
Preliminary Study of Vibrotactile Feedback during Home-Based Balance and Coordination Training in Individuals with Cerebellar Ataxia

 ,
,  , ,
, ,  ,
,
Abstract
1. Introduction
2. Methods
2.1. Study Cohort
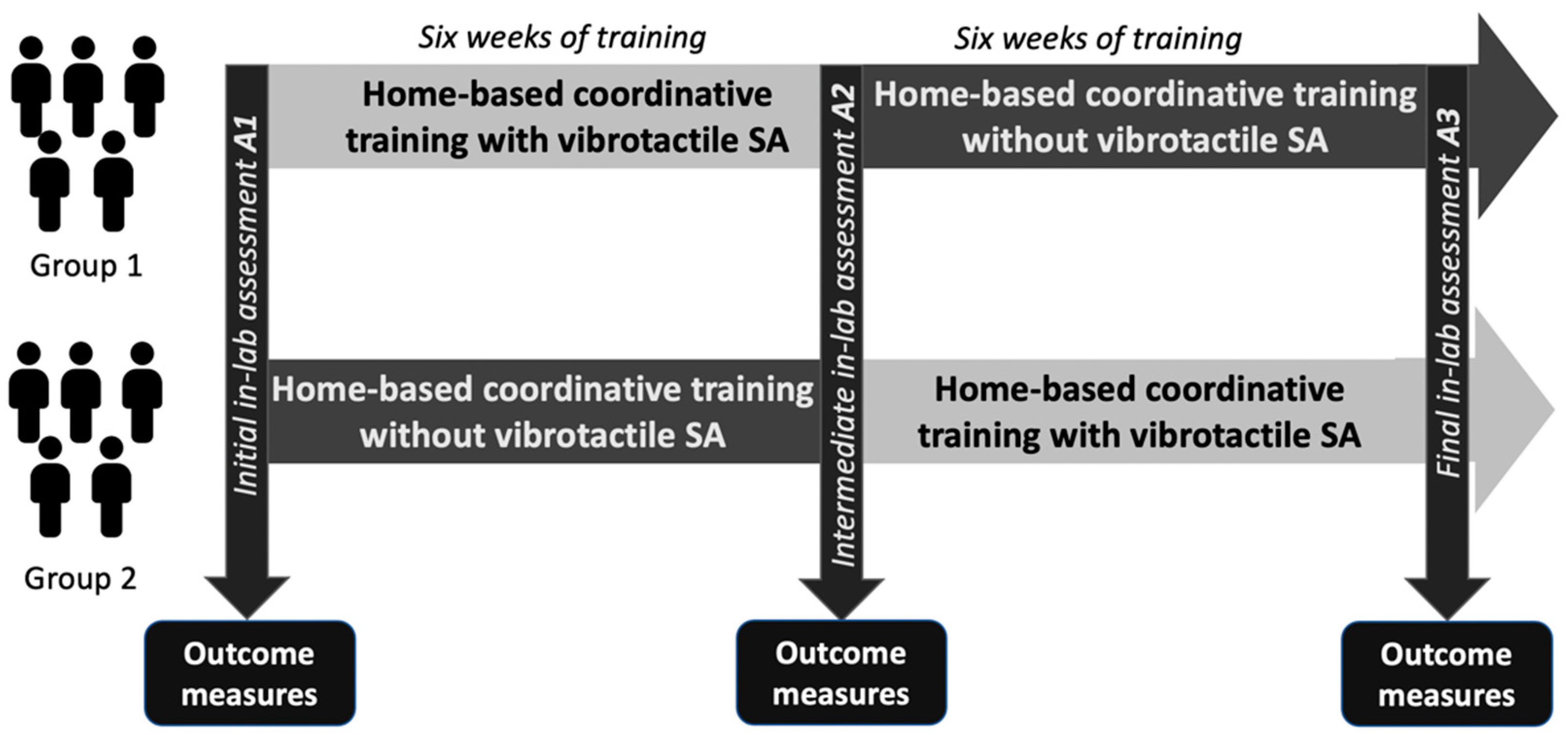
2.2. Home-Based Balance and Coordination Training
2.3. In-Laboratory Assessments
2.4. Statistical Analysis
2.4.1. Effects of 12 Weeks of Training
2.4.2. Effects of Six Weeks of Training with and without Vibrotactile SA
2.4.3. Comparison of the Effects of Training with versus without Vibrotactile SA
3. Results
3.1. Analysis of Clinical Outcome Measures
3.1.1. Effects of 12 Weeks of Training
3.1.2. Effects of Six Weeks of Training without Vibrotactile SA
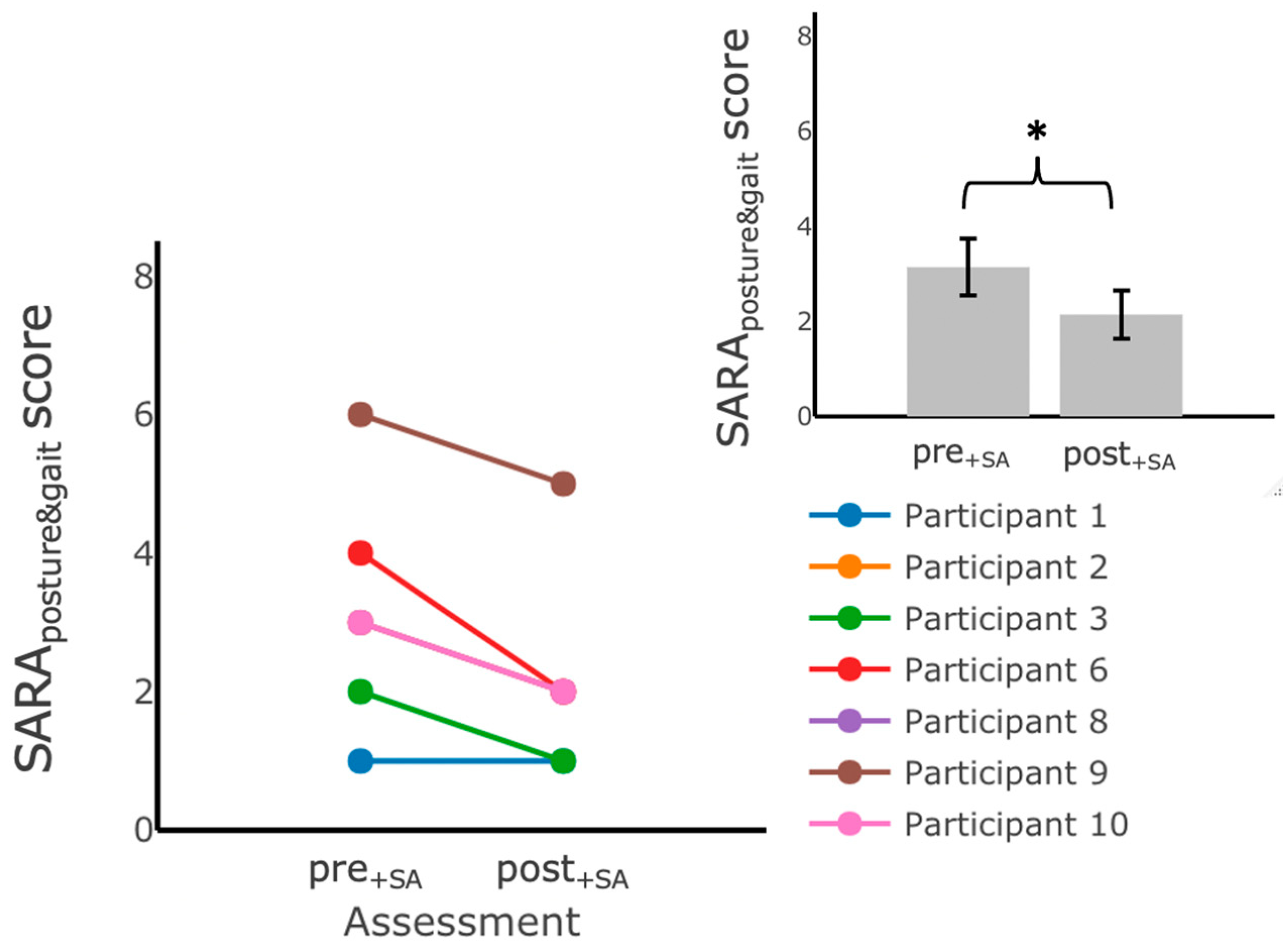
3.1.3. Effects of Six Weeks of Training with Vibrotactile SA
3.1.4. Comparison of the Effects of Training with versus without Vibrotactile SA
3.2. Effects on IMU-Based Kinematic Features
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exercise | ||||
| Firm EO | Firm EC | Foam EO | Foam EC | |
 | ||||
| MS ML Sway (deg) |  |  |  |  |
| RMS AP Sway (deg) |  |  |  |  |
| ML Sway Velocity (deg/s) |  |  |  |  |
| Exercise | ||||
| Firm EO | Firm EC | Foam EO | Foam EC | |
| AP Sway Velocity (deg/s) |  |  |  |  |
| Ellipse Area of Sway (deg2) |  |  |  |  |
| Path Length of Sway (deg) |  |  |  |  |
References
- Martino, G.; Ivanenko, Y.P.; Serrao, M.; Ranavolo, A.; d’Avella, A.; Draicchio, F.; Conte, C.; Casali, C.; Lacquaniti, F. Locomotor patterns in cerebellar ataxia. J. Neurophysiol. 2014, 112, 2810–2821. [Google Scholar] [CrossRef] [PubMed]
- Naeije, G.; Rai, M.; Allaerts, N.; Sjogard, M.; Tiège, X.D.; Pandolfo, M. Cerebellar cognitive disorder parallels cerebellar motor symptoms in Friedreich ataxia. Ann. Clin. Transl. Neurol. 2020, 7, 1050–1054. [Google Scholar] [CrossRef] [PubMed]
- Schniepp, R.; Schlick, C.; Pradhan, C.; Dieterich, M.; Brandt, T.; Jahn, K.; Wuehr, M. The interrelationship between disease severity, dynamic stability, and falls in cerebellar ataxia. J. Neurol. 2016, 263, 1409–1417. [Google Scholar] [CrossRef] [PubMed]
- Marsden, J.; Harris, C. Cerebellar ataxia: Pathophysiology and rehabilitation. Clin. Rehabil. 2011, 25, 195–216. [Google Scholar] [CrossRef]
- Asahina, M.; Nakajima, M.; Kojima, S.; Hirayama, K. Postural sway in patients with hereditary ataxia. Rinsho Shinkeigaku 1994, 34, 1105–1110. [Google Scholar]
- Diener, H.C.; Dichgans, J.; Bacher, M.; Gompf, B. Quantification of postural sway in normals and patients with cerebellar diseases. Electroencephalogr. Clin. Neurophysiol. 1984, 57, 134–142. [Google Scholar] [CrossRef]
- Buckley, E.; Mazzà, C.; McNeill, A. A systematic review of the gait characteristics associated with Cerebellar Ataxia. Gait Posture 2018, 60, 154–163. [Google Scholar] [CrossRef]
- Stolze, H.; Klebe, S.; Petersen, G.; Raethjen, J.; Wenzelburger, R.; Witt, K.; Deuschl, G. Typical features of cerebellar ataxic gait. J. Neurol. Neurosurg. Psychiatry 2002, 73, 310–312. [Google Scholar] [CrossRef]
- Ilg, W.; Timmann, D. Gait ataxia—Specific cerebellar influences and their rehabilitation. Mov. Disord. 2013, 28, 1566–1575. [Google Scholar] [CrossRef]
- Crowdy, K.A.; Hollands, M.A.; Ferguson, I.T.; Marple-Horvat, D.E. Evidence for interactive locomotor and oculomotor deficits in cerebellar patients during visually guided stepping. Exp. Brain Res. 2000, 135, 437–454. [Google Scholar] [CrossRef]
