Vincent J. Barone, Geeta Peethambaran, Susan L. Whitney, Rachael D. Seidler, and Kathleen H. Sienko. 2022. "Retention Effects of Long-Term Balance Training with Vibrotactile Sensory Augmentation in Healthy Older Adults" Sensors 22, no. 8: 3014. https://doi.org/10.3390/s22083014
APA StyleBao, T., Noohi, F., Kinnaird, C., Carender, W. J., Barone, V. J., Peethambaran, G., Whitney, S. L., Seidler, R. D., & Sienko, K. H. (2022). Retention Effects of Long-Term Balance Training with Vibrotactile Sensory Augmentation in Healthy Older Adults. Sensors, 22(8), 3014. https://doi.org/10.3390/s22083014