- Bunn, L.M.; Marsden, J.F.; Voyce, D.C.; Giunti, P.; Day, B.L. Sensorimotor processing for balance in spinocerebellar ataxia type 6. Mov. Disord. 2015, 30, 1259–1266. [Google Scholar] [CrossRef] [PubMed]
- Bo, J.; Block, H.J.; Clark, J.E.; Bastian, A.J. A Cerebellar Deficit in Sensorimotor Prediction Explains Movement Timing Variability. J. Neurophysiol. 2008, 100, 2825–2832. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ilg, W.; Synofzik, M.; Brötz, D.; Burkard, S.; Giese, M.A.; Schöls, L. Intensive coordinative training improves motor performance in degenerative cerebellar disease. Neurology 2009, 73, 1823–1830. [Google Scholar] [CrossRef] [PubMed]
- Ilg, W.; Bastian, A.J.; Boesch, S.; Burciu, R.G.; Celnik, P.; Claaßen, J.; Feil, K.; Kalla, R.; Miyai, I.; Nachbauer, W.; et al. Consensus Paper: Management of Degenerative Cerebellar Disorders. Cerebellum 2014, 13, 248–268. [Google Scholar] [CrossRef]
- Milne, S.C.; Corben, L.A.; Georgiou-Karistianis, N.; Delatycki, M.B.; Yiu, E.M. Rehabilitation for Individuals With Genetic Degenerative Ataxia: A Systematic Review. Neurorehabil. Neural Repair 2017, 31, 609–622. [Google Scholar] [CrossRef]
- Assländer, L.; Peterka, R.J. Sensory reweighting dynamics in human postural control. J. Neurophysiol. 2014, 111, 1852–1864. [Google Scholar] [CrossRef]
- Haran, F.J.; Keshner, E.A. Sensory Reweighting as a Method of Balance Training for Labyrinthine Loss. J. Neurol. Phys. Ther. JNPT 2008, 32, 186–191. [Google Scholar] [CrossRef]
- Anson, E.; Jeka, J. Sensory Reweighting: A Rehabilitative Mechanism? In Handbook of Medical Neuropsychology: Applications of Cognitive Neuroscience; Armstrong, C.L., Morrow, L., Eds.; Springer: New York, NY, USA, 2010; pp. 519–529. ISBN 978-1-4419-1364-7. [Google Scholar]
- van Dieën, J.H.; van Leeuwen, M.; Faber, G.S. Learning to balance on one leg: Motor strategy and sensory weighting. J. Neurophysiol. 2015, 114, 2967–2982. [Google Scholar] [CrossRef]
- Zesiewicz, T.A.; Wilmot, G.; Kuo, S.-H.; Perlman, S.; Greenstein, P.E.; Ying, S.H.; Ashizawa, T.; Subramony, S.H.; Schmahmann, J.D.; Figueroa, K.P.; et al. Comprehensive systematic review summary: Treatment of cerebellar motor dysfunction and ataxia: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2018, 90, 464–471. [Google Scholar] [CrossRef]
- Ilg, W.; Brötz, D.; Burkard, S.; Giese, M.A.; Schöls, L.; Synofzik, M. Long-term effects of coordinative training in degenerative cerebellar disease. Mov. Disord. 2010, 25, 2239–2246. [Google Scholar] [CrossRef]
- Miyai, I.; Ito, M.; Hattori, N.; Mihara, M.; Hatakenaka, M.; Yagura, H.; Sobue, G.; Nishizawa, M. Cerebellar Ataxia Rehabilitation Trial in Degenerative Cerebellar Diseases. Neurorehabil. Neural Repair 2012, 26, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Ilg, W.; Schatton, C.; Schicks, J.; Giese, M.A.; Schöls, L.; Synofzik, M. Video game-based coordinative training improves ataxia in children with degenerative ataxia. Neurology 2012, 79, 2056–2060. [Google Scholar] [CrossRef] [PubMed]
- Tercero-Pérez, K.; Cortés, H.; Torres-Ramos, Y.; Rodríguez-Labrada, R.; Cerecedo-Zapata, C.M.; Hernández-Hernández, O.; Pérez-González, N.; González-Piña, R.; Leyva-García, N.; Cisneros, B.; et al. Effects of Physical Rehabilitation in Patients with Spinocerebellar Ataxia Type 7. Cerebellum Lond. Engl. 2019, 18, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Díaz, J.C.; Velázquez-Pérez, L.; Rodríguez Labrada, R.; Aguilera Rodríguez, R.; Laffita Pérez, D.; Canales Ochoa, N.; Medrano Montero, J.; Estupiñán Rodríguez, A.; Osorio Borjas, M.; Góngora Marrero, M.; et al. Neurorehabilitation therapy in spinocerebellar ataxia type 2: A 24-week, rater-blinded, randomized, controlled trial. Mov. Disord. 2018, 33, 1481–1487. [Google Scholar] [CrossRef]
- Keller, J.L.; Bastian, A.J. A Home Balance Exercise Program Improves Walking in People With Cerebellar Ataxia. Neurorehabil. Neural Repair 2014, 28, 770–778. [Google Scholar] [CrossRef]
- Marquer, A.; Barbieri, G.; Pérennou, D. The assessment and treatment of postural disorders in cerebellar ataxia: A systematic review. Ann. Phys. Rehabil. Med. 2014, 57, 67–78. [Google Scholar] [CrossRef]
- Seco, J.; Gago Fernández, I.; Casado, V.; Rodríguez Pérez, V.; Fernández-Atutxa, A.; Torres-Unda, J. Improvements in Quality of Life in Individuals with Friedreich’s Ataxia after Participation in a 5-Year Program of Physical Activity: An observational Study Pre-Post Test Design, and Two Years Follow-Up. Int. J. Neurorehabil. 2014, 1, 129. [Google Scholar] [CrossRef]
- Trouillas, P.; Takayanagi, T.; Hallett, M.; Currier, R.D.; Subramony, S.H.; Wessel, K.; Bryer, A.; Diener, H.C.; Massaquoi, S.; Gomez, C.M.; et al. International Cooperative Ataxia Rating Scale for pharmacological assessment of the cerebellar syndrome. J. Neurol. Sci. 1997, 145, 205–211. [Google Scholar] [CrossRef]
- Kao, C.-L.; Chen, L.-K.; Chern, C.-M.; Hsu, L.-C.; Chen, C.-C.; Hwang, S.-J. Rehabilitation outcome in home-based versus supervised exercise programs for chronically dizzy patients. Arch. Gerontol. Geriatr. 2010, 51, 264–267. [Google Scholar] [CrossRef]
- Lacroix, A.; Hortobágyi, T.; Beurskens, R.; Granacher, U. Effects of Supervised vs. Unsupervised Training Programs on Balance and Muscle Strength in Older Adults: A Systematic Review and Meta-Analysis. Sports Med. 2017, 47, 2341–2361. [Google Scholar] [CrossRef]
- Youssef, E.F.; Shanb, A.A. elhameed Supervised Versus Home Exercise Training Programs on Functional Balance in Older Subjects. Malays. J. Med. Sci. MJMS 2016, 23, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Barbuto, S.; Kuo, S.-H.; Stein, J. Investigating the Clinical Significance and Research Discrepancies of Balance Training in Degenerative Cerebellar Disease: A Systematic Review. Am. J. Phys. Med. Rehabil. 2020, 99, 989–998. [Google Scholar] [CrossRef] [PubMed]
- Sienko, K.H.; Seidler, R.D.; Carender, W.J.; Goodworth, A.D.; Whitney, S.L.; Peterka, R.J. Potential Mechanisms of Sensory Augmentation Systems on Human Balance Control. Front. Neurol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Sienko, K.H.; Whitney, S.L.; Carender, W.J.; Wall, C. The role of sensory augmentation for people with vestibular deficits: Real-time balance aid and/or rehabilitation device? J. Vestib. Res. Equilib. Orientat. 2017, 27, 63–76. [Google Scholar] [CrossRef]
- Zimmet, A.M.; Cao, D.; Bastian, A.J.; Cowan, N.J. Cerebellar patients have intact feedback control that can be leveraged to improve reaching. eLife 2020, 9, e53246. [Google Scholar] [CrossRef]
- Shull, P.B.; Damian, D.D. Haptic wearables as sensory replacement, sensory augmentation and trainer—A review. J. NeuroEng. Rehabil. 2015, 12, 59. [Google Scholar] [CrossRef]
- Bao, T.; Carender, W.J.; Kinnaird, C.; Barone, V.J.; Peethambaran, G.; Whitney, S.L.; Kabeto, M.; Seidler, R.D.; Sienko, K.H. Effects of long-term balance training with vibrotactile sensory augmentation among community-dwelling healthy older adults: A randomized preliminary study. J. NeuroEng. Rehabil. 2018, 15, 5. [Google Scholar] [CrossRef]
- Bao, T.; Klatt, B.N.; Carender, W.J.; Kinnaird, C.; Alsubaie, S.; Whitney, S.L.; Sienko, K.H. Effects of long-term vestibular rehabilitation therapy with vibrotactile sensory augmentation for people with unilateral vestibular disorders - A randomized preliminary study. J. Vestib. Res. Equilib. Orientat. 2019, 29, 323–334. [Google Scholar] [CrossRef]
- Gordt, K.; Gerhardy, T.; Najafi, B.; Schwenk, M. Effects of Wearable Sensor-Based Balance and Gait Training on Balance, Gait, and Functional Performance in Healthy and Patient Populations: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Gerontology 2018, 64, 74–89. [Google Scholar] [CrossRef]
- Huang, H.; Wolf, S.L.; He, J. Recent developments in biofeedback for neuromotor rehabilitation. J. NeuroEng. Rehabil. 2006, 3, 11. [Google Scholar] [CrossRef]
- Sienko, K.H.; Balkwill, M.D.; Oddsson, L.I.E.; Wall, C. Effects of multi-directional vibrotactile feedback on vestibular-deficient postural performance during continuous multi-directional support surface perturbations. J. Vestib. Res. 2008, 18, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Karan, A.; Alptekin, H.K.; Çapan, N.; Dıraçoğlu, D.; Saral, İ.; Aydın, S.; Aksoy, C. The efficacy of vestibular electrical stimulation on patients with unilateral vestibular pathologies. Turk. J. Phys. Med. Rehabil. 2017, 63, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Čakrt, O.; Vyhnálek, M.; Slabý, K.; Funda, T.; Vuillerme, N.; Kolář, P.; Jeřábek, J. Balance rehabilitation therapy by tongue electrotactile biofeedback in patients with degenerative cerebellar disease. NeuroRehabilitation 2012, 31, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Tyler, M.; Danilov, Y.; Bach-Y-Rita, P. Closing an open-loop control system: Vestibular substitution through the tongue. J. Integr. Neurosci. 2003, 2, 159–164. [Google Scholar] [CrossRef]
- Bach-y-Rita, P.; Kercel, S.W. Sensory substitution and the human-machine interface. Trends Cogn. Sci. 2003, 7, 541–546. [Google Scholar] [CrossRef]
- Audio-biofeedback for Balance Improvement: An Accelerometry-Based System. IEEE J. Mag. IEEE Xplore 2005, 52, 2108–2111. Available online: https://ieeexplore.ieee.org/document/1542462 (accessed on 20 July 2021).
- Dozza, M.; Horak, F.B.; Chiari, L. Auditory biofeedback substitutes for loss of sensory information in maintaining stance. Exp. Brain Res. 2007, 178, 37–48. [Google Scholar] [CrossRef]
- Schatton, C.; Synofzik, M.; Fleszar, Z.; Giese, M.A.; Schöls, L.; Ilg, W. Individualized exergame training improves postural control in advanced degenerative spinocerebellar ataxia: A rater-blinded, intra-individually controlled trial. Parkinsonism Relat. Disord. 2017, 39, 80–84. [Google Scholar] [CrossRef]
- Davis, J.R.; Carpenter, M.G.; Tschanz, R.; Meyes, S.; Debrunner, D.; Burger, J.; Allum, J.H.J. Trunk sway reductions in young and older adults using multi-modal biofeedback. Gait Posture 2010, 31, 465–472. [Google Scholar] [CrossRef]
- Lee, B.-C.; Kim, J.; Chen, S.; Sienko, K.H. Cell phone based balance trainer. J. NeuroEng. Rehabil. 2012, 9, 10. [Google Scholar] [CrossRef]
- Wu, G. Real-time feedback of body center of gravity for postural training of elderly patients with peripheral neuropathy. IEEE Trans. Rehabil. Eng. Publ. IEEE Eng. Med. Biol. Soc. 1997, 5, 399–402. [Google Scholar] [CrossRef]
- Shen, X.; Mak, M.K.Y. Balance and Gait Training With Augmented Feedback Improves Balance Confidence in People With Parkinson’s Disease: A Randomized Controlled Trial. Neurorehabil. Neural Repair 2014, 28, 524–535. [Google Scholar] [CrossRef] [PubMed]
- van den Heuvel, M.R.C.; van Wegen, E.E.H.; de Goede, C.J.T.; Burgers-Bots, I.A.L.; Beek, P.J.; Daffertshofer, A.; Kwakkel, G. The effects of augmented visual feedback during balance training in Parkinson’s disease: Study design of a randomized clinical trial. BMC Neurol. 2013, 13, 137. [Google Scholar] [CrossRef] [PubMed]
- Yen, C.-Y.; Lin, K.-H.; Hu, M.-H.; Wu, R.-M.; Lu, T.-W.; Lin, C.-H. Effects of virtual reality-augmented balance training on sensory organization and attentional demand for postural control in people with Parkinson disease: A randomized controlled trial. Phys. Ther. 2011, 91, 862–874. [Google Scholar] [CrossRef]
- Therrien, A.S.; Statton, M.A.; Bastian, A.J. Reinforcement Signaling Can Be Used to Reduce Elements of Cerebellar Reaching Ataxia. Cerebellum Lond. Engl. 2021, 20, 62–73. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Subramanian, S.K.; Massie, C.L.; Malcolm, M.P.; Levin, M.F. Does provision of extrinsic feedback result in improved motor learning in the upper limb poststroke? A systematic review of the evidence. Neurorehabil. Neural Repair 2010, 24, 113–124. [Google Scholar] [CrossRef]
- Thomas, D.M. The Effects of Relative Frequency of Knowledge of Results on Brain Injured and Neurologically Normal Individuals Learning a Linear Positioning Task. Master’s Thesis, Grand Valley State University, Allendale, MI, USA, 1995. [Google Scholar]
- Klatt, B.N.; Carender, W.J.; Lin, C.C.; Alsubaie, S.F.; Kinnaird, C.R.; Sienko, K.H.; Whitney, S.L. A Conceptual Framework for the Progression of Balance Exercises in Persons with Balance and Vestibular Disorders. Phys. Med. Rehabil. Int. 2015, 2, 1044. [Google Scholar]
- Schmitz-Hübsch, T.; du Montcel, S.T.; Baliko, L.; Berciano, J.; Boesch, S.; Depondt, C.; Giunti, P.; Globas, C.; Infante, J.; Kang, J.-S.; et al. Scale for the assessment and rating of ataxia: Development of a new clinical scale. Neurology 2006, 66, 1717–1720. [Google Scholar] [CrossRef]
- Ilg, W.; Seemann, J.; Giese, M.; Traschütz, A.; Schöls, L.; Timmann, D.; Synofzik, M. Real-life gait assessment in degenerative cerebellar ataxia: Toward ecologically valid biomarkers. Neurology 2020, 95, e1199–e1210. [Google Scholar] [CrossRef]
- Winser, S.J.; Smith, C.M.; Hale, L.A.; Claydon, L.S.; Whitney, S.L. Clinical assessment of balance using BBS and SARAbal in cerebellar ataxia: Synthesis of findings of a psychometric property analysis. Hong Kong Physiother. J. 2018, 38, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Cohen, H.; Blatchly, C.A.; Gombash, L.L. A Study of the Clinical Test of Sensory Interaction and Balance. Phys. Ther. 1993, 73, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Dynamic Gait Index|RehabMeasures Database. Available online: https://www.sralab.org/rehabilitation-measures/dynamic-gait-index (accessed on 20 July 2021).
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the Probability for Falls in Community-Dwelling Older Adults Using the Timed Up & Go Test. Phys. Ther. 2000, 80, 896–903. [Google Scholar] [CrossRef]
- Bohannon, R.W. Test-Retest Reliability of the Five-Repetition Sit-to-Stand Test: A Systematic Review of the Literature Involving Adults. J. Strength Cond. Res. 2011, 25, 3205–3207. [Google Scholar] [CrossRef]
- Ghislieri, M.; Gastaldi, L.; Pastorelli, S.; Tadano, S.; Agostini, V. Wearable Inertial Sensors to Assess Standing Balance: A Systematic Review. Sensors 2019, 19, 4075. [Google Scholar] [CrossRef]
- Neville, C.; Ludlow, C.; Rieger, B. Measuring postural stability with an inertial sensor: Validity and sensitivity. Med. Devices Auckl. NZ 2015, 8, 447–455. [Google Scholar] [CrossRef]
- Bigelow, K.E. Identification of Key Traditional and Fractal Postural Sway Parameters to Develop a Clinical Protocol for Fall Risk Assessment in Older Adults. Ph.D. Thesis, Department of Mechanical Engineering, The Ohio State University, Columbus, OH, USA, 2008. [Google Scholar]
- Sakanaka, T.E.; Lakie, M.; Reynolds, R.F. Idiosyncratic Characteristics of Postural Sway in Normal and Perturbed Standing. Front. Hum. Neurosci. 2021, 15, 243. [Google Scholar] [CrossRef]
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 3 December 2021).
- Armstrong, R.A. When to use the Bonferroni correction. Ophthalmic Physiol. Opt. 2014, 34, 502–508. [Google Scholar] [CrossRef]
- Bunn, L.M.; Marsden, J.F.; Giunti, P.; Day, B.L. Training balance with opto-kinetic stimuli in the home: A randomized controlled feasibility study in people with pure cerebellar disease. Clin. Rehabil. 2015, 29, 143–153. [Google Scholar] [CrossRef]
- Bao, T.; Noohi, F.; Kinnaird, C.; Carender, W.J.; Barone, V.J.; Peethambaran, G.; Whitney, S.L.; Seidler, R.D.; Sienko, K.H. Retention Effects of Long-Term Balance Training with Vibrotactile Sensory Augmentation in Healthy Older Adults. Sensors 2022, 22, 3014. [Google Scholar] [CrossRef] [PubMed]
- Burciu, R.G.; Fritsche, N.; Granert, O.; Schmitz, L.; Spönemann, N.; Konczak, J.; Theysohn, N.; Gerwig, M.; van Eimeren, T.; Timmann, D. Brain Changes Associated with Postural Training in Patients with Cerebellar Degeneration: A Voxel-Based Morphometry Study. J. Neurosci. 2013, 33, 4594–4604. [Google Scholar] [CrossRef] [PubMed]
- Scale for Assessment and Rating of Ataxia. Available online: https://www.sralab.org/rehabilitation-measures/scale-assessment-and-rating-ataxia (accessed on 22 July 2021).








| Participant ID | Experimental Group | Diagnosis | Sex | Age |
|---|---|---|---|---|
| 1 | Group 1 | Spinocerebellar ataxia type 2 (SCA2) | M | 27 |
| 2 | Group 1 | Autosomal recessive cerebellar ataxia type 1 (ARCA1) | M | 49 |
| 3 | Group 1 | Spinocerebellar ataxia type 2 (SCA2) | M | 63 |
| 4 | Group 1 * | Spinocerebellar ataxia type 2 (SCA2) | F | 41 |
| 5 | Group 1 † | Friedreich’s Ataxia (FA) | F | 49 |
| 6 | Group 2 | Spinocerebellar ataxia type 1 (SCA1) | F | 32 |
| 7 | Group 2 † | Spinocerebellar ataxia type 1 (SCA1) | M | 37 |
| 8 | Group 2 | Niemann–Pick C (NPC) | F | 63 |
| 9 | Group 2 | Spinocerebellar ataxia type 1 (SCA1) | M | 57 |
| 10 | Group 2 | Niemann–Pick C (NPC) | F | 49 |
| Exercise Category | Brief Description | Vibrotactile SA Threshold |
|---|---|---|
| Static Standing | Standing on a firm surface, e.g., a tiled, linoleum or wood-covered floor. Participants were instructed to stand tall with eyes looking straight ahead and to minimize sway. | Anterior: 2.0° Posterior: 2.0° ML: 2.5° (on each side) |
| Standing on a Compliant Surface | Standing on a compliant surface, e.g., a foam pad or Bosu ball Participants were instructed to stand tall with eyes looking straight ahead and to minimize sway. | Anterior: 3.0° Posterior: 2.0° ML: 3.0° (on each side) |
| Arm Raises | Participants were instructed to stand tall with eyes looking straight ahead and to minimize sway as arms were lifted forward to shoulder height (90°). | Anterior: 3.0° Posterior: 3.0° ML: 3.0° (on each side) |
| Weight Shifting | Participants were instructed to keep feet in one position and move the body from side to side or forward and backward. The magnitude of the side-to-side or forward–backward tilt was included in the instructions (maximum tilt or medium tilt) and defined as a target position within the smartphone-based balance trainer. | Anterior: 1.0° Posterior: 1.0° ML: 1.0° (on each side) |
| Gait | Participants were instructed to perform gait tasks that included walking fast, walking slow, walking with horizontal or vertical head turns, side-stepping, high march, etc. | N/A (no vibrotactile SA was provided) |
 | Standing with feet apart on firm ground with eyes open (Firm, EO) |
 | Standing with feet apart on firm ground with eyes closed (Firm, EC) |
 | Standing with feet apart on foam with eyes open (Foam, EO) |
 | Standing with feet apart on foam with eyes closed (Foam, EC) |
| Feature | Definition | Equation |
|---|---|---|
| RMS ML Sway (°) | Root-mean-square of the ML angular displacement | N = number of data points |
| RMS AP Sway (°) | Root-mean-square of the AP angular displacement | N = number of data points |
| RMS ML Sway Velocity (°/s) | Root-mean-square of the ML angular velocity | N = number of data point |
| RMS AP Sway Velocity (°/s) | Root-mean-square of the AP angular velocity | N = number of data points |
| 95% confidence interval of an ellipse fit to angular displacement | ||
| Path Length (°) | Total angular distance traveled | angular displacement (°) |
| Participant ID | Group | Asessment | SARA | SARAposture&gait | TUG | TUG-Motor | 5XSST | mCTSIB | DGI |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 1 | A1 | 7 | 1 | 10.8 | 13.6 | 9.1 | 99.1 | 19 |
| A2 | 6.5 | 1 | 11.6 | 13.8 | 8.3 | 104.6 | 20 | ||
| A3 | 5.5 | 1 | 11.8 | 12.7 | 9.0 | 97.9 | 20 | ||
| 2 | 1 | A1 | 8 | 3 | 14.5 | 15.9 | 13.0 | 120 | 19 |
| A2 | 7 | 2 | 12.2 | 12.6 | 14.1 | 120 | - | ||
| A3 | 9.5 | 3 | 11.4 | 12.0 | 12.2 | 120 | 13 | ||
| 3 | 1 | A1 | 6.5 | 2 | 9.5 | 12.6 | 14.0 | 120 | 20 |
| A2 | 4 | 1 | 9.6 | 15.1 | 12.0 | 120 | 19 | ||
| A3 | 5 | 1 | 9.0 | 16.5 | 11.4 | 113.6 | 22 | ||
| 5 | 1 | A1 | 13 | 5 | 12.6 | 14.2 | 15.2 | 91.6 | 12 |
| A2 | 13.5 | 5 | 12.2 | 14.8 | 17.8 | 103.7 | 17 | ||
| - | - | - | - | - | - | - | - | ||
| 6 | 2 | A1 | 8.5 | 2 | 18.6 | 21.7 | 19.0 | 103.1 | 17 |
| A2 | 10.5 | 4 | 14.9 | 27.5 | 22.2 | 102.4 | 18 | ||
| A3 | 8 | 2 | 14.4 | 20.4 | 22.9 | 113.8 | 13 | ||
| 7 | 2 | A1 | 7.5 | 3 | 11.3 | 22.0 | 12.9 | 100.8 | 21 |
| A2 | 6 | 2 | 13.0 | 18.0 | 14.5 | 120 | 17 | ||
| - | - | - | - | - | - | - | - | ||
| 8 | 2 | A1 | 7 | 2 | 24.6 | 30.1 | 27.1 | 117.9 | 8 |
| A2 | 7.5 | 3 | 18.1 | 22.7 | 17.0 | 120 | 10 | ||
| A3 | 7 | 2 | 16.5 | 20.9 | 19.3 | 117.3 | 10 | ||
| 9 | 2 | A1 | 17 | 8 | 48.5 | - | 20.1 | 90 | 0 |
| A2 | 14 | 6 | 41.4 | - | 24.9 | 79 | 3 | ||
| A3 | 13.5 | 5 | 41.5 | - | 24.3 | 94.4 | 3 | ||
| 10 | 2 | A1 | 11.5 | 3 | 11.2 | 13.3 | 12.1 | 120 | 18 |
| A2 | 9.5 | 3 | 12.1 | 13.6 | 11.5 | 120 | 21 | ||
| A3 | 8.5 | 2 | 12.4 | 14.0 | 10.8 | 120 | 22 |
| Outcome Measures | Baseline | Change (Post−Pre) | ||||
|---|---|---|---|---|---|---|
| Training without Vibrotactile SA | Training with Vibrotactile SA | Training without Vibrotactile SA | Training with Vibrotactile SA | Training Overall | ||
| SARA | Group 1 | 5.83 (1.61) | 7.17 (0.76) | 0.83 (1.76) | −1.33 (1.04) | −0.50 (1.73) |
| Mean (SD) | Group 2 | 11.00 (4.42) | 10.38 (2.72) | −0.63 (2.29) | −1.13 (0.95) | −1.75 (1.76) |
| Overall | 8.79 (4.27) | 9.00 (2.61) | 0.00 (2.06) | −1.21 (0.91) * | −1.21 (1.73) | |
| SARAposture&gait | Group 1 | 1.33 (0.58) | 2.00 (1.00) | 0.33 (0.58) | −0.67 (0.58) | −0.33 (0.58) |
| Mean (SD) | Group 2 | 4 (2.87) | 4.00 (1.14) | 0.25 (1.71) | −1.25 (0.50) | −1.0 (1.41) |
| Overall | 2.71 (2.43) | 3.14 (1.57) | 0.29 (1.25) | −1.00 (0.58) * | −0.71 (1.11) | |
| TUG | Group 1 | 11.13 (1.36) | 11.6 (2.59) | −0.40 (0.53) | −0.47 (1.63) | −0.87 (2.07) |
| Mean (SD) | Group 2 | 25.73 (16.14) | 21.63 (13.41) | −4.10 (3.65) | −0.43 (0.85) | −4.53 (4.15) |
| Overall | 19.47 (13.84) | 17.33 (10.99) | −2.51 (3.26) | −0.44 (1.12) | −2.96 (3.73) | |
| TUG-Motor | Group 1 | 13.83 (1.25) | 14.03 (1.69) | −0.10 (1.32) | −0.20 (2.92) | −0.30 (3.93) |
| Mean (SD) | Group 2 | 16.28 (8.4) | 21.27 (7.06) | −0.33 (6.63) | −2.13 (3.86) | −0.20 (1.01) |
| Overall | 17.77 (6.89) | 17.65 (6.06) | −0.27 (4.28) | −1.52 (3.38) | −0.25 (2.57) | |
| 5XSST | Group 1 | 11.47 (2.94) | 11.33 (3.79) | −0.60 (1.3) | −0.57 (1.56) | −1.17 (1.29) |
| Mean (SD) | Group 2 | 19.58 (6.14) | 18.90 (5.92) | −0.68 (6.68) | 0.43 (1.40) | −0.25 (5.63) |
| Overall | 16.10 (6.36) | 15.66 (6.22) | −0.64 (4.78) | 0.00 (1.44) | −0.64 (4.08) | |
| mCTSIB | Group 1 | 114.87 (8.89) | 113.03 (12.07) | −4.37 (3.78) | 1.83 (3.18) | −2.53 (3.40) |
| Mean (SD) | Group 2 | 107.75 (14.02) | 105.35 (19.43) | −2.40 (5.86) | 6.03 (8.74) | 3.63 (5.22) |
| Overall | 110.80 (11.79) | 108.64 (15.94) | −3.24 (4.80) | 4.23 (6.83) | 0.99 (5.32) | |
| DGI | Group 1 | 19.5 (0.71) | 19.5 (0.71) | 1.50 (2.12) | 0.00 (1.41) | 1.50 (0.71) |
| Mean (SD) | Group 2 | 10.75 (8.46) | 13.00 (8.12) | 2.25 (0.96) | −1.00 (2.71) | 1.25 (3.59) |
| Overall | 13.67 (7.97) | 15.17 (7.14) | 2.00 (1.26) * | −0.67 (2.25) | 1.33 (2.80) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jabri, S.; Bushart, D.D.; Kinnaird, C.; Bao, T.; Bu, A.; Shakkottai, V.G.; Sienko, K.H. Preliminary Study of Vibrotactile Feedback during Home-Based Balance and Coordination Training in Individuals with Cerebellar Ataxia. Sensors 2022, 22, 3512. https://doi.org/10.3390/s22093512
Jabri S, Bushart DD, Kinnaird C, Bao T, Bu A, Shakkottai VG, Sienko KH. Preliminary Study of Vibrotactile Feedback during Home-Based Balance and Coordination Training in Individuals with Cerebellar Ataxia. Sensors. 2022; 22(9):3512. https://doi.org/10.3390/s22093512
Chicago/Turabian StyleJabri, Safa, David D. Bushart, Catherine Kinnaird, Tian Bao, Angel Bu, Vikram G. Shakkottai, and Kathleen H. Sienko. 2022. "Preliminary Study of Vibrotactile Feedback during Home-Based Balance and Coordination Training in Individuals with Cerebellar Ataxia" Sensors 22, no. 9: 3512. https://doi.org/10.3390/s22093512
APA StyleJabri, S., Bushart, D. D., Kinnaird, C., Bao, T., Bu, A., Shakkottai, V. G., & Sienko, K. H. (2022). Preliminary Study of Vibrotactile Feedback during Home-Based Balance and Coordination Training in Individuals with Cerebellar Ataxia. Sensors, 22(9), 3512. https://doi.org/10.3390/s22093